Diagnostic Reasoning across the Medical Education Continuum

Abstract
:1. Introduction
2. Experimental Section
- If someone complained of shortness of breath, how would you figure out that the cause was [insert disease]?
- What do you believe are the critical elements for making that diagnosis?
- What helped or hindered you in learning this?
- Can you remember anyone (an acquaintance, family member, or patient) with this disease?
3. Results
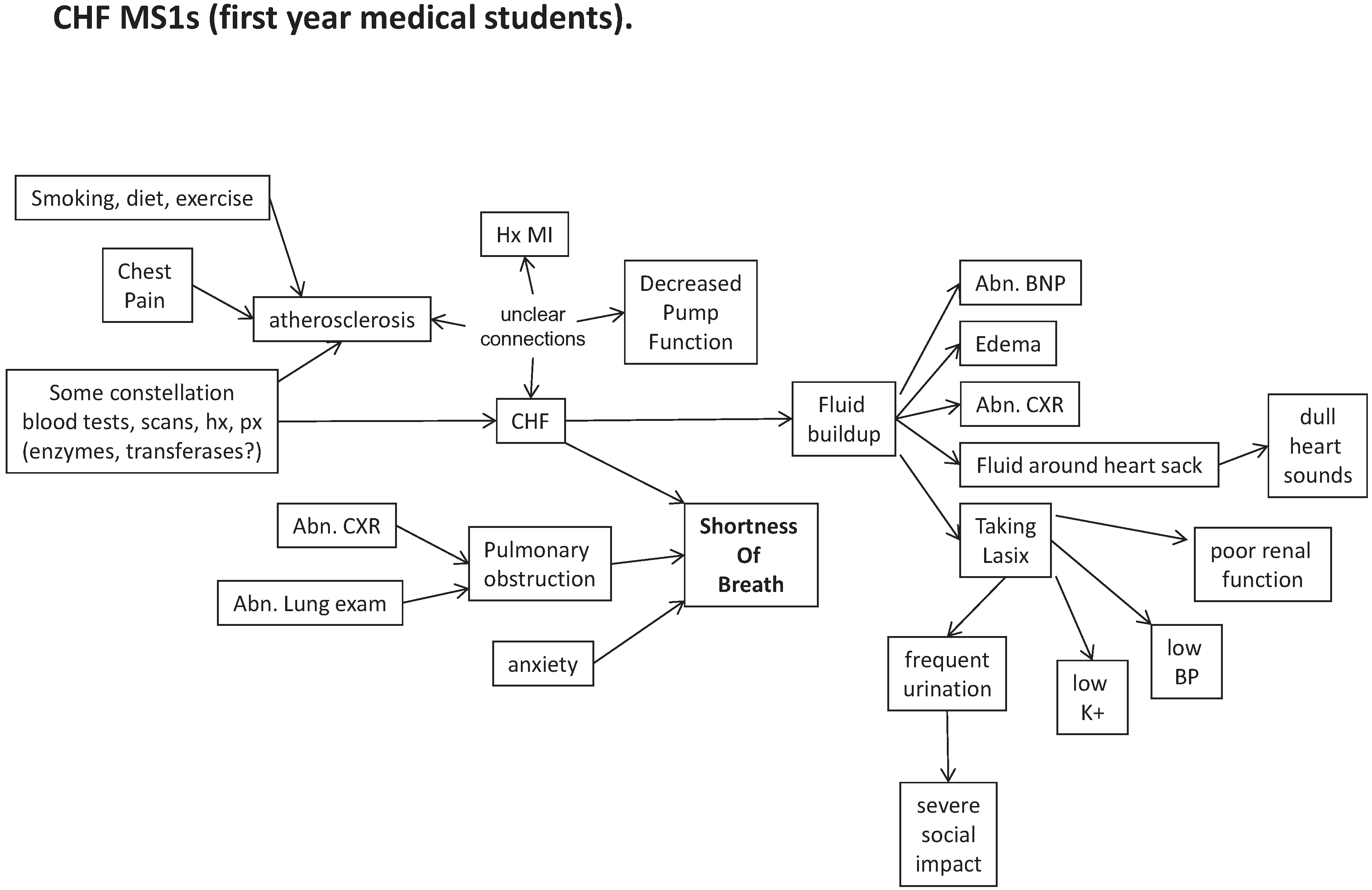
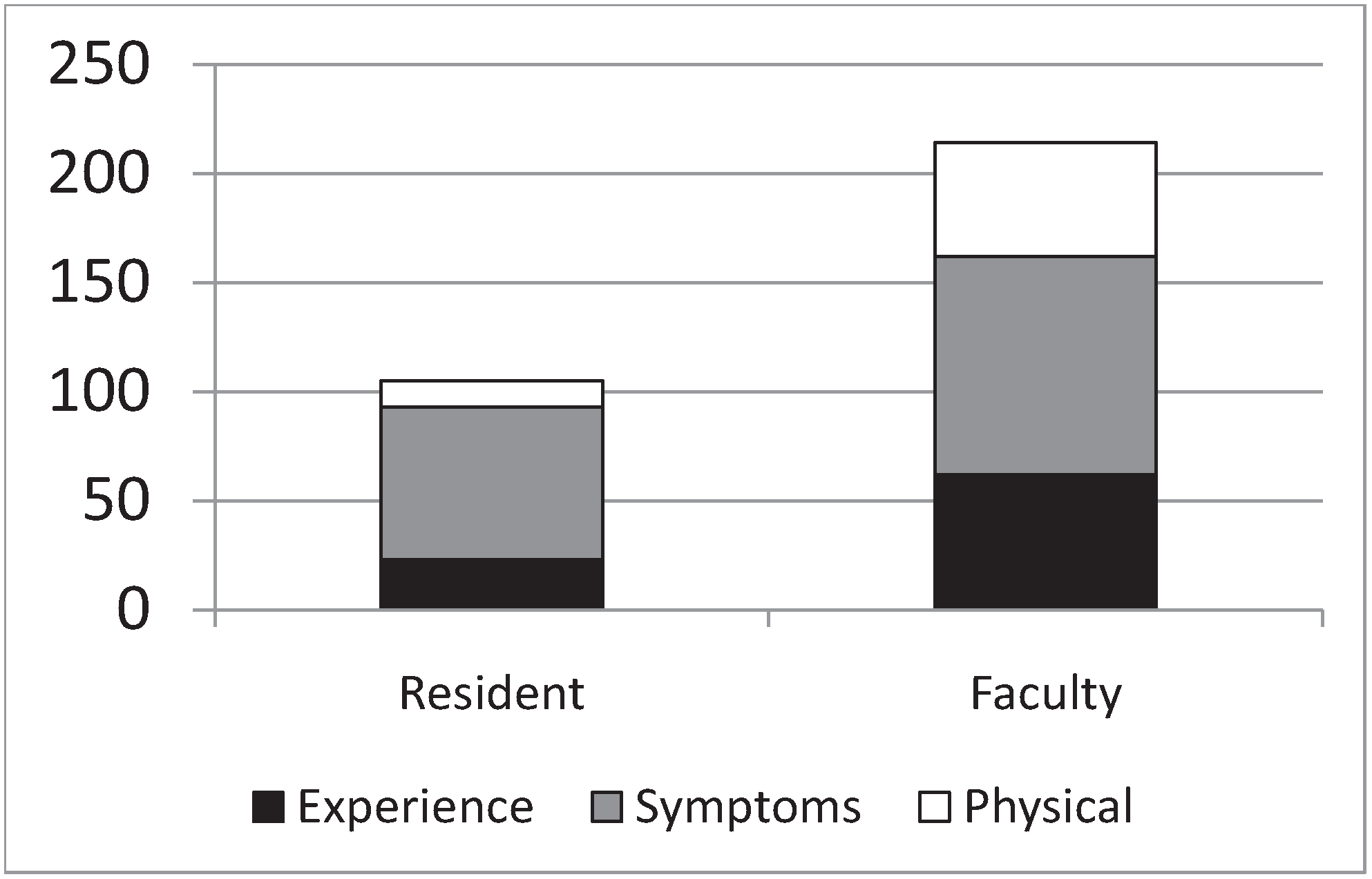
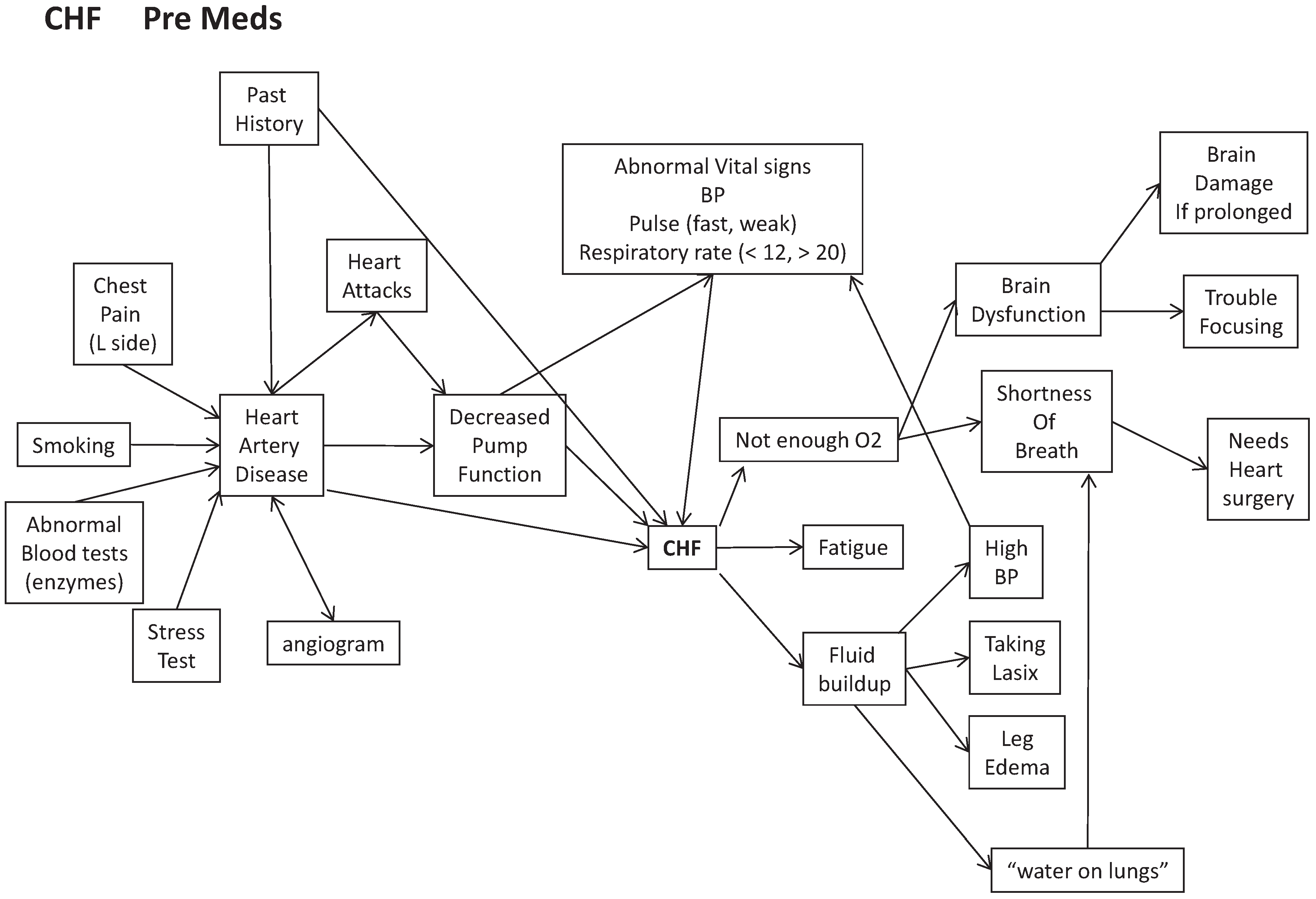
3.1. Novices: The Apprentice Effect

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
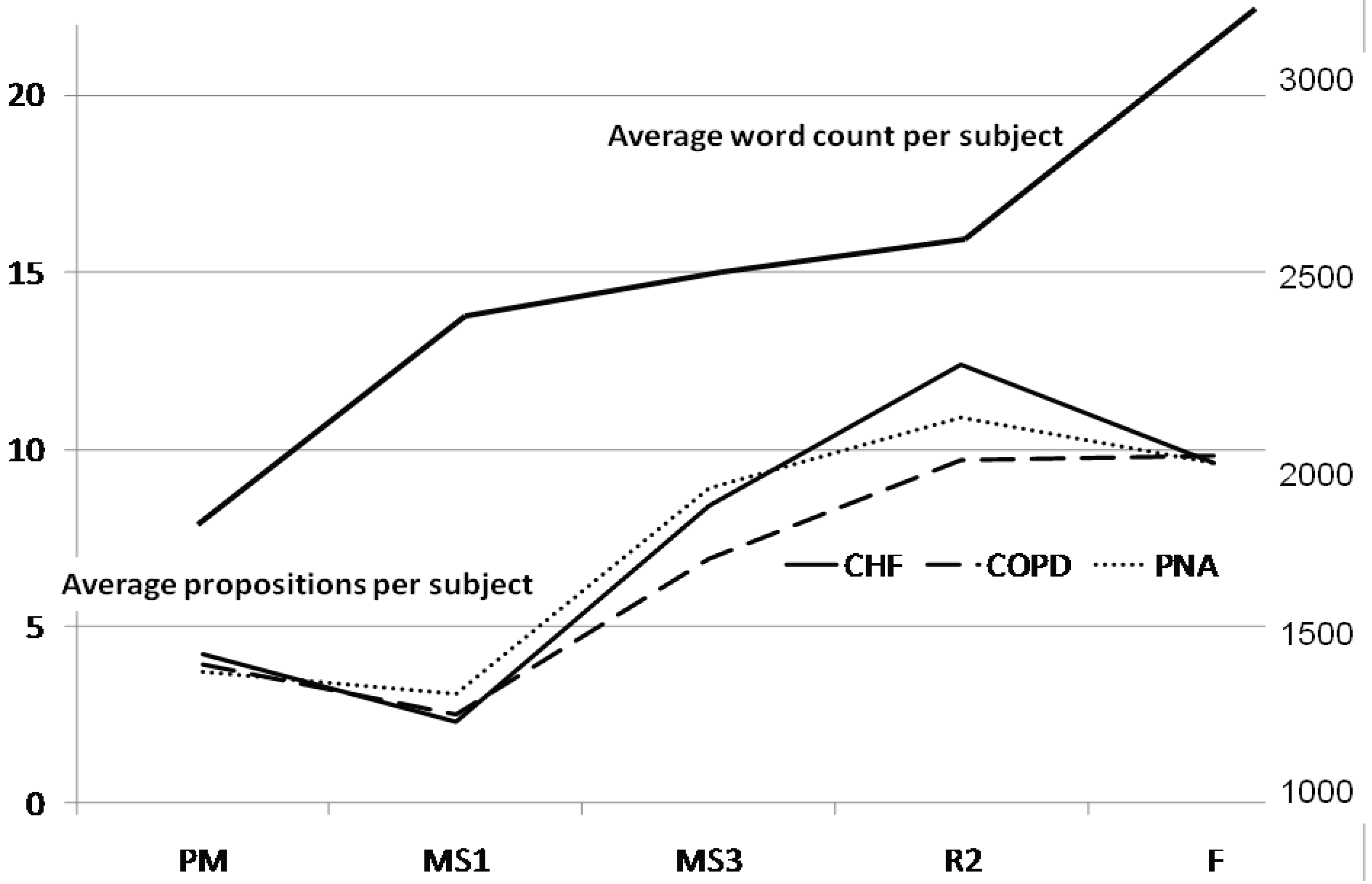
| Training Level | Average # of Propositions Per Disease Group (Standard Deviation) | Percentage of Total Words that Are Propositions | Number of Concept Connections in Summary Concept Map |
|---|---|---|---|
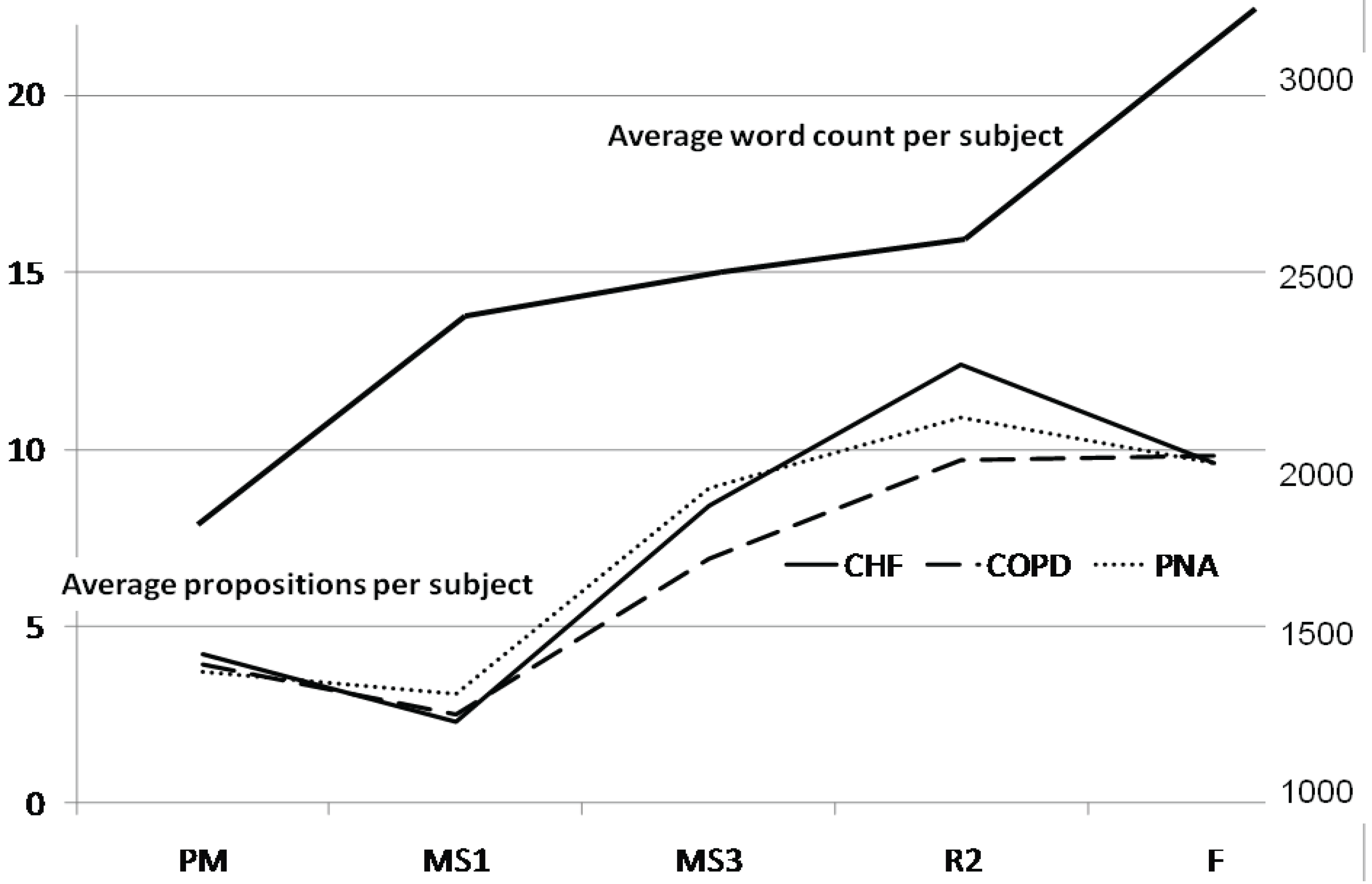
| PM | 4.2 (2) | 2.7% | 30 |
| MS1 | 2.3 (1.8) | 1.4% | 25 |
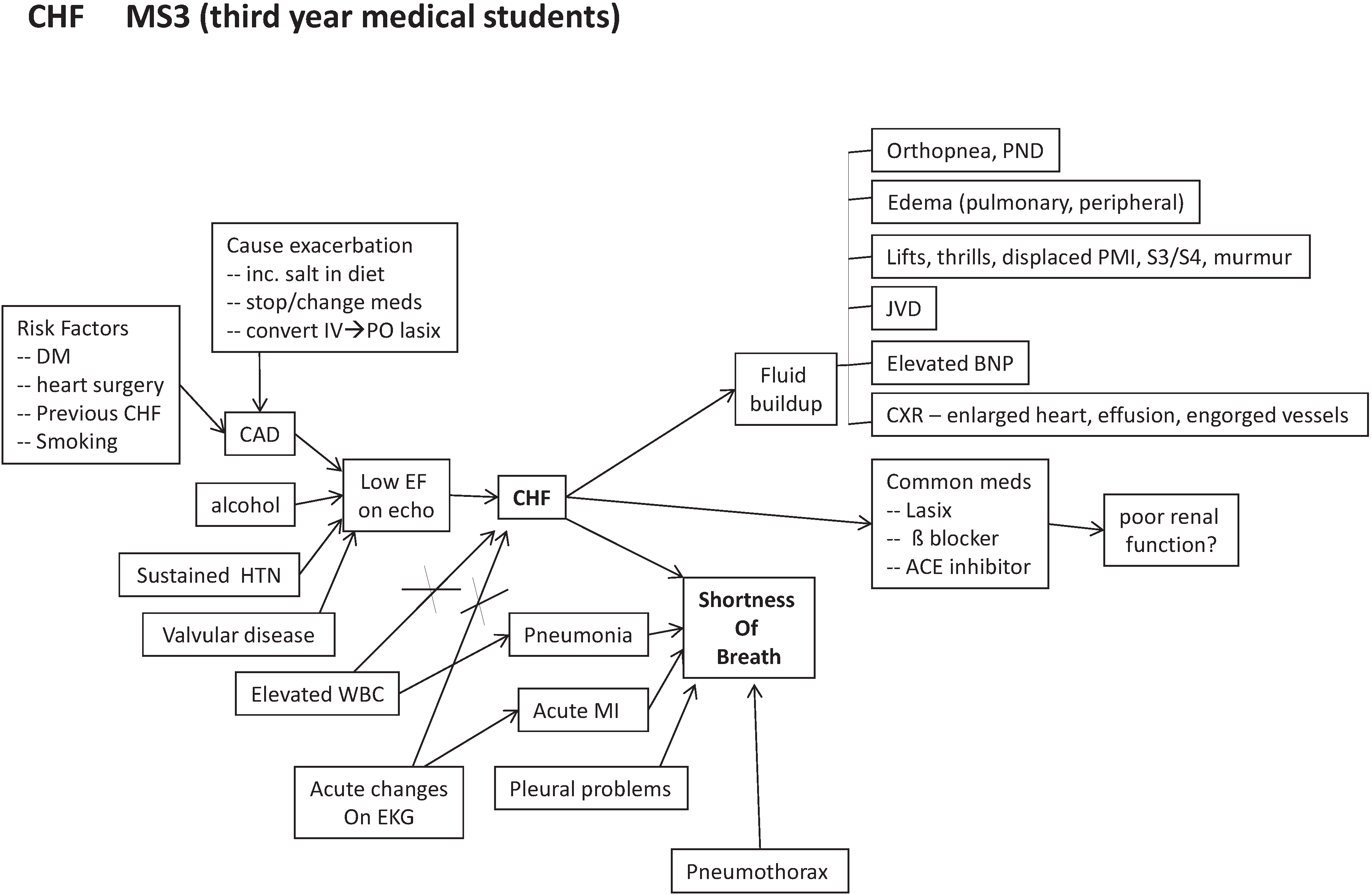
| MS3 | 8.4 (3.1) | 5.5% | 34 |
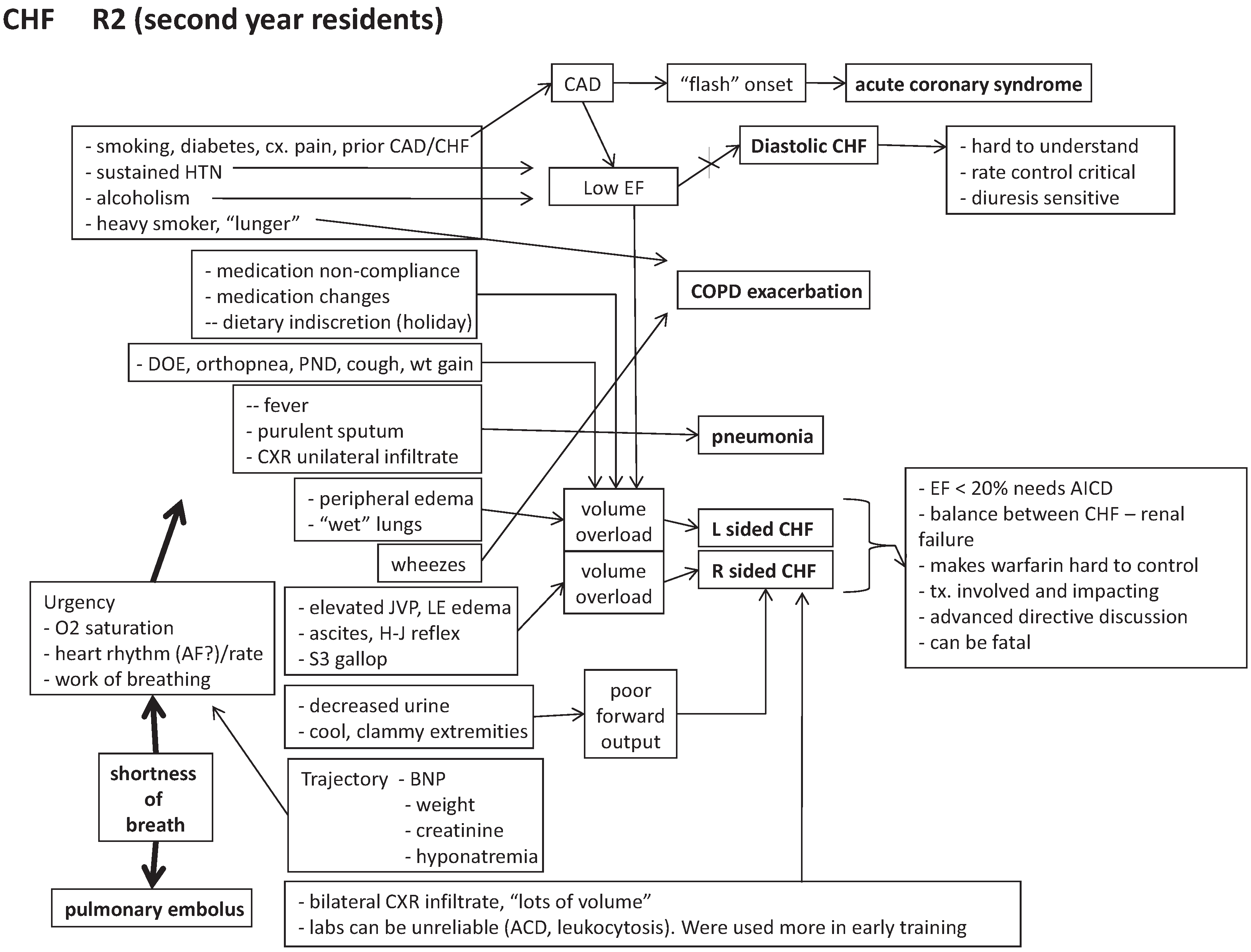
| R2 | 12.4 (5.4) | 7.8% | 56 |
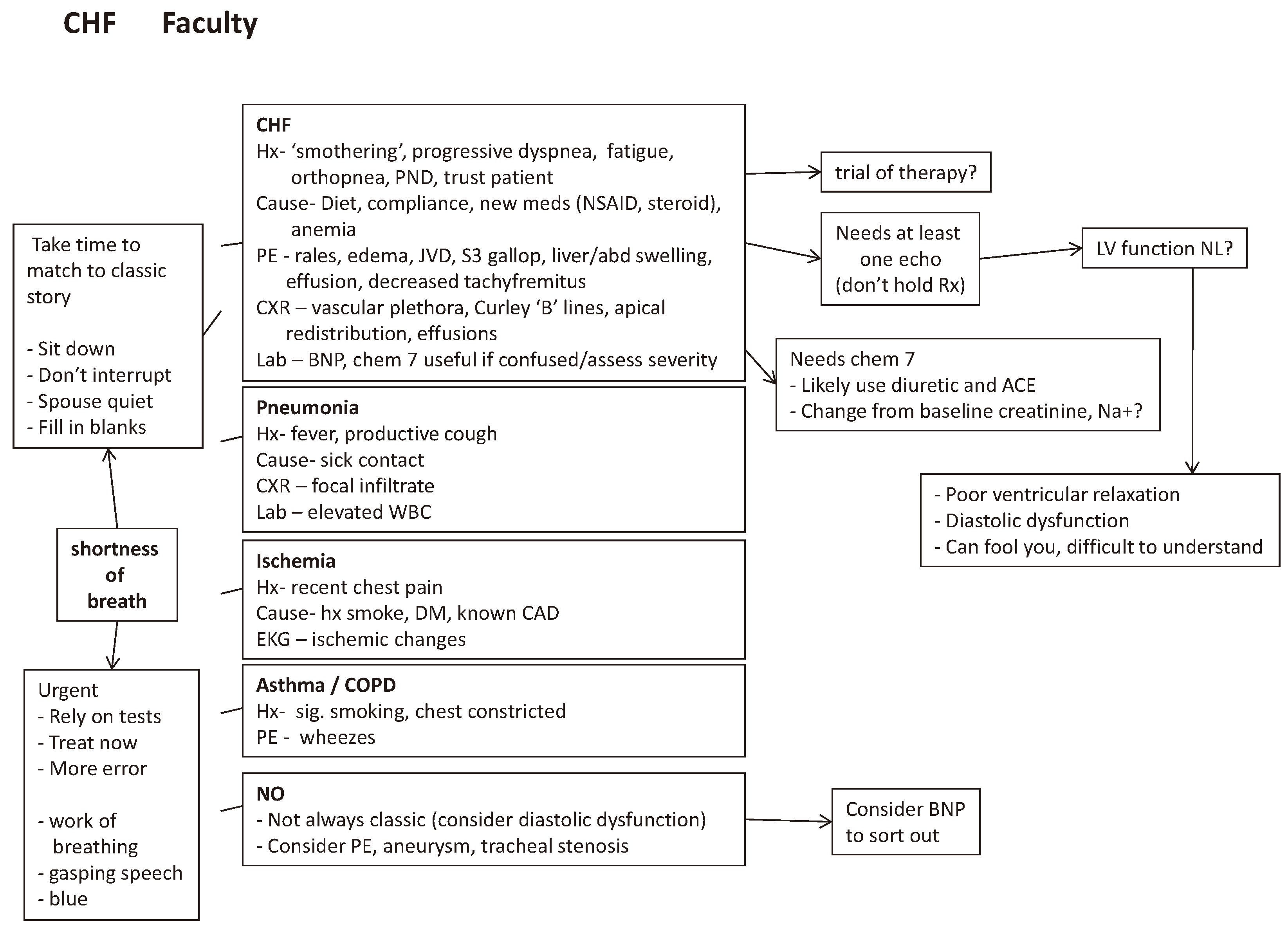
| F | 9.6 (4.2) | 4.3% | 35 |
- Example 1 (PM) “… on TV if they had specials on Oprah or on any other shows”.
- Example 2 (PM) “… with congestive heart failure, um… I’d check for weight, check cholesterol levels, and this is mainly from ‘House’ [a TV show]”.
- Example 3 (MS1) “I feel like labs would help a lot… x-rays or CT scans”.
- Example 4 (MS1) “There might be some kind of a characteristic signature in the lab values that would lead you to that [diagnosis]”.
- Example 5 (MS1) “Shortness of breath you can tell upon, just observation of the patient. How to determine that it’s due to congestive heart failure? Um, I don’t know the exact process, or which exams, or which laboratory I would order.”
| Category Title | Definition |
|---|---|
| A Story | Where the participant relates personal experience related to a specific other(s). Each specific other is another story. |
| Cue Generation | A list of cues generated to explain or define diagnosis. |
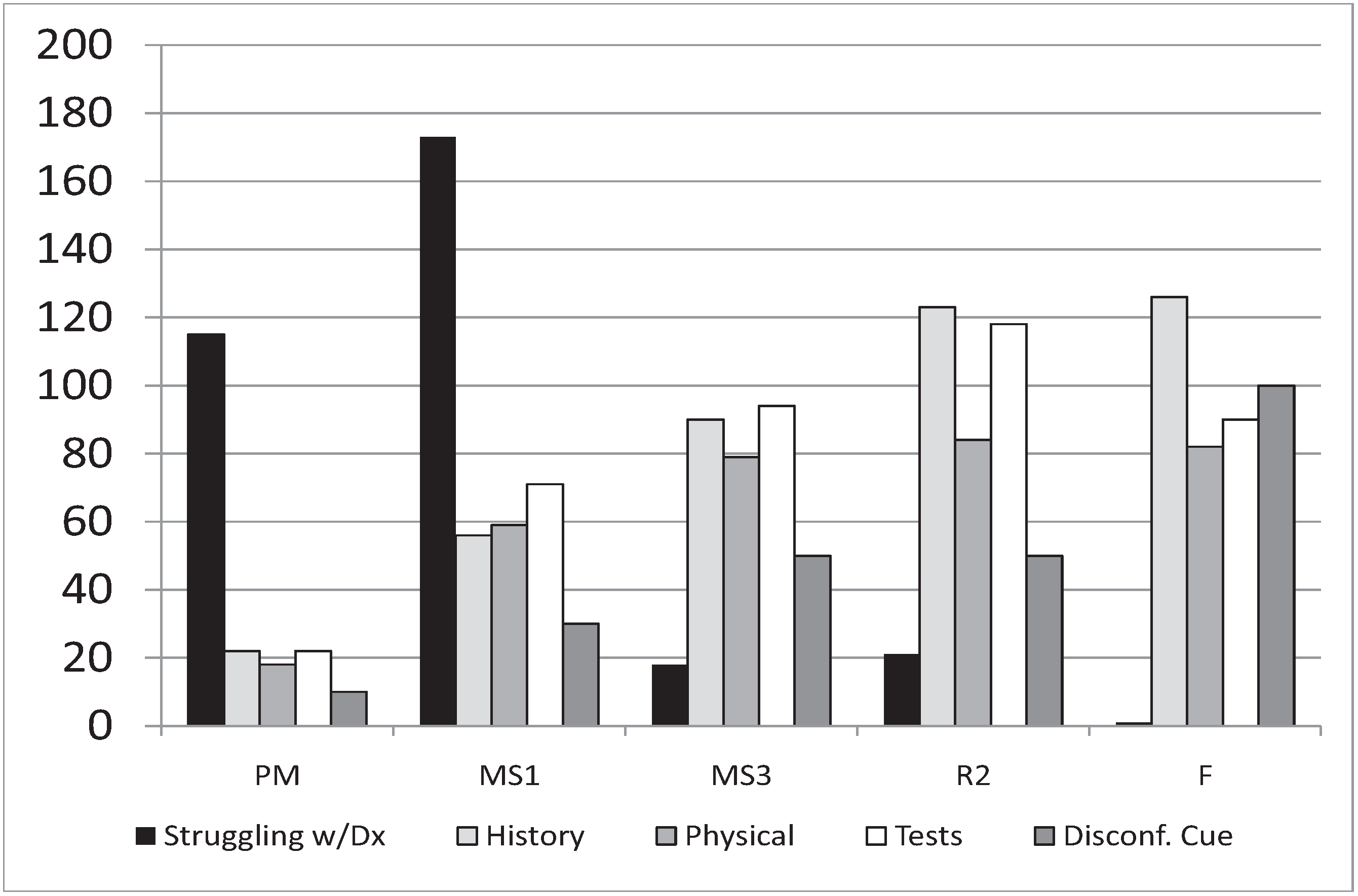
| Disconfirming Cue | The absence of an expected cue or the presence of a cue that negates a diagnosis. |
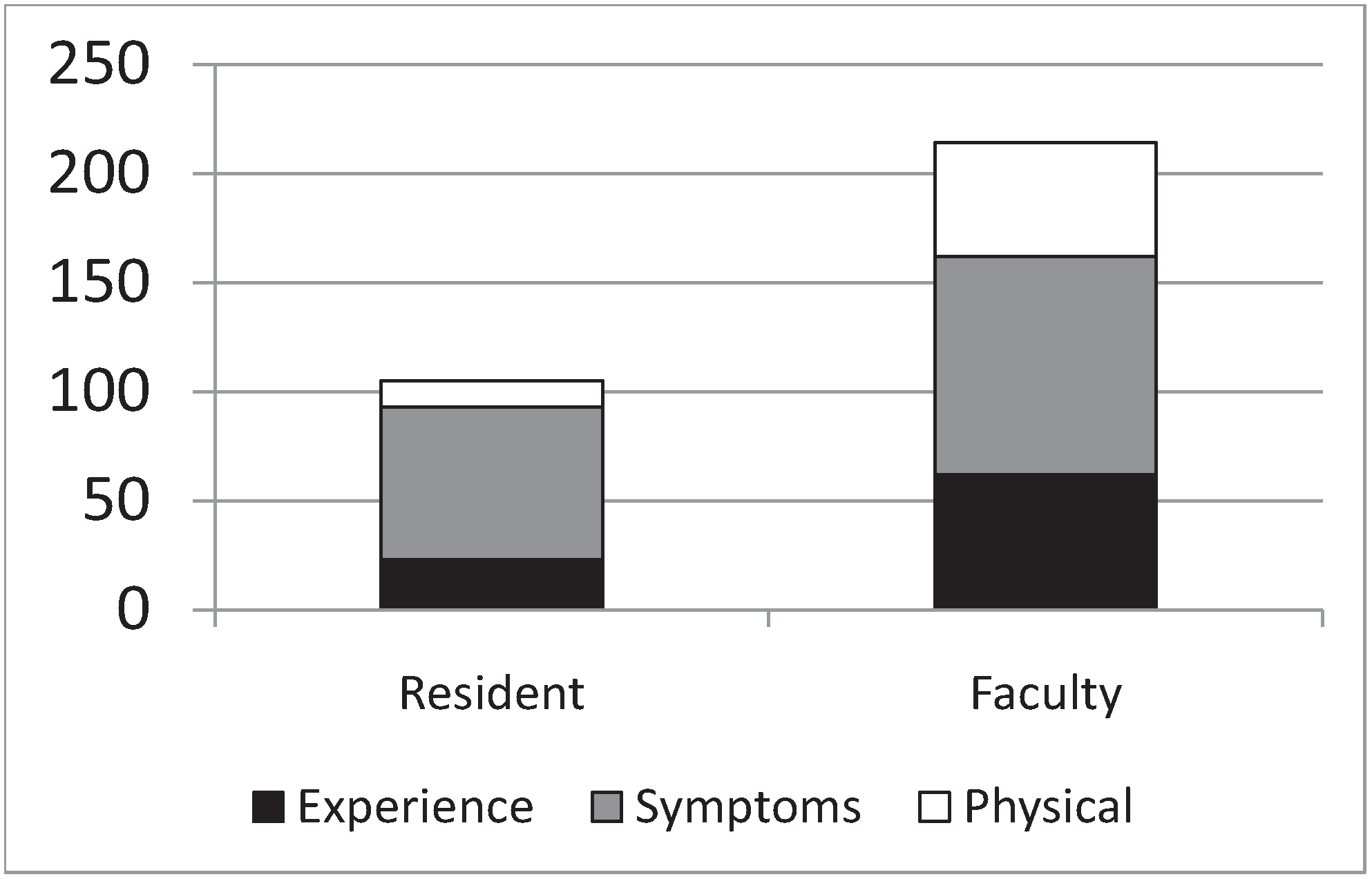
| Experience | Referral to personal experience by participant as a guide for diagnostic thinking. |
| Group Identity | Where participants refer to or include a “we” or group identifier to their language. |
| Logic | Where some effort is made to formalize an argument for a diagnosis. |
| Patient History | Where the participant explicitly refers to patient history to help them make a diagnosis. |
| Physical Exam | Explicit specific reference to the physical exam as the source of information for the diagnosis. |
| Recognition of Case Complexity | Where there is reference to two or more target diagnoses or other complex factors complicating accurate response to the diagnostic question. |
| Rule Based Response | Participants rely on a general rule or algorithm to respond completely to the question. |
| Social Context | Commentary or conversation around the broader implications of a diagnosis. Intersection of diagnosis and wider social world. |
| Struggling with Disease Definition | Where the participant appears to struggle with the definition or list of disease or diagnosis. |
| Symptoms | Participant refers to the symptoms associated with an ailment. |
| Technical Definition | Using any terminology most lay persons wouldn’t know. |
| Tests | Participant language that suggests or refers to some sort of test to determine diagnosis. |
| Treatment | A referral by the participant to a medical intervention. |
| Memory Episodes | PM | MS1 | MS3 | R2 | F |
|---|---|---|---|---|---|
| Episodic | 20 | 4 | 20 | 21 | 18 |
| Semantic | 6 | 6 | 34 | 59 | 72 |
| Explanation | 1 | 1 | 4 | 9 | 6 |
| Prediction | 0 | 0 | 5 | 10 | 3 |
| Prototype | 4 | 3 | 12 | 25 | 40 |
| Qualifier | 1 | 2 | 13 | 15 | 23 |
- Example 6 (MS1) “I’ll never be able to learn that much… but something that’s really helped, knowing people who have done it. I mean the fact that there are doctors, doctors exist, so it must be possible”.
- Example 7 (MS1) “I may have seen cardiac enzymes but, you know, that kind of went in one ear and then came out on the exam”.
- Example 8 (MS1) “My exposure has been limited… although there is some, because… you know, I’ve-I’ve been told to listen for the crackling in the lungs… maybe it’s not crackling in the lungs, in which case it’s my [pause] misperception”.
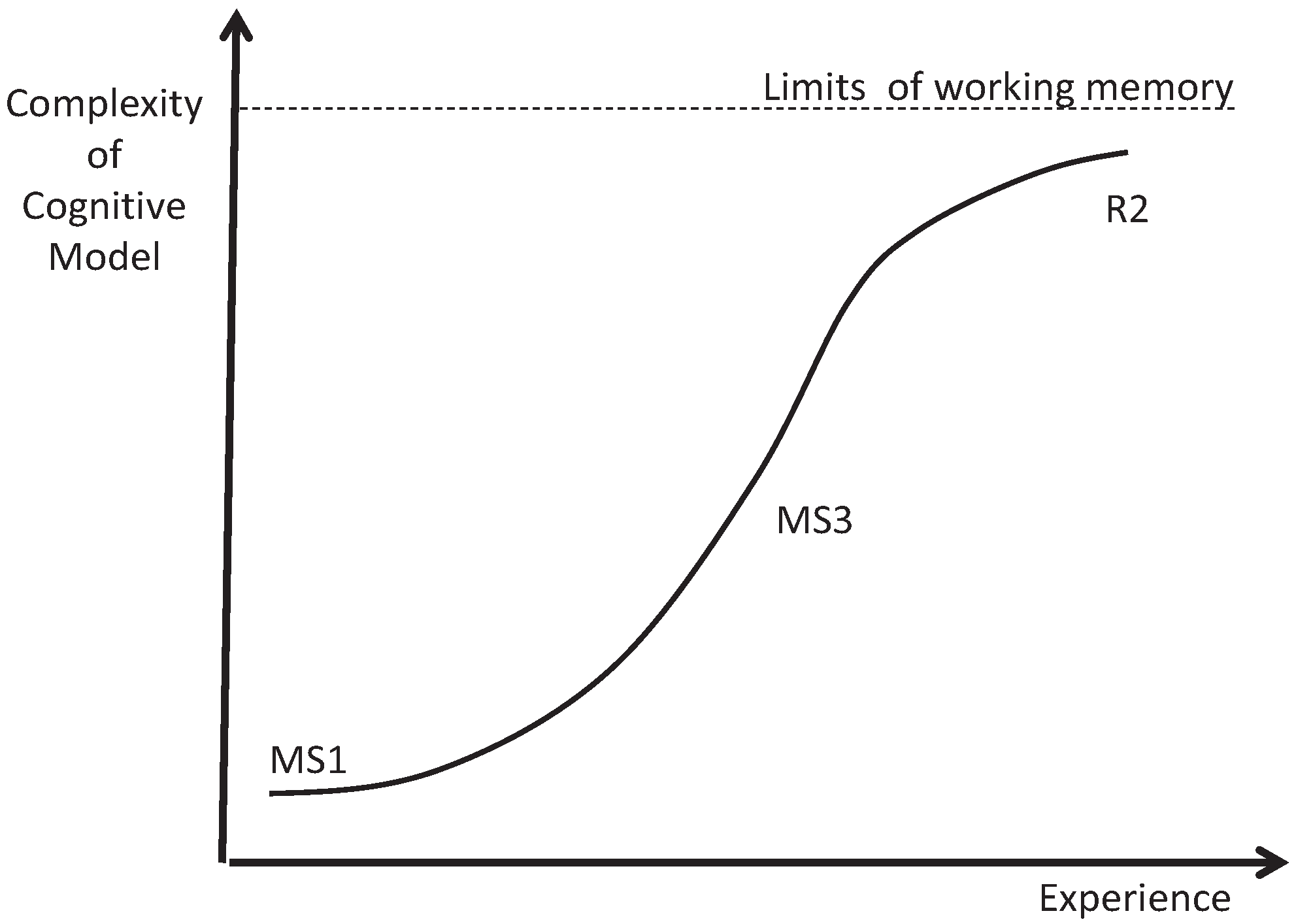
3.2. Intermediates: Logistic Growth
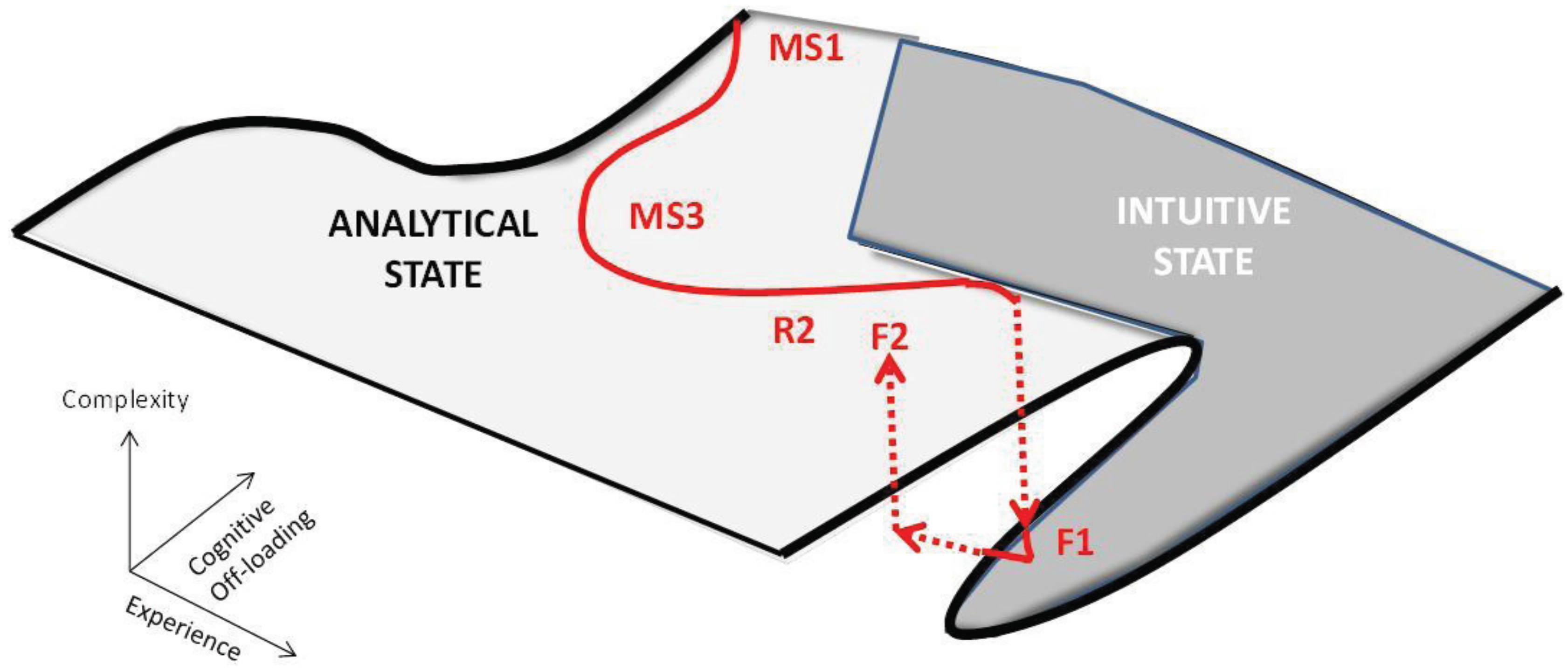
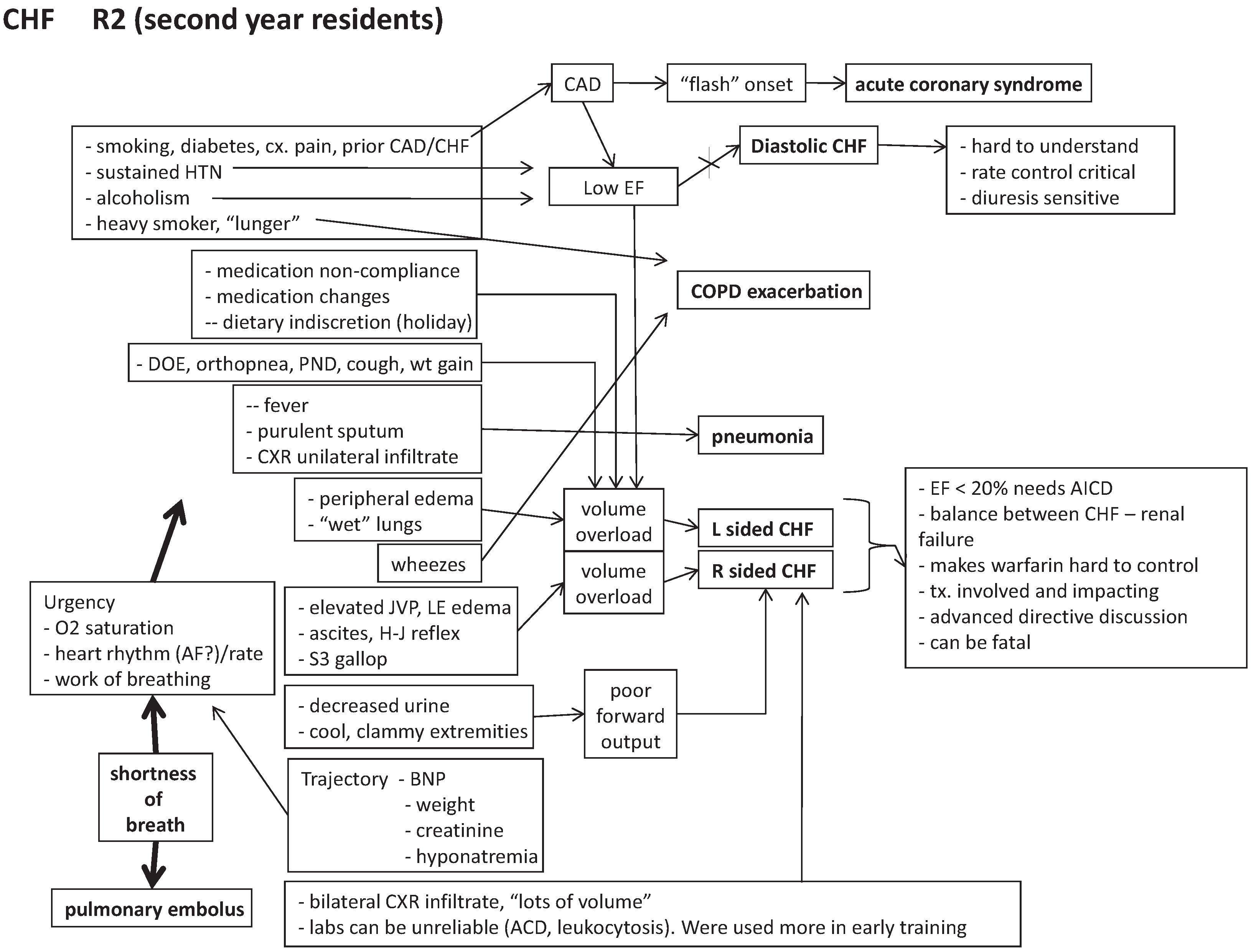
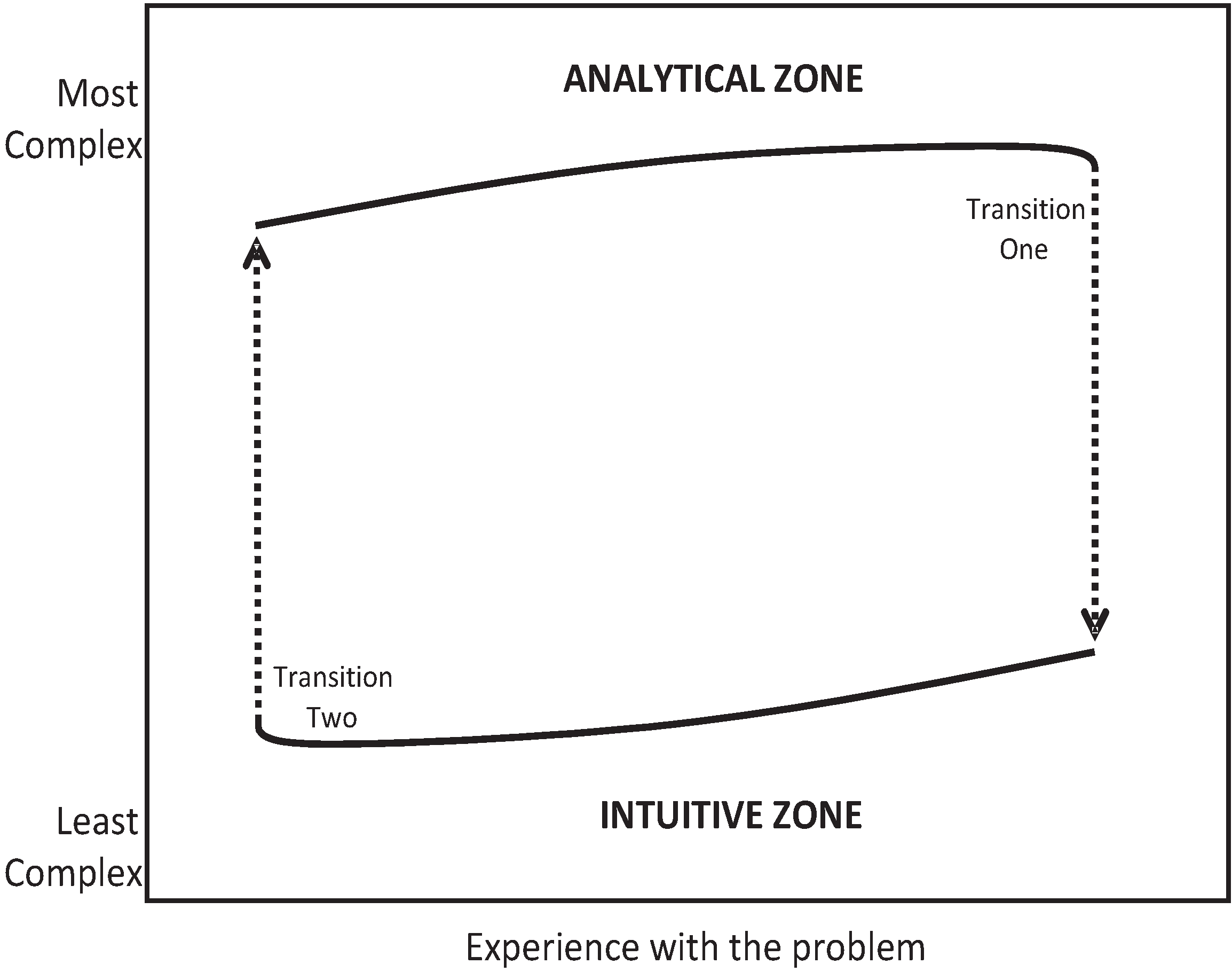
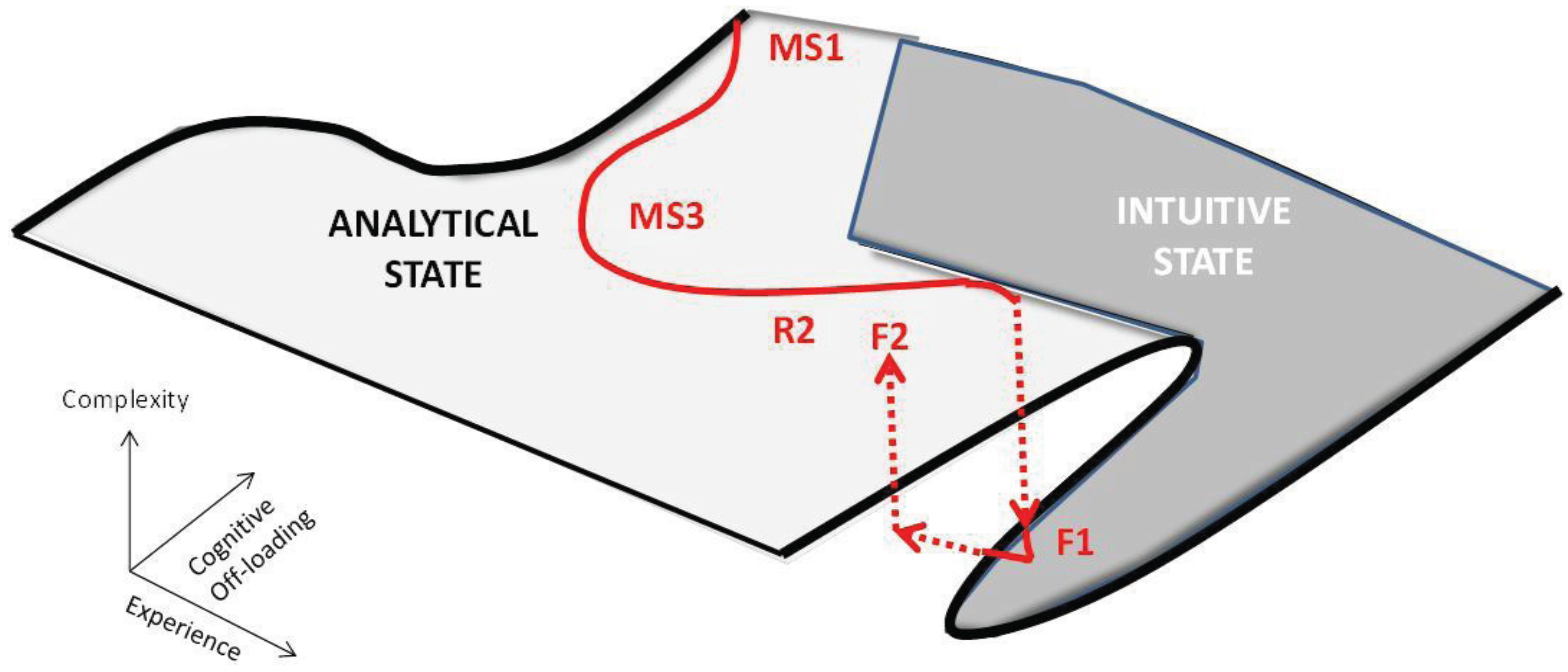
3.3. Experts: Cognitive State Transition
- Example 9 (R2) “My last call, one patient had diastolic heart failure and had gained like 25 pounds, and they were not able to diurese him [as an outpatient]… The essential part here was to control his heart rate so the Lasix could start working.” (episodic memory supporting the rule diastolic heart failure ➔ control heart rate).
- Example 10 (R2) “I had a patient in clinic last week who presented with a weight gain of 25 pounds… (episodic memory) The classic is they have a trigger: Thanksgiving dinner, missing their medications, a small heart attack.” (semantic memory: explanations).
- Example 11 (F) “My wife and I were having dinner at some friend’s house… She was a 26 year old woman who had twins about four weeks before and [we] were carrying on a conversation… something was bothering me… I looked over and realized she had Cheyne-Stokes breathing… Turns out she had post-partum congestive cardiomyopathy.” (episodic memory, unfamiliar cause of heart failure anchored to semantic qualifier for environmental information, Cheyne-Stokes breathing).
- Example 12 (F) “I was working in a small town, around 6000 [people], in the mountains. It was July, black fly season, and a woman came in with all the classic signs of pneumonia: cough, shortness of breath and fever and the classic physical findings, but it was the wrong season… I rechecked the chart and noticed she had Faget’s sign (pulse-temperature disparity)… she had Legionella.” (episodic memory, unfamiliar cause of pneumonia anchored to semantic qualifier for environmental information, Faget’s sign).
- Example 13 (F) “I haven’t had any really clear cut [cases of pneumonia] in the [last] two weeks. The ones that I admitted as a fellow are kinda blurring together into an archetype… you know, the person coming in without another explanatory cause who has fevers, respiratory symptoms, maybe some hypoxia, an infiltrate on their x-ray” (semantic memory: prototype).
- Example 14 (F) “Well, I see that in the clinic every week, I mean, it’s just numerous examples. I don’t remember a specific one… but they’re breathless by the time they get to your exam room, from the waiting room. I usually go out and get patients just ‘cause we have only one [exam] room and I typically have to walk slower and they’re pulling their oxygen bottle. Some of them kind of reek of cigarette smoke… I have a quite a few, [that are] pretty advanced, and typically they’re thin and, [the] spouse does most of the talking ‘cause the-patient gets breathless” (semantic memory: prototype).
4. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Boshuizen, H.P.A.; Schmidt, H.G. On the role of biomedical knowledge in clinical reasoning by experts, intermediates, and novices. Cogn. Sci. 1992, 16, 153–184. [Google Scholar] [CrossRef]
- Patel, V.L.; Groen, G.J. Developmental Accounts of the transition from medical student to doctor: Some problems and suggestions. Med. Educ. 1991, 25, 527–538. [Google Scholar]
- Elstein, A.S.; Shulman, L.S.; Sprafka, S.A. Medical Problem Solving: An Analysis of Clinical Reasoning; Harvard University Press: Cambridge, MA, USA, 1978. [Google Scholar]
- Joseph, G.M.; Patel, V.L. Domain knowledge and hypothesis generation in diagnostic reasoning. Med. Decis. Mak. 1990, 10, 31–46. [Google Scholar] [CrossRef]
- Groves, M.; O’Rourke, P.; Alexander, H. The clinical reasoning characteristics of diagnostic experts. Med. Teach. 2003, 25, 308–313. [Google Scholar] [CrossRef]
- Regehr, G.; Norman, G.R. Issues in cognitive psychology: Implications for professional education. Acad. Med. 1996, 71, 988–1001. [Google Scholar] [CrossRef]
- Schmidt, H.G.; Norman, G.R.; Boshuizen, H.P.A. A Cognitive perspective on medical expertise: Theory and implications. Acad. Med. 1990, 65, 611–621. [Google Scholar] [CrossRef]
- Bordage, G. Elaborated Knowledge: A key to successful diagnostic thinking. Acad. Med. 1994, 69, 883–885. [Google Scholar] [CrossRef]
- Schmidt, H.G.; Rikers, R.M.J.P. How expertise develops in medicine: Knowledge encapsulation and illness scritp formation. Med. Educ. 2007, 41, 1133–1139. [Google Scholar]
- Bordage, G.; Lemieux, M. Semantic structures and diagnostic thinking of experts and novices. Acad. Med. 1991, 66, s70–s72. [Google Scholar] [CrossRef]
- Bordage, G.; Zacks, R. The structure of medical knowledge in the memories of medical students and general practitioners: categories and prototypes. Med. Educ. 1994, 18, 406–416. [Google Scholar] [CrossRef]
- Kushniruk, A.W.; Patel, V.L.; Marley, A.A.J. Small worlds and medical expertise: Implications for medical cognition and knowledge engineering. Int. J. Med. Inform. 1998, 49, 255–271. [Google Scholar] [CrossRef]
- Feltovich, P.J.; Johnson, P.E.; Moller, J.A.; Swanson, D.B. The role and development of medical knowledge and diagnostic expertise. In Readings in Medical Artificial Intelligence; Clancey, W.J., Shortliffe, E.H., Eds.; Addison-Wesley: Reading, MA, USA, 1984; Chapter 12; p. 7. [Google Scholar]
- Coderre, S.; Mandin, H.; Harasym, P.H.; Fick, G.H. Diagnostic reasoning strategies and diagnostic success. Med. Educ. 2003, 37, 695–703. [Google Scholar] [CrossRef]
- Charlin, B.; Boshuizen, H.P.A.; Custers, E.J.; Feltovich, P.J. Scripts and clinical reasoning. Med. Educ. 2007, 41, 1178–1184. [Google Scholar] [CrossRef]
- Rowlands, M. The New Science of the Mind: From Extended Mind to Embodied Phenomenology; Bradford Books/MIT Press: Cambridge, MA, USA, 2010. [Google Scholar]
- Gibson, J.J. The Ecological Approach to Visual Perception; Houghton Mifflin: Boston, MA, USA, 1979. [Google Scholar]
- Reed, E.S. Encountering the World: Toward an Ecological Psychology; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- Durning, S.J.; Artino, A.R. Situativity Theory: A perspective on how participants and the environment can interact. Med. Teach. 2011, 33, 188–199. [Google Scholar] [CrossRef]
- Durning, S.J.; Artino, A.R.; Schuwirth, L.; van der Vleuten, C. Clarifying assumptions to enhance our understanding and assessment of clinical reasoning. Acad. Med. 2013, 88, 1–7. [Google Scholar] [CrossRef]
- Bereiter, C.; Scardemalia, M. Surpassing Ourselves. An Inquiry into the Nature and Implications of Expertise; Open Court: Chicago, IL, USA, 1993. [Google Scholar]
- Klein, G. Sources of Power. How People Make Decisions; MIT Press: Cambridge, MA, USA, 1998. [Google Scholar]
- Kahneman, D. A perspective on judgment and choice. Mapping bounded rationality. Am. Psychol. 2003, 58, 697–720. [Google Scholar] [CrossRef]
- Reyna, V.F. A theory of medical decision making and health: Fuzzy trace theory. Med. Decis. Mak. 2008, 28, 850–865. [Google Scholar] [CrossRef]
- Schultz, W. Predictive reward signal of dopamine neurons. J. Neurophysiol. 1998, 80, 1–27. [Google Scholar]
- Hollerman, J.R.; Schultz, W. Dopamine neurons report an error in the temporal prediction of reward during learning. Nat. Neurosci. 1998, 1, 304–309. [Google Scholar] [CrossRef]
- Boyd, B. On the Origin of Stories: Evolution, Cognition, and Fiction; Belknap Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Siegel, D.J. The Developing Mind; The Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Pennington, N.; Hastie, R. The story model for juror decision making. In Inside the Juror: The Psychology of Juror Decision Making; Hastie, R., Ed.; Cambridge University Press: New York, NY, USA, 1993. [Google Scholar]
- Daley, B.J.; Torre, D.M. Concept maps in medical education: An analytical literature review. Med. Educ. 2010, 44, 440–448. [Google Scholar] [CrossRef]
- Kring, A.M.; Sloan, D.M. The facial expression coding system (FACES): Development, validation, and utility. Psychol. Assess 2007, 19, 210–224. [Google Scholar] [CrossRef]
- Hebb, D.O. The Organization of Behavior; Wiley & Sons: New York, NY, USA, 1949. [Google Scholar]
- Miller, G.A. The magical number seven, plus or minus two: Some limits on our capacity for processing information. Psychol. Rev. 1956, 63, 81–97. [Google Scholar] [CrossRef]
- Marian, D. The Correspondence Theory of Truth. Available online: http://plato.stanford.edu/archives/fall2009/entries/truth-correspondence/ (accessed on 3 March 2014).
- Young, J.O. The Coherence Theory of Truth. Available online: http://plato.stanford.edu/archives/fall2008/entries/truth-coherence/ (accessed on 3 March 2014).
- Scheffer, M. Critical Transitions in Nature and Society; Princeton University Press: Princeton, NJ, USA, 2009. [Google Scholar]
Appendix

© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Smith, C.S.; Hill, W.; Francovich, C.; Morris, M.; Robbins, B.; Robins, L.; Turner, A. Diagnostic Reasoning across the Medical Education Continuum. Healthcare 2014, 2, 253-271. https://doi.org/10.3390/healthcare2030253
Smith CS, Hill W, Francovich C, Morris M, Robbins B, Robins L, Turner A. Diagnostic Reasoning across the Medical Education Continuum. Healthcare. 2014; 2(3):253-271. https://doi.org/10.3390/healthcare2030253
Chicago/Turabian StyleSmith, C. Scott, William Hill, Chris Francovich, Magdalena Morris, Bruce Robbins, Lynne Robins, and Andrew Turner. 2014. "Diagnostic Reasoning across the Medical Education Continuum" Healthcare 2, no. 3: 253-271. https://doi.org/10.3390/healthcare2030253
APA StyleSmith, C. S., Hill, W., Francovich, C., Morris, M., Robbins, B., Robins, L., & Turner, A. (2014). Diagnostic Reasoning across the Medical Education Continuum. Healthcare, 2(3), 253-271. https://doi.org/10.3390/healthcare2030253