A Fast and Effective System for Analysis of Optokinetic Waveforms with a Low-Cost Eye Tracking Device


Abstract
1. Introduction
2. Materials and Methods
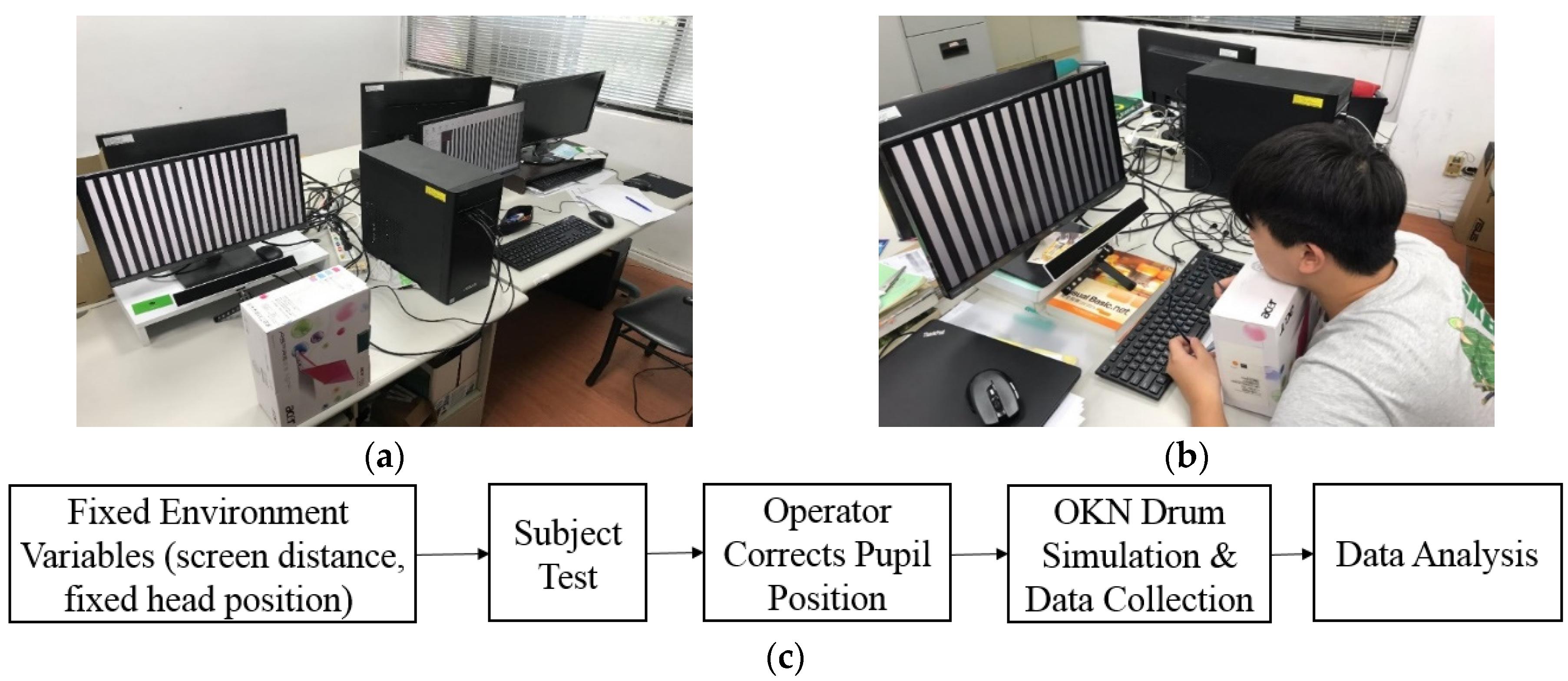
2.1. Materials
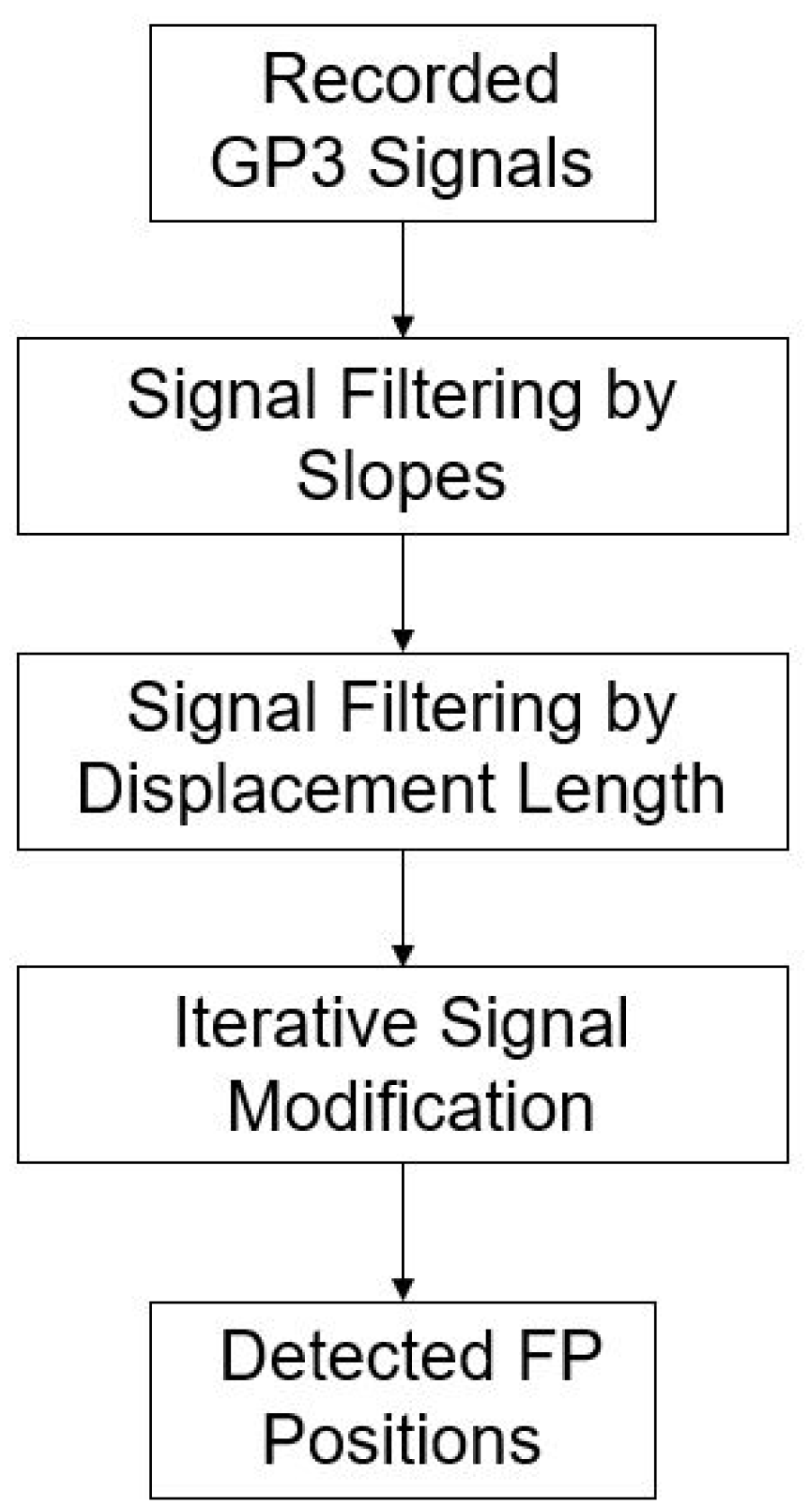
2.2. Proposed OKN Eye Movement Measure System
| Algorithm 1. Proposed FP position detection. | |
| 1 | for i = 1: length (I) |
| 2 | if (I’s slope meet S) |
| 3 | Put Up/Down point to matrix; |
| 3 | end |
| 4 | end |
| 5 | for j = 1: IC |
| 6 | for i = length(M) |
| 7 | gather points around peak (±1) |
| 9 | find maximum/minimum of points |
| 10 | end |
| 11 | end |
| I: | is the input data |
| S: | is the slope threshold |
| M: | is the matrix after select matching data from input |
| IC: | is the iteration Counts (interationCount), through multiple iterations, the signal identified as the FP interval gradually moves to the highest and lowest points of FP |
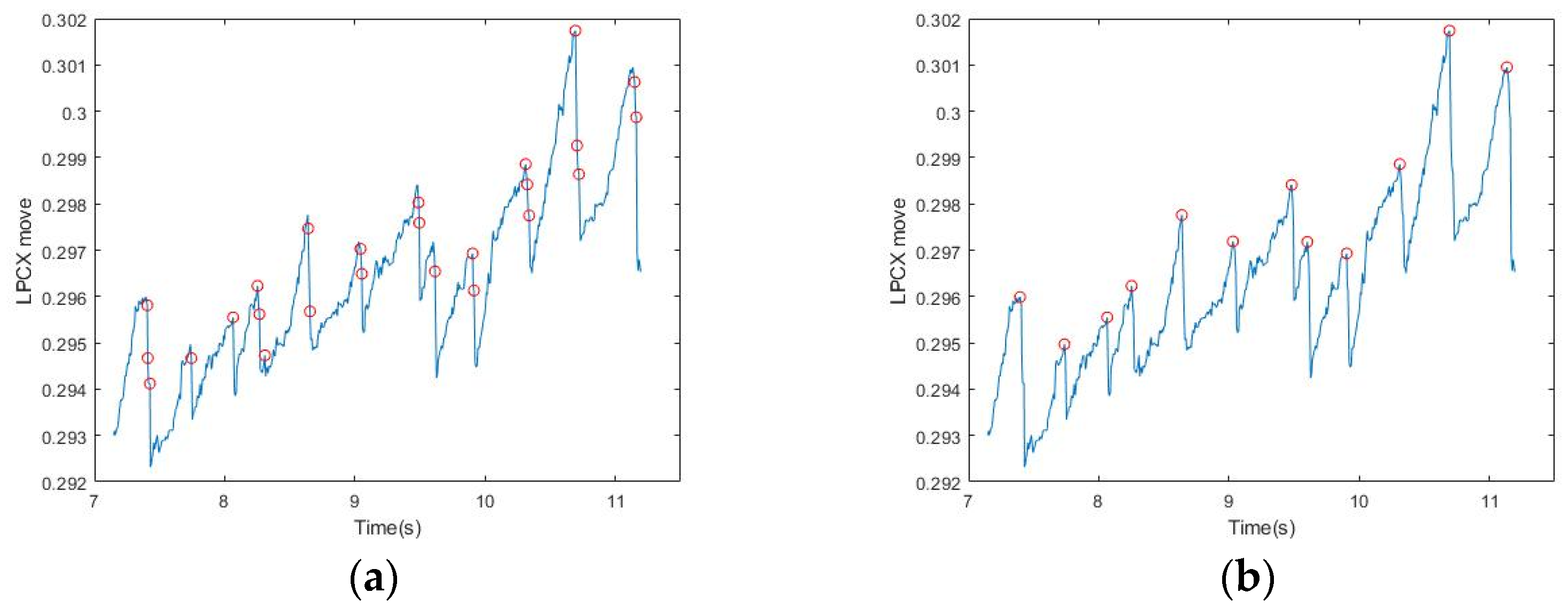
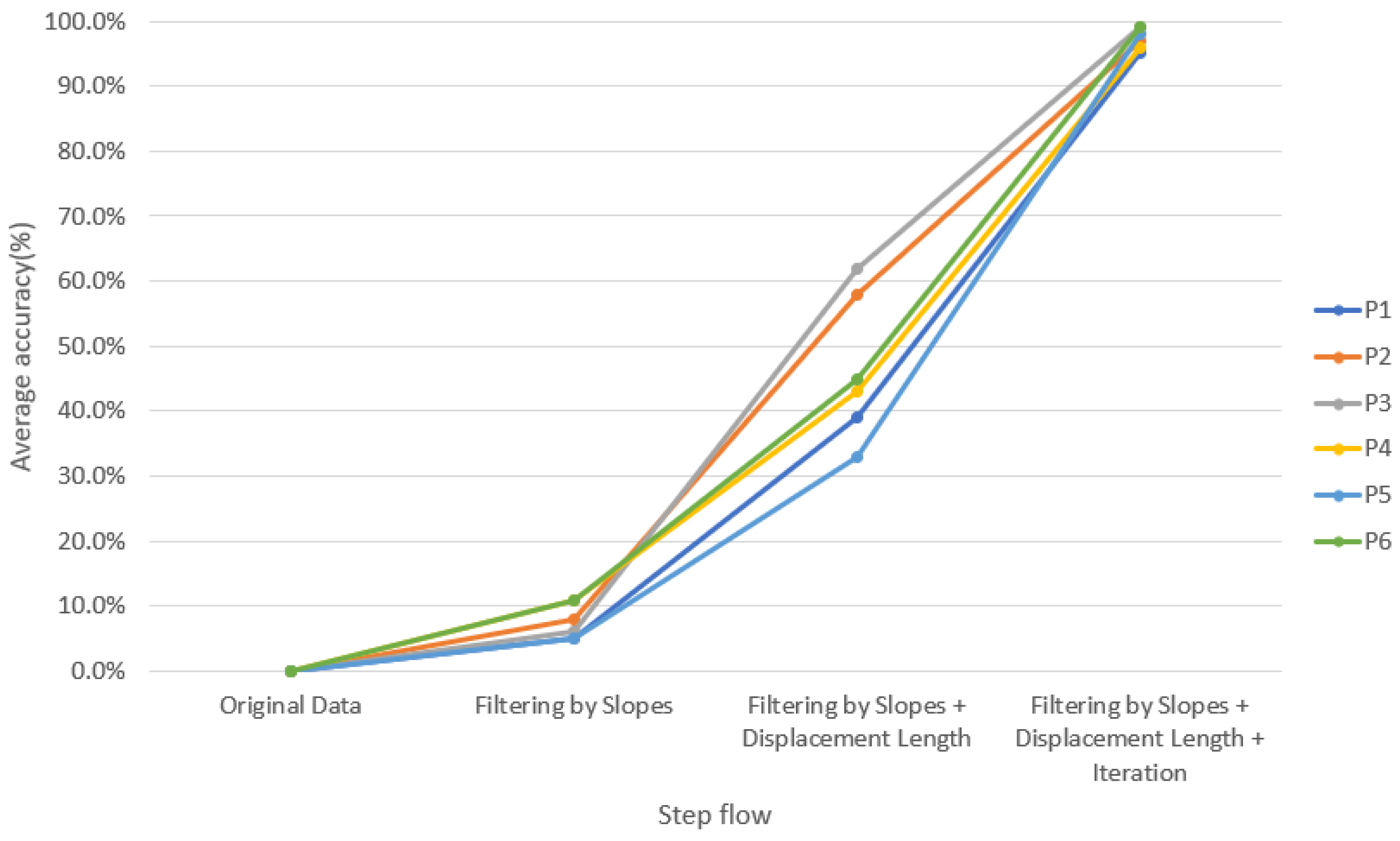
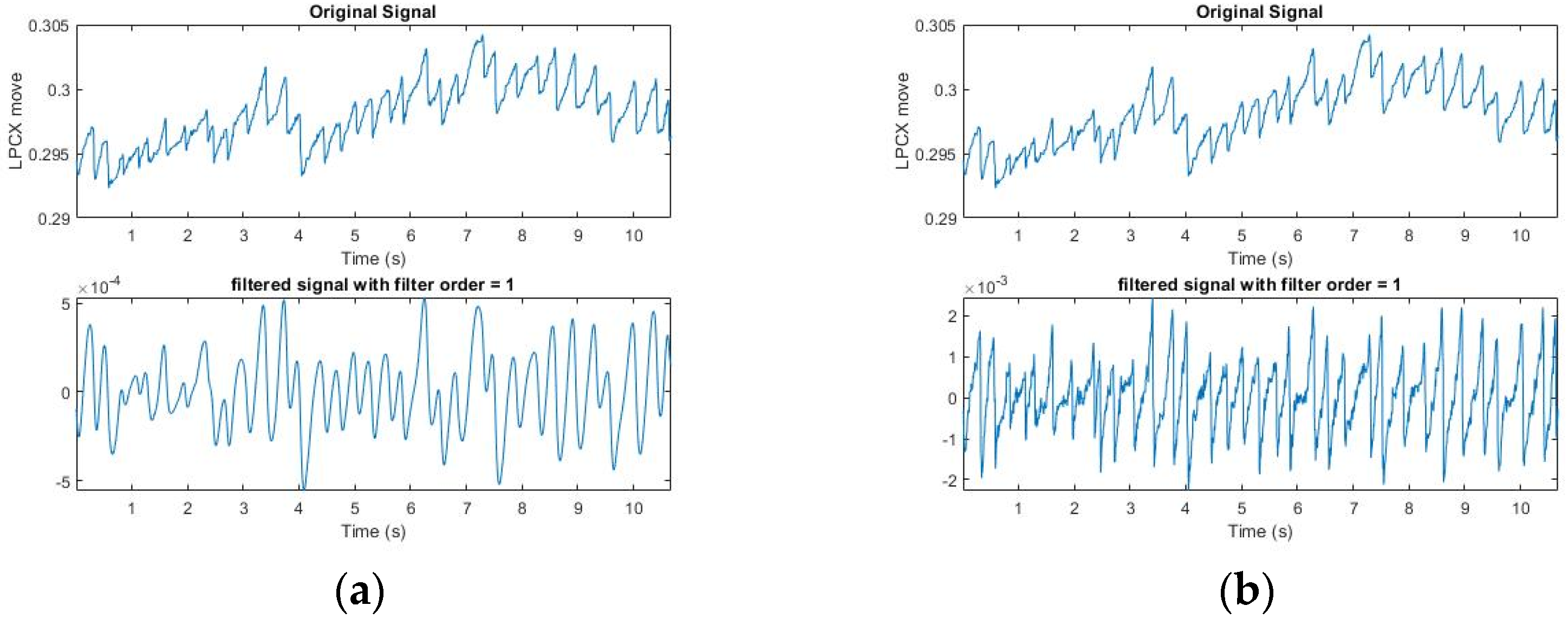
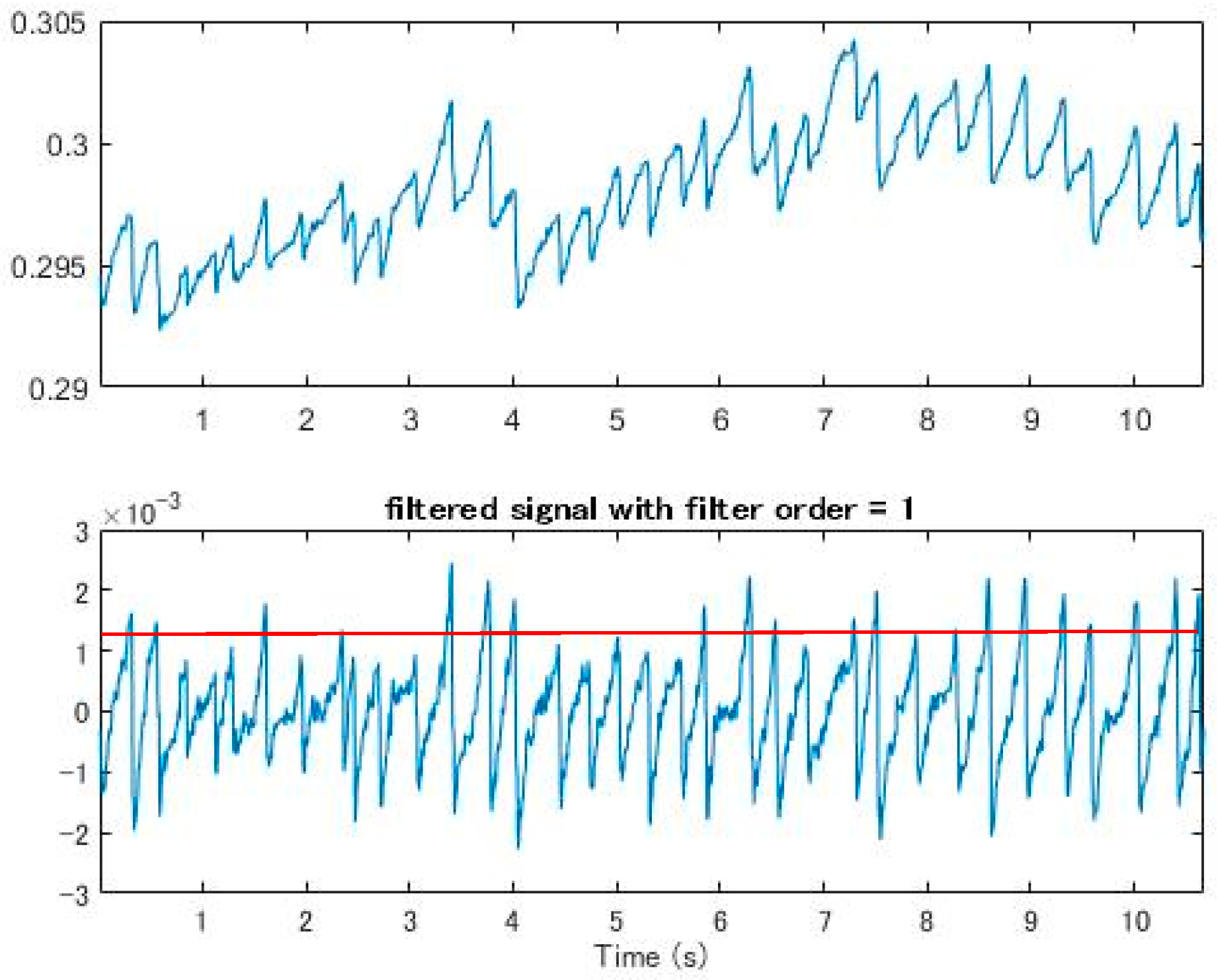
2.2.1. Signal Filtering by Slopes
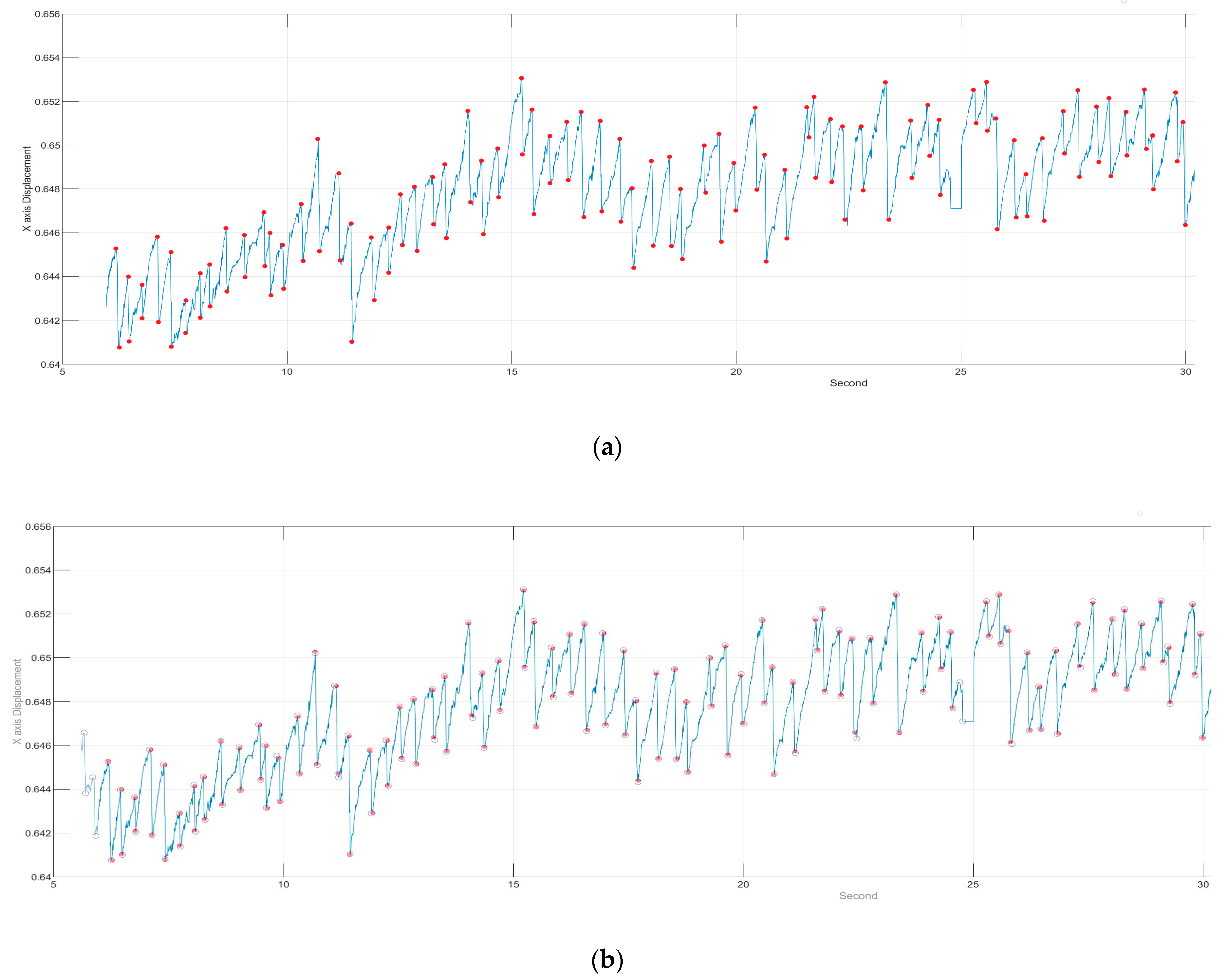
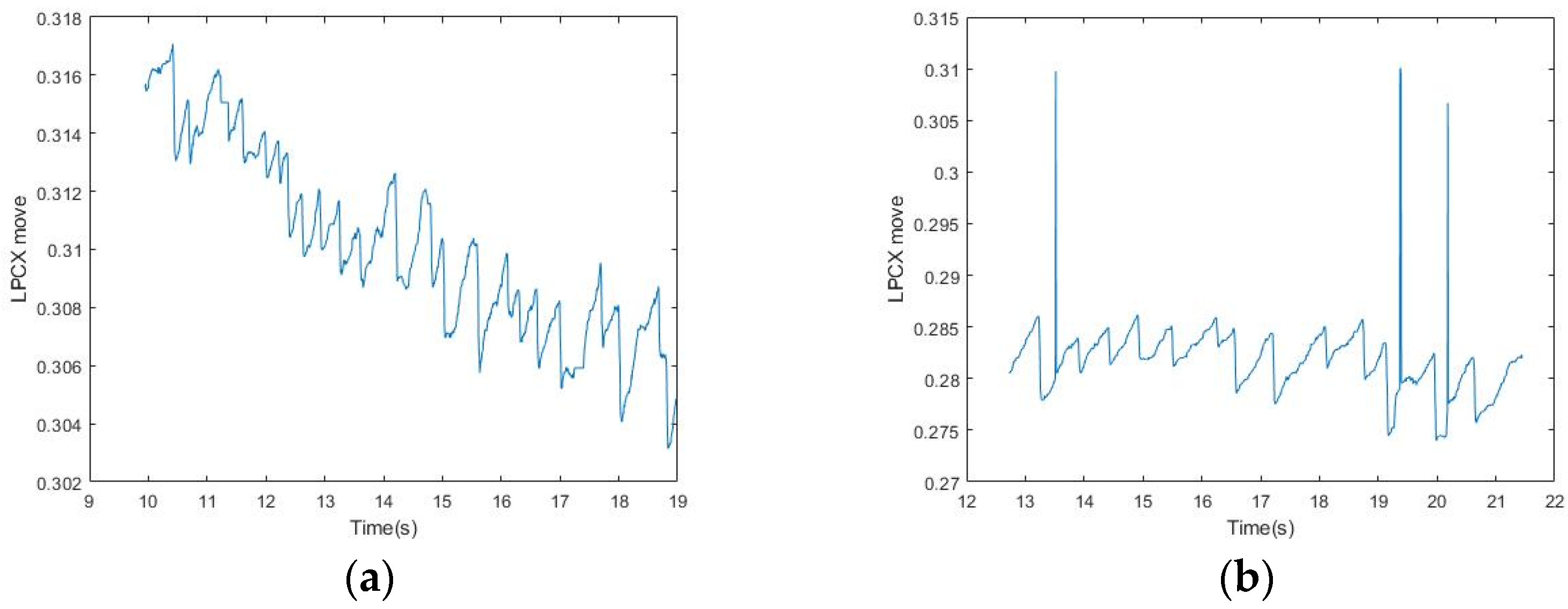
2.2.2. Signal Filtering by Displacement Length
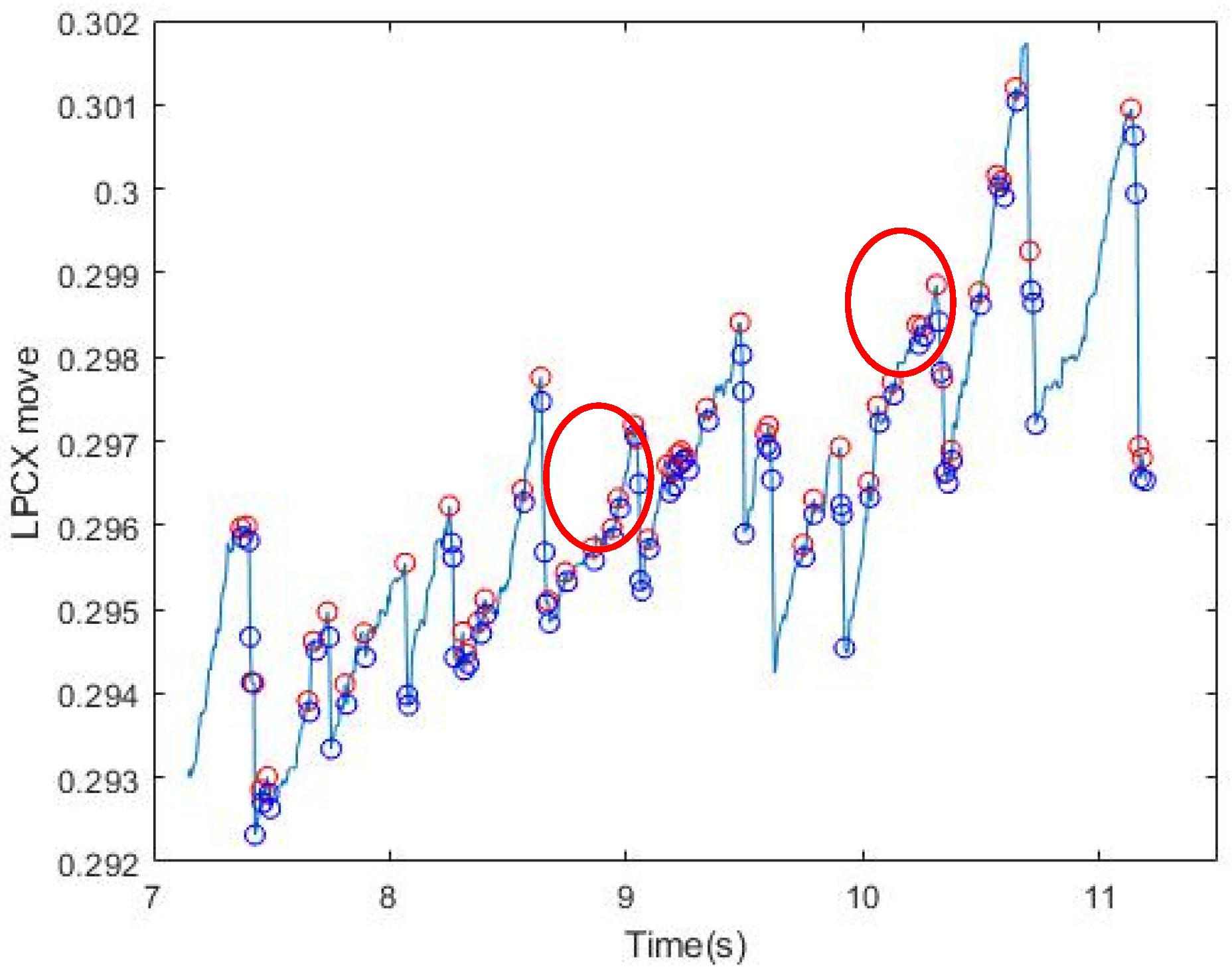
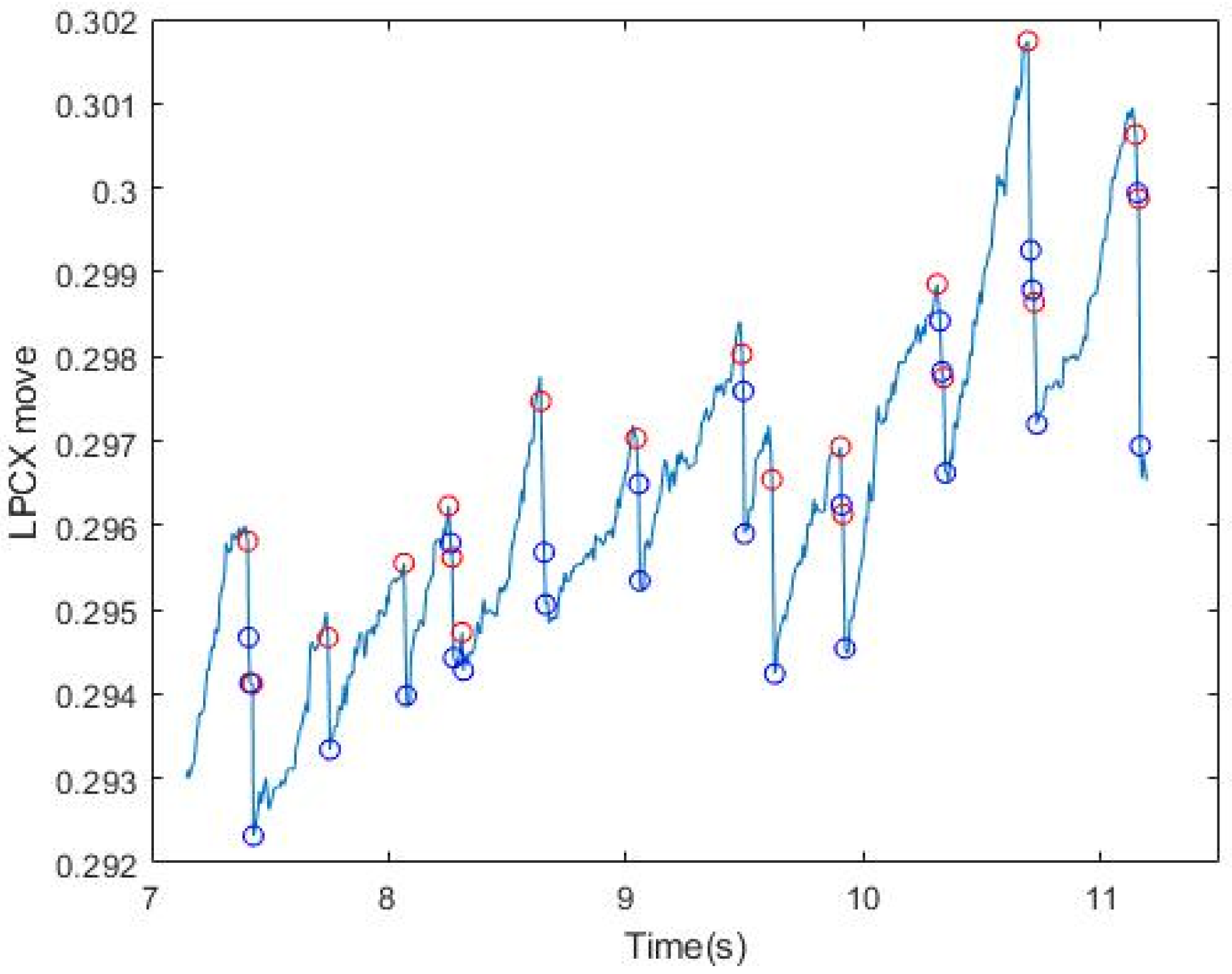
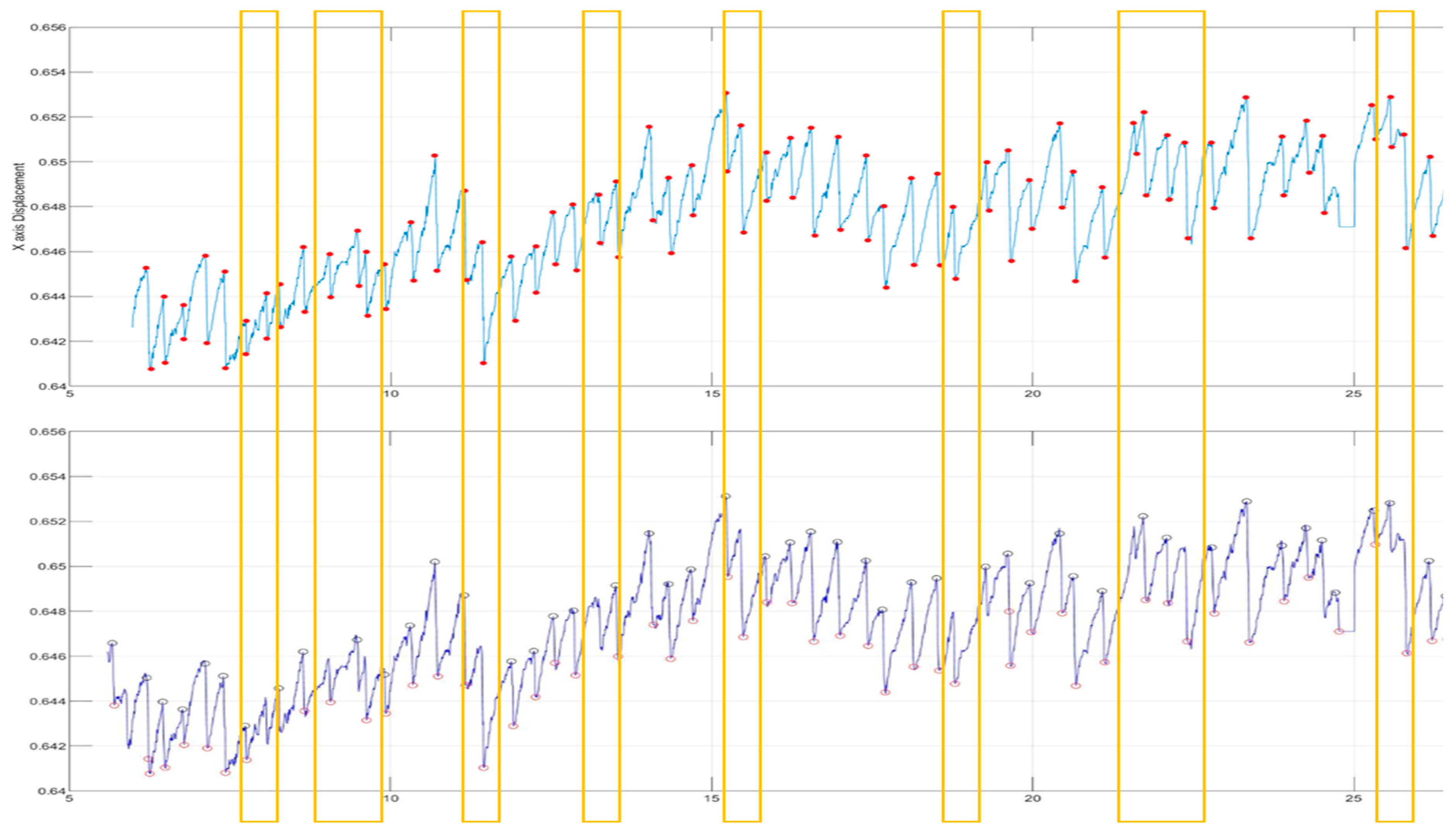
2.2.3. Iterative Signal Modification
3. Experimental Results and Discussion
3.1. Quantitative Measurement of Elicited OKN
3.2. Comparisons with the State-of-the-Art Approaches
3.3. Research Contributions and Limitations
4. Conclusions and Future Work
Author Contributions
Funding
Conflicts of Interest
References
- Wright, K.W. Clinical optokinetic nystagmus asymmetry in treated esotropes. J. Pediatr. Ophthalmol. Strabismus 1996, 33, 153–155. [Google Scholar] [PubMed]
- Hansen, D.W.; Ji, Q. In the Eye of the Beholder: A Survey of Models for Eyes and Gaze. IEEE Trans. Pattern Anal. Mach. Intell. 2010, 32, 478–500. [Google Scholar] [CrossRef] [PubMed]
- Sangi, M.; Thompson, B.; Turuwhenua, J. An Optokinetic Nystagmus Detection Method for Use with Young Children. IEEE J. Transl. Eng. Health Med. 2015, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Castro, F.L. Class I infrared eye blinking detector. Sens. Actuators A Phys. 2008, 148, 388–394. [Google Scholar] [CrossRef]
- Al-Rahayfeh, A.; Faezipour, M. Eye Tracking and Head Movement Detection: A State-of-Art Survey. IEEE J. Transl. Eng. Health Med. 2013, 1, 2100212. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Kolakowski, S.M.; Pelz, J.B. Using Structured Illumination to Enhance Video-Based Eye Tracking. In Proceedings of the 2007 IEEE International Conference on Image Processing, San Antonio, TX, USA, 16–19 September 2007. [Google Scholar]
- Kumar, D.; Dutta, A.; Das, A.; Lahiri, U. SmartEye: Developing a Novel Eye Tracking System for Quantitative Assessment of Oculomotor Abnormalities. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.; Hussain, A.J.; Kuru, K.; Alaskar, H. Pupil Localisation and Eye Centre Estimation Using Machine Learning and Computer Vision. Sensors 2020, 20, 3785. [Google Scholar] [CrossRef] [PubMed]
- Ehinger, B.V.; Groß, K.; Ibs, I.; König, P. A new comprehensive eye-tracking test battery concurrently evaluating the Pupil Labs glasses and the EyeLink 1000. PeerJ 2019, 7, e7086. [Google Scholar] [CrossRef] [PubMed]
- Baloh, R.W.; Yee, R.D.; Honrubia, V. Optokinetic nystagmus and parietal lobe lesions. Ann. Neurol. 1980, 7, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Pulaski, P.D.; Zee, D.S.; Robinson, D.A. The behavior of the vestibulo-ocular reflex at high velocities of head rotation. Brain Res. 1981, 222, 159–165. [Google Scholar] [CrossRef]
- Khan, W.; Kuru, K. An Intelligent System for Spoken Term Detection That Uses Belief Combination. IEEE Intell. Syst. 2017, 32, 70–79. [Google Scholar] [CrossRef]
- Keogh, E.; Ratanamahatana, C. Exact indexing of dynamic time warping. Knowl. Inf. Syst. 2005, 7, 358–386. [Google Scholar] [CrossRef]
- Yuan, Y.; Leung, C.-C.; Xie, L.; Chen, H.; Ma, B. Query-by-Example Speech Search Using Recurrent Neural Acoustic Word Embeddings with Temporal Context. IEEE Access 2019, 7, 67656–67665. [Google Scholar] [CrossRef]
- Pander, T.; Czabański, R.; Przybyła, T.; Pojda-Wilczek, D. An automatic saccadic eye movement detection in an optokinetic nystagmus signal. Biomed. Tech. Eng. 2014, 59, 529–543. [Google Scholar] [CrossRef] [PubMed]
- Swindal, J.C. The International encyclopedia of ethics. Choice Rev. Online 2013, 51, 51-0021. [Google Scholar] [CrossRef]
- Kanari, K.; Sakamoto, K.; Kaneko, H. Effect of visual attention on the properties of optokinetic nystagmus. PLoS ONE 2017, 12, e0175453. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, N.; Ni, S. Research on submarine signal detection method based on Welch algorithm. In Proceedings of the 2018 IEEE 4th Information Technology and Mechatronics Engineering Conference (ITOEC), Chongqing, China, 14–16 December 2018. [Google Scholar]
- Pasquariello, G.; Cesarelli, M.; Romano, M.; La Gatta, A.; Bifulco, P.; Fratini, A. Waveform type evaluation in congenital nystagmus. Comput. Methods Programs Biomed. 2010, 100, 49–58. [Google Scholar] [CrossRef] [PubMed]
- T.O.H. (toh@umd.edu). Peak Finding and Measurement. Available online: https://terpconnect.umd.edu/~toh/spectrum/PeakFindingandMeasurement.htm (accessed on 1 December 2020).
- Larrazabal, A.; Cena, C.G.; Martínez, C. Video-oculography eye tracking towards clinical applications: A review. Comput. Biol. Med. 2019, 108, 57–66. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Filtering by Slopes | |
|---|---|
| Subjects | Accuracy (%) |
| 1 | 0.05 |
| 2 | 0.08 |
| 3 | 0.06 |
| 4 | 0.11 |
| 5 | 0.05 |
| 6 | 0.11 |
| Filtering by Slopes and Displacement Length | |
|---|---|
| Subjects | Accuracy (%) |
| 1 | 0.39 |
| 2 | 0.58 |
| 3 | 0.62 |
| 4 | 0.43 |
| 5 | 0.33 |
| 6 | 0.45 |
| Iterative Signal Modification After the Previous Steps (Our Method) | |
|---|---|
| Subjects | Accuracy (%) |
| 1 | 0.95 |
| 2 | 0.97 |
| 3 | 0.99 |
| 4 | 0.96 |
| 5 | 0.98 |
| 6 | 0.99 |
| Average Accuracy (%) | |||
|---|---|---|---|
| Filtering by Slopes | Filtering by Slopes and Displacement Length | Our Method | |
| mean | 0.07 | 0.47 | 0.97 |
| p-value | <0.001 | <0.001 | >0.01 |
| Methods | Normal OKN Signals | p-Value | OKN Signals with Noise | p-Value |
|---|---|---|---|---|
| Peak Finding [8] | 0.43 | <0.001 | 0.35 | <0.001 |
| FFT plus Band-Pass Filter [6] | 0.96 | <0.05 | 0.86 | <0.01 |
| FFT plus High-Pass Filter [6] | 1 | >0.05 | 0.91 | <0.05 |
| Proposed Method | 1 | - | 0.97 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, C.-B.; Hung, W.-Y.; Hsu, W.-Y. A Fast and Effective System for Analysis of Optokinetic Waveforms with a Low-Cost Eye Tracking Device. Healthcare 2021, 9, 10. https://doi.org/10.3390/healthcare9010010
Tsai C-B, Hung W-Y, Hsu W-Y. A Fast and Effective System for Analysis of Optokinetic Waveforms with a Low-Cost Eye Tracking Device. Healthcare. 2021; 9(1):10. https://doi.org/10.3390/healthcare9010010
Chicago/Turabian StyleTsai, Chong-Bin, Wei-Yu Hung, and Wei-Yen Hsu. 2021. "A Fast and Effective System for Analysis of Optokinetic Waveforms with a Low-Cost Eye Tracking Device" Healthcare 9, no. 1: 10. https://doi.org/10.3390/healthcare9010010
APA StyleTsai, C.-B., Hung, W.-Y., & Hsu, W.-Y. (2021). A Fast and Effective System for Analysis of Optokinetic Waveforms with a Low-Cost Eye Tracking Device. Healthcare, 9(1), 10. https://doi.org/10.3390/healthcare9010010