Practice-Based Research in Complementary Medicine: Could N-of-1 Trials Become the New Gold Standard?


Abstract
1. Introduction
1.1. Evidence-Based Practice in Context
1.2. Origins of the RCT Research Design
1.3. RCTs and Their Relevance to Clinical Practice
1.4. Single Case Experimental Designs (SCEDs)
1.5. N-of-1 Trials Versus RCTs for Complementary Medicine
1.6. Governance of N-of-1 Trials
1.6.1. Research Ethics
1.6.2. Insurance
1.6.3. Oversight
2. Practice-Based Clinical Scenarios in Complementary Medicine
2.1. Clinical Scenario: Probiotics for Fibromyalgia
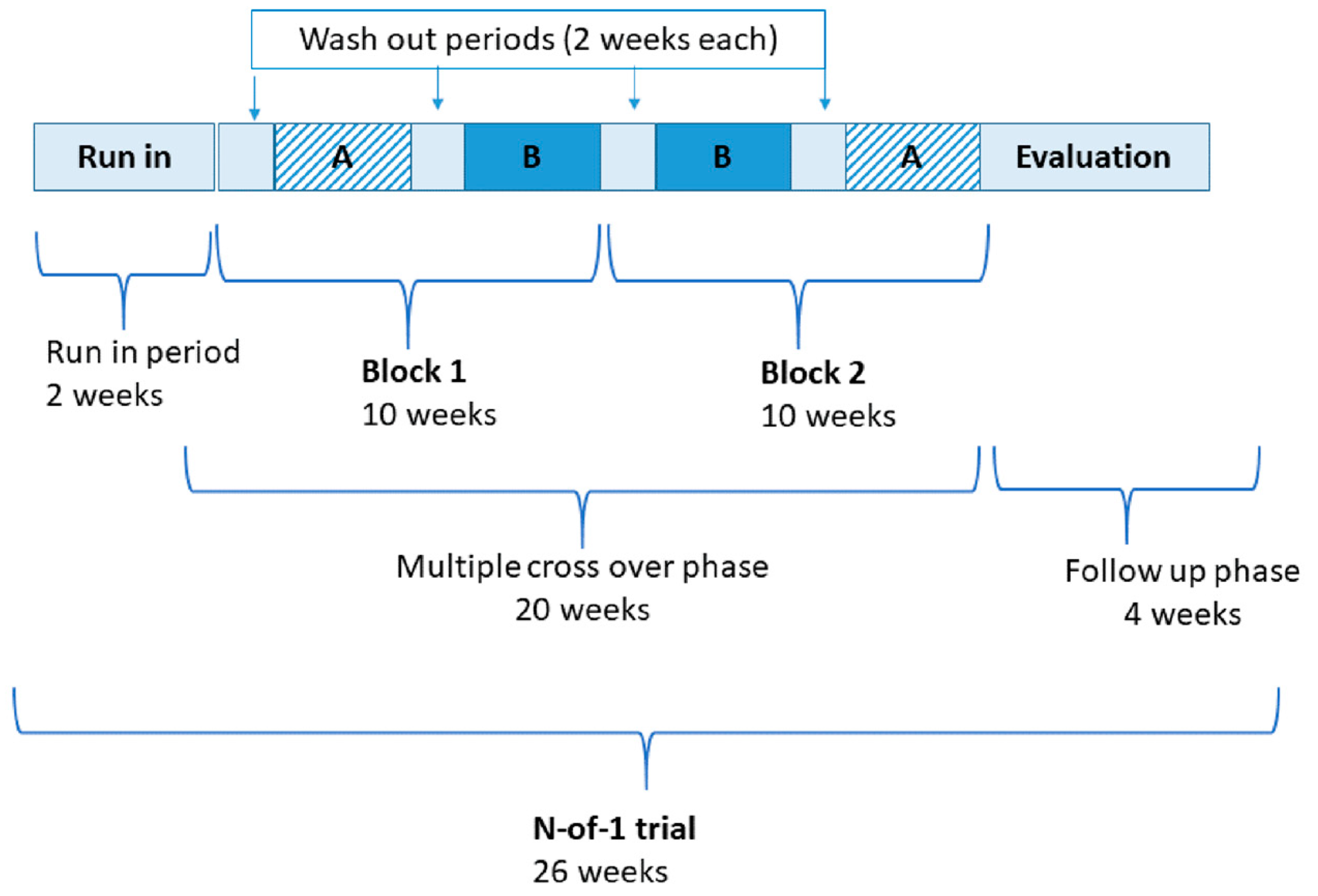
2.1.1. Trial Design
2.1.2. Primary Outcome Measurement
2.1.3. Primary Hypothesis
2.1.4. Statistical Analysis
2.1.5. Process Evaluation
3. Discussion
3.1. Patient-Centred Approach
3.2. Limitations of N-of-1 Trials as a Research Methodology
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baggoley, C. Review of the Australian Government Rebate on Natural Therapies for Private Health Insurance; Australian Government Department of Health: Canberra, Australia, 2015.
- WNF White Paper: Naturopathic Philosophies; Principles and Theories; World Naturopathic Federation: Organization, ON, Canada, 2017.
- Di Stefano, V. Holism and Complementary Medicine; Allen & Unwin: Crows Nest, Australia, 2006. [Google Scholar]
- Cabana, M.D.; Rand, C.S.; Powe, N.R.; Wu, A.W.; Wilson, M.H.; Abboud, P.-A.C.; Rubin, H.R. Why don’t physicians follow clinical practice guidelines?: A framework for improvement. JAMA 1999, 282, 1458–1465. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, S.; Kravitz, R.; Duan, N.; Kaplan, S.H. Heterogeneity of treatment effects: Implications for guidelines, payment, and quality assessment. Am. J. Med. 2007, 120, S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Claridge, J.A.; Fabian, T.C. History and development of evidence-based medicine. World J. Surg. 2005, 29, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Sackett, D.L.; Rosenberg, W.M.C.; Gray, J.A.M.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. Br. Med. J. 1996, 312, 71. [Google Scholar] [CrossRef]
- Miettinen, O.S. The modern scientific physician: 1. Can practice be science? Can. Med. Assoc. J. 2001, 165, 441–442. [Google Scholar]
- Tonelli, M.R.; Callahan, T.C. Why alternative medicine cannot be evidence-based. Acad. Med. J. Assoc. Am. Med Coll. 2001, 76, 1213–1220. [Google Scholar] [CrossRef]
- Bates, D.W.; Kuperman, G.J.; Wang, S.; Gandhi, T.; Kittler, A.; Volk, L.; Spurr, C.; Khorasani, R.; Tanasijevic, M.; Middleton, B. Ten commandments for effective clinical decision support: Making the practice of evidence-based medicine a reality. J. Am. Med. Inform. Assoc. 2003, 10, 523–530. [Google Scholar] [CrossRef]
- Davies, K.S.P. Physicians and their use of information: A survey comparison between the United States, Canada, and the United Kingdom. J. Med. Libr. Assoc. 2011, 99, 88–91. [Google Scholar] [CrossRef]
- Grace, S.; Rogers, S.; Eddey, S. The natural medicine workforce in Australia: A national survey part 2. J. Aust. Tradit. Med. Soc. 2013, 19, 79. [Google Scholar]
- Lafuente-Lafuente, C.; Leitao, C.; Kilani, I.; Kacher, Z.; Engels, C.; Canouï-Poitrine, F.; Belmin, J. Knowledge and use of evidence-based medicine in daily practice by health professionals: A cross-sectional survey. BMJ Open 2019, 9, e025224. [Google Scholar] [CrossRef]
- Fontanarosa, P.B.; Lundberg, G.D. Alternative medicine meets science. JAMA 1998, 280, 1618–1619. [Google Scholar] [CrossRef] [PubMed]
- MRC Streptomycin in Tuberculosis Trials Committee. Streptomycin treatment of pulmonary tuberculosis: A medical research council investigation. Br. Med. J. 1948, 2, 769–782. [Google Scholar] [CrossRef]
- Bhatt, A. Evolution of clinical research: A history before and beyond james lind. Perspect. Clin. Res. 2010, 1, 6–10. [Google Scholar] [PubMed]
- Australia’s Health 2016; Volume Australia’s Health Series no. 15 Cat. no. AUS 199; Australian Institute of Health and Welfare: Canberra, Australia, 2016.
- Temple, J.B.; Williams, R. Multiple health conditions and barriers to healthcare among older Australians: Prevalence, reasons and types of barriers. Aust. J. Prim. Health 2018, 24, 82–89. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, P.B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Maher, R.L.; Hanlon, J.T.; Hajjar, E.R. Clinical consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 2014, 13. [Google Scholar] [CrossRef]
- Guthrie, B.; Makubate, B.; Hernandez-Santiago, V.; Dreischulte, T. The rising tide of polypharmacy and drug-drug interactions: Population database analysis 1995–2010. BMC Med. 2015, 13, 74. [Google Scholar] [CrossRef]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Waite, L.; Seibel, M.J.; McLachlan, A.J.; Cumming, R.G.; Handelsman, D.J.; Le Couteur, D.G. Polypharmacy cutoff and outcomes: Five or more medicines were used to identify community-dwelling older men at risk of different adverse outcomes. J. Clin. Epidemiol. 2012, 65, 989–995. [Google Scholar] [CrossRef]
- Patsopoulos, N.A. A pragmatic view on pragmatic trials. Dialogues Clin. Neurosci. 2011, 13, 217–224. [Google Scholar]
- Sam, A.T.; Lian Jessica, L.L.; Parasuraman, S. A retrospective study on the incidences of adverse drug events and analysis of the contributing trigger factors. J. Basic Clin. Pharm. 2015, 6, 64–68. [Google Scholar] [CrossRef]
- Johnston, B.C.; Mills, E. N-of-1 randomized controlled trials: An opportunity for complementary and alternative medicine evaluation. J. Altern. Complement. Med. 2004, 10, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Leach, M.J.; Canaway, R.; Hunter, J. Evidence based practice in traditional & complementary medicine: An agenda for policy, practice, education and research. Complement. Ther. Clin. Pract. 2018, 31, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Veziari, Y.; Leach, M.J.; Kumar, S. Barriers to the conduct and application of research in complementary and alternative medicine: A systematic review. BMC Complement. Altern. Med. 2017, 17, 166. [Google Scholar] [CrossRef] [PubMed]
- Law, K.; Howick, J. Glossary. Available online: http://www.cebm.net/glossary/ (accessed on 16 December 2019).
- Vohra, S.; Shamseer, L.; Sampson, M.; Bukutu, C.; Schmid, C.H.; Tate, R.; Nikles, J.; Zucker, D.R.; Kravitz, R.; Guyatt, G.; et al. CONSORT extension for reporting N-of-1 trials (CENT) 2015 statement. BMJ Clin. Res. 2015, 350, h1738. [Google Scholar] [CrossRef]
- Lillie, E.O.; Patay, B.; Diamant, J.; Issell, B.; Topol, E.J.; Schork, N.J. The n-of-1 clinical trial: The ultimate strategy for individualizing medicine? Pers. Med. 2011, 8, 161–173. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, H.; et al. The Oxford 2011 Levels of Evidence. Available online: http://www.cebm.net/index.aspx?o=5653 (accessed on 2 November 2019).
- Punja, S.; Bukutu, C.; Shamseer, L.; Sampson, M.; Hartling, L.; Urichuk, L.; Vohra, S. N-of-1 trials are a tapestry of heterogeneity. J. Clin. Epidemiol. 2016, 76, 47–56. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Inauen, J.; Nieuwenboom, W.; Nurmi, J.; Schneider, A.; Short, C.E.; Dekkers, T.; Williams, A.J.; Bierbauer, W.; Haukkala, A.; et al. Challenges and solutions for N-of-1 design studies in health psychology. Health Psychol. Rev. 2019, 13, 163–178. [Google Scholar] [CrossRef]
- Tate, R.L.; Perdices, M. N-of-1 trials in the behavioral sciences. In The Essential Guide to N-of-1 Trials in Health; Springer: Berlin, Germany, 2015; pp. 19–41. [Google Scholar]
- Harris, T.; Nikles, J. Herbal medicines used in the treatment of chronic insomnia and how they influence sleep patterns: A review. J. Complement. Med. Altern. Healthc. 2018, 6. [Google Scholar] [CrossRef]
- Piantadosi, S. Treatment effects monitoring. In Clinical Trials: A Methodological Perspective, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2005. [Google Scholar]
- Shamseer, L.; Hopewell, S.; Altman, D.G.; Moher, D.; Schulz, K.F. Update on the endorsement of CONSORT by high impact factor journals: A survey of journal “Instructions to Authors” in 2014. Trails 2016, 17, 301. [Google Scholar] [CrossRef]
- Tate, R.; Mcdonald, S.; Perdices, M.; Togher, L.; Schultz, R.; Savage, S. Rating the methodological quality of single-subject designs and n-of-1 trials: Introducing the Single-Case Experimental Design (SCED) scale. Neuropsychol. Rehabil. 2008, 18, 385–401. [Google Scholar] [CrossRef]
- Nikles, C.J.; Clavarino, A.M.; Del Mar, C.B. Using n-of-1 trials as a clinical tool to improve prescribing. Br. J. Gen. Pract. 2005, 55, 175–180. [Google Scholar] [PubMed]
- Foley, H.; Steel, A. Patient perceptions of clinical care in complementary medicine: A systematic review of the consultation experience. Patient Educ. Couns. 2017, 100, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Scuffham, P.A.; Nikles, J.; Mitchell, G.K.; Yelland, M.J.; Vine, N.1; Poulos, C.J.; Pillans, P.I.; Bashford, G.; del Mar, C.; Schluter, P.J.; et al. Using N-of-1 trials to improve patient management and save costs. J. Gen. Intern. Med. 2010, 25, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Avins, A.L.; Bent, S.; Neuhaus, J.M. Use of an embedded N-of-1 trial to improve adherence and increase information from a clinical study. Contemp. Clin. Trials 2005, 26, 397–401. [Google Scholar] [CrossRef]
- Rodnick, J.E. Australia: The N of 1 trial, an underappreciated research method. US Natl. Libr. Med. Natl. Inst. Health 2006, 38, 63. [Google Scholar]
- Kronish, I.M.; Hampsey, M.; Falzon, L.; Konrad, B.; Davidson, K.W. Personalized (N-of-1) trials for depression: A systematic review. J. Clin. Psychopharmacol. 2018, 38, 218–225. [Google Scholar] [CrossRef]
- Clough, A.J.; Hilmer, S.N.; Naismith, S.L.; Kardell, L.D.; Gnjidic, D. N-of-1 trials for assessing the effects of deprescribing medications on short-term clinical outcomes in older adults: A systematic review. J. Clin. Epidemiol. 2018, 93, 112–119. [Google Scholar] [CrossRef]
- Huang, H.; Yang, P.; Xue, J.; Tang, J.; Ding, L.; Ma, Y.; Wang, J.; Guyatt, G.H.; Vanniyasingam, T.; Zhang, Y. Evaluating the individualized treatment of traditional Chinese medicine: A pilot study of N-of-1 trials. Evid. Based Complement. Altern. Med. 2014, 2014. [Google Scholar] [CrossRef]
- Mitchell, G.K.; Hardy, J.R.; Nikles, C.J.; Carmont, S.-A.S.; Senior, H.E.; Schluter, P.J.; Good, P.; Currow, D.C. The effect of methylphenidate on fatigue in advanced cancer: An aggregated n-of-1 trial. J. Pain Symptom Manag. 2015, 50, 289–296. [Google Scholar] [CrossRef]
- Li, J.; Gao, W.; Punja, S.; Ma, B.; Vohra, S.; Duan, N.; Gabler, N.; Yang, K.; Kravitz, R.L. Reporting quality of N-of-1 trials published between 1985 and 2013: A systematic review. J. Clin. Epidemiol. 2016. [Google Scholar] [CrossRef]
- Zucker, D.R.; Ruthazer, R.; Schmid, C.H. Individual (N-of-1) trials can be combined to give population comparative treatment effect estimates: Methodologic considerations. J. Clin. Epidemiol. 2010, 63, 1312–1323. [Google Scholar] [CrossRef] [PubMed]
- Duan, N.; Kravitz, R.L.; Schmid, C.H. Single-patient (n-of-1) trials: A pragmatic clinical decision methodology for patient-centered comparative effectiveness research. J. Clin. Epidemiol. 2013, 66, S21–S28. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Carlino, E.; Piedimonte, A. Increasing uncertainty in CNS clinical trials: The role of placebo, nocebo, and Hawthorne effects. Lancet Neurol. 2016, 15, 736–747. [Google Scholar] [CrossRef]
- Berthelot, J.-M.; Le, B.G.; Maugars, Y. The hawthorne effect: Stronger than the placebo effect? Jt. Bone Spine 2011, 78, 335–336. [Google Scholar] [CrossRef]


{kind=link}
| RCT | N-of-1 Trials | |
|---|---|---|
| Advantages | Experimental design to determine cause effect relationship for the intervention on the outcome in carefully selected sample. | Experimental design to determine best intervention for individual patient. |
| Tightly controlled clinical environment, increases internal validity. | Patient-centered research, through shared decision making about the study design (e.g., outcomes and/or interventions may be chosen by patient). For example, patients need not withdraw from their usual care, which can be incorporated into the design as a baseline or placebo condition. | |
| Bias minimized via random allocation to groups, allocation concealment and ongoing blinding of participants and data collectors. | Bias minimized via random allocation of exposure to treatments, allocation concealment and ongoing blinding of participants and data collectors to condition, where possible. | |
| Effect size estimated and generalizable to populations. | Determination about whether a particular treatment works for an individual at a given point in time. | |
| Powerful statistical analysis that enable conclusive determinations based on experimental hypothesis testing in adequately powered study designs, based on number of participants. | Power is derived from number of measurement points rather than number of participants. | |
| Can be included in systematic reviews and meta-analyses of RCTs. | Can be included in systematic reviews and meta-analyses of N-of-1 trials. | |
| More concerned with efficacy than effectiveness. | More concerned with effectiveness than efficacy. | |
| Limitations | Results apply to population means rather than individuals. | Results apply only to the specific individual who was included in the trial. |
| Strict inclusion/exclusion criteria means that the sample is not necessarily reflective of clinical usage in a general clinical population (i.e., increasing internal validity reduces the generalizability/external validity of the findings). | Lack of generalizability to estimate effect size in populations in single N-of-1 trials. However, multiple N-of-1 trials can be aggregated as an N-of-1 series or meta-analysis, in order to estimate population effect sizes. | |
| Expensive and time consuming to run. | Time consuming for practitioner and patient. | |
| Results often not known for years | Statistical analysis not as powerful as parametric tests are not suited to small number and repeated measures samples (usually violate assumptions of normality and independence); usually uses simple visual descriptive analyses or more complex Bayesian analyses. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bradbury, J.; Avila, C.; Grace, S. Practice-Based Research in Complementary Medicine: Could N-of-1 Trials Become the New Gold Standard? Healthcare 2020, 8, 15. https://doi.org/10.3390/healthcare8010015
Bradbury J, Avila C, Grace S. Practice-Based Research in Complementary Medicine: Could N-of-1 Trials Become the New Gold Standard? Healthcare. 2020; 8(1):15. https://doi.org/10.3390/healthcare8010015
Chicago/Turabian StyleBradbury, Joanne, Cathy Avila, and Sandra Grace. 2020. "Practice-Based Research in Complementary Medicine: Could N-of-1 Trials Become the New Gold Standard?" Healthcare 8, no. 1: 15. https://doi.org/10.3390/healthcare8010015
APA StyleBradbury, J., Avila, C., & Grace, S. (2020). Practice-Based Research in Complementary Medicine: Could N-of-1 Trials Become the New Gold Standard? Healthcare, 8(1), 15. https://doi.org/10.3390/healthcare8010015