Factors Associated with Quality of Dying and Death in Korean Intensive Care Units: Perceptions of Nurses


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
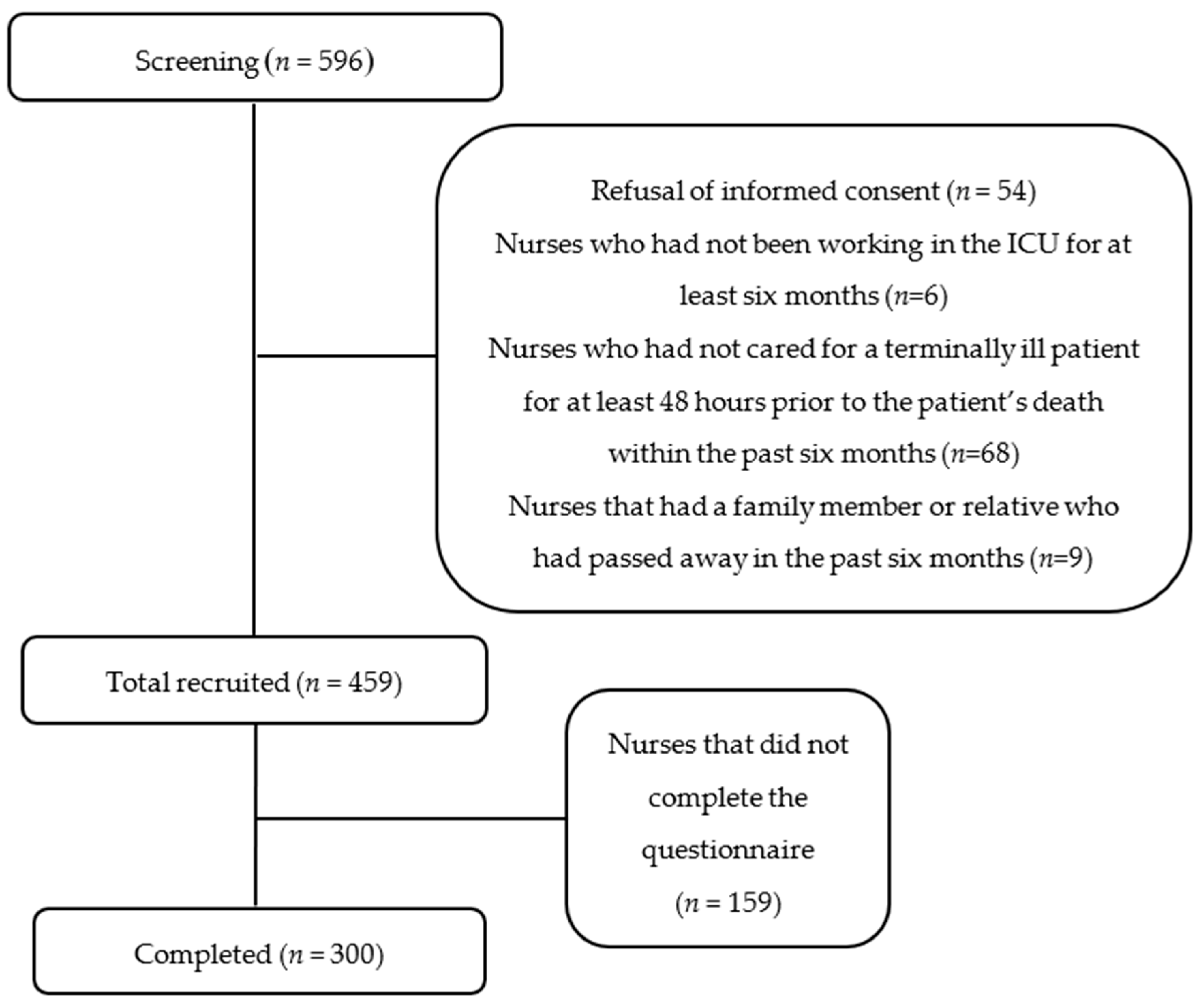
2.3. Participants
2.4. Ethical Considerations
2.5. Data Collection
2.6. Instruments
2.6.1. The QODD Korean Language Version 3.2
2.6.2. Person-Centered Critical Care Nursing (PCCN)
2.7. Data Analysis
3. Results
3.1. QODD, PCCN, and Overall Quality of Death as Perceived by Nurses
3.2. QODD and PCCN Based on the Treatment Received during the Patient’s Hours of Death
3.3. QODD and PCCN Scores According to the General Characteristics of Nurses
3.4. The Correlations among QODD, PCCN, and Overall Quality of Death
3.5. Factors Associated with QODD
4. Discussion
4.1. QOOD and PCCN Score of ICU Nurses
4.2. QODD and PCCN According to the Patient’s Treatment at the End of Life
4.3. Improving PCCN Could Increase QOOD
4.4. Consultation with Patients on the End-of-Life Treatment Issue Could Increase QOOD
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistics Korea. Statistics on Birth and Death of 2018. 2018. Available online: http://kostat.go.kr/portal/eng/pressReleases/8/10/index.board (accessed on 1 March 2020).
- Connor, S.R.; Tecca, M.; LundPerson, J.; Teno, J. Measuring hospice care: The National Hospice and Palliative Care Organization National Hospice Data Set. J. Pain Symptom Manag. 2004, 28, 316–328. [Google Scholar] [CrossRef] [PubMed]
- Park, S. Current Status of the Life-Sustaining Treatment in Elderly Patients Admitted to the Intensive Care Unit at a University Hospital. Hanyang University, Seoul, Korea, 2016. Unpublished Master’s Thesis. [Google Scholar]
- Min, D.; Cho, E. Concept Analysis of Good Death in Korean Society. J. Korean Gerontol. Nurs. 2017, 19, 28–38. [Google Scholar] [CrossRef]
- Kim, Y. Signification and challenges of the act on life-prolongation determination-with focus on patient-oriented medical care. Korean J. Health Commun. 2019, 13, 53–61. [Google Scholar]
- Seo, H.K. One Year and Five Months into Effect of the Lifelong Health Care Determination Act…54,000 People Chose Dignity History. Available online: https://www.yna.co.kr/view/AKR20190710119300017 (accessed on 25 September 2020).
- Korean Catholic Hospice Association. Understanding of Hospice; Hyunmoon Publishing Co.: Seoul, Korea, 2005. [Google Scholar]
- O’Connell, E. Therapeutic relationships in critical care nursing: A reflection on practice. Nurs. Crit. Care 2008, 13, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- University of Washington School of Medicine. Quality of Dying and Death Questionnaire for Nurses: Version 3.2. Healthcare Professional After-Death Self-Administered Questionnaire [Internet]; University of Washington School of Medicine: Seattle, WA, USA; Available online: http://depts.washington.edu/eolcare/pubs/wp-content/uploads/2011/08/nurseqodd3_2.pdf (accessed on 2 February 2020).
- Cho, J.Y.; Lee, J.; Lee, S.M.; Park, J.H.; Kim, J.; Kim, Y.; Lee, S.H.; Park, J.S.; Cho, Y.J.; Yoon, H.I.; et al. Transcultural Adaptation and Validation of Quality of Dying and Death Questionnaire in Medical Intensive Care Units in South Korea. Acute Crit. Care 2018, 33, 95–101. [Google Scholar] [CrossRef]
- Cho, J.Y.; Park, J.H.; Kim, J.; Lee, J.; Park, J.S.; Cho, Y.J.; Yoon, H.I.; Lee, S.M.; Lee, J.H.; Lee, C.T.; et al. Factors Associated with Quality of Death in Korean ICUs As Perceived by Medical Staff: A Multicenter Cross-Sectional Survey. Crit. Care Med. 2019, 47, 1208–1215. [Google Scholar] [CrossRef]
- Kang, J.Y.; Cho, Y.S.; Jung, Y.J.; Kim, S.K.; Youn, S.Y.; Shim, M.Y. Development and Validation of a Measurement to Assess Person-centered Critical Care Nursing. J. Korean Acad. Nurs. 2018, 48, 323–334. [Google Scholar] [CrossRef]
- Choi, S. Factors affecting to the Person-Centered Care among Critical Care Nurses. J. Korean Crit. Care Nurs. 2020, 13, 36–44. [Google Scholar] [CrossRef]
- Boissier, F.; Seegers, V.; Seguin, A.; Legriel, S.; Cariou, A.; Jaber, S.; Lefrant, J.-Y.; Rimmelé, T.; Renault, A.; Vinatier, I.; et al. Assessing physicians’ and nurses’ experience of dying and death in the ICU: Development of the CAESAR-P and the CAESAR-N instruments. Crit. Care 2020, 24. [Google Scholar] [CrossRef]
- Han, S.K.; Eo, Y. Patients’ Dying Process from the Point of View of Family and Hospice Team: A Qualitative Exploration of Family Member and Hospice Team Experiences with Hospice in Korea. OMEGA-J. Death Dying 2020, 0030222820976428. [Google Scholar] [CrossRef]
- Gerritsen, R.T.; Hofhuis, J.G.; Koopmans, M.; van der Woude, M.; Bormans, L.; Hovingh, A.; Spronk, P.E. Perception by family members and ICU staff of the quality of dying and death in the ICU: A prospective multicenter study in The Netherlands. Chest 2013, 143, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, R.T.; Koopmans, M.; Hofhuis, J.G.; Curtis, J.R.; Jensen, H.I.; Zijlstra, J.G.; Engelberg, R.A.; Spronk, P.E. Comparing quality of dying and death perceived by family members and nurses for patients dying in US and Dutch ICUs. Chest 2017, 151, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Levy, C.R.; Wesley, E.; Payne, K.; Engelberg, R.A.; Patrick, D.L.; Curtis, J.R. Quality of dying and death in two medical ICUs: Perceptions of family and clinicians. Chest 2005, 127, 1775–1783. [Google Scholar] [CrossRef]
- Brinkman-Stoppelenburg, A.; Witkamp, F.E.; van Zuylen, L.; van der Rijt, C.C.; van der Heide, A. Palliative care team consultation and quality of death and dying in a university hospital: A secondary analysis of a prospective study. PLoS ONE 2018, 13, e0201191. [Google Scholar] [CrossRef]
- Guo, Q.; Jacelon, C.S. An integrative review of dignity in end-of-life care. Palliat. Med. 2014, 28, 931–940. [Google Scholar] [CrossRef]
- Ahmed, N.; Bestall, J.E.; Ahmedzai, S.H.; Payne, S.A.; Clark, D.; Noble, B. Systematic review of the problems and issues of accessing specialist palliative care by patients, careers and health and social care professionals. Palliat. Med. 2004, 18, 525–542. [Google Scholar] [CrossRef]
- Wentlandt, K.; Krzyzanowska, M.K.; Swami, N.; Rodin, G.M.; Le, L.W.; Zimmermann, C. Referral practices of oncologists to specialized palliative care. J. Clin. Oncol. 2012, 30, 4380–4386. [Google Scholar] [CrossRef]
- Hui, D.; Kim, S.H.; Roquemore, J.; Dev, R.; Chisholm, G.; Bruera, E. Impact of timing and setting of palliative care referral on quality of end-of-life care in cancer patients. Cancer 2014, 120, 1743–1749. [Google Scholar] [CrossRef]
- Jensen, H.I.; Halvorsen, K.; Jerpseth, H.; Fridh, I.; Lind, R. Practice Recommendations for End-of-Life Care in the Intensive Care Unit. Crit. Care Nurse 2020, 40, 14–22. [Google Scholar] [CrossRef]
- Cook, D.; Rocker, G. Dying with dignity in the intensive care unit. N. Engl. J. Med. 2014, 370, 2506–2514. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mean ± SD | Possible Score Range | |
|---|---|---|
| Total Quality of Dying and Death score | 39.12 ± 91.40 | 0–100 |
| Patient’s experiences at the end of life | ||
| Having pain under control | 5.23 ± 2.88 | 0–10 |
| Having control over what is going on around oneself | 3.51 ± 5.98 | 0–10 |
| Being able to feed oneself | 2.30 ± 3.16 | 0–10 |
| Being able to breathe comfortably | 3.72 ± 7.39 | 0–10 |
| Feeling at peace with dying | 3.58 ± 5.32 | 0–10 |
| Feeling unafraid of dying | 4.05 ± 0.23 | 0–10 |
| Being able to laugh and smile | 2.81 ± 8.14 | 0–10 |
| Keeping one’s dignity and self-respect | 3.19 ± 1.39 | 0–10 |
| Spending time with family, friends | 4.43 ± 4.51 | 0–10 |
| Spending time alone | 3.31 ± 3.00 | 0–10 |
| Being touched or hugged by loved ones | 5.58 ± 5.13 | 0–10 |
| Saying goodbye to loved ones | 4.02 ± 0.59 | 0–10 |
| Clearing up bad feelings | 3.22 ± 2.02 | 0–10 |
| Visits from a religious advisor | 5.17 ± 1.07 | 0–10 |
| Spiritual service before death | 4.86 ± 8.19 | 0–10 |
| Medical care at the end of life | ||
| Experience in receiving mechanical ventilation | 3.35 ± 3.51 | 0–10 |
| Experience of receiving dialysis | 3.11 ± 1.45 | 0–10 |
| Discussion with doctors about wishes | 3.34 ± 3.00 | 0–10 |
| Experience at the moment of death | ||
| Anyone present at the moment of death | 5.58 ± 5.01 | 0–10 |
| State at the moment of death | 3.88 ± 8.89 | 0–10 |
| PCCN | 53.27 ± 0.83 | 15–75 |
| Compassion | 13.35 ± 0.84 | 4–20 |
| Individuality | 13.86 ± 0.20 | 4–20 |
| Respect | 14.68 ± 0.72 | 4–20 |
| Comfort | 11.38 ± 0.15 | 3–15 |
| Overall quality of death | 6.13 ± 1.44 | 0–10 |
| QODD | PCCN | |||||
|---|---|---|---|---|---|---|
| N (%) | Mean ± SD | t or F (p) | Mean ± SD | t or F (p) | ||
| Received CPR within 48 h of death | Yes | 139 (46.3) | 34.83 ± 0.83 | −3.282 (0.001) | 53.46 ± 0.90 | 0.398 (0.691) |
| No | 161 (53.7) | 42.82 ± 1.25 | 53.10 ± 0.79 | |||
| Received sedative treatment while staying in ICU | Yes | 247 (82.3) | 40.51 ± 0.92 | 2.511 (0.013) | 53.68 ± 0.85 | 2.115 (0.035) |
| No | 41 (13.7) | 31.64 ± 0.98 | 50.88 ± 0.86 | |||
| Suspension of life-sustaining treatments | Yes | 125 (47.2) | 40.32 ± 0.32 | 1.631 (0.104) | 52.68 ± 0.12 | 0.039 (0.969) |
| No | 140 (52.8) | 36.16 ± 1.06 | 52.64 ± 0.29 | |||
| Patient consulted with doctor regarding the treatment at the end of life | Yes | 97 (32.3) | 46.83 ± 0.26 a | 10.111 (<0.001) a > b * a > c * | 55.21 ± 0.78 a | 5.250 (0.006) a > b * |
| No | 179 (59.7) | 35.81 ± 1.54 b | 52.10 ± 0.54 b | |||
| Not sure | 24 (8.0) | 32.60 ± 6.29 c | 54.13 ± 0.81 c | |||
| The reason for not suspending the life-sustaining treatments | Ethically impossible | 13 (9.3) | 26.61 ± 9.81 | 1.318 (0.267) | 49.15 ± 0.30 | 0.854 (0.493) |
| Insufficient legal grounds | 37 (26.4) | 38.28 ± 3.07 | 53.65 ± 0.27 | |||
| Refused by the family doctor | 10 (7.1) | 39.35 ± 3.61 | 53.70 ± 0.45 | |||
| Refused by the family | 77 (55.0) | 34.99 ± 9.53 | 52.49 ± 0.89 | |||
| Others | 3 (2.1) | 57.65 ± 6.84 | 55.67 ± 1.93 | |||
| QODD | PCCN | |||||
|---|---|---|---|---|---|---|
| N (%) | Mean ± SD | t (p) | Mean ± SD | t (p) | ||
| Gender | Male | 27 (9.0) | 41.45 ± 0.65 | 0.593 (0.554) | 54.74 ± 0.13 | 1.026 (0.306) |
| Female | 273 (91.0) | 38.88 ± 1.49 | 53.12 ± 0.80 | |||
| Duration of service in ICU | 6 months—less than 1 year | 13 (4.3) | 46.35 ± 8.06 | 0.892 (0.411) | 51.46 ± 0.99 | 0.468 (0.627) |
| 1 year—less than 3 years | 90 (30.0) | 39.69 ± 0.13 | 53.67 ± 0.63 | |||
| 3 years or more | 197 (65.7) | 38.37 ± 2.14 | 53.20 ± 0.04 | |||
| Religion | Catholic | 47 (15.7) | 37.97 ± 9.97 | 1.047 (0.372) | 54.91 ± 0.60 | 1.573 (0.196) |
| Christian | 82 (27.3) | 42.24 ± 3.34 | 53.85 ± 0.32 | |||
| Buddhist | 11 (3.7) | 43.28 ± 9.82 | 54.36 ± 0.20 | |||
| None | 160 (53.3) | 37.56 ± 0.84 | 52.41 ± 0.68 | |||
| Education level | Bachelor’s | 251 (83.7) | 39.14 ± 1.35 | 0.365 (0.695) | 53.08 ± 0.80 | 0.731 (0.482) |
| Master’s | 46 (15.3) | 38.31 ± 2.33 | 53.98 ± 0.14 | |||
| Doctorate | 3 (1.0) | 49.20 ± 0.20 | 57.67 ± 0.73 | |||
| Received specialized training for caring for the terminally ill after graduation | None | 164 (54.7) | 37.60 ± 1.55 | 1.302 (0.274) | 52.19 ± 0.61 | 1.417 (0.238) |
| One-time training | 36 (12.0) | 38.52 ± 2.75 | 54.11 ± 0.04 | |||
| Less than 6 h of training | 64 (21.3) | 45.25 ± 0.85 | 55.11 ± 0.61 | |||
| More than 6 h of training (n = 36, 12.0%) | 36 (12.0) | 39.90 ± 0.35 | 51.95 ± 0.47 | |||
| Variables | QODD | PCCN | Overall Quality of Death and Dying |
|---|---|---|---|
| r (p) | |||
| QODD | 1 | 0.296 (<0.001) | 0.306 (<0.001) |
| PCCN | 0.296 (<0.001) | 1 | 0.131 (0.023) |
| Overall quality of death and dying | 0.306 (<0.001) | 0.131 (0.023) | 1 |
| Variables | B | S.E | β | t | p | Adj R2 | F (p) |
|---|---|---|---|---|---|---|---|
| Constant | 12.036 | 10.828 | 1.112 | 0.267 | 0.16 | 9.345 (<0.001) | |
| Age (years) | −0.273 | 0.215 | −0.068 | −1.265 | 0.207 | ||
| Received sedative treatment (No) | −5.447 | 3.361 | −0.088 | −1.621 | 0.106 | ||
| Received sedative treatment (Not sure) | −4.281 | 5.800 | −0.039 | −0.738 | 0.461 | ||
| Patient consulted with a doctor regarding the treatment at the end of life (No) | −8.020 | 2.541 | −0.184 | −3.156 | 0.002 | ||
| Patient consulted with a doctor regarding the treatment at the end of life (Not sure) | −12.805 | 4.480 | −0.163 | −2.859 | 0.005 | ||
| Received CPR within 48 h of death (No) | 8.212 | 2.293 | 0.192 | 3.581 | <0.001 | ||
| PCCN | 0.714 | 0.148 | 0.261 | 4.829 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Choi, S.-H. Factors Associated with Quality of Dying and Death in Korean Intensive Care Units: Perceptions of Nurses. Healthcare 2021, 9, 40. https://doi.org/10.3390/healthcare9010040
Lee H, Choi S-H. Factors Associated with Quality of Dying and Death in Korean Intensive Care Units: Perceptions of Nurses. Healthcare. 2021; 9(1):40. https://doi.org/10.3390/healthcare9010040
Chicago/Turabian StyleLee, Haeyoung, and Seung-Hye Choi. 2021. "Factors Associated with Quality of Dying and Death in Korean Intensive Care Units: Perceptions of Nurses" Healthcare 9, no. 1: 40. https://doi.org/10.3390/healthcare9010040
APA StyleLee, H., & Choi, S.-H. (2021). Factors Associated with Quality of Dying and Death in Korean Intensive Care Units: Perceptions of Nurses. Healthcare, 9(1), 40. https://doi.org/10.3390/healthcare9010040