Systematic Review and Meta-Analysis of Incidence and Prevalence of Endometriosis

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
2.2. Methods of the Review
2.3. Data Extraction
2.4. Assessment for Risk of Bias
2.5. Statistical Analysis
3. Results
- Population-based integrated information systems (seven articles): including ambulatory and hospital discharge data that permit to calculate
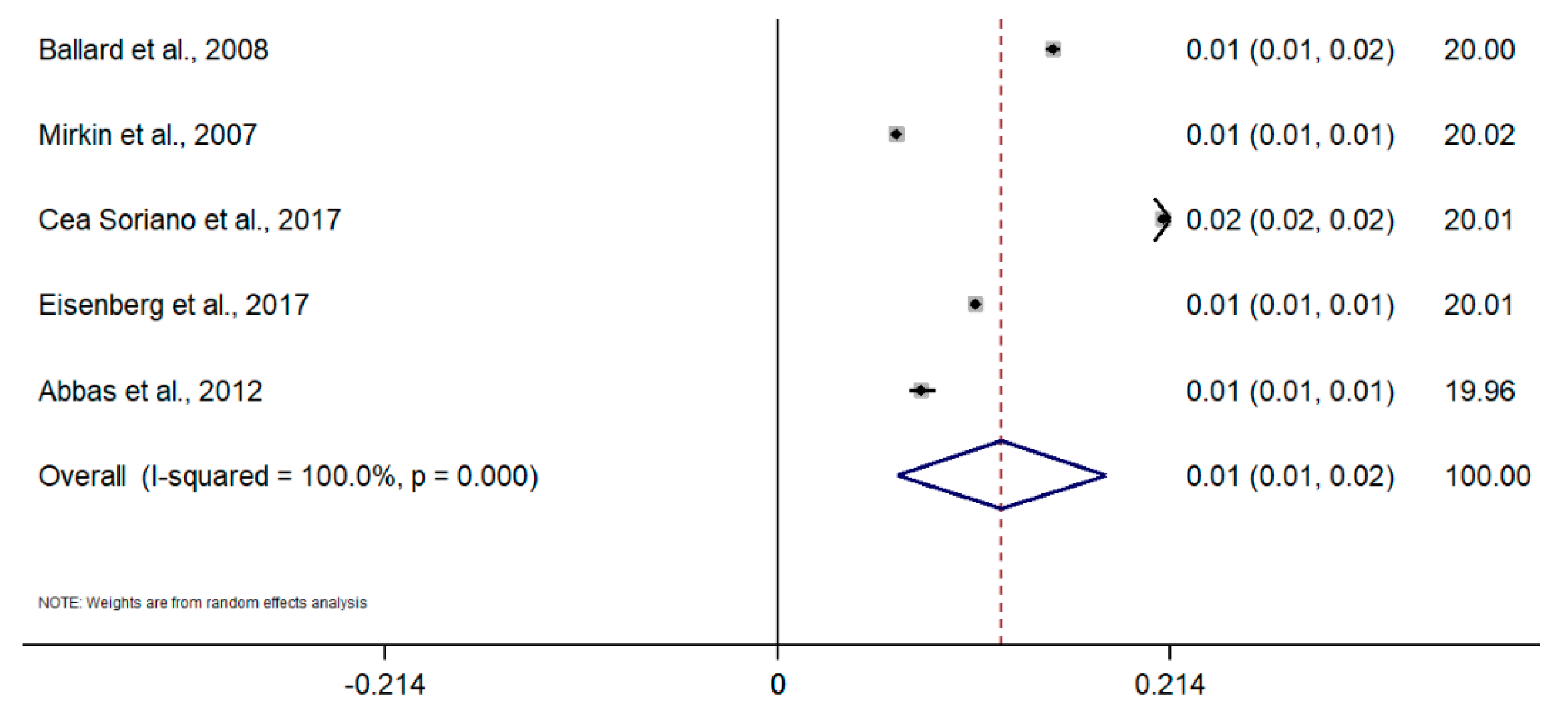
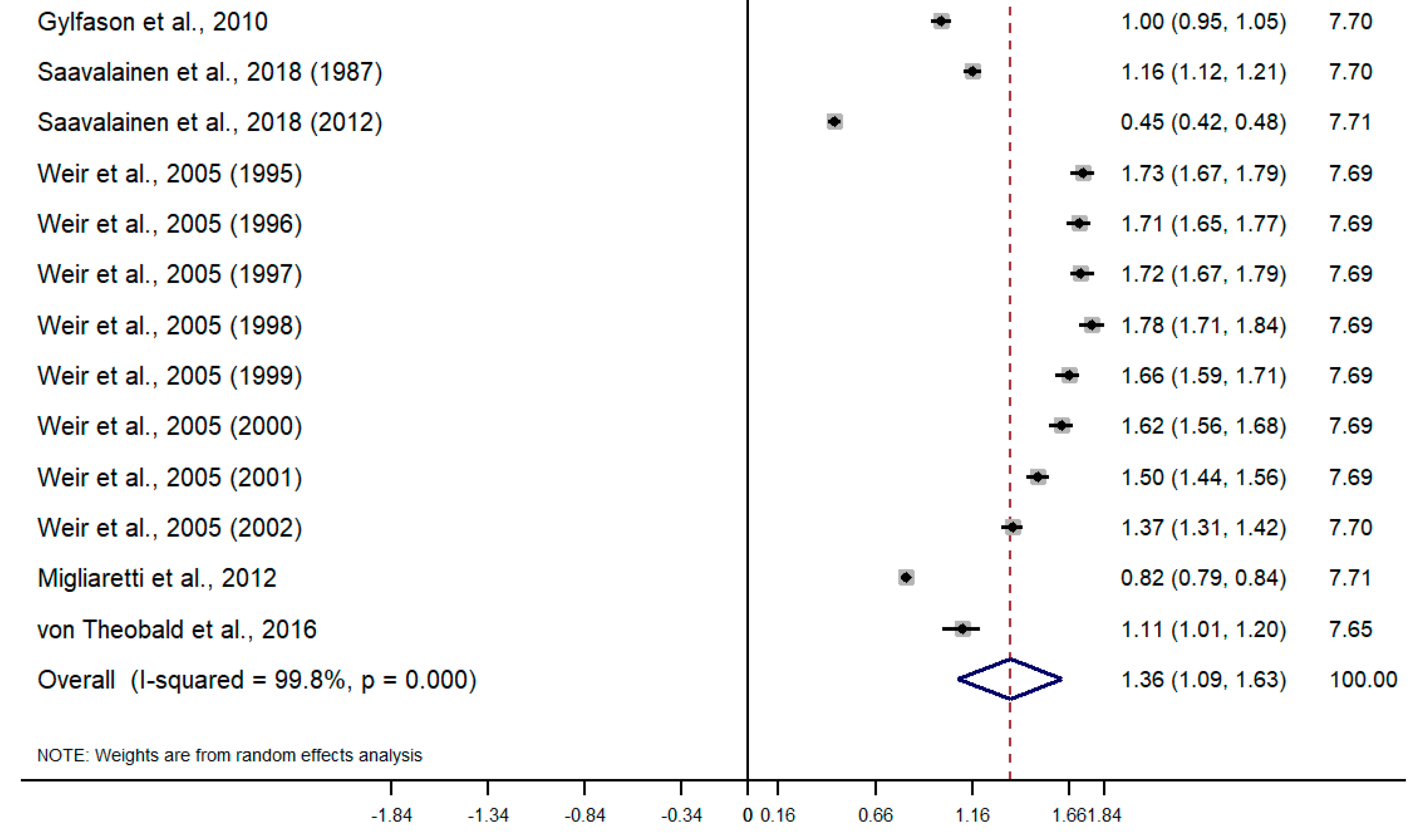
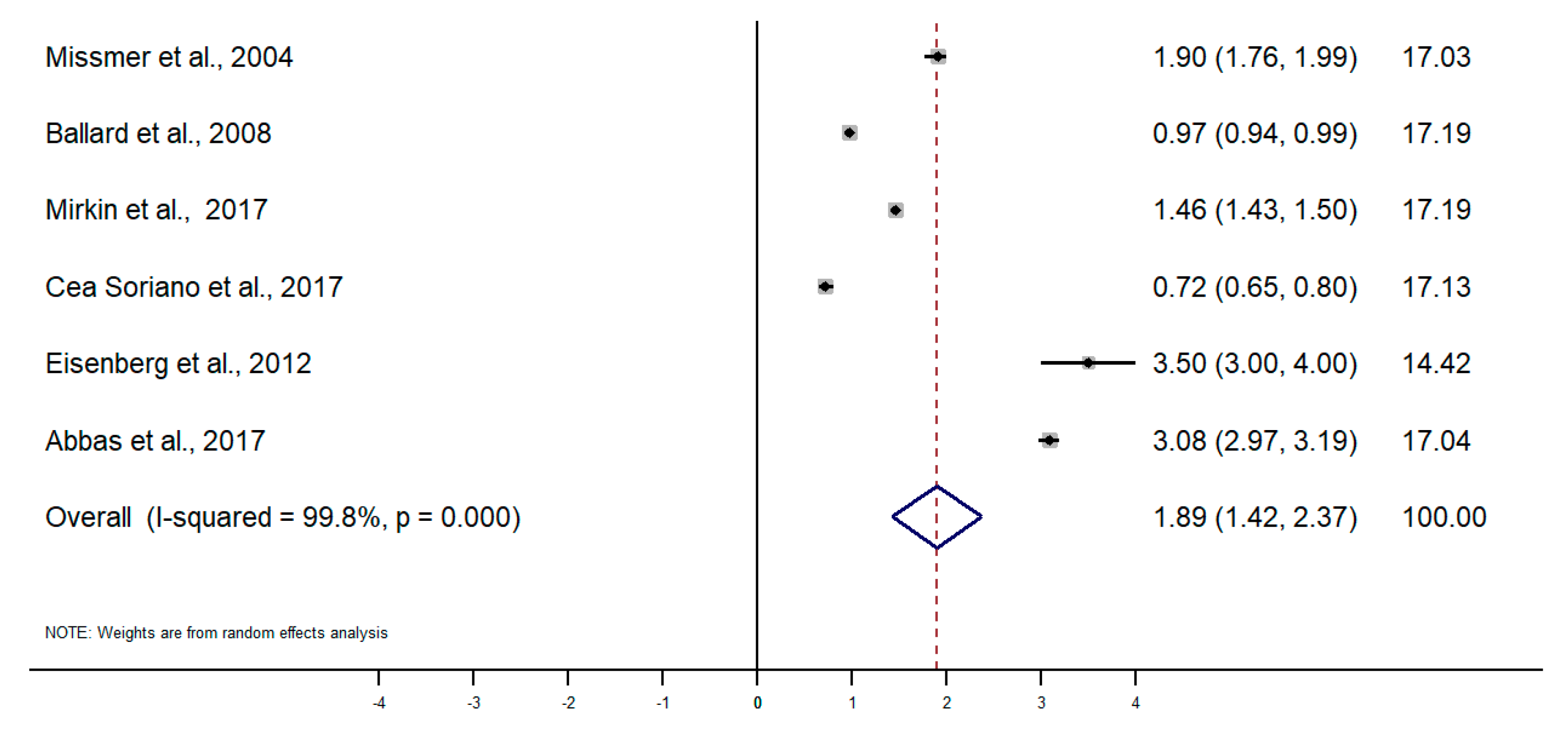
3.1. Pooled Prevalence and Incidence Rate of Endometriosis
3.2. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


References
- Zondervan, K.T.; Becker, C.M.; Missmer, S.A. Endometriosis. N. Engl. J. Med. 2020, 382. [Google Scholar] [CrossRef] [PubMed]
- As-Sanie, S.; Black, R.; Giudice, L.C.; Valbrun, T.G.; Gupta, J.; Jones, B.; Laufer, M.R.; Milspaw, A.T.; Missmer, S.A.; Norman, A. Assessing research gaps and unmet needs in endometriosis. Am. J. Obstet. Gynecol. 2019, 221, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Rokitansky, C.V. Ueber Uterusdrusen-Neubildung in Uterus and Ovariul Sarcomen; Carl Ueberreuter: Wien, Austria, 1860. [Google Scholar]
- Eskenazi, B.; Warner, M.L. Epidemiology of endometriosis. Obstet. Gynecol. Clin. N. Am. 1997, 24, 235–258. [Google Scholar] [CrossRef]
- Vessey, M.P.; Villard-Mackintosh, L.; Painter, R. Epidemiology of endometriosis in women attending family planning clinics. Br. Med. J. 1993, 306, 182–184. [Google Scholar] [CrossRef]
- Houston, D.E.; Noller, K.L.; MELTON III, L.J.; Selwyn, B.J.; Hardy, R.J. Incidence of pelvic endometriosis in Rochester, Minnesota, 1970–1979. Am. J. Epidemiol. 1987, 125, 959–969. [Google Scholar] [CrossRef]
- Kjerulff, K.H.; Erickson, B.A.; Langenberg, P.W. Chronic gynecological conditions reported by US women: Findings from the National Health Interview Survey, 1984 to 1992. Am. J. Public Health 1996, 86, 195–199. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Riitano, D.; Lisy, K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int. J. Health Policy Manag. 2014, 3, 123. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Moen, M.H.; Schei, B. Epidemiology of endometriosis in a Norwegian county. Acta Obstetricia et Gynecologica Scandinavica 1997, 76, 559–562. [Google Scholar] [CrossRef]
- Loving, S.; Thomsen, T.; Jaszczak, P.; Nordling, J. Female chronic pelvic pain is highly prevalent in Denmark. A cross-sectional population-based study with randomly selected participants. Scand. J. Pain 2014, 5, 93–101. [Google Scholar] [CrossRef]
- Fuldeore, M.J.; Soliman, A.M. Prevalence and symptomatic burden of diagnosed endometriosis in the United States: National estimates from a cross-sectional survey of 59,411 women. Gynecol. Obstet. Investig. 2017, 82, 453–461. [Google Scholar] [CrossRef]
- Fisher, C.; Adams, J.; Hickman, L.; Sibbritt, D. The use of complementary and alternative medicine by 7427 Australian women with cyclic perimenstrual pain and discomfort: A cross-sectional study. BMC Complementary Altern. Med. 2016, 16, 129. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.; Steel, A.; Wardle, J.; McIntyre, E.; Harnett, J.; Foley, H.; Adams, J. The prevalence of self-reported diagnosed endometriosis in the Australian population: Results from a nationally-representative survey. BMC Res. Notes 2019, 12, 1–6. [Google Scholar] [CrossRef]
- Flores, I.; Abreu, S.; Abac, S.; Fourquet, J.; Laboy, J.; Ríos-Bedoya, C. Self-reported prevalence of endometriosis and its symptoms among Puerto Rican women. Int. J. Gynecol. Obstet. 2008, 100, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Leibson, C.L.; Good, A.E.; Hass, S.L.; Ransom, J.; Yawn, B.P.; O’Fallon, W.M.; Melton, L.J. Incidence and characterization of diagnosed endometriosis in a geographically defined population. Fertil. Steril. 2004, 82, 314–321. [Google Scholar] [CrossRef]
- Gao, M.; Allebeck, P.; Mishra, G.D.; Koupil, I. Developmental origins of endometriosis: A Swedish cohort study. J. Epidemiol. Community Health 2019, 73, 353–359. [Google Scholar] [CrossRef]
- Yasui, T.; Hayashi, K.; Nagai, K.; Mizunuma, H.; Kubota, T.; Lee, J.-S.; Suzuki, S. Risk profiles for endometriosis in Japanese women: Results from a repeated survey of self-reports. J. Epidemiol. 2015, 25, 194–203. [Google Scholar] [CrossRef]
- Kvaskoff, M.; Han, J.; Qureshi, A.A.; Missmer, S.A. Pigmentary traits, family history of melanoma and the risk of endometriosis: A cohort study of US women. Int. J. Epidemiol. 2014, 43, 255–263. [Google Scholar] [CrossRef]
- Missmer, S.A.; Hankinson, S.E.; Spiegelman, D.; Barbieri, R.L.; Marshall, L.M.; Hunter, D.J. Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. Am. J. Epidemiol. 2004, 160, 784–796. [Google Scholar] [CrossRef]
- Ballard, K.D.; Seaman, H.E.; de Vries, C.S.; Wright, J.T. Can symptomatology help in the diagnosis of endometriosis? Findings from a national case–control study—Part 1. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 1382–1391. [Google Scholar] [CrossRef]
- Cea Soriano, L.; López-Garcia, E.; Schulze-Rath, R.; Garcia Rodríguez, L.A. Incidence, treatment and recurrence of endometriosis in a UK-based population analysis using data from The Health Improvement Network and the Hospital Episode Statistics database. Eur. J. Contracept. Reprod. Health Care 2017, 22, 334–343. [Google Scholar] [CrossRef]
- Eisenberg, V.H.; Weil, C.; Chodick, G.; Shalev, V. Epidemiology of endometriosis: A large population-based database study from a healthcare provider with 2 million members. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Abbas, S.; Ihle, P.; Köster, I.; Schubert, I. Prevalence and incidence of diagnosed endometriosis and risk of endometriosis in patients with endometriosis-related symptoms: Findings from a statutory health insurance-based cohort in Germany. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 160, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Stahlman, S.; Williams, V.F.; Taubman, S.B. Incidence and burden of gynecologic disorders, active component service women, US Armed Forces, 2012–2016. MSMR 2017, 24, 30–38. [Google Scholar] [PubMed]
- Mirkin, D.; Murphy-Barron, C.; Iwasaki, K. Actuarial analysis of private payer administrative claims data for women with endometriosis. J. Manag. Care Pharm. 2007, 13, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Gylfason, J.T.; Kristjansson, K.A.; Sverrisdottir, G.; Jonsdottir, K.; Rafnsson, V.; Geirsson, R.T. Pelvic endometriosis diagnosed in an entire nation over 20 years. Am. J. Epidemiol. 2010, 172, 237–243. [Google Scholar] [CrossRef]
- Saavalainen, L.; Lassus, H.; But, A.; Tiitinen, A.; Härkki, P.; Gissler, M.; Heikinheimo, O.; Pukkala, E. A Nationwide Cohort Study on the risk of non-gynecological cancers in women with surgically verified endometriosis. Int. J. Cancer 2018, 143, 2725–2731. [Google Scholar] [CrossRef]
- Weir, E.; Mustard, C.; Cohen, M.; Kung, R. Endometriosis: What is the risk of hospital admission, readmission, and major surgical intervention? J. Minim. Invasive Gynecol. 2005, 12, 486–493. [Google Scholar] [CrossRef]
- Migliaretti, G.; Deltetto, F.; Delpiano, E.M.; Bonino, L.; Berchialla, P.; Dalmasso, P.; Cavallo, F.; Camanni, M. Spatial analysis of the distribution of endometriosis in northwestern Italy. Gynecol. Obstet. Investig. 2012, 73, 135–140. [Google Scholar] [CrossRef]
- von Théobald, P.; Cottenet, J.; Iacobelli, S.; Quantin, C. Epidemiology of endometriosis in France: A large, nation-wide study based on hospital discharge data. BioMed Res. Int. 2016. [Google Scholar] [CrossRef]
- Morassutto, C.; Monasta, L.; Ricci, G.; Barbone, F.; Ronfani, L. Incidence and estimated prevalence of endometriosis and adenomyosis in Northeast Italy: A data linkage study. PLoS ONE 2016, 11, e0154227. [Google Scholar] [CrossRef]
- Louis, G.M.B.; Hediger, M.L.; Peterson, C.M.; Croughan, M.; Sundaram, R.; Stanford, J.; Chen, Z.; Fujimoto, V.Y.; Varner, M.W.; Trumble, A. Incidence of endometriosis by study population and diagnostic method: The ENDO study. Fertil. Steril. 2011, 96, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, S.; Arena, E.; Morando, A.; Remorgida, V. Prevalence of newly diagnosed endometriosis in women attending the general practitioner. Int. J. Gynecol. Obstet. 2010, 110, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.Y.; Grajewski, B.; Lawson, C.C.; Whelan, E.A.; Bertke, S.J.; Tseng, C.-Y. Occupational risk factors for endometriosis in a cohort of flight attendants. Scand. J. Work Environ. Health 2016, 42, 52. [Google Scholar] [CrossRef][Green Version]
- Eskenazi, B.; Mocarelli, P.; Warner, M.; Samuels, S.; Vercellini, P.; Olive, D.; Needham, L.L.; Patterson Jr, D.G.; Brambilla, P.; Gavoni, N. Serum dioxin concentrations and endometriosis: A cohort study in Seveso, Italy. Environ. Health Perspect. 2002, 110, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Stratton, P.; Winkel, C.; Premkumar, A.; Chow, C.; Wilson, J.; Hearns-Stokes, R.; Heo, S.; Merino, M.; Nieman, L.K. Diagnostic accuracy of laparoscopy, magnetic resonance imaging, and histopathologic examination for the detection of endometriosis. Fertil. Steril. 2003, 79, 1078–1085. [Google Scholar] [CrossRef]
- Mounsey, A.; Wilgus, A.; Slawson, D.C. Diagnosis and management of endometriosis. Am. Family Phys. 2006, 74, 594–600. [Google Scholar]
- Taylor, H.S.; Adamson, G.D.; Diamond, M.P.; Goldstein, S.R.; Horne, A.W.; Missmer, S.A.; Snabes, M.C.; Surrey, E.; Taylor, R.N. An evidence-based approach to assessing surgical versus clinical diagnosis of symptomatic endometriosis. Int. J. Gynecol. Obstet. 2018, 142. [Google Scholar] [CrossRef]
- Kuznetsov, L.; Dworzynski, K.; Davies, M.; Overton, C. Diagnosis and management of endometriosis: Summary of NICE guidance. BMJ 2017. [Google Scholar] [CrossRef]
- Saha, R.; Marions, L.; Tornvall, P. Validity of self-reported endometriosis and endometriosis-related questions in a Swedish female twin cohort. Fertil. Steril. 2017, 107. [Google Scholar] [CrossRef]
- Surrey, E.; Soliman, A.M.; Trenz, H.; Blauer-Peterson, C.; Sluis, A. Impact of Endometriosis Diagnostic Delays on Healthcare Resource Utilization and Costs. Adv. Ther. 2020, 37. [Google Scholar] [CrossRef]
- Kvaskoff, M.; Mu, F.; Terry, K.L.; Harris, H.R.; Poole, E.M.; Farland, L.; Missmer, S.A. Endometriosis: A high-risk population for major chronic diseases? Hum. Reprod. Update 2015, 21, 500–516. [Google Scholar] [CrossRef] [PubMed]
- Ghai, V.; Jan, H.; Shakir, F.; Haines, P.; Kent, A. Diagnostic delay for superficial and deep endometriosis in the United Kingdom. J. Obstet. Gynaecol. 2020, 40. [Google Scholar] [CrossRef]
- Soliman, A.M.; Fuldeore, M.; Snabes, M.C. Factors Associated with Time to Endometriosis Diagnosis in the United States. J. Women’s Health 2017, 26. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, R.; Rowe, H.; Fisher, J. Managing endometriosis: A cross-sectional survey of women in Australia. J. Psychosom. Obstet. Gynecol. 2020. [Google Scholar] [CrossRef] [PubMed]
- van der Zanden, M.; Arens, M.W.J.; Braat, D.D.M.; Nelen, W.L.M.; Nap, A.W. Gynaecologists’ view on diagnostic delay and care performance in endometriosis in the Netherlands. Reprod. Biomed. Online 2018, 37. [Google Scholar] [CrossRef] [PubMed]
- Hudelist, G.; Fritzer, N.; Thomas, A.; Niehues, C.; Oppelt, P.; Haas, D.; Tammaa, A.; Salzer, H. Diagnostic delay for endometriosis in Austria and Germany: Causes and possible consequences. Hum. Reprod. 2012, 27. [Google Scholar] [CrossRef] [PubMed]
- Han, X.T.; Guo, H.Y.; Kong, D.L.; Han, J.S.; Zhang, L.F. Analysis of characteristics and influence factors of diagnostic delay of endometriosis. Zhonghua fu chan ke za zhi 2018, 53, 92–98. [Google Scholar]
- Sirohi, D.; Al Ramadhani, R.; Knibbs, L.D. Environmental exposures to endocrine disrupting chemicals (EDCs) and their role in endometriosis: A systematic literature review. Rev. Environ. Health 2020. [Google Scholar] [CrossRef]
- Upson, K. Environmental Risk Factors for Endometriosis: A Critical Evaluation of Studies and Recommendations from the Epidemiologic Perspective. Curr. Epidemiol. Rep. 2020, 7. [Google Scholar] [CrossRef]
- Olšarová, K.; Mishra, G.D. Early life factors for endometriosis: A systematic review. Hum. Reprod. Update 2020, 26. [Google Scholar] [CrossRef]
- Murvoll, K.M.; Skaare, J.U.; Jensen, H.; Jenssen, B.M. Associations between persistent organic pollutants and vitamin status in Brünnich’s guillemot and common eider hatchlings. Sci. Total Environ. 2007, 381. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Gong, T.-T.; Wang, H.-Y.; Zhao, Y.-H.; Wu, Q.-J. Global, regional, and national endometriosis trends from 1990 to 2017. Ann. N. Y. Acad. Sci. 2020. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Ussia, A.; Adamyan, L.; Tahlak, M.; Keckstein, J.; Wattiez, A.; Martin, D.C. The epidemiology of endometriosis is poorly known as the pathophysiology and diagnosis are unclear. Best Pract. Res. Clin. Obstet. Gynaecol. 2020. [Google Scholar] [CrossRef] [PubMed]
- De Ziegler, D.; Borghese, B.; Chapron, C. Endometriosis and infertility: Pathophysiology and management. Lancet 2010, 376, 730–738. [Google Scholar] [CrossRef]
- Bulletti, C.; Coccia, M.E.; Battistoni, S.; Borini, A. Endometriosis and infertility. J. Assist. Reprod. Genet. 2010, 27. [Google Scholar] [CrossRef] [PubMed]
- D Hooghe, T.M.; Debrock, S.; Hill, J.A.; Meuleman, C. Endometriosis and Subfertility: Is the Relationship Resolved? Semin. Reprod. Med. 2003, 21. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Years of Follow up | Setting | Population of Reference | Age | Source of Information | Method of Diagnosis | Prevalence | Incidence |
|---|---|---|---|---|---|---|---|---|
| Moen and Schei, 1997 [10] | 1992–1993 | Sor-Trondelag, Norway | 5139 invited, 4089 (79.6%) participating, 4034 (78.5%) returned the questionnaire | 42–44 | Questionnaire sent to women as part of a cardiovascular risk prevention program | Self-reported | 2.2% | 0.30% |
| Loving et al., 2014 [11] | 2010–2011 | Denmark | 2500 (response rate of 48%) | ≥18 | Questionnaire sent by mail as part of a study on chronic pelvic pain | Self-reported | 8% | |
| Fuldeore and Soliman, 2017 [12] | 2012 | USA | 59,411 contacted 48,020 responded (response rate of 15.5%) | 18–49 | Questionnaire sent by email to 3 panels | Self-reported | 6.1% | |
| Fisher et al., 2016 [13] | 2012 | Australia | 7427 | 34–39 | Australian Longitudinal Study of Women’s Health | Self-reported | 3.7% | |
| Reid et al., 2019 [14] | 2017 | Australia | 652 | 18–49 | Questionnaire sent to a panel | Self-reported in the last 3 year | 3.4% | |
| Flores et al., 2008 [15] | Puerto Rico | 1285 (response rate of 93%) | Questionnaire in specific places | Self-reported | 4% |
| Article | Years of Follow up | Setting | Population of Reference | Age | Source of Information | Method of Diagnosis | Incidence |
|---|---|---|---|---|---|---|---|
| Leibson et al., 2004 [16] | 1989–1999 | USA | 726,205 women-year | Nurses’ Health Study II | Review of clinical reports of self-reported cases | 237/100,000 women-year | |
| Gao et al., 2019 [17] | 1996–2008 | Uppsala, Sweden | 4429 identified 3476 with obstetric record 3406 included | Born 1933–1972 | Uppsala Birth Cohort Multigenerational Study and a national registry of hospital discharges | Diagnostic codes | 1.08 per 1000 women-year |
| Yasui et al., 2015 [18] | 2001–2012 | Japan | 15,019 | Japan Nurses’ Health Study | Questionnaire sent to women that have reported endometriosis: confirmed with image or surgery | 6.8% 1025 reported, 862 responded to the questionnaire, 638 diagnoses confirmed
| |
| Kvaskoff et al., 2014 [19] | 1989 | USA | A cohort of 116,430 female US nurses (response rate >90%) | 25–42 | Nurses’ Health Study II | Self-reported laparoscopically confirmed endometriosis | 3.9 per 1000 person-years |
| Article | Years of Follow up | Setting | Population of Reference | Age | Source of Information | Method of Diagnosis | Prevalence | Incidence |
|---|---|---|---|---|---|---|---|---|
| Missmer et al., 2004 [20] | 1987–1992 | County Olmsted, USA | ≥15 | Rochester Epidemiology Project | Diagnostic codes and review of medical records | 1.9 per 1000 women-year (85% surgical confirmation) | ||
| Ballard et al., 2008 [21] | 1992–2001 | UK | 15–55 | United Kingdom General Practice Research Database | Diagnostic codes from primary care and hospitals | 1.5% | 0.97/1000 women-year 0.77/1000 women-year with cases “definitive” and “probable” | |
| Mirkin et al., 2007 [26] | 1999–2003 | USA | 6,220,349 | 18–55 | Private insurance database | Diagnostic codes | 0.7% | |
| Cea Soriano et al., 2017 [22] | 2000–2010 | UK | 4,990,621 person-years | 12–54 | The Health Improvement Network and the Hospital Episode | Diagnostic codes and review of medical records | 2.1% | 1.5 per 1000 women-year |
| Eisenberg et al., 2018 [23] | 2000–2015 | Israel | 6146 | 15–55 | Private insurance database | Diagnostic codes | 10.8 per 1000 | 7.2 per 10,000 |
| Abbas et al., 2012 [24] | 2004–2008 | Hesse, Germany | Prevalence: 62,323 Incidence: 54,364 | 15–54 | Private insurance database | Diagnostic codes | 7.8 per 1000 | 3.5 per 1000 |
| Stahlman et al., 2017 [25] | 2012–2016 | USA | Women in active service Army, USAF, Navy y Marines | Electronic medical record of Defense Medical Surveillance System | Diagnostic codes | 30.8 per 10,000 women-year |
| Article | Years of Follow up | Setting | Population of Reference | Age | Source of Information | Method of Diagnosis | Incidence |
|---|---|---|---|---|---|---|---|
| Gylfason et al., 2010 [27] | 1981–2000 | Iceland | 1,303,815 | 15–49 | Hospital discharge registry | Diagnostic codes and review of medical records | Surgical confirmation: 10.0 histological: 5.7 10,000 women-year |
| Saavalainen et al., 2018 [28] | 1987–2012 | Finland | Women included in the Finnish Population Register Center | 10–84 | National hospital discharge registry | Diagnostic codes | 45–116 per 100,000 |
| Weir et al., 2005 [29] | 1994–2002 | Ontario, Canada | 15–70 | National hospital discharge registry | Diagnostic codes | 137–173 per 100,000 | |
| Migliaretti et al., 2012 [30] | 2000–2005 | Piamonte, Italia | 3929 | 18–45 | Regional hospital discharge registry | Diagnostic codes | 81.8 per 100,000 women-year |
| von Théobald et al., 2016 [31] | 2008–2012 | France | 14,239,197 | 15–49 | National hospital discharge registry | Diagnostic codes | 0.4–1.6% |
| Morassutto et al., 2016 [32] | 2011–2013 | Friuli Venezia Giulia, Italia | 807,050 without a diagnosis in the previous 10 years | 15–50 | Regional hospital discharge registry | Diagnostic codes and histological confirmation | 0.11% Histologically confirmed: 0.07% Prevalence: 1.14% |
| Article | Years of Follow up | Setting | Population of Reference | Age | Source of Information | Method of Diagnosis | Prevalence | Incidence |
|---|---|---|---|---|---|---|---|---|
| Louis et al., 2011 [33] | 2007–2009 | California, Utah, USA | 127 | 18–44 | Population controls | Image | 11% | |
| Ferrero et al., 2009 [34] | 2009 | Local general practitioner clinic, Italy | 1612 met inclusion criteria, 1291 were agreed to participate and complete questionnaire | Reproductive age <50 years | Questionnaire, medical records | Clinical exploration, surgery, image | 3.7% | |
| Johnson et al., 2016 [35] | 1999–2001 | Flight attendants and school teachers from Detroit, Miami, and Seattle | 1945 flight attendants and 236 school teachers | 18–45 | Reproductive health occupational assessment | Self-reported laparoscopic confirmed via telephone interview | 4.67% 3.38% | |
| Eskenazi et al., 2002 [36] | 20 years of follow up after the 1976 factory explosion in Italy | Seveso, Italy | 601 | Women who were ≤30 years old in 1976 | Retrospective cohort study | Surgically confirmed disease or an ultrasound consistent with endometriosis | 3.2% |
| # | Author, Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Total | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Moen and Schei, 1997 [10] | No | Yes | Yes | Yes | No | No | No | Yes | No | NA | 44.4% | High |
| 2 | Loving et al., 2014 [11] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | NA | 77.8% | Low |
| 3 | Fuldeore and Soliman, 2017 [12] | Yes | Yes | Yes | Yes | No | No | No | Yes | No | NA | 55.6% | Moderate |
| 4 | Fisher et al., 2016 [13] | No | Yes | Yes | Yes | No | No | No | Yes | No | NA | 44.4% | High |
| 5 | Reid et al., 2019 [14] | No | Yes | No | Yes | No | No | No | Yes | Yes | NA | 44.4% | High |
| 6 | Flores et al., 2008 [15] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | NA | 55.6% | Moderate |
| 7 | Ballard et al., 2008 [21] | Yes | NA | Yes | Yes | NA | Yes | Unclear | Yes | Yes | NA | 87.5% | Low |
| 8 | Cea Soriano et al., 2017 [22] | Yes | NA | Yes | No | NA | Yes | Yes | Yes | No | NA | 71.4% | Low |
| 9 | Eisenberg et al., 2018 [23] | Yes | NA | Yes | No | NA | Yes | Yes | Yes | No | NA | 71.4% | Low |
| 10 | Abbas et al., 2012 [24] | Yes | NA | Yes | Yes | NA | Yes | Yes | Yes | No | NA | 85.7% | Low |
| 11 | Mirkin et al., 2007 [26] | Yes | NA | Yes | No | NA | Yes | Yes | Yes | No | NA | 71.4% | Low |
| 12 | Ferrero et al., 2009 [34] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | NA | 88.9% | Low |
| 13 | Johnson et al., 2016 [35] | Yes | No | Yes | Yes | No | No | No | Yes | Yes | NA | 55.6% | Moderate |
| 14 | Eskenazi et al., 2002 [36] | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | NA | 88.9% | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarria-Santamera, A.; Orazumbekova, B.; Terzic, M.; Issanov, A.; Chaowen, C.; Asúnsolo-del-Barco, A. Systematic Review and Meta-Analysis of Incidence and Prevalence of Endometriosis. Healthcare 2021, 9, 29. https://doi.org/10.3390/healthcare9010029
Sarria-Santamera A, Orazumbekova B, Terzic M, Issanov A, Chaowen C, Asúnsolo-del-Barco A. Systematic Review and Meta-Analysis of Incidence and Prevalence of Endometriosis. Healthcare. 2021; 9(1):29. https://doi.org/10.3390/healthcare9010029
Chicago/Turabian StyleSarria-Santamera, Antonio, Binur Orazumbekova, Milan Terzic, Alpamys Issanov, Chen Chaowen, and Angel Asúnsolo-del-Barco. 2021. "Systematic Review and Meta-Analysis of Incidence and Prevalence of Endometriosis" Healthcare 9, no. 1: 29. https://doi.org/10.3390/healthcare9010029
APA StyleSarria-Santamera, A., Orazumbekova, B., Terzic, M., Issanov, A., Chaowen, C., & Asúnsolo-del-Barco, A. (2021). Systematic Review and Meta-Analysis of Incidence and Prevalence of Endometriosis. Healthcare, 9(1), 29. https://doi.org/10.3390/healthcare9010029