Correlations of Self-Reported Androgen Deficiency in Ageing Males (ADAM) with Stress and Sleep among Young Adult Males

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Harman, S.M.; Metter, E.J.; Tobin, J.D.; Pearson, J.; Blackman, M.R. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. J. Clin. Endocrinol. Metab. 2001, 86, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Chiles, K.A. Hypogonadism and erectile dysfunction as harbingers of systemic disease. Transl. Androl. Urol. 2016, 5, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Rastrelli, G.; Monami, M.; Guay, A.; Buvat, J.; Sforza, A.; Forti, G.; Mannucci, E.; Maggi, M. Hypogonadism as a risk factor for cardiovascular mortality in men: A meta-analytic study. Eur. J. Endocrinol. 2011, 165, 687–701. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, M.; Thomas, M.C.; Panagiotopoulos, S.; Sharpe, K.; MacIsaac, R.J.; Clarke, S.; Zajac, J.D.; Jerums, G. Low testosterone levels are common and associated with insulin resistance in men with diabetes. J. Clin. Endocrinol. Metab. 2008, 93, 1834–1840. [Google Scholar] [CrossRef] [PubMed]
- Guay, A.T.; Traish, A. Testosterone deficiency and risk factors in the metabolic syndrome: Implications for erectile dysfunction. Urol. Clin. 2011, 38, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Traish, A.M.; Saad, F.; Feeley, R.J.; Guay, A. The dark side of testosterone deficiency: III. Cardiovascular disease. J. Androl. 2009, 30, 477–494. [Google Scholar] [CrossRef] [PubMed]
- Dandona, P.; Rosenberg, M. A practical guide to male hypogonadism in the primary care setting. Int. J. Clin. Pract. 2010, 64, 682–696. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of Obesity among Adults and Youth: United States, 2011–2014; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Washington, DC, USA, 2015.
- Sterling, J.; Bernie, A.M.; Ramasamy, R. Hypogonadism: Easy to define, hard to diagnose, and controversial to treat. Can. Urol. Assoc. J. 2015, 9, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Traish, A.; Haider, A.; Doros, G.; Saad, F. Long-term testosterone therapy in hypogonadal men ameliorates elements of the metabolic syndrome: An observational, long-term registry study. Int. J. Clin. Pract. 2014, 68, 314–329. [Google Scholar] [CrossRef] [PubMed]
- El Saghier, E.O.; Shebl, S.E.; Fawzy, O.A.; Eltayeb, L.M.; Bekhet, L.M.; Gharib, A. Androgen deficiency and erectile dysfunction in patients with type 2 diabetes. Clin. Med. Insights Endocrinol. Diabetes 2015, 8, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Ugwu, T.E.; Ikem, R.T.; Kolawole, B.A.; Ezeani, I.U. Clinicopathologic assessment of hypogonadism in men with type 2 diabetes mellitus. Indian J. Endocrinol. Metab. 2016, 20, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Dhindsa, S.; Ghanim, H.; Batra, M.; Kuhadiya, N.D.; Abuaysheh, S.; Sandhu, S.; Green, K.; Makdissi, A.; Hejna, J.; Chaudhuri, A. Insulin resistance and inflammation in hypogonadotropic hypogonadism and their reduction after testosterone replacement in men with type 2 diabetes. Diabetes Care 2016, 39, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Helmreich, D.L.; Parfitt, D.; Lu, X.-Y.; Akil, H.; Watson, S. Relation between the hypothalamic-pituitary-thyroid (HPT) axis and the hypothalamic-pituitary-adrenal (HPA) axis during repeated stress. Neuroendocrinology 2005, 81, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Leproult, R.; Van Cauter, E. Role of sleep and sleep loss in hormonal release and metabolism. In Pediatric Neuroendocrinology; Karger Publishers: Basel, Switzerland, 2010; Volume 17, pp. 11–21. [Google Scholar]
- Mong, J.A.; Cusmano, D.M. Sex differences in sleep: Impact of biological sex and sex steroids. Philos. Trans. R. Soc. B 2016, 371, 20150110. [Google Scholar] [CrossRef] [PubMed]
- Lund, H.G.; Reider, B.D.; Whiting, A.B.; Prichard, J.R. Sleep patterns and predictors of disturbed sleep in a large population of college students. J. Adolesc. Health 2010, 46, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Patel, S. Reduced sleep as an obesity risk factor. Obes. Rev. 2009, 10, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Sundquist, J.; Winkleby, M.A.; Sundquist, K. Stress resilience and subsequent risk of type 2 diabetes in 1.5 million young men. Diabetologia 2016, 59, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Bernie, A.M.; Scovell, J.M.; Ramasamy, R. Comparison of questionnaires used for screening and symptom identification in hypogonadal men. Aging Male 2014, 17, 195–198. [Google Scholar] [CrossRef] [PubMed]
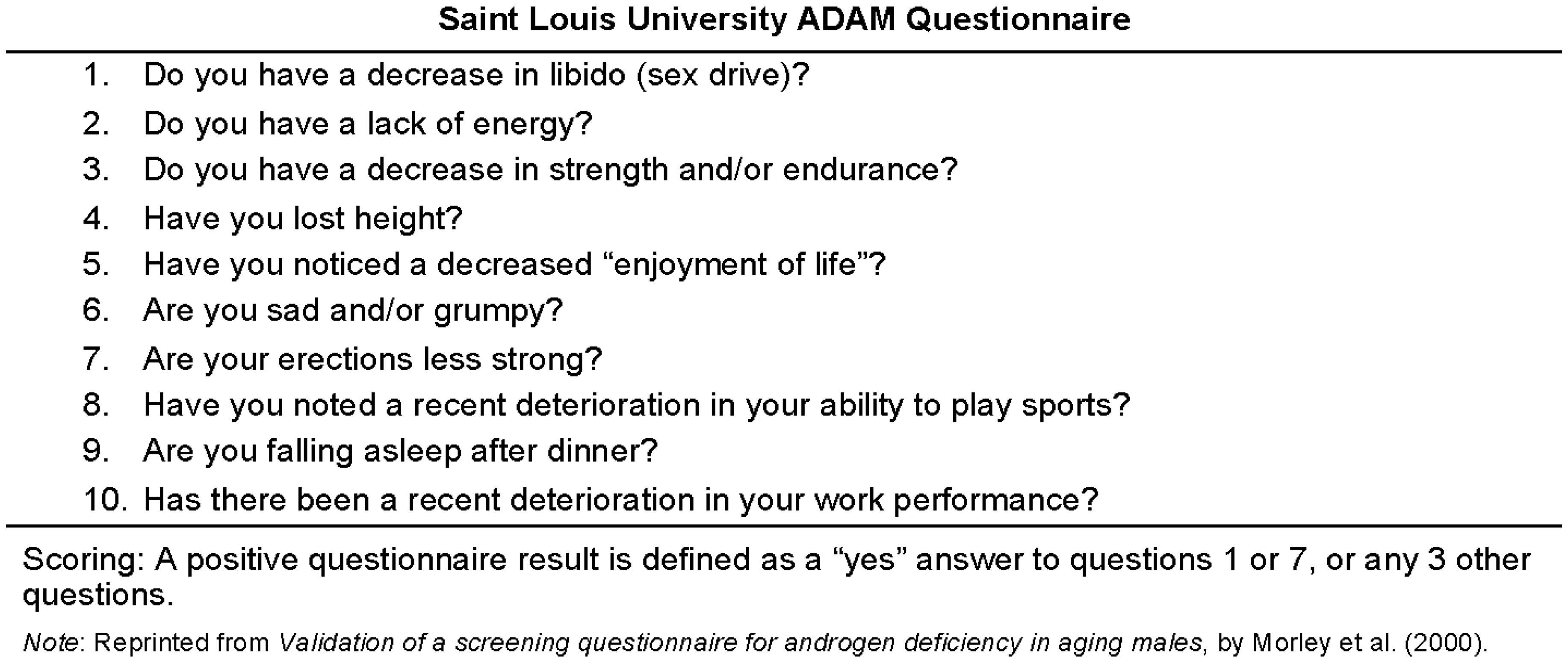
- Morley, J.E.; Charlton, E.; Patrick, P.; Kaiser, F.; Cadeau, P.; McCready, D.; Perry, H. Validation of a screening questionnaire for androgen deficiency in aging males. Metab. Clin. Exp. 2000, 49, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 385–396. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- JMP®. V.S.I.I. [Statistical Software]; A Business Unit of SAS; SAS Campus Drive: Cary, NC, USA, 1989–2007. [Google Scholar]
- SAS Institute Inc. Base SAS® 9.3 Procedures Guide; N.S.I.I.; SAS Institute Inc.: Cary, NC, USA, 2011. [Google Scholar]
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System (BRFSS) Prevalence Data (2011 to present) | Chronic Disease and Health Promotion Data & Indicators; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018.
- Wells, J.C. Sexual dimorphism of body composition. Best Pract. Res. Clin. Endocrinol. Metab. 2007, 21, 415–430. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, S.; Cunningham, G.R.; Hayes, F.J.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Montori, V.M. Testosterone therapy in adult men with androgen deficiency syndromes: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2006, 91, 1995–2010. [Google Scholar] [CrossRef] [PubMed]
- Mayo Clinic. Test ID: TTFB—Testosterone, T., Bioavailable, and Free, Serum; Mayo Medical Laboratories: Rochester, MN, USA, 2018. [Google Scholar]
- Cabral, R.D.; Busin, L.; Rosito, T.E.; Koff, W.J. Performance of Massachusetts Male Aging Study (MMAS) and androgen deficiency in the aging male (ADAM) questionnaires in the prediction of free testosterone in patients aged 40 years or older treated in outpatient regimen. Aging Male 2014, 17, 147–154. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic | Frequency (%) | ||
|---|---|---|---|
| Male Sample | ADAM Positive Sub-Sample | ||
| N = 409 | N = 144 | ||
| Race * | Alaska Native/American Indian | 16 (3.91) | 5 (3.47) |
| Asian | 59 (14.43) | 21 (14.58) | |
| Black/African-American | 49 (11.98) | 18 (12.50) | |
| Hispanic/Latino | 70 (17.11) | 21 (14.58) | |
| Native Hawaiian/Pacific Islander | 3 (0.73) | 1 (0.69) | |
| White | 287 (70.17) | 100 (69.44) | |
| Other or Choose not to answer | 17 (4.16) | 8 (5.56) | |
| State | Alabama | 23 (5.62) | 9 (6.25) |
| Florida | 79 (19.32) | 28 (19.44) | |
| Kansas | 35 (8.26) | 11 (7.64) | |
| Maine | 63 (15.40) | 14 (9.72) | |
| New York | 65 (15.89) | 20 (13.89) | |
| South Dakota | 15 (3.67) | 6 (4.17) | |
| Tennessee | 85 (20.78) | 33 (22.92) | |
| West Virginia | 40 (9.78) | 21 (14.58) | |
| Choose not to answer | 4 (0.98) | 2 (1.39) | |
| Anthropometric | Total Male Sample | ADAM SCORES | Significance | |
|---|---|---|---|---|
| Positive | Negative | |||
| Height (cm) | 176.06 ± 7.40 | 175.50 ± 7.23 | 176.36 ± 7.48 | Z = −0.975, p = 0.3293, Wilcoxon |
| Weight (kg) | 77.43 ± 15.98 | 77.95 ± 16.67 | 77.15 ± 15.62 | Z = 0.323, p = 0.7460, Wilcoxon |
| BMI (kg/m2) | 24.90 ± 4.62 | 25.20 ± 4.88 | 24.74 ± 4.48 | Z = 0.905, p = 0.3652, Wilcoxon |
| Waist Circumference (cm) | 82.94 ± 10.49 | 82.46 ± 9.66 | 83.19 ± 10.92 | Z = 0.7542, p = 0.7538, Wilcoxon |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charlier, C.M.; Barr, M.L.; Colby, S.E.; Greene, G.W.; Olfert, M.D. Correlations of Self-Reported Androgen Deficiency in Ageing Males (ADAM) with Stress and Sleep among Young Adult Males. Healthcare 2018, 6, 121. https://doi.org/10.3390/healthcare6040121
Charlier CM, Barr ML, Colby SE, Greene GW, Olfert MD. Correlations of Self-Reported Androgen Deficiency in Ageing Males (ADAM) with Stress and Sleep among Young Adult Males. Healthcare. 2018; 6(4):121. https://doi.org/10.3390/healthcare6040121
Chicago/Turabian StyleCharlier, Camille M., Makenzie L. Barr, Sarah E. Colby, Geoffrey W. Greene, and Melissa D. Olfert. 2018. "Correlations of Self-Reported Androgen Deficiency in Ageing Males (ADAM) with Stress and Sleep among Young Adult Males" Healthcare 6, no. 4: 121. https://doi.org/10.3390/healthcare6040121
APA StyleCharlier, C. M., Barr, M. L., Colby, S. E., Greene, G. W., & Olfert, M. D. (2018). Correlations of Self-Reported Androgen Deficiency in Ageing Males (ADAM) with Stress and Sleep among Young Adult Males. Healthcare, 6(4), 121. https://doi.org/10.3390/healthcare6040121