

Full-Mouth Digital Dental Rehabilitation Under General Anesthesia in a Post-Treatment Intraoral Squamous Cell Carcinoma Patient: A Case Report


Abstract
1. Introduction
2. Case Report
2.1. Patient Information
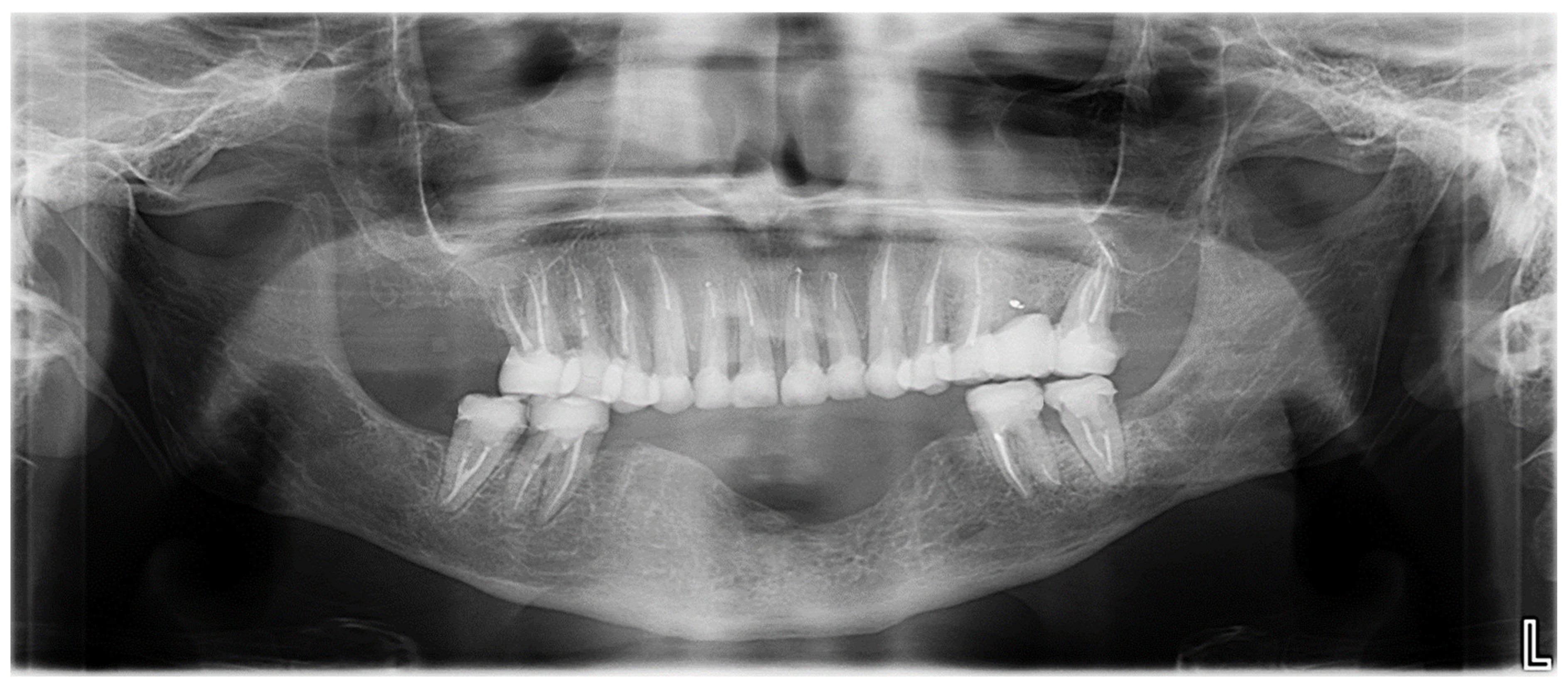
2.2. Clinical History and Diagnostic Assessment
2.3. Therapeutic Goals
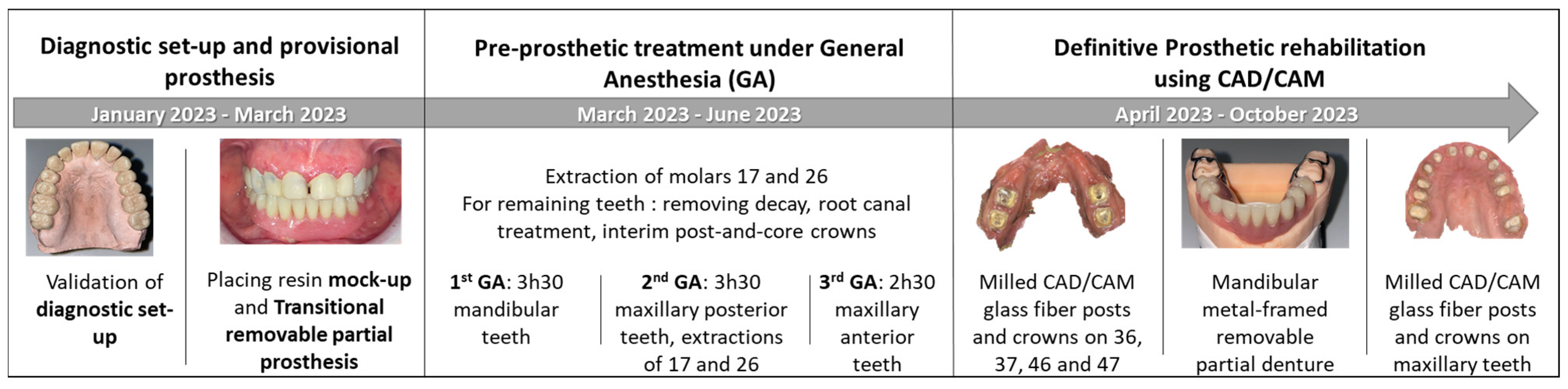
2.4. Intervention and Treatment Process
2.4.1. Step 1: Diagnostic Set-Up and Provisional Prosthesis
2.4.2. Step 2: Pre-Prosthetic Treatment Under General Anesthesia
- First GA session (March 2023, lasted 3 h and 30 min): Pre-prosthetic care for mandibular teeth.
- Second GA session (June 2023, lasted 3 h and 30 min): Pre-prosthetic care for maxillary posterior teeth, and non-traumatic extractions of teeth 17 and 26.
- Third GA session (June 2023, lasted 2 h and 30 min): Pre-prosthetic care for maxillary anterior teeth [9].
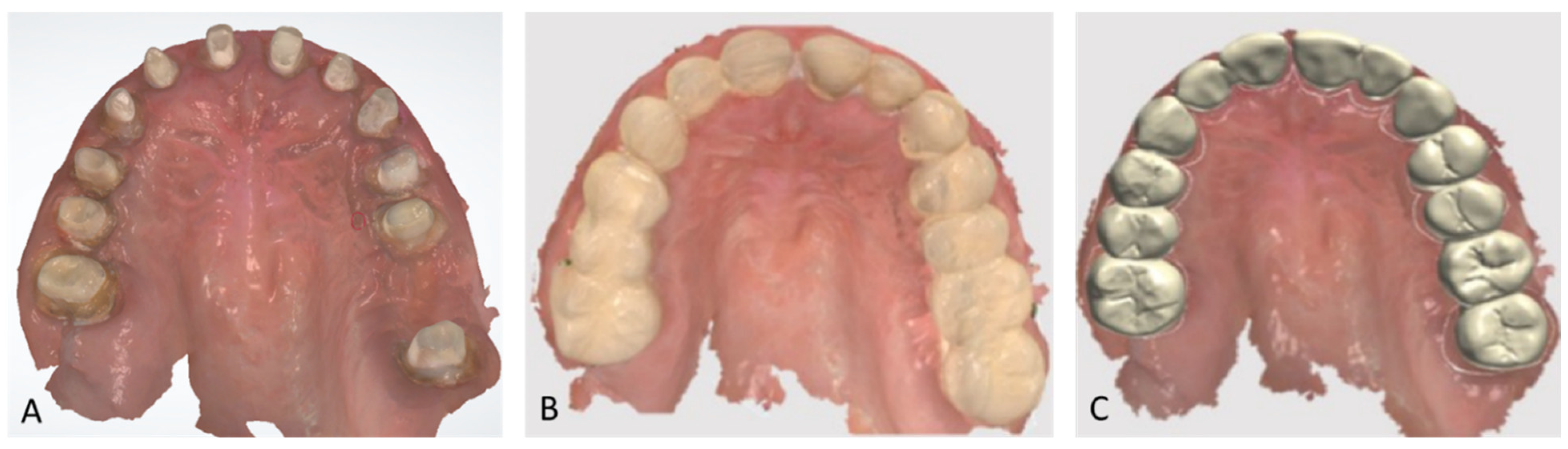
2.4.3. Step 3: Definitive Prosthetic Rehabilitation
2.5. Outcomes and Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vermaire, J.A.; Partoredjo, A.S.K.; de Groot, R.J.; Brand, H.S.; Speksnijder, C.M. Mastication in Health-Related Quality of Life in Patients Treated for Oral Cancer: A Systematic Review. Eur. J. Cancer Care 2022, 31, e13744. [Google Scholar] [CrossRef] [PubMed]
- Depeyre, A.; Pereira, B.; Pham-Dang, N.; Barthélémy, I.; Hennequin, M. Impairments in Food Oral Processing in Patients Treated for Tongue Cancer. Dysphagia 2020, 35, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.; Butterworth, C.; Lowe, D.; Rogers, S.N. Factors Associated with Restricted Mouth Opening and Its Relationship to Health-Related Quality of Life in Patients Attending a Maxillofacial Oncology Clinic. Oral Oncol. 2008, 44, 430–438. [Google Scholar] [CrossRef]
- de Groot, R.J.; Rosenberg, A.J.W.P.; van der Bilt, A.; Aalto, D.; Merkx, M.A.W.; Speksnijder, C.M. The Association between a Mixing Ability Test and Patient Reported Chewing Ability in Patients Treated for Oral Malignancies. J. Oral Rehabil. 2019, 46, 140–150. [Google Scholar] [CrossRef]
- Yuwanati, M.; Gondivkar, S.; Sarode, S.C.; Gadbail, A.; Desai, A.; Mhaske, S.; Pathak, S.K.; N Khatib, M. Oral Health-Related Quality of Life in Oral Cancer Patients: Systematic Review and Meta-Analysis. Future Oncol. 2021, 17, 979–990. [Google Scholar] [CrossRef]
- Covrig, V.I.; Lazăr, D.E.; Costan, V.V.; Postolică, R.; Ioan, B.G. The Psychosocial Role of Body Image in the Quality of Life of Head and Neck Cancer Patients. What Does the Future Hold?-A Review of the Literature. Medicina 2021, 57, 1078. [Google Scholar] [CrossRef] [PubMed]
- Abed, H. Dental Considerations for Head and Neck Cancer: A Clinical Review. Saudi Dent. J. 2023, 35, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Husein, A.B.; Butterworth, C.J.; Ranka, M.S.; Kwasnicki, A.; Rogers, S.N. A Survey of General Dental Practitioners in the North West of England Concerning the Dental Care of Patients Following Head and Neck Radiotherapy. Prim. Dent. Care 2011, 18, 59–65. [Google Scholar] [CrossRef]
- El-Rabbany, M.; Duchnay, M.; Raziee, H.R.; Zych, M.; Tenenbaum, H.; Shah, P.S.; Azarpazhooh, A. Interventions for Preventing Osteoradionecrosis of the Jaws in Adults Receiving Head and Neck Radiotherapy. Cochrane Database Syst. Rev. 2019, 2019, CD011559. [Google Scholar] [CrossRef]
- Sonis, S.T.; Elting, L.S.; Keefe, D.; Peterson, D.E.; Schubert, M.; Hauer-Jensen, M.; Bekele, B.N.; Raber-Durlacher, J.; Donnelly, J.P.; Rubenstein, E.B.; et al. Perspectives on Cancer Therapy-Induced Mucosal Injury: Pathogenesis, Measurement, Epidemiology, and Consequences for Patients. Cancer 2004, 100, 1995–2025. [Google Scholar] [CrossRef]
- Moore, C.; McLister, C.; Cardwell, C.; O’Neill, C.; Donnelly, M.; McKenna, G. Dental Caries Following Radiotherapy for Head and Neck Cancer: A Systematic Review. Oral Oncol. 2020, 100, 104484. [Google Scholar] [CrossRef] [PubMed]
- Topkan, E.; Kucuk, A.; Somay, E.; Yilmaz, B.; Pehlivan, B.; Selek, U. Review of Osteoradionecrosis of the Jaw: Radiotherapy Modality, Technique, and Dose as Risk Factors. J. Clin. Med. 2023, 12, 3025. [Google Scholar] [CrossRef] [PubMed]
- Dutheil, F.; Guillemin, F.; Biau, J.; Pham-Dang, N.; Saroul, N.; Clavère, P.; Lapeyre, M. Predictive factors for mandibular osteoradionecrosis after irradiation of head and neck cancers. Cancer Radiother. 2021, 25, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Nooh, N. Dental Implant Survival in Irradiated Oral Cancer Patients: A Systematic Review of the Literature. Int. J. Oral Maxillofac. Implant. 2013, 28, 1233–1242. [Google Scholar] [CrossRef]
- Schiegnitz, E.; Müller, L.K.; Sagheb, K.; Theis, L.; Cagiran, V.; Kämmerer, P.W.; Wegener, J.; Wagner, W.; Al-Nawas, B. Clinical Long-Term and Patient-Reported Outcomes of Dental Implants in Oral Cancer Patients. Int. J. Implant. Dent. 2021, 7, 93. [Google Scholar] [CrossRef]
- Vosselman, N.; Alberga, J.; Witjes, M.H.J.; Raghoebar, G.M.; Reintsema, H.; Vissink, A.; Korfage, A. Prosthodontic Rehabilitation of Head and Neck Cancer Patients-Challenges and New Developments. Oral Dis. 2021, 27, 64–72. [Google Scholar] [CrossRef]
- Bessadet, M.; Drancourt, N.; El Osta, N. Time Efficiency and Cost Analysis between Digital and Conventional Workflows for the Fabrication of Fixed Dental Prostheses: A Systematic Review. J. Prosthet. Dent. 2024, 133, 71–84. [Google Scholar] [CrossRef]
- Bessadet, M.; Auduc, C.; Drancourt, N.; Nicolas, E.; El Osta, N. Comparative Analyses of Time Efficiency and Cost in Fabricating Fixed Implant-Supported Prostheses in Digital, Hybrid, and Conventional Workflows: A Systematic Review and Meta-Analysis. J. Prosthet. Dent. 2024, 133, 689–712. [Google Scholar] [CrossRef]
- El Osta, N.; Bessadet, M.; Drancourt, N.; Batisse, C. Time Efficiency and Cost of Fabricating Removable Complete Dentures Using Digital, Hybrid, and Conventional Workflows: A Systematic Review. J. Prosthet. Dent. 2024. [Google Scholar] [CrossRef]
- Dougherty, N. The Dental Patient with Special Needs: A Review of Indications for Treatment under General Anesthesia. Spec. Care Dent. 2009, 29, 17–20. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE Guidelines: Consensus-Based Clinical Case Reporting Guideline Development. J. Med. Case Rep. 2013, 7, 223. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.N.; Lowe, D.; Yueh, B.; Weymuller, E.A. The Physical Function and Social-Emotional Function Subscales of the University of Washington Quality of Life Questionnaire. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.N.; O’donnell, J.P.; Williams-Hewitt, S.; Christensen, J.C.; Lowe, D. Health-Related Quality of Life Measured by the UW-QoL—Reference Values from a General Dental Practice. Oral Oncol. 2006, 42, 281–287. [Google Scholar] [CrossRef]
- Tubert-Jeannin, S.; Riordan, P.J.; Morel-Papernot, A.; Porcheray, S.; Saby-Collet, S. Validation of an Oral Health Quality of Life Index (GOHAI) in France. Community Dent. Oral Epidemiol. 2003, 31, 275–284. [Google Scholar] [CrossRef]
- Schimmel, M.; Christou, P.; Miyazaki, H.; Halazonetis, D.; Herrmann, F.R.; Müller, F. A Novel Colourimetric Technique to Assess Chewing Function Using Two-Coloured Specimens: Validation and Application. J. Dent. 2015, 43, 955–964. [Google Scholar] [CrossRef]
- Schimmel, M.; Christou, P.; Herrmann, F.; Müller, F. A Two-Colour Chewing Gum Test for Masticatory Efficiency: Development of Different Assessment Methods. J. Oral Rehabil. 2007, 34, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Palmier, N.R.; Migliorati, C.A.; Prado-Ribeiro, A.C.; de Oliveira, M.C.Q.; Vechiato Filho, A.J.; de Goes, M.F.; Brandão, T.B.; Lopes, M.A.; Santos-Silva, A.R. Radiation-Related Caries: Current Diagnostic, Prognostic, and Management Paradigms. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 52–62. [Google Scholar] [CrossRef]
- Interventions Courantes D’odontologie et de Stomatologie: Quand Pratiquer L’anesthésie Générale? Available online: https://www.has-sante.fr/jcms/c_240338/fr/interventions-courantes-d-odontologie-et-de-stomatologie-quand-pratiquer-l-anesthesie-generale (accessed on 25 October 2024).
- Pohl, Y.; Filippi, A.; Geiger, G.; Kirschner, H.; Boll, M. Dental Treatment of Handicapped Patients Using Endotracheal Anesthesia. Anesth. Prog. 1996, 43, 20–23. [Google Scholar]
- Savanheimo, N.; Sundberg, S.A.; Virtanen, J.I.; Vehkalahti, M.M. Dental Care and Treatments Provided under General Anaesthesia in the Helsinki Public Dental Service. BMC Oral Health 2012, 12, 45. [Google Scholar] [CrossRef]
- Decerle, N.; Cousson, P.-Y.; Nicolas, E.; Hennequin, M. A Comprehensive Approach Limiting Extractions under General Anesthesia Could Improve Oral Health. Int. J. Environ. Res. Public Health 2020, 17, 7336. [Google Scholar] [CrossRef]
- Vermaire, J.A.; Raaijmakers, C.P.J.; Verdonck-de Leeuw, I.M.; Jansen, F.; Leemans, C.R.; Terhaard, C.H.J.; Speksnijder, C.M. Mastication, Swallowing, and Salivary Flow in Patients with Head and Neck Cancer: Objective Tests versus Patient-Reported Outcomes. Support. Care Cancer 2021, 29, 7793–7803. [Google Scholar] [CrossRef] [PubMed]
- Garner, S.J.; Patel, S.; Pollard, A.J.; Jerreat, M.P. Post-Treatment Evaluation of Oral Health-Related Quality of Life in Head and Neck Cancer Patients after Dental Implant Rehabilitation. Br. Dent. J. 2023. [Google Scholar] [CrossRef] [PubMed]
- Roumanas, E.D.; Garrett, N.; Blackwell, K.E.; Freymiller, E.; Abemayor, E.; Wong, W.K.; Beumer, J.; Fueki, K.; Fueki, W.; Kapur, K.K. Masticatory and Swallowing Threshold Performances with Conventional and Implant-Supported Prostheses after Mandibular Fibula Free-Flap Reconstruction. J. Prosthet. Dent. 2006, 96, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Martínez, P.; Peña-Cardelles, J.-F.; Pozo-Kreilinger, J.-J.; Esparza-Gómez, G.; Montesdeoca-García, N.; Cebrián-Carretero, J.-L. Dental Implants Rehabilitation in a Patient with Head and Neck Radiotherapy for Osteosarcoma in the Jaw. A Clinical Case Report. J. Clin. Exp. Dent. 2021, 13, e418–e421. [Google Scholar] [CrossRef]
- Huang, Y.-F.; Chang, C.-T.; Lin, C.-H.; Shen, Y.-F. Prosthodontic Rehabilitation with All-on-Four Implant Treatment Combined CAD/CAM Prosthesis in an Oral Cancer Patient: A Case Report. BMC Oral Health 2024, 24, 1080. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| UW-QOL Domains | Scores Prior to Treatment (/100) | Scores After Treatment (/100) | Healthy Population Reference Scores (/100) |
|---|---|---|---|
| Chewing | 50 | 50 | 94 |
| Swallowing | 100 | 100 | 98 |
| Speech | 70 | 70 | 98 |
| Taste | 100 | 100 | 95 |
| Saliva | 30 | 100 | 97 |
| Appearance | 25 | 75 | 93 |
| Physical score | 62.5 | 82.5 | 95.8 |
| Anxiety | 70 | 70 | 83 |
| Mood | 75 | 75 | 82 |
| Pain | 25 | 75 | 86 |
| Activity | 50 | 50 | 86 |
| Recreation | 75 | 75 | 86 |
| Shoulder | 100 | 100 | 91 |
| Socio-emotional score | 65.9 | 74.2 | 85.7 |
| Global score | 64.2 | 78.35 | 90.8 |
| GOHAI Domains | Scores Prior to Treatment | Scores After Treatment |
|---|---|---|
| Functional domain (/20) | 12 | 12 |
| Psychosocial domain (/25) | 14 | 22 |
| Pain and discomfort (/15) | 4 | 10 |
| Total score (/60) | 30 | 44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batisse, C.; El Osta, N.; Cousson, P.-Y. Full-Mouth Digital Dental Rehabilitation Under General Anesthesia in a Post-Treatment Intraoral Squamous Cell Carcinoma Patient: A Case Report. Healthcare 2025, 13, 940. https://doi.org/10.3390/healthcare13080940
Batisse C, El Osta N, Cousson P-Y. Full-Mouth Digital Dental Rehabilitation Under General Anesthesia in a Post-Treatment Intraoral Squamous Cell Carcinoma Patient: A Case Report. Healthcare. 2025; 13(8):940. https://doi.org/10.3390/healthcare13080940
Chicago/Turabian StyleBatisse, Cindy, Nada El Osta, and Pierre-Yves Cousson. 2025. "Full-Mouth Digital Dental Rehabilitation Under General Anesthesia in a Post-Treatment Intraoral Squamous Cell Carcinoma Patient: A Case Report" Healthcare 13, no. 8: 940. https://doi.org/10.3390/healthcare13080940
APA StyleBatisse, C., El Osta, N., & Cousson, P.-Y. (2025). Full-Mouth Digital Dental Rehabilitation Under General Anesthesia in a Post-Treatment Intraoral Squamous Cell Carcinoma Patient: A Case Report. Healthcare, 13(8), 940. https://doi.org/10.3390/healthcare13080940