
A Mixed Methods Approach to Understanding Mental Health Literacy Among University Health Students

 ,
,  ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
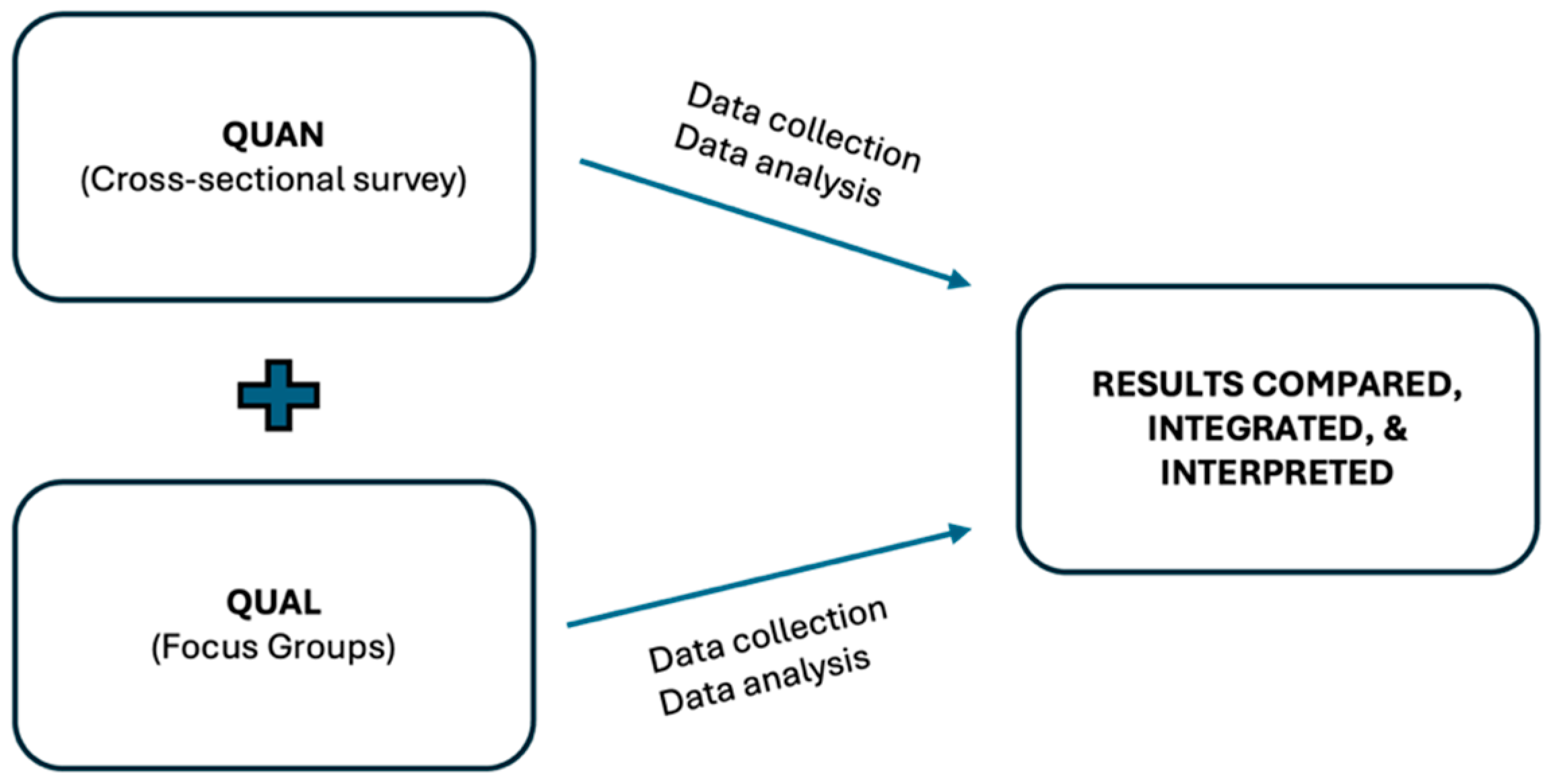
2.1. Study Design
2.2. Ethics Considerations
2.3. Participant Recruitment and Data Collection
2.4. Data Analysis
3. Results
3.1. Quantitative Data Results
3.2. Qualitative Data Results
3.2.1. Concept
3.2.2. Intervention
“…also integrate some things into the curricular units, because whether it seems like it or not, when we’re in the health field, it’s important to have this ability to have knowledge about what mental health is and I think it’s important throughout the year…”.(F2E9)
“I think we could have a hybrid model, as we started by talking about being online, because it’s so easy. If from time to time a different dynamic comes up, with a different theme it could be face-to-face. We could do something like this, and then involve different groups, because in our case, as much as we socialise between different years, we’re all from the same course. So, we end up having a different perception and I can better understand the reality of my colleagues, who have a totally different reality to mine”.(F2E13)
“I don’t think there necessarily has to be a number, because if there’s only one session it might not be enough. And so, I think, depending on the availability of the teachers or psychologists, I think it should be more or less planned throughout the semester, several sessions”.(F1E7)
3.2.3. Caring for MH
“…but health is also defined as complete physical, mental and psychological well-being and is a finding of a balance between the three dimensions. And if our mental health is affected, we won’t be in balance with our lives and everything around us. This goes hand in hand with what my colleague said about being in complete balance with all the dimensions of our lives”.(F2E14)
3.2.4. Challenges in Higher Education
“There were internship placements I had with a colleague where they were almost in paradise, everything was fine for them, while I felt like I just wanted it to end quickly and leave that place. In other words, even if I spoke to them, they would never be able to understand, and it ended up being a bit like what the colleague was saying—although not judging, they couldn’t comprehend my pain, so to speak. In the end, it felt like my experience was being devalued”.(F2E13)
3.2.5. Institutional Resources
3.3. Data Integration and Triangulation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MH | Mental health |
| MHL | Mental health literacy |
| PMeHL | Positive MHL |
| MMARS | Mixed Methods Article Reporting Standards |
| FG | focus group |
| MHLq-SVa | MHL Questionnaire |
| ALS | Academic Life Satisfaction |
| SHS | Subjective Happiness Scale |
| PWBS | Psychological Well-Being Scale |
| DASS | Depression Anxiety Stress Scale |
| MHFA | Mental Health Fist Aid |
References
- Jorm, A.F. Why We Need the Concept of “Mental Health Literacy”. Health Commun. 2015, 30, 1166–1168. [Google Scholar]
- Miles, R.; Rabin, L.; Krishnan, A.; Grandoit, E.; Kloskowski, K. Mental health literacy in a diverse sample of undergraduate students: Demographic, psychological, and academic correlates. BMC Public Health 2020, 20, 1699. [Google Scholar]
- Kim, E.J.; Yu, J.H.; Kim, E.Y. Pathways linking mental health literacy to professional help-seeking intentions in Korean college students. J. Psychatr. Ment. Health Nurs. 2020, 27, 393–405. [Google Scholar]
- Cormier, E.; Park, H.; Schluck, G. College Students’ eMental Health Literacy and Risk of Diagnosis with Mental Health Disorders. Healthcare 2022, 10, 2406. [Google Scholar] [CrossRef] [PubMed]
- Reavley, N.J.; McCann, T.V.; Jorm, A.F. Mental health literacy in higher education students. Early Interv. Psychiatry 2012, 6, 45–52. [Google Scholar]
- Noroozi, A.; Khademolhosseini, F.; Lari, H.; Tahmasebi, R. The mediator role of mental health literacy in the relationship between demographic variables and health-promoting behaviours. Iran. J. Psychiatry Behav. Sci. 2018, 12, e12603. [Google Scholar]
- Carvalho, D.; Sequeira, C.; Querido, A.; Tomás, C.; Morgado, T.; Valentim, O.; Moutinho, L.; Gomes, J.; Laranjeira, C. Positive mental health literacy: A concept analysis. Front. Psychol. 2022, 13, 877611. [Google Scholar]
- Lipson, S.K.; Zhou, S.; Abelson, S.; Heinze, J.; Jirsa, M.; Morigney, J.; Patterson, A.; Singh, M.; Eisenberg, D. Trends in college student mental health and help-seeking by race/ethnicity: Findings from the national healthy minds study, 2013–2021. J. Affect. Disord. 2022, 306, 138–147. [Google Scholar]
- Pedrelli, P.; Nyer, M.; Yeung, A.; Zulauf, C.; Wilens, T. College Students: Mental Health Problems and Treatment Considerations. Acad. Psychiatry 2015, 39, 503–511. [Google Scholar]
- Kutcher, S.; Wei, Y.; Coniglio, C. Mental health literacy: Past, present, and future. Can. J. Psychiatry 2016, 61, 154–158. [Google Scholar]
- Wei, Y.; McGrath, P.J.; Hayden, J.; Kutcher, S. Measurement properties of mental health literacy tools measuring help-seeking: A systematic review. J. Ment. Health 2017, 26, 543–555. [Google Scholar] [PubMed]
- Fung, K.; Cheng, S.L.; Ning, X.; Li, A.T.; Zhang, J.; Liu, J.J.; Hilario, C.T.; Cheng, X.; Yu, M.; Jia, C.X.; et al. Mental Health Promotion and Stigma Reduction Among University Students Using the Reach, Efficacy, Adoption, Implementation, and Maintenance (RE-AIM) Framework: Protocol for a Mixed Methods Study. JMIR Res. Protoc. 2021, 10, e25592. [Google Scholar] [PubMed]
- Loureiro, L.M.; Sousa, C.F. Programa de primeiros socorros em saúde mental: Estudo piloto. Rev. Port. Investig. Comport. E Soc. 2019, 5, 72–86. [Google Scholar]
- Loureiro, L.M.; Amorim, R.; Frajuca, M.; Cunha, S.; Correia, S.; Morgado, T.; Costa, L. Primeira Ajuda em Saúde Mental: Contributo do programa para o incremento da literacia em saúde mental dos estudantes do ensino superior. Rev. Port. Investig. Comport. E Soc. 2020, 6, 24–38. [Google Scholar]
- Yeo, G.; Reich, S.M.; Liaw, N.A.; Chia, E.Y. The Effect of Digital Mental Health Literacy Interventions On Mental Health: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2024, 26, e51268. [Google Scholar]
- Borghouts, J.; Eikey, E.V.; Mark, G.; De Leon, C.; Schueller, S.M.; Schneider, M.; Stadnick, N.; Zheng, K.; Mukamel, D.B.; Sorkin, D.H. Understanding mental health app use among community college Students: Web-Based Survey study. J. Med. Internet Res. 2021, 23, e27745. [Google Scholar]
- Liang, M.; Chen, Q.; Guo, J.; Mei, Z.; Wang, J.; Zhang, Y.; He, L.; Li, Y. Mental Health Fist Aid Improves Mental Health Literacy among College Students: A meta-analysis. J. Am. Coll. Health 2021, 71, 1196–1205. [Google Scholar]
- Teixeira, S.; Ferré-Grau, C.; Canut, T.L.; Pires, R.; Carvalho, J.C.; Ribeiro, I.; Sequeira, C.; Rodrigues, T.; Sampaio, F.; Costa, T.; et al. Positive Mental Health in University Students and Its Relations with Psychological Vulnerability, Mental Health Literacy, and Sociodemographic Characteristics: A Descriptive Correlational Study. Int. J. Environ. Res. Public Health 2022, 19, 3185. [Google Scholar] [CrossRef]
- Kılınç, N.; Kendirkıran, G. Determining the Mental Health Literacy Level of University Students and Examining Their Attitudes Towards Seeking Psychological Help. Int. J. Ment. Health Nurs. 2025, 34, e13506. [Google Scholar]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Personal. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Michael, K.; Schujovitzky, D.; Karnieli-Miller, O. The associations between resilience, selfcare, and burnout among medical students. PLoS ONE 2024, 19, e0309994. [Google Scholar] [CrossRef]
- Nogueira, M.J.; Sequeira, C. A satisfação com a vida académica. Relação com bem-estar e distress psicológico. Rev. Port. Enferm. Saúde Ment. 2018, 6, 71–76. [Google Scholar] [CrossRef]
- Cahyawulan, W.; Fazny, B.Y.; Karsih, K. Academic major satisfaction as a predictor of Psychological Well-Being and psychological distress. PSIKOPEDAGOGIA J. Bimbing. Dan Konseling 2022, 11, 87. [Google Scholar] [CrossRef]
- Zalazar-Jaime, M.F.; Moretti, L.S.; Medrano, L.A. Contribution of Academic Satisfaction Judgments to Subjective Well-Being. Front. Psychol. 2022, 13, 772346. [Google Scholar] [CrossRef]
- Cao, F.; Zhang, L.; Li, M.; Xie, Z. Subjective well-being among PhD students in mainland China: The roles of psychological capital and academic engagement. Front. Psychol. 2024, 15, 1354451. [Google Scholar] [CrossRef] [PubMed]
- Moussa, N.M.; Ali, W.F. Exploring the relationship between students’ academic success and happiness levels in the higher education settings during the lockdown period of COVID-19. Psychol. Rep. 2021, 125, 986–1010. [Google Scholar] [CrossRef]
- Saunders, I.M.; Pick, A.M.; Lee, K.C. Grit, subjective happiness, satisfaction with life, and academic resilience among pharmacy and physical therapy students at two universities. Am. J. Pharm. Educ. 2023, 87, 100041. [Google Scholar] [CrossRef]
- Moss, R.A.; Gorczynski, P.; Sims-Schouten, W.; Heard-Laureote, K.; Creaton, J. Mental health and wellbeing of postgraduate researchers: Exploring the relationship between mental health literacy, help-seeking behaviour, psychological distress, and wellbeing. High. Educ. Res. Dev. 2021, 41, 1168–1183. [Google Scholar] [CrossRef]
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar]
- Abed, H.A.; El-Raouf, A.; Salah, M. Stress, anxiety, depression among medical undergraduate students at Benha university and their socio-demographic correlates. Egypt. J. Hosp. Med. 2021, 86, 27–32. [Google Scholar]
- Agyapong-Opoku, G.; Agyapong, B.; Obuobi-Donkor, G.; Eboreime, E. Depression and Anxiety among Undergraduate Health Science Students: A Scoping Review of the Literature. Behav. Sci. 2023, 13, 1002. [Google Scholar] [CrossRef]
- Posluns, K.; Gall, T.L. Dear mental health practitioners, take care of yourselves: A literature review on self-care. Int. J. Adv. Couns. 2020, 42, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- APA—American Psychology Association. APA Style JARS for Mixed Methods Research (JARS–Mixed). Available online: https://apastyle.apa.org/jars/mixed-methods (accessed on 29 December 2024).
- Jorm, A.F. Mental health literacy: Empowering the community to take action for better mental health. Am. Psychol. 2012, 67, 231–243. [Google Scholar] [PubMed]
- Campos, L.; Dias, P.; Costa, M.; Rabin, L.; Miles, R.; Lestari, S.; Feraihan, R.; Pant, N.; Sriwichai, N.; Yu, L.; et al. Mental health literacy questionnaire-short version for adults (MHLq-SVa): Validation study in China, India, Indonesia, Portugal, Thailand, and the United States. BMC Psychiatry 2022, 22, 713. [Google Scholar]
- Nogueira, M.J.; Antunes, J.; Sequeira, C. Development and psychometric study of the academic life satisfaction scale (ALSS) in a higher education students sample. Nurs. Healthc. Int. J. 2019, 3, 1–8. [Google Scholar]
- Lyubomirsky, S.; Lepper, H. A measure of subjective happiness: Preliminary reliability and construct validation. Soc. Indic. Res. 1999, 46, 137–155. [Google Scholar]
- Pais-Ribeiro, J.L. Validação transcultural da escala de felicidade subjectiva de Lyubomirsky e Lepper. Psicol. Saúde Doenças 2012, 13, 157–168. [Google Scholar]
- Novo, R.F.; Duarte-Silva, M.E.; Peralta, E. O bem-estar psicológico em adultos: Estudo das características psicométricas da versão portuguesa das escalas de C. Ryff. In Avaliação Psicológica: Formas e Contextos; Gonçalves, M., Ribeiro, I., Araújo, S., Machado, C., Almeida, L., Simões, M., Eds.; Associação dos Psicólogos Portugueses: Braga, Portugal, 1997; Volume V, pp. 313–324. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety & Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Ribeiro, J.L.; Honrado, A.A.; Leal, I.P. Contribuição para o estudo da adaptação portuguesa das escalas de ansiedade, depressão e stress (EADS) de 21 itens de Lovibond e Lovibond. Psicol. Saúde Doenças 2004, 36, 229–239. [Google Scholar]
- Nunnally, J.C. Psychometric Theory, 3rd ed.; Tata McGraw-Hill Education: New York, NY, USA, 1994. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistics notes: Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar]
- Bardin, L. Análise de Conteúdo; Edições 70: São Paulo, Brasil, 2016. [Google Scholar]
- Kajamaa, A.; Mattick, K.; de la Croix, A. How to… do mixed-methods research. Clin. Teach. 2020, 17, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 5th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2015; p. 252. [Google Scholar]
- Hill, T.D.; Needham, B.L. Rethinking gender and mental health: A critical analysis of three propositions. Soc. Sci. Med. 2013, 92, 83–91. [Google Scholar] [CrossRef]
- Reis, A.; Saheb, R.; Moyo, T.; Smith, C.; Sperandei, S. The impact of mental health literacy training programs on the mental health literacy of tertiary students: A systematic review. Prev. Sci. 2022, 23, 648–662. [Google Scholar] [CrossRef] [PubMed]
- Lo, K.; Gupta, T.; Keating, J.L. Interventions to Promote Mental Health Literacy in University Students and Their Clinical Educators. A Systematic Review of Randomised Control Trials. Health Prof. Educ. 2018, 4, 161–175. [Google Scholar] [CrossRef]
- Zhang, X.; Yue, H.; Hao, X.; Liu, X.; Bao, H. Exploring the relationship between mental health literacy and psychological distress in adolescents: A moderated mediation model. Prev. Med. Rep. 2023, 33, 102199. [Google Scholar] [CrossRef]
- Samuolis, J.; Griffin, K.; Mason, M.J.; Dekraker, N. Connectedness to campus and likelihood of help-seeking for suicidality among college women. J. Coll. Stud. Psychother. 2017, 31, 238–246. [Google Scholar] [CrossRef]
- Wahyuni, E.N.; Mangestuti, R.; Rahayu, I.T.; Aziz, R.; Muhid, A. Enhancing Mental Health Literacy in University; Interactions between Student Initiatives and Counselor Strategies. Health Educ. Health Promot. 2024, 12, 215–223. [Google Scholar]
- Yang, X.; Hu, J.; Zhang, B.; Ding, H.; Hu, D.; Li, H. The relationship between mental health literacy and professional psychological help-seeking behavior among Chinese college students: Mediating roles of perceived social support and psychological help-seeking stigma. Front. Psychol. 2024, 15, 1356435. [Google Scholar] [CrossRef]

{kind=link}
| Age (years), mean (SD) | 25.5 (8.07) |
| Sex, n (%) | |
| Male | 6 (25.0%) |
| Female | 18 (75.0%) |
| Marital Status, n (%) | |
| Single | 22 (91.6%) |
| Married | 1 (4.2%) |
| Divorced | 1 (4.2%) |
| Degree Studies, n (%) | |
| Nursing | 16 (66.7%) |
| Physiotherapy | 8 (33.3%) |
| Year of Study, n (%) | |
| 1st year | 4 (16.7%) |
| 2nd year | 4 (16.7%) |
| 3rd year | 10 (41.6%) |
| 4th year | 6 (25.0%) |
| Previous MH support, n (%) (n = 23) | |
| Yes | 17 (73.9%) |
| No | 6 (26.1%) |
| Diagnosis of mental disorder/disease, n (%) (n = 21) | |
| Yes | 4 (19.0%) |
| No | 17 (81.0%) |
| Current MH support, n (%) (n = 23) | |
| Yes | 4 (17.4%) |
| No | 19 (82.6%) |
| Currently taking medication for anxiety, depression, or sleep problems, n (%) (n = 23) | |
| Yes | 5 (21.7%) |
| No | 18 (78.3%) |
| Nuclear family member with a mental illness or disorder, n (%) (n = 23) | |
| Yes | 13 (56.5%) |
| No | 10 (43.5%) |
| MHLq-SVa | |||||
|---|---|---|---|---|---|
| Total | Knowledge of Mental Health Problems | First Aid and Help-Seeking Skills | Erroneous Beliefs/Stereotypes | Self-Help Strategies | |
| ALS (n = 22) | |||||
| Total | −0.277 | −0.373 | 0.075 | −0.086 | −0.198 |
| Personal Satisfaction | 0.034 | 0.029 | 0.118 | 0.110 | −0.080 |
| Satisfaction with the Academic Environment | −0.404 | −0.571 ** | 0.135 | −0.211 | −0.188 |
| SHS (total) (n = 22) | 0.045 | −0.105 | 0.410 | 0.113 | −0.010 |
| PWBS (n = 22) | 0.045 | −0.105 | 0.410 | 0.113 | −0.010 |
| Total | −0.122 | −0.206 | 0.076 | 0.066 | −0.012 |
| Autonomy | −0.062 | −0.111 | −0.028 | −0.380 | 0.310 |
| Environmental Mastery | −0.215 | −0.216 | −0.076 | 0.071 | −0.091 |
| Personal Growth | 0.214 | 0.188 | 0.120 | 0.076 | 0.179 |
| Positive Relations with Others | −0.123 | −0.106 | 0.283 | 0.202 | −0.311 |
| Purpose in Life | −0.047 | −0.087 | 0.223 | 0.236 | −0.120 |
| Self-acceptance | −0.172 | −0.335 | 0.100 | 0.234 | −0.093 |
| DASS (n = 21) | |||||
| Total | 0.040 | 0.156 | −0.147 | −0.198 | 0.100 |
| Depression | −0.118 | 0.000 | −0.296 | −0.308 | 0.018 |
| Anxiety | 0.069 | 0.190 | −0.150 | −0.072 | 0.078 |
| Stress | 0.082 | 0.181 | −0.179 | −0.144 | 0.147 |
| Quantitative Results | Qualitative Results | Comparasion and Integration of Results | Convergence, Divergence, Reinforcement |
|---|---|---|---|
| Students with previous MH support needs showed more MHL (p = 0.020) and MH self-help strategies (p = 0.044). | Category: Caring for MH and Concept | Almost 74% of students reported previous support needs for MH problems, which was associated with more MHL and MH self-strategies. This is corroborated by qualitative data, with the emergence of the category Caring for MH, where students exposed many strategies for promoting and preventing MH. Also, students identified that MHL involves putting knowledge about MH into practice and adopting behaviors favorable to the strategy’s adoption. | Convergence |
| Students with family MH history presented lower levels of erroneous beliefs/stereotypes (p = 0.007). | Category: Challenges in Higher Education—Subcategory: Beliefs and stereotypes | Half of the sample had a nuclear family member with a history of mental illness. These students also showed fewer stereotypes about mental illness. These data were reinforced by the subcategory Beliefs and stereotypes, which showed that students had a perception of what contributes to stigma and discrimination around MH and illness. | Reinforcement |
| Students with higher knowledge of MH problems had less satisfaction with the academic environment (rs = −0.571; p < 0.01). | Category: Challenges in Higher Education—Subcategories: Academic environment; Interest and initiative Category: Institutional resources | The association between greater knowledge of MH problems and lower satisfaction with the academic environment can be partly explained by these students perceiving that the academic environment does not provide the appropriate conditions for promoting MH. This is reinforced by the category about existing resources in the institution, which comprised suggestions from students for strategies to promote MH at an institutional level. | Reinforcement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teixeira, A.I.; Martins, S.; Lima, S.; Pinto, F.; Morgado, T.; Valentim, O. A Mixed Methods Approach to Understanding Mental Health Literacy Among University Health Students. Healthcare 2025, 13, 724. https://doi.org/10.3390/healthcare13070724
Teixeira AI, Martins S, Lima S, Pinto F, Morgado T, Valentim O. A Mixed Methods Approach to Understanding Mental Health Literacy Among University Health Students. Healthcare. 2025; 13(7):724. https://doi.org/10.3390/healthcare13070724
Chicago/Turabian StyleTeixeira, Ana Isabel, Sónia Martins, Sara Lima, Francisca Pinto, Tânia Morgado, and Olga Valentim. 2025. "A Mixed Methods Approach to Understanding Mental Health Literacy Among University Health Students" Healthcare 13, no. 7: 724. https://doi.org/10.3390/healthcare13070724
APA StyleTeixeira, A. I., Martins, S., Lima, S., Pinto, F., Morgado, T., & Valentim, O. (2025). A Mixed Methods Approach to Understanding Mental Health Literacy Among University Health Students. Healthcare, 13(7), 724. https://doi.org/10.3390/healthcare13070724