
The Effects of a Home-Based Cardiac Rehabilitation Program via the Line Application on Functional Capacity and Quality of Life Among Open-Heart Surgery Patients: A Quasi-Experimental Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Sample
2.3. Sample Size
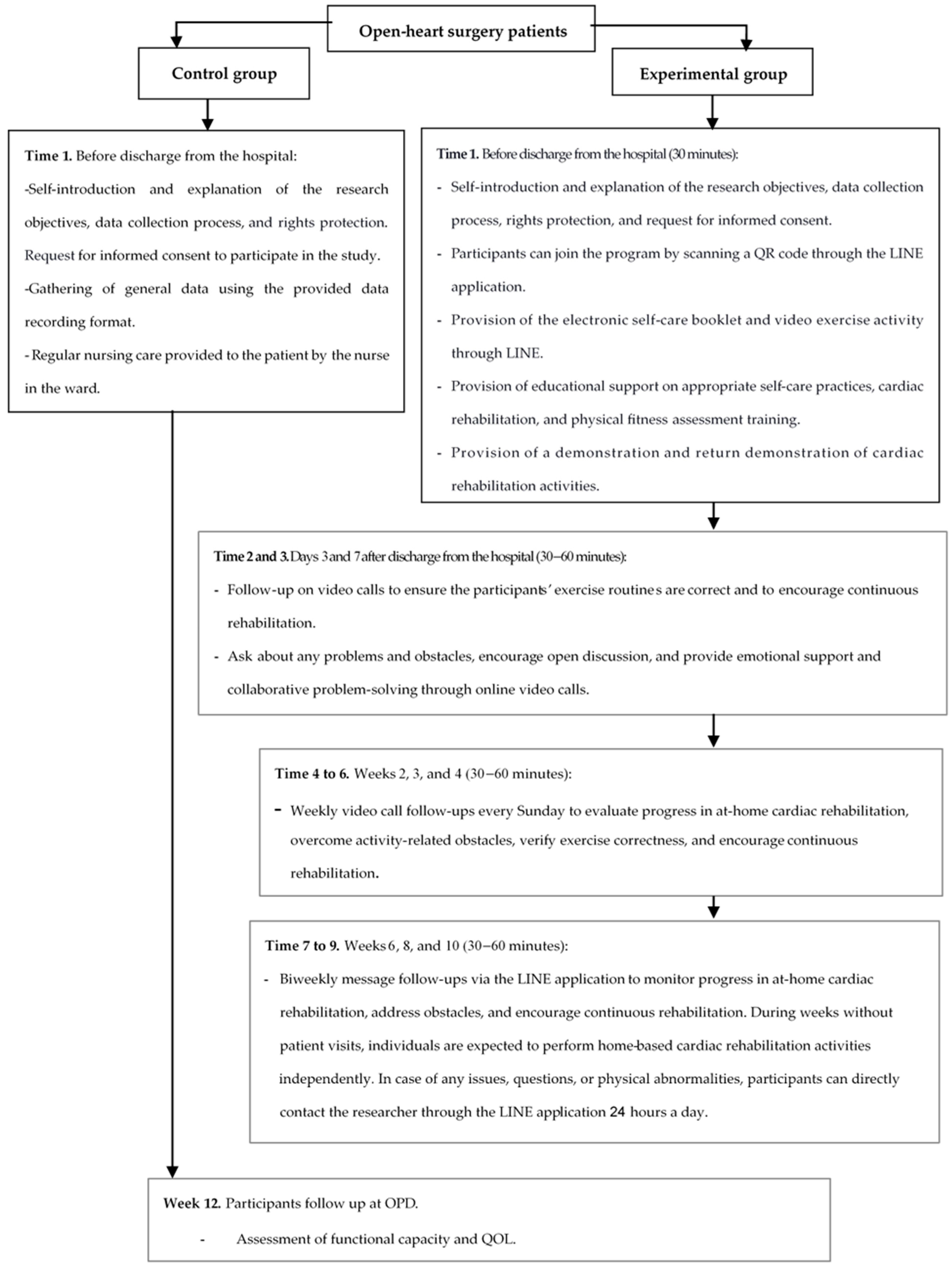
2.4. Research Procedures
2.4.1. Intervention
2.4.2. Standard Care
2.5. Research Instruments
2.6. Ethical Considerations
2.7. Statistic Analysis
3. Results
3.1. Functional Capacity
3.2. Quality of Life Among Open-Heart Surgery Patients
4. Discussion
Limitations and Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases 2021. Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 (accessed on 3 October 2021).
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart Disease and Stroke Statistics—2014 Update. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed]
- Thai Heart Association of Thailand Under The Royal Patronage of H.M. The King. Guideline for Ischemic Heart Disease; Srimuang Printing: Bangkok, Thailand, 2014. [Google Scholar]
- Division of Non-Communicable Diseases. Number and Mortality Rate, Noncommunicable Diseases Year 2019–2021 Ministry of Public Health Thailand: Ministry of Public Health Thailand; 2023. Available online: http://www.thaincd.com/2016/mission/documents-detail.phpz?id=14480&tid=32&gid=1-020 (accessed on 29 April 2024).
- Thoracic Surgeons Association of Thailand. Statistics on Heart Surgery in Thailand in 2023 2024. Available online: https://www.thaists.or.th/download-category/statistics-on-heart-surgery-in-thailand// (accessed on 1 June 2024).
- Hokkanen, M.; Huhtala, H.; Laurikka, J.; Järvinen, O. The effect of postoperative complications on health-related quality of life and survival 12 years after coronary artery bypass grafting—A prospective cohort study. J. Cardiothorac. Surg. 2021, 16, 173. [Google Scholar] [CrossRef]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Kitzman, D.W.; Sanderson, B.K.; Whooley, M.A. Home-Based Cardiac Rehabilitation: A Scientific Statement From the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. J. Am. Coll. Cardiol. 2019, 74, 133–153. [Google Scholar] [CrossRef]
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat. Rev. Cardiol. 2022, 19, 180–194. [Google Scholar] [CrossRef]
- Anchah, L.; Hassali, M.A.; Lim, M.S.; Ibrahim, M.I.; Sim, K.H.; Ong, T.K. Health related quality of life assessment in acute coronary syndrome patients: The effectiveness of early phase I cardiac rehabilitation. Health Qual. Life Outcomes 2017, 15, 10. [Google Scholar] [CrossRef]
- Chen, Y.W.; Wang, C.Y.; Lai, Y.H.; Liao, Y.C.; Wen, Y.K.; Chang, S.T.; Huang, J.L.; Wu, T.J. Home-based cardiac rehabilitation improves quality of life, aerobic capacity, and readmission rates in patients with chronic heart failure. Medicine 2018, 97, e9629. [Google Scholar] [CrossRef] [PubMed]
- Paorod, P.; Chidnok, W.; Sayasathid, J. The effectiveness of cardiac rehabilitation program in open heart surgery patients at Heart Clinic, Naresuan University Hospital. J. R. Thai Army Nurses 2020, 21, 255–261. [Google Scholar]
- Pirruccello, J.P.; Traynor, K.; Aragam, K.G. “Road Map” to Improving Enrollment in Cardiac Rehabilitation: Identifying Barriers and Evaluating Alternatives. J. Am. Heart Assoc. 2017, 6, e007468. [Google Scholar] [CrossRef]
- Platz, K.; Kools, S.; Howie-Esquivel, J. Benefits, Facilitators, and Barriers of Alternative Models of Cardiac Rehabilitation: A Qualitative Systematic Review. J. Cardiopulm. Rehabil. Prev. 2023, 43, 83–92. [Google Scholar] [CrossRef]
- Chindhy, S.; Taub, P.R.; Lavie, C.J.; Shen, J. Current challenges in cardiac rehabilitation: Strategies to overcome social factors and attendance barriers. Expert. Rev. Cardiovasc. Ther. 2020, 18, 777–789. [Google Scholar] [CrossRef]
- Paorod, P.; Chidnok, W.; Sayasathid, J. Effect of home-based cardiac rehabilitation program on exercise capacity in open heart surgery patients at Naresuan university hospital. Songklanagarind Med. J. 2017, 35, 285–291. [Google Scholar] [CrossRef]
- Arjunan, P.; D’Souza, M.S. Efficacy of nurse-led cardiac rehabilitation on health care behaviours in adults with chronic heart failure: An experimental design. Clin. Epidemiol. Glob. Health 2021, 12, 100859. [Google Scholar] [CrossRef]
- Ruan, T.; Xu, M.; Zhu, L.; Ding, Y. Nurse-coordinated home-based cardiac rehabilitation for patients with heart failure: A scoping review. Int. J. Nurs. Sci. 2023, 10, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Ge, C.; Shi, Y.; Xu, Y.; Zhao, C.; Gao, L.; Wen, D.; Li, T.; Wang, J.; Yan, S.; et al. Chinese Home-Based Cardiac Rehabilitation Model Delivered by Smartphone Interaction Improves Clinical Outcomes in Patients with Coronary Heart Disease. Front. Cardiovasc. Med. 2021, 8, 731557. [Google Scholar] [CrossRef] [PubMed]
- Santiago de Araújo Pio, C.; Beckie, T.M.; Varnfield, M.; Sarrafzadegan, N.; Babu, A.S.; Baidya, S.; Buckley, J.; Chen, S.Y.; Gagliardi, A.; Heine, M.; et al. Promoting patient utilization of outpatient cardiac rehabilitation: A joint International Council and Canadian Association of Cardiovascular Prevention and Rehabilitation position statement. Int. J. Cardiol. 2020, 298, 1–7. [Google Scholar] [CrossRef]
- Tahsin, F.; Armas, A.; Kirakalaprathapan, A.; Kadu, M.; Sritharan, J.; Steele Gray, C. Information and Communications Technologies Enabling Integrated Primary Care for Patients With Complex Care Needs: Scoping Review. J. Med. Internet Res. 2023, 25, e44035. [Google Scholar] [CrossRef]
- Su, J.J.; Yu, D.S.F. Effectiveness of eHealth cardiac rehabilitation on health outcomes of coronary heart disease patients: A randomized controlled trial protocol. BMC Cardiovasc. Disord. 2019, 19, 274. [Google Scholar] [CrossRef]
- Saelim, S. Usage Behavior Line Application of Elderly in Bangkok Area. Master’s Thesis, Thammasat University, Bangkok, Thailand, 2015. [Google Scholar]
- Polhan, B.; Wattanakitkrileart, D.; Pongthavornkamol, K. The Effects of Education and Inhaler Skills Program through Line Application on Symptom Control among Asthmatic Patient. J. R. Thai Army Nurses 2019, 20, 93–103. [Google Scholar]
- Booncherd, C. Follow-up for Disabled, Bedridden, Cancer Patients and Primary Pharmaceutical Care by Using the LINE Application in Kut Chum District, Yasothon Province. J. Health Sci. Thail. 2018, 27, 920–926. [Google Scholar]
- Orem, D.E.; Taylor, S.G.; Renpenning, K.M. Nursing: Concepts of Practice, 6th ed.; Mosby: St. Louis, MI, USA, 2001. [Google Scholar]
- Morisawa, T.; Ueno, K.; Fukuda, Y.; Kanazawa, N.; Kawaguchi, H.; Zaiki, R.; Fuzisaki, H.; Yoshioka, H.; Sasaki, M.; Iwata, K.; et al. Significance of sequential cardiac rehabilitation program through inter-hospital cooperation between acute care and rehabilitation hospitals in elderly patients after cardiac surgery in Japan. Heart Vessels. 2017, 32, 1220–1226. [Google Scholar] [CrossRef]
- Paneroni, M.; Scalvini, S.; Corrà, U.; Lovagnini, M.; Maestri, R.; Mazza, A.; Raimondo, R.; Agostoni, P.; La Rovere, M.T. The Impact of Cardiac Rehabilitation on Activities of Daily Life in Elderly Patients with Heart Failure. Front. Physiol. 2021, 12, 785501. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.N.; Kamat, H.; Ganjiwale, J. The functional capacity of the patients after open heart surgery following physiotherapy utilizing inspiratory muscle training. Int. J. Med. Sci. Public Health 2020, 9, 563–568. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Kobkitsumongkol, K.; Uaaree, P.; Voraakom, A.; Sanjaroensuttikun, N. Clinical outcome in cardiac rehabilitation patients of Ramathibodi university hospital. J. Health Nurs. Res. 2011, 27, 1–13. Available online: https://he01.tci-thaijo.org/index.php/bcnbangkok/article/view/4824 (accessed on 3 October 2021).
- McMahon, S.R.; Ades, P.A.; Thompson, P.D. The role of cardiac rehabilitation in patients with heart disease. Trends Cardiovasc. Med. 2017, 27, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Schopfer, D.W.; Whooley, M.A.; Allsup, K.; Pabst, M.; Shen, H.; Tarasovsky, G.; Duvernoy, C.S.; Forman, D.E. Effects of Home-Based Cardiac Rehabilitation on Time to Enrollment and Functional Status in Patients With Ischemic Heart Disease. J. Am. Heart Assoc. 2020, 9, e016456. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A.G. Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Nakon, O.; Sindhu, S.; Tansawatdi, R. Effectiveness of a Hospital-Based Comprehensive Cardiac Rehabilitation Program on Postoperative Recovery of Patients Undergoing Coronary Artery Bypass Grafting. Nurs. Sci. J. Thail. 2015, 33, 51–64. [Google Scholar]
- The Heart Association of Thailand Under the Royal Patronage of H.M. the King. Cardiac Rahabilitation Guideline 2010. Available online: http://www.thaiheart.org/images/column_1291454908/RehabGuideline.pdf (accessed on 20 June 2022).
- Hlatky, M.A.; Boineau, R.E.; Higginbotham, M.B.; Lee, K.L.; Mark, D.B.; Califf, R.M.; Cobb, F.R.; Pryor, D.B. A brief self-administered questionnaire to determine functional capacity (the Duke Activity Status Index). Am. J. Cardiol. 1989, 64, 651–654. [Google Scholar] [CrossRef]
- Fan, X.; Lee, K.S.; Frazier, S.K.; Lennie, T.A.; Moser, D.K. Psychometric testing of the Duke Activity Status Index in patients with heart failure. Eur. J. Cardiovasc. Nurs. 2015, 14, 214–221. [Google Scholar] [CrossRef]
- Numpijit, N.; Jitpraphai, C.; Kantaratanakul, V.; Eararee, P.; Kobkitsumongkol, K. Effects of Second Stage Cardiac Rehabilitation and Factors Relating to Exercise Role in Heart Failure at Ramathibodi Hospital. Ramathibodi Nurs. J. 2000, 6, 142–153. [Google Scholar]
- Leurmarnkul, W.; Meetam, P. Properties Testing of the Retranslated SF-36 (Thai Version). Thai J. Pharm. Sci. 2005, 29, 69–88. [Google Scholar] [CrossRef]
- Jenkinson, C.; Stewart-Brown, S.; Petersen, S.; Paice, C. Assessment of the SF-36 version 2 in the United Kingdom. J. Epidemiol. Community Health 1999, 53, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.L.; Seubsman, S.A.; Sleigh, A. Thai SF-36 health survey: Tests of data quality, scaling assumptions, reliability and validity in healthy men and women. Health Qual. Life Outcomes 2008, 6, 52. [Google Scholar] [CrossRef]
- Krittayaphong, R.; Bhuripanyo, K.; Raungratanaamporn, O.; Chotinaiwatarakul, C.; Chaowalit, N.; Punlee, K.; Kangkagate, C.; Chaithiraphan, S. Reliability of Thai version of SF-36 questionnaire for the evaluation of quality of life in cardiac patients. J. Med. Assoc. Thai. 2000, 83 (Suppl. S2), S130–S136. [Google Scholar]
- Prabhu, N.V.; Maiya, A.G.; Prabhu, N.S. Impact of Cardiac Rehabilitation on Functional Capacity and Physical Activity after Coronary Revascularization: A Scientific Review. Cardiol. Res. Pract. 2020, 2020, 1236968. [Google Scholar] [CrossRef]
- Uddin, J.; Joshi, V.L.; Moniruzzaman, M.; Karim, R.; Uddin, J.; Siraj, M.; Rashid, M.A.; Rossau, H.K.; Taylor, R.S.; Zwisler, A.D. Effect of Home-Based Cardiac Rehabilitation in a Lower-Middle Income Country: Results from a controlled trial. J. Cardiopulm. Rehabil. Prev. 2020, 40, 29–34. [Google Scholar] [CrossRef]
- Prasada, S.; Rambarat, C.; Winchester, D.; Park, K. Implementation and Impact of Home-Based Cardiac Rehabilitation in a Veterans Affair Medical Center. Mil. Med. 2020, 185, 859–863. [Google Scholar] [CrossRef]
- Buckingham, S.A.; Taylor, R.S.; Jolly, K.; Zawada, A.; Dean, S.G.; Cowie, A.; Norton, R.J.; Dalal, H.M. Home-based versus centre-based cardiac rehabilitation: Abridged Cochrane systematic review and meta-analysis. Open Heart. 2016, 3, e000463. [Google Scholar] [CrossRef]
- Cristo, D.D.; Nascimento, N.P.D.; Dias, A.S.; Sachetti, A. Telerehabilitation for cardiac patients: Systematic review. Int. J. Cardiovasc. Sci. 2018, 31, 443–450. [Google Scholar] [CrossRef]
- Ricci, M.; Pozzi, G.; Caraglia, N.; Chieffo, D.P.R.; Polese, D.; Galiuto, L. Psychological Distress Affects Performance during Exer-cise-Based Cardiac Rehabilitation. Life 2024, 14, 236. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Experimental Group (n = 27), n (%) | Control Group (n = 27), n (%) | p-Value | |
|---|---|---|---|
| Gender | |||
| Male | 21 (77.8) | 15 (55.6) | 0.803 |
| Female | 6 (22.2) | 12 (44.4) | |
| Age (mean, SD) (Range 22–60, M = 46.98, SD = 10.74) | 46.85 (11.2) | 47.11 (9.8) | 0.646 |
| 21–30 | 4 (14.8) | 1 (3.7) | |
| 31–40 | 4 (14.8) | 6 (22.2) | |
| 41–50 | 5 (18.5) | 9 (33.3) | |
| 51–60 | 14 (51.9) | 11 (40.8) | |
| Marital status | 0.424 | ||
| Single | 6 (22.2) | 3 (11.1) | |
| Married | 19 (70.4) | 23 (85.2) | |
| Windowed | 2 (7.4) | 1 (3.7) | |
| Education background | 0.503 | ||
| Elementary education | 4 (14.8) | 5 (18.5) | |
| Secondary education | 10 (37.0) | 14 (51.9) | |
| Certificate level | 5 (18.5) | 2 (7.4) | |
| Bachelor’s degree or higher | 8 (29.6) | 6 (22.2) | |
| Body Mass Index (kg/m2) (mean, SD) (Range 15.61–38.79, M = 25.69, SD = 5.23) | 25.62 (3.8) | 25.77 (6.4) | 0.436 |
| Occupation | 0.669 | ||
| Unemployed | 5 (18.5) | 5 (18.5) | |
| Government officer | 1 (3.7) | 1 (3.7) | |
| Company employee | 13 (48.2) | 17 (63.0) | |
| Agriculture | 2 (7.4) | 2 (7.4) | |
| Merchant | 5 (18.5) | 1 (3.7) | |
| Other | 1 (3.7) | 1 (3.7) | |
| Diagnosis | 0.432 | ||
| Coronary disease | 11 (40.7) | 8 (29.6) | |
| Valve disease | 15 (55.6) | 18 (66.7) | |
| Vascular and valve disease | 0 | 1 (3.7) | |
| DCM | 1 (3.70) | 0 | |
| Comorbidities * | 0.500 | ||
| No underlying disease | 7 (25.9) | 8 (29.6) | |
| Presence of underlying disease | 20 (74.1) | 19 (70.4) | |
| Hypertension | 15 (55.6) | 17 (51.9) | |
| Diabetes | 5 (18.5) | 7 (25.9) | |
| Hyperlipidemia | 14 (51.9) | 13 (48.2) | |
| Chronic kidney disease | 3 (11.1) | 0 | |
| Other | 11 (40.7) | 5 (18.5) | |
| NYHA Class | 0.189 | ||
| Class I | 4 (14.8) | 8 (29.6) | |
| Class II | 17 (63.0) | 17 (63.0) | |
| Class III | 6 (22.2) | 2 (7.4) | |
| Ejection Fraction (EF) | 0.638 | ||
| EF > 50% | 18 (66.7) | 18 (66.7) | |
| EF 40–50% | 3 (11.1) | 5 (18.5) | |
| EF < 40% | 6 (22.2) | 4 (14.8) | |
| Surgical procedure | 0.198 | ||
| OPCAB | 8 (29.6) | 2 (7.4) | |
| CABG | 3 (11.1) | 4 (14.8) | |
| Valve surgery | 15 (55.6) | 18 (66.7) | |
| Valve surgery + CABG | 0 | 2 (7.4) | |
| Heart transplant | 1 (3.7) | 1 (3.7) | |
| Cardiopulmonary bypass time (hours) (mean, SD) (Range 0–5.00, M = 1.69, SD = 1.16) | 1.55 (1.3) | 1.84 (1.0) | 0.517 |
| Surgery time (hours) (mean, SD) (Range 2.15–9.45, M = 5.37, SD = 1.62) | 5.41 (1.9) | 5.33 (1.4) | 0.500 |
| Length of stay (days) (mean, SD) (Range 5–23, M = 10.63, SD = 3.32) | 10.96 (3.2) | 10.30 (3.5) | 0.452 |
| Functional Capacity | Experimental Group (n = 27) | Control Group (n = 27) | Total (n = 54) | t | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| SD | SD | SD | ||||||
| 6 MWT | 377.30 | 77.16 | 326.19 | 47.45 | 351.74 | 68.49 | 2.93 | 0.005 |
| Physical activity | 42.71 | 10.23 | 30.89 | 9.24 | 36.80 | 11.35 | 4.46 | 0.000 |
| Quality of Life | Experimental Group (n = 27) | Control Group (n = 27) | Total (n = 54) | t | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| SD | SD | SD | ||||||
| Physical functioning | 86.48 | 13.07 | 71.48 | 17.48 | 78.99 | 17.06 | 3.57 | 0.001 |
| Physical roles | 93.52 | 16.40 | 90.74 | 18.54 | 92.13 | 17.40 | 0.58 | 0.562 |
| Emotional roles | 98.76 | 6.41 | 90.12 | 18.06 | 94.44 | 14.11 | 2.34 | 0.023 |
| Vitality | 75.37 | 9.08 | 66.11 | 9.74 | 70.74 | 10.43 | 3.61 | 0.001 |
| Mental health | 79.26 | 5.77 | 69.63 | 7.38 | 74.44 | 8.16 | 5.34 | 0.000 |
| Social functioning | 87.96 | 12.73 | 75.93 | 14.26 | 81.94 | 14.70 | 3.27 | 0.002 |
| Bodily pain | 81.57 | 19.82 | 72.22 | 14.94 | 76.90 | 18.01 | 1.96 | 0.056 |
| General health | 71.67 | 13.45 | 50.00 | 17.76 | 60.83 | 19.05 | 5.05 | 0.000 |
| Overall QOL | 674.60 | 65.86 | 586.23 | 76.54 | 630.42 | 83.61 | 4.55 | 0.000 |
| Physical functioning | 86.48 | 13.07 | 71.48 | 17.48 | 78.99 | 17.06 | 3.57 | 0.001 |
| Physical roles | 93.52 | 16.40 | 90.74 | 18.54 | 92.13 | 17.40 | 0.58 | 0.562 |
| Emotional roles | 98.76 | 6.41 | 90.12 | 18.06 | 94.44 | 14.11 | 2.34 | 0.023 |
| Vitality | 75.37 | 9.08 | 66.11 | 9.74 | 70.74 | 10.43 | 3.61 | 0.001 |
| Mental health | 79.26 | 5.77 | 69.63 | 7.38 | 74.44 | 8.16 | 5.34 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saensoda, S.; Pokpalagon, P.; Chaiviboontham, S. The Effects of a Home-Based Cardiac Rehabilitation Program via the Line Application on Functional Capacity and Quality of Life Among Open-Heart Surgery Patients: A Quasi-Experimental Study. Healthcare 2025, 13, 1051. https://doi.org/10.3390/healthcare13091051
Saensoda S, Pokpalagon P, Chaiviboontham S. The Effects of a Home-Based Cardiac Rehabilitation Program via the Line Application on Functional Capacity and Quality of Life Among Open-Heart Surgery Patients: A Quasi-Experimental Study. Healthcare. 2025; 13(9):1051. https://doi.org/10.3390/healthcare13091051
Chicago/Turabian StyleSaensoda, Suteetida, Piyawan Pokpalagon, and Suchira Chaiviboontham. 2025. "The Effects of a Home-Based Cardiac Rehabilitation Program via the Line Application on Functional Capacity and Quality of Life Among Open-Heart Surgery Patients: A Quasi-Experimental Study" Healthcare 13, no. 9: 1051. https://doi.org/10.3390/healthcare13091051
APA StyleSaensoda, S., Pokpalagon, P., & Chaiviboontham, S. (2025). The Effects of a Home-Based Cardiac Rehabilitation Program via the Line Application on Functional Capacity and Quality of Life Among Open-Heart Surgery Patients: A Quasi-Experimental Study. Healthcare, 13(9), 1051. https://doi.org/10.3390/healthcare13091051