
The Impact of Mental Health Comorbidities on Unplanned Admissions for Physical Conditions: A Retrospective Observational Analysis

 ,
,  ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Payne, R.A.; Abel, G.A.; Guthrie, B.; Mercer, S.W. The effect of physical multimorbidity, mental health conditions and socioeconomic deprivation on unplanned admissions to hospital: A retrospective cohort study. CMAJ 2013, 185, E221–E228. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Nicholson, K.; Liu, W.; Fitzpatrick, D.; Hardacre, K.A.; Roberts, S.; Salerno, J.; Stranges, S.; Fortin, M.; Mangin, D. Prevalence of multimorbidity and polypharmacy among adults and older adults: A systematic review. Lancet Healthy Longev. 2024, 9, e287–e296. [Google Scholar]
- Taylor, A.; Price, K.; Gill, T.; Adams, R.; Pilkington, R.; Carrangis, N.; Shi, Z.; Wilson, D. Multimorbidity—Not just an older person’s issue. Results from an Australian biomedical study. BMC Public Health 2010, 32, 718. [Google Scholar]
- Okuma, A.; Nakajima, M.; Sonoo, T.; Nakamura, K.; Goto, T. Association between comorbid mental illness and preceding emergency department visits in unplanned admissions. Acute Med. Surg. 2023, 10, e814. [Google Scholar] [CrossRef]
- Jayatilleke, N.; Hayes, R.D.; Chang, C.K.; Stewart, R. Acute general hospital admissions in people with serious mental illness. Psychol. Med. 2018, 48, 2676–2683. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.; Kisely, S.; Pais, J. The Epidemiology of Excess Mortality in People with Mental Illness. Can. J. Psychiatry 2010, 55, 752–760. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Parker, C.; Coupland, C.; Vinogradova, Y. Inequalities in the primary care of patients with coronary heart disease and serious mental health problems: A cross-sectional study. Heart 2007, 93, 1256–1262. [Google Scholar] [CrossRef] [PubMed]
- Sa, Z.; Badgery-Parker, T.; Long, J.C.; Braithwaite, J.; Brown, M.; Levesque, J.F.; Watson, D.E.; Westbrook, J.I.; Mitchell, R. Impact of mental disorders on unplanned readmissions for congestive heart failure patients: A population-level study. ESC Heart Fail. 2024, 11, ehf2.14644. [Google Scholar] [CrossRef]
- Sokoreli, I.; De Vries, J.J.G.; Pauws, S.C.; Steyerberg, E.W. Depression and anxiety as predictors of mortality among heart failure patients: Systematic review and meta-analysis. Heart Fail Rev. 2016, 21, 49–63. [Google Scholar] [CrossRef]
- Druss, B.G.; Bradford, W.D.; Rosenheck, R.A.; Radford, M.J.; Krumholz, H.M. Quality of Medical Care and Excess Mortality in Older Patients With Mental Disorders. Arch. Gen. Psychiatry 2001, 58, 565. [Google Scholar] [CrossRef]
- Burns, T.; Cohen, A. Item-of-service payments for general practitioner care of severely mentally ill persons: Does the money matter? Br. J. Gen. Pract. 1998, 48, 1415–1416. [Google Scholar]
- Dang, T.; Chan, W.; Khawaja, S.; Fryar, J.; Gannon, B.; Kularatna, S.; Parsonage, W.; Ranasinghe, I. Hospital costs for unplanned re-admissions within 30 days of hospitalisations with heart failure, Australia, 2013–2017: A retrospective cohort study. Med. J. Aust. 2024, 221, 317–323. [Google Scholar]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Caranci, N.; Biggeri, A.; Grisotto, L.; Pacelli, B.; Spadea, T.; Costa, G. The Italian deprivation index at census block level: Definition, description and association with general mortality. Epidemiol. Prev. 2010, 34, 167–176. [Google Scholar]
- Caranci, N.; Costa, G. Un indice di deprivazione a livello aggregato da utilizzare su scala nazionale: Giustificazioni e composizione dell’indice. In Le Disuguaglianze di Salute. Problemi di Definizione e di Misura. Salute e Società; Costa, G., Cislaghi, C., Caranci, N., Eds.; Franco Angeli: Milano, Italy, 2009; pp. 58–78. [Google Scholar]
- Rosano, A.; Pacelli, B.; Zengarini, N.; Costa, G.; Cislaghi, C.; Caranci, N. Update and reviewof the 2011 Italian deprivation index calculated at the census section level. Epidemiol. Prev. 2020, 44, 162–170. [Google Scholar]
- Di Giovanni, P.; Cedrone, F.; Di Martino, G.; Romano, F.; Staniscia, T. Paediatric ambulatory care sensitive hospitalisation and Italian deprivation index: Retrospective multilevel analysis of administrative data from 2008 to 2018 in the Abruzzo Region (Southern Italy). Epidemiol. Prev. 2020, 44 (Suppl. 1), 163–169. [Google Scholar] [CrossRef] [PubMed]
- Geier, T.J.; Simske, N.; Melin, S.; Trevino, C.; Murphy, P.; Schroeder, M.E.; Brandolino, A.; deRoon-Cassini, T.; Schramm, A.T. Psychiatric comorbidity in emergency general surgery patients: A prospective observational study. Trauma Surg Acute Care Open 2023, 8, e001117. [Google Scholar] [CrossRef]
- Pilowsky, J.K.; von Huben, A.; Elliott, R.; Roche, M.A. Development and validation of a risk score to predict unplanned hospital readmissions in ICU survivors: A data linkage study. Aust. Crit. Care 2023, 37, 383–390. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Mittal, D.; Reaves, C.M.; Haynes, T.F.; Han, X.; Morris, S.; Sullivan, G. Mental health stigma and primary health care decisions. Psychiatry Res. 2014, 218, 35–38. [Google Scholar] [CrossRef]
- Ljungqvist, I.; Topor, A.; Forssell, H.; Svensson, I.; Davidson, L. Money and Mental Illness: A Study of the Relationship Between Poverty and Serious Psychological Problems. Community Ment. Health J. 2016, 52, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Carter, P.; Reynolds, J.; Carter, A.; Potluri, S.; Uppal, H.; Chandran, S.; Potluri, R. The impact of psychiatric comorbidities on the length of hospital stay in patients with heart failure. Int. J. Cardiol. 2016, 207, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Gentil, L.; Grenier, G.; Vasiliadis, H.M.; Fleury, M.J. Predictors of Length of Hospitalization and Impact on Early Readmission for Mental Disorders. Int. J. Environ. Res. Public Health 2022, 19, 15127. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hill, E.; Nguyen, N.H.; Qian, A.S.; Patel, S.; Chen, P.L.; Tse, C.S.; Singh, S. Impact of Comorbid Psychiatric Disorders on Healthcare Utilization in Patients with Inflammatory Bowel Disease: A Nationally Representative Cohort Study. Dig. Dis. Sci. 2022, 67, 4373–4381. [Google Scholar] [CrossRef] [PubMed]
- Protty, M.B.; Lacey, A.; Smith, D.; Hannoodee, S.; Freeman, P. Increased morbidity, mortality and length of in-hospital stay for patients with acute coronary syndrome with pre-morbid psychiatric diagnoses. Int. J. Cardiol. 2017, 236, 5–8. [Google Scholar] [CrossRef]
- Fleury, M.J.; Cao, Z.; Grenier, G. Emergency Department Use among Patients with Mental Health Problems: Profiles, Correlates, and Outcomes. Int. J. Environ. Res. Public Health 2024, 21, 864. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.E.; Rosen, C.B.; Roberts, S.E.; Moneme, A.; Wirtalla, C.; Kelz, R.R. Postdischarge Mental Health Care and Emergency General Surgery Readmission for Patients with Serious Mental Illness. Ann. Surg. 2025, 281, 508–513. [Google Scholar] [CrossRef]
- Yorganci, E.; Stewart, R.; Sampson, E.L.; Sleeman, K.E. Patterns of unplanned hospital admissions among people with dementia: From diagnosis to the end of life. Age Ageing 2022, 51, afac098. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cedrone, F.; Catalini, A.; Stacchini, L.; Berselli, N.; Caminiti, M.; Mazza, C.; Cosma, C.; Minutolo, G.; Di Martino, G. The Role of Gender in the Association between Mental Health and Potentially Preventable Hospitalizations: A Single-Center Retrospective Observational Study. Int. J. Environ. Res. Public Health 2022, 22, 14691. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Overall | % | Unplanned Admission | % | Planned Admission | % | ||
|---|---|---|---|---|---|---|---|
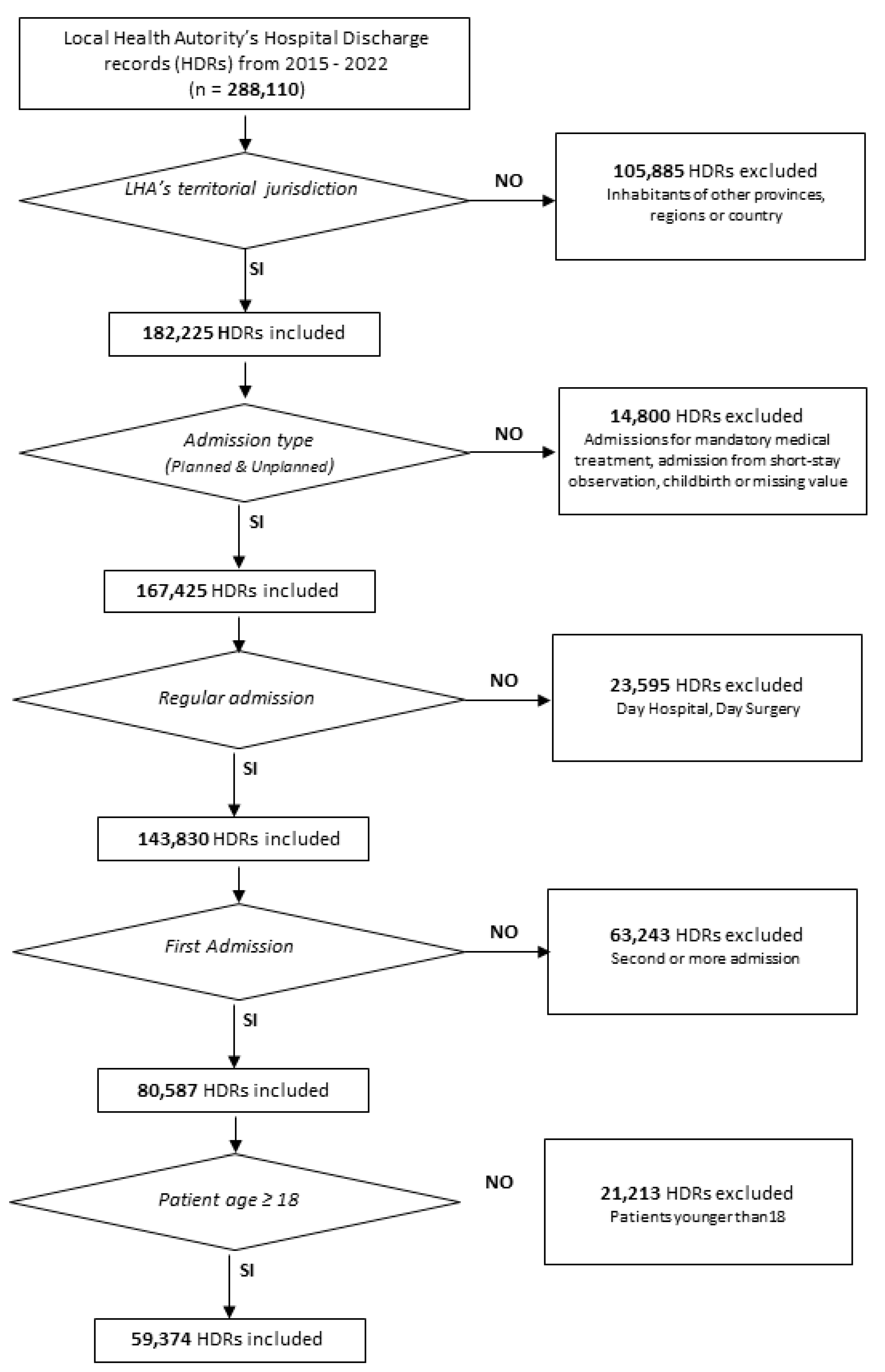
| Sample | 59,374 | 43,293 | 16,081 | ||||
| Gender | |||||||
| M | 25,805 | 43.5% | 18,284 | 42.2% | 7521 | 46.8% | |
| F | 33,569 | 56.5% | 25,009 | 57.8% | 8560 | 53.2% | |
| Age classes | |||||||
| 18–44 | 18,001 | 30.3% | 13,833 | 32.0% | 4168 | 25.9% | |
| 45–64 | 14,705 | 24.8% | 9260 | 21.4% | 5445 | 33.9% | |
| 65–79 | 15,559 | 26.2% | 10,507 | 24.3% | 5052 | 31.4% | |
| 80+ | 11,109 | 18.7% | 9693 | 22.4% | 1416 | 8.8% | |
| Caranci’s deprivation index classes | |||||||
| 1 | 1772 | 3.0% | 1288 | 3.0% | 484 | 3.0% | |
| 2 | 7983 | 13.4% | 5756 | 13.3% | 2227 | 13.8% | |
| 3 | 13,191 | 22.2% | 9268 | 21.4% | 3923 | 24.4% | |
| 4 | 1743 | 2.9% | 1311 | 3.0% | 432 | 2.7% | |
| 5 | 34,489 | 58.1% | 25,524 | 59.0% | 8965 | 55.7% | |
| Physical comorbidities | |||||||
| 0 | 35,357 | 59.5% | 25,000 | 57.7% | 10,357 | 64.4% | |
| 1 | 12,553 | 21.1% | 9230 | 21.3% | 3323 | 20.7% | |
| 2 or more | 11,464 | 19.3% | 9063 | 20.9% | 2401 | 14.9% | |
| Mental comorbidities | |||||||
| No | 57,822 | 97.4% | 41,811 | 96.6% | 16,011 | 99.6% | |
| Yes | 1552 | 2.6% | 1482 | 3.4% | 70 | 0.4% | |
| Variable | Odds | p | Upper IC95% | Lower IC95% |
|---|---|---|---|---|
| Female gender | 1.09 | <0.01 | 1.05 | 1.14 |
| Age classes | ||||
| 18–44 | 0.58 | <0.01 | 0.54 | 0.62 |
| 45–64 | 0.26 | <0.01 | 0.25 | 0.28 |
| 65–79 | 0.30 | <0.01 | 0.28 | 0.32 |
| 80+ | ref | |||
| Caranci’s deprivation index classes | ||||
| 1 | 0.93 | 0.207 | 0.83 | 1.04 |
| 2 | 0.89 | <0.01 | 0.48 | 0.94 |
| 3 | 0.84 | <0.01 | 0.81 | 0.88 |
| 4 | 1.05 | 0.32 | 0.94 | 1.18 |
| 5 | ref | |||
| Physical comorbidities | ||||
| 0 | ref | |||
| 1 | 1.23 | <0.01 | 1.17 | 1.30 |
| 2 or more | 1.65 | <0.01 | 1.56 | 1.75 |
| Mental comorbidities | 9.85 | <0.01 | 7.74 | 12.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cedrone, F.; Santangelo, O.E.; Di Michele, V.; Catalini, A.; Pennisi, F.; Stacchini, L.; Fonzo, M.; Montagna, V.; Gianfredi, V.; Di Martino, G. The Impact of Mental Health Comorbidities on Unplanned Admissions for Physical Conditions: A Retrospective Observational Analysis. Healthcare 2025, 13, 827. https://doi.org/10.3390/healthcare13070827
Cedrone F, Santangelo OE, Di Michele V, Catalini A, Pennisi F, Stacchini L, Fonzo M, Montagna V, Gianfredi V, Di Martino G. The Impact of Mental Health Comorbidities on Unplanned Admissions for Physical Conditions: A Retrospective Observational Analysis. Healthcare. 2025; 13(7):827. https://doi.org/10.3390/healthcare13070827
Chicago/Turabian StyleCedrone, Fabrizio, Omar Enzo Santangelo, Vittorio Di Michele, Alessandro Catalini, Flavia Pennisi, Lorenzo Stacchini, Marco Fonzo, Vincenzo Montagna, Vincenza Gianfredi, and Giuseppe Di Martino. 2025. "The Impact of Mental Health Comorbidities on Unplanned Admissions for Physical Conditions: A Retrospective Observational Analysis" Healthcare 13, no. 7: 827. https://doi.org/10.3390/healthcare13070827
APA StyleCedrone, F., Santangelo, O. E., Di Michele, V., Catalini, A., Pennisi, F., Stacchini, L., Fonzo, M., Montagna, V., Gianfredi, V., & Di Martino, G. (2025). The Impact of Mental Health Comorbidities on Unplanned Admissions for Physical Conditions: A Retrospective Observational Analysis. Healthcare, 13(7), 827. https://doi.org/10.3390/healthcare13070827