
A Systematic Review and Meta-Analysis of Virtual and Traditional Physical Activity Programs: Effects on Physical, Health, and Cognitive Outcomes

 , ,
, ,  ,
, 
 , , , , ,
, , , , ,  , and
, and 
Abstract
1. Introduction
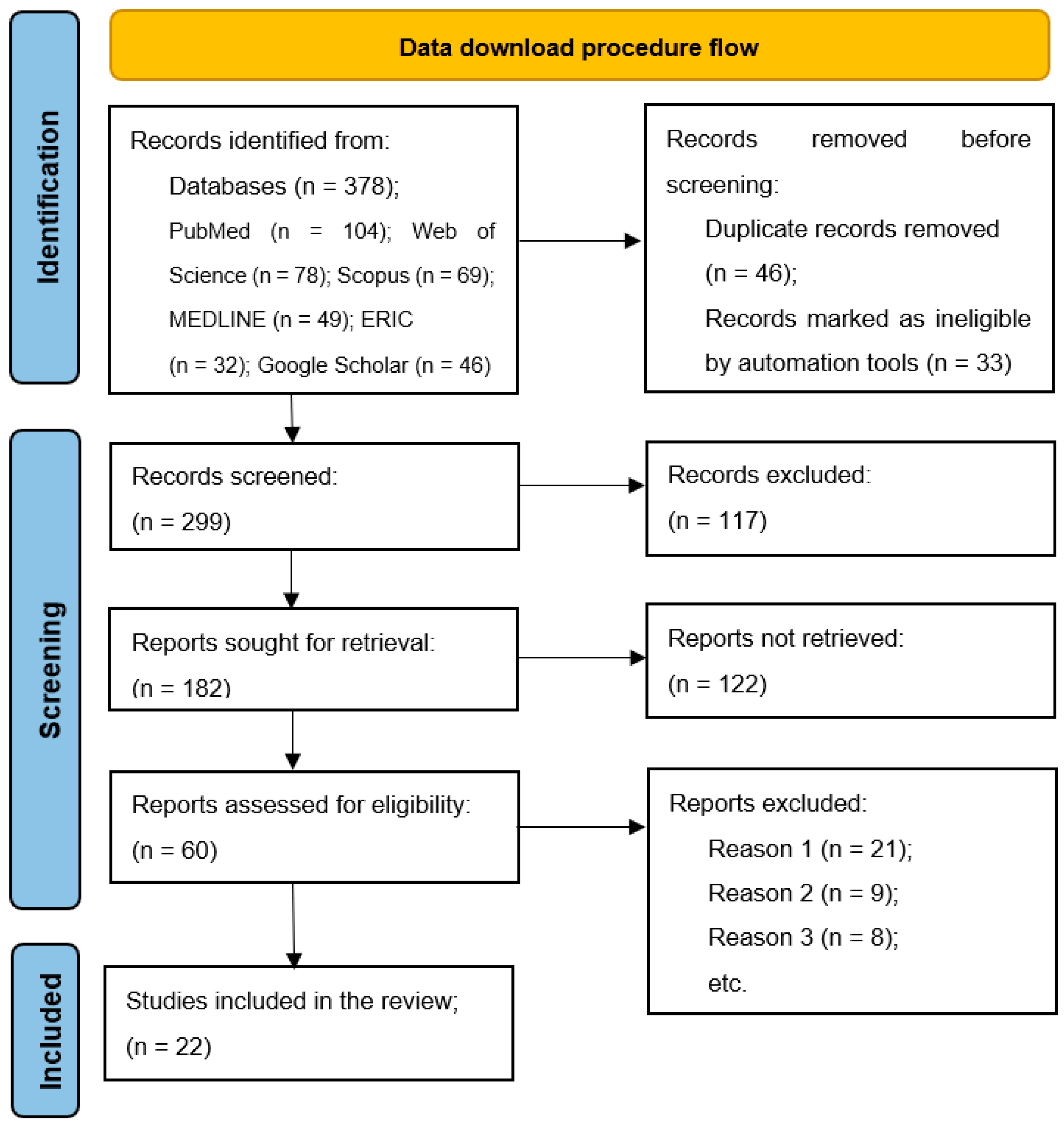
- A systematic search of electronic databases;
- A review of the collected literature.
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Methodological Quality
3. Results
3.1. Literature Characteristics
3.2. Characteristics of the Studies
3.3. The Methodological Quality Assessment of the Included Studies
4. Discussion
4.1. Comparative Analysis of Traditional and Virtual Training Methods
4.2. Impact of Virtual Training Programs on Physical, Health, and Cognitive Aspects
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Willumsen, J.F. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Ahn, S.J.G.; Fox, J. Immersive virtual environments, avatars, and agents for health. In Encyclopedia of Health and Risk Message Design and Processing; Oxford University: Oxford, UK, 2017. [Google Scholar] [CrossRef]
- Salmon, J.; Owen, N.; Crawford, D.; Bauman, A.; Sallis, J.F. Physical activity and sedentary behavior: A population-based study of barriers, enjoyment, and preference. Health Psychol. 2003, 22, 178–188. [Google Scholar] [CrossRef]
- Entertainment Software Association. Essential Facts About the Computer and Video Game Industry. 2011. Available online: https://etcjournal.com/wp-content/uploads/2011/11/esa_ef_2011.pdf?utm_source=chatgpt.com) (accessed on 21 March 2025).
- Peng, W.; Crouse, J.C.; Lin, J.H. Using active video games for physical activity promotion: A systematic review of the current state of research. Health Educ. Behav. 2013, 40, 171–192. [Google Scholar] [CrossRef]
- Plante, T.G.; Aldridge, A.; Su, D.; Bogdan, R.; Belo, M.; Kahn, K. Does virtual reality enhance the management of stress when paired with exercise? An exploratory study. Int. J. Stress Manag. 2003, 10, 203–216. [Google Scholar] [CrossRef]
- Plante, T.G.; Aldridge, A.; Bogden, R.; Hanelin, C. Might virtual reality promote the mood benefits of exercise? Comp. Hum. Behav. 2003, 19, 495–509. [Google Scholar] [CrossRef]
- Zeng, N.; Pope, Z.; Gao, Z. Acute effect of virtual reality exercise bike games on college students’ physiological and psychological outcomes. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 453–457. [Google Scholar] [CrossRef]
- Kim, J.; Son, J.; Ko, N.; Yoon, B. Unsupervised virtual reality-based exercise program improves hip muscle strength and balance control in older adults: A pilot study. Arch. Phys. Med. Rehabil. 2013, 94, 937–943. [Google Scholar] [CrossRef]
- Zaal, F.T.J.M.; Bootsma, R.J. Virtual reality as a tool for the study of perception-action: The case of running to catch fly balls. Presence 2011, 20, 93–103. [Google Scholar] [CrossRef]
- Seo, E.; Kim, Y.; Lee, Y.; Hur, M. Virtual reality exercise program effects on body mass index, depression, exercise fun and exercise immersion in overweight middle-aged women: A randomized controlled trial. Int. J. Environ. Res. Public Health 2023, 20, 900. [Google Scholar] [CrossRef]
- Touloudi, E.; Hassandra, M.; Galanis, E.; Goudas, M.; Theodorakis, Y. Applicability of an immersive virtual reality exercise training system for office workers during working hours. Sports 2022, 10, 104. [Google Scholar] [CrossRef]
- Mokmin, N.A.M.; Jamiat, N. The effectiveness of a virtual fitness trainer app in motivating and engaging students for fitness activity by applying motor learning theory. Educ. Inf. Technol. 2021, 26, 1847–1864. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Nitkiewicz, S.; Zaremba, A.; Tytuła, J. The analysis of the possibilities of using a virtual reality system in fitness training. Tech. Sci. 2023, 26, 97–110. [Google Scholar] [CrossRef]
- Tirp, J.; Steingrover, C.; Wattie, N.; Baker, J.; Schorer, J. Virtual realities as optimal learning environments in sport–A transfer study of virtual and real dart throwing. Psychol. Test Assess. Model 2015, 57, 57–69. [Google Scholar]
- Peng, W.; Crouse, J.C.; Lin, J.H. A meta-analysis of the effectiveness of digital games in increasing physical activity. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 515–522. [Google Scholar] [CrossRef]
- Zeng, N.; Pope, Z.; Gao, Z. Virtual reality exercise for health: A literature review. Comp. Hum. Behav. 2017, 70, 212–219. [Google Scholar] [CrossRef]
- Gonçalves, R.; Pedrozo, A.L.; Coutinho, E.S.F.; Figueira, I.; Ventura, P. Efficacy of virtual reality exposure therapy in the treatment of PTSD: A systematic review. PLoS ONE 2012, 7, e48469. [Google Scholar] [CrossRef]
- Rutkowski, S.; Kiper, P.; Cacciante, L.; Cieslik, B.; Mazurek, J.; Turolla, A.; Szczepanska-Gieracha, J. Use of virtual reality-based training in different fields of rehabilitation: A systematic review and meta-analysis. J. Rehabil. Med. 2020, 52, 1–16. [Google Scholar] [CrossRef]
- Ho, F.K.W.; Louie, L.H.T.; Wong, W.H.; Chan, K.L.; Tiwari, A.; Chow, C.B.; Ho, W.; Wong, W.; Chan, M.; Chen, E.Y.H.; et al. AA sports-based youth development program, teen mental health, and physical fitness: An RCT. Pediatrics 2017, 140, e20171543. [Google Scholar] [CrossRef]
- Ho, F.K.W.; Louie, L.H.T.; Chow, C.B.; Wong, W.H.S.; Ip, P. Physical activity improves mental health through resilience in Hong Kong Chinese adolescents. BMC Pediatrics 2015, 15, 48. [Google Scholar] [CrossRef]
- García-Bravo, S.; Cuesta-Gómez, A.; Campuzano-Ruiz, R.; López-Navas, M.J.; Domínguez-Paniagua, J.; Araújo-Narváez, A.; Cano-de-la-Cuerda, R. Virtual reality and video games in cardiac rehabilitation programs. A systematic review. Disabil. Rehabil. 2021, 43, 448–457. [Google Scholar] [CrossRef]
- Condon, C.; Lam, W.T.; Mosley, C.; Gough, S. A systematic review and meta-analysis of the effectiveness of virtual reality as an exercise intervention for individuals with a respiratory condition. Adv. Simul. 2020, 5, 33. [Google Scholar] [CrossRef]
- Kolbe, L.; Jaywant, A.; Gupta, A.; Vanderlind, W.M.; Jabbour, G. Use of virtual reality in the inpatient rehabilitation of COVID-19 patients. Gen. Hosp. Psychiatry 2021, 71, 76–81. [Google Scholar] [CrossRef]
- Lammfromm, R.; Gopher, D. Transfer of skill from a virtual reality trainer to real juggling. BIO Web Conf. 2011, 1, 00054. [Google Scholar] [CrossRef]
- Rauter, G.; Sigrist, R.; Koch, C.; Crivelli, F.; van Raai, M.; Riener, R.; Wolf, P. Transfer of complex skill learning from virtual to real rowing. PLoS ONE 2013, 8, e82145. [Google Scholar] [CrossRef]
- Rutkowski, S.; Rutkowska, A.; Kiper, P.; Jastrzebski, D.; Racheniuk, H.; Turolla, A.; Szczegielniak, J.; Casaburi, R. Virtual Reality Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 117–124. [Google Scholar] [CrossRef]
- Wang, L.T. Effectiveness of virtual reality exercise for functional fitness in community-dwelling older adults: A 12-week follow-up study. SAGE Open 2023, 13, 21582440231218515. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 2021, 372, n71. [Google Scholar] [CrossRef]
- Oginni, J.; Otinwa, G.; Gao, Z. Physical impact of traditional and virtual physical exercise programs on health outcomes among corporate employees. J. Clin. Med. 2024, 13, 694. [Google Scholar] [CrossRef]
- Eckmann, T.; Golly, H.; Gamas, W.; Magnus, L. A 10 week study to determine the effects of live vs virtual delivery of transitions program on fitness related components. W. J. Yoga Phys. Ther. Rehabil. 2021, 3, 1–4. [Google Scholar] [CrossRef]
- de Melo Ghisi, G.L.; Aultman, C.; Vanzella, L.; Konidis, R.; Sandison, N.; Oh, P. Effectiveness of a virtual vs. in-person group-based education curriculum to increase disease-related knowledge and change health behaviour among cardiac rehabilitation participants. Patient Educ. Couns. 2024, 118, 108021. [Google Scholar] [CrossRef]
- Chau, P.H.; Kwok, Y.Y.J.; Chan, M.K.M.; Kwan, K.Y.D.; Wong, K.L.; Tang, Y.H.; Chau, K.L.P.; Lau, S.W.M.; Yiu, Y.Y.Y.; Kwong, M.Y.F.; et al. Feasibility, acceptability, and efficacy of virtual reality training for older adults and people with disabilities: Single-arm pre-post study. J. Med. Internet Res. 2021, 23, e27640. [Google Scholar] [CrossRef]
- McDaniel, A.T.; Heijnen, M.J.H.; Kawczynski, B.; Haugen, K.H.; Caldwell, S.; Campe, M.M.; Conley, E.C.; Tseh, W. Efficacy of army combat fitness test 12-week virtual exercise program. Mil. Med. 2022, 188, e2035–e2040. [Google Scholar] [CrossRef]
- Proffitt, R.; Lange, B.; Chen, C.; Winstein, C.A. Comparison of older adults’ subjective experiences with virtual and real environments during dynamic balance activities. J. Aging Phys. Act. 2015, 23, 24–33. [Google Scholar] [CrossRef]
- Suderman, K.; Skene, T.; Sellar, C.; Dolgoy, N.; Pituskin, E.; Joy, A.A.; Culos-Reed, S.N.; McNeely, M.L. Virtual or in-person: A mixed methods survey to determine exercise programming preferences during COVID-19. Curr. Oncol. 2022, 29, 6735–6748. [Google Scholar] [CrossRef]
- Maden, Ç.; Bayramlar, K.; Arıcak, O.T.; Yagli, N.V. Effects of virtual Reality-Based Training and aerobic training on gaming disorder, physical activity, physical fitness, and anxiety: A randomized, controlled trial. Ment. Health Phys. Act. 2022, 23, 100465. [Google Scholar] [CrossRef]
- Irving, B.A.; Davis, C.K.; Brock, D.W.; Weltman, J.Y.; Swift, D.; Barrett, E.J.; Gaesser, G.A.; Weltman, A. Effect of exercise training intensity on abdominal visceral fat and body composition. Med. Sci. Sports Exerc. 2008, 40, 1863–1872. [Google Scholar] [CrossRef]
- Park, E.; Kim, S.; Lee, C. The effects of virtual reality game exercise on balance and gait of the elderly. J. Phys. Ther. Sci. 2015, 27, 1157–1159. [Google Scholar] [CrossRef]
- Ross-Stewart, L.; Price, J.; Jackson, D.; Hawkins, C.A. Preliminary investigation into the use of an imagery assisted virtual reality intervention in sport. J. Sports Sci. 2018, 6, 20–30. [Google Scholar] [CrossRef]
- Daveri, M.; Fusco, A.; Cortis, C.; Mascherini, G. Effectiveness of different modalities of remote online training in young healthy males. Sports 2022, 10, 170. [Google Scholar] [CrossRef]
- Harris, D.J.; Buckingham, G.; Wilson, M.R.; Brookes, J.; Mushtaq, F.; Mon-Williams, M.; Vine, S.J. The effect of a virtual reality environment on gaze behaviour and motor skill learning. Psychol. Sport Exerc. 2020, 50, 101721. [Google Scholar] [CrossRef]
- Gani, R.A.; Setiawan, E.; Achmad, I.Z.; Aminudin, R.; Purbangkara, T.; Hofmeister, M. Virtual reality-based tabata training: A professional method for changing levels physical fitness and psychological well-being on student-athletes. Pedagog. Phys. Cult. Sports 2023, 27, 91–101. [Google Scholar] [CrossRef]
- Gray, R. Transfer of training from virtual to real baseball batting. Front. Psychol. 2017, 8, 2183. [Google Scholar] [CrossRef]
- McClure, C.; Schofield, D. Running virtual: The effect of virtual reality on exercise. J. Hum. Sport Exerc. 2019, 15, 861–870. [Google Scholar] [CrossRef]
- Rubio-Arias, J.Á.; Verdejo-Herrero, A.; Andreu-Caravaca, L.; Ramos-Campo, D.J. Impact of immersive virtual reality games or traditional physical exercise on cardiovascular and autonomic responses, enjoyment and sleep quality: A randomized crossover study. Virtual Real. 2024, 28, 64. [Google Scholar] [CrossRef]
- Meldrum, D.; Herdman, S.; Vance, R.; Murray, D.; Malone, K.; Duffy, D.; Glennon, A.; McConn-Walsh, R. Effectiveness of conventional versus virtual reality-based balance exercises in vestibular rehabilitation for unilateral peripheral vestibular loss: Results of a randomized controlled trial. Arch. Phyc. Med. Rehab. 2015, 96, 1319–1328.e1. [Google Scholar] [CrossRef]
- Ng, Y.L.; Ma, F.; Ho, F.K.; Ip, P.; Fu, K.W. Effectiveness of virtual and augmented reality-enhanced exercise on physical activity, psychological outcomes, and physical performance: A systematic review and meta-analysis of randomized controlled trials. Comp. Hum. Behav. 2019, 99, 278–291. [Google Scholar] [CrossRef]
- Liu, M.; Zhou, K.; Chen, Y.; Zhou, L.; Bao, D.; Zhou, J. Is virtual reality training more effective than traditional physical training on balance and functional mobility in healthy older adults? a systematic review and meta-analysis. Front. Hum. Neurosci. 2022, 16, 843481. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| P (Population) | Men and women, regardless of restrictions on lifestyle, age, and health status. | People with serious health problems or injuries that prevent physical activity. |
| I (Intervention) | Papers in which an experimental procedure was used in which several groups participated, as well as papers in which data were collected through questionnaires or interviews. | Studies with incompatible virtual methods, studies whose primary focus was not physical and cognitive training but rather participants’ impressions, and studies that relied solely on self-reported physical activity data without objective verification were excluded. |
| C (Comparators) | Studies comparing experimental and control groups (e.g., VA vs. CG, IPE vs. NA, etc.) or comparing different groups within virtual training (e.g., EXP1 vs. EXP2, PA vs. VA). | Studies between unrelated sports (e.g., men’s basketball players vs. handball players or soccer players). |
| O (Outcomes) | Effects of virtual activity (VA-VR) on physical and cognitive abilities after implementation of the program; Information about the personal impressions of participants. | Incomplete results. |
| S (Study design) | Randomized and non-randomized controlled studies; Longitudinal and transferal studies; Studies written in Serbian and English. | Duplicates; Conference papers and abstracts; Case reports (e.g., <5 participants per group); Review articles; Preprints; Inappropriate frame of analysis in the period between 2008 and 2024; Studies written in a language that was not Serbian or English. |
| References | Sample | Testing/Instrument | Exposure | Dose | Findings |
|---|---|---|---|---|---|
| Oginni et al., 2024 [33] | n = 30 ♀ y = 37.8 ± 8.8 | Blood pressure, Waist, Hip, Heart rate, Circumferences, Physical activity readiness questionnaire, Body mass index | VA-VCZ PA-SPA CG-NA | 2 × 60 min 6 w | Diastolic blood pressure ↓ Body mass index ↓ Waist, hip ↓ |
| Eckmann et al., 2021 [34] | n = /♀ y = 45–65 | Body mass index, Bioelectrical impedance, Heart rate, Motor ability | VA-WBP Well-WBP | 3 × 60 min 10 w | Body mass index ↓ Motor ability ↑ Heart rate ↓ |
| de Melo Ghisi et al., 2024 [35] | n = 160 ♀ ♂ y = / | Survey, Mediterranean food, Pedometer | VA IPE | - 12–24 w | Mediterranean food ↑ Pedometer ↑ Survey ↑ |
| Mokmin et al., 2021 [16] | n = 33 ♀ n = 21 ♂ y = 19–24 | Survey, Interview | VA-BMTMCTOM | 26 w | Survey ↑ Interview ↑ |
| Chau et al., 2021 [36] | n = 135 ♀ ♂ y = 62.7 | Upper extremities, Lower extremities, Cognitive functions | VA PA-TUG, BBT CG-HK-MoCA 5-min, BTO | 3 × 30 min 6 w | Upper extremities ↑ Lower extremities× Cognitive functions ↑ |
| McDaniel et al., 2022 [37] | n = 2 ♀ n = 11 ♂ y = 29.8 ± 6.2 | Height, Body mass, Body composition, Army combat fitness test, Mean body fat percentage | VA-TRX Elite ACFT Kit PA-DC-430 U, ACFT | 3 ses 12 w | Mean body fat percentage ↓ Army combat fitness test ↑ Body fat ↓ Body mass× |
| Proffitt et al., 2015 [38] | n = 30/ y = 50+ | Health activity information form, Immersive tendencies questionnaire, Tellegen absorption scale, Minimal heart rate, Maximal heart rate, Virtual environment preferences, Perception of challenge, Focus on movement | VA-JM+MKM PA-TBT+MKM | - | Minimum heart rate × Maximal heart rate × Tellegen absorption scale ↓ Virtual environment preferences ↑ Perception of challenge ↑ Focus on movement ↑ |
| Suderman et al., 2022 [39] | n = 127 ♀ ♂ y = 59 ± 11.4 | Survey | VA-ACE PA-ACE+IN | - | Survey ↑ |
| Seo et al., 2023 [14] | n = 75 ♀ y = 40–65 | Body mass index, Depression, The amount of fun during exercise, Exercise immersion | VA-IBE (VRfit) PA-IBE | 3–5 × 50 min 8 w | Body mass index ↓ Depression ↓ The amount of fun during exercise ↑ Exercise immersion ↑ |
| Touloudi et al., 2022 [15] | n = 40 ♀ y = 20–61 | Survey, Expectations, Usability or utilization, Usability or learning, Usability or pleasantness, Sense of presence or spatial presence, Sense of presence or engagement, Sense of presence or realism, Tolerability, Use in the workplace | VA-IBE (VRADA) PA-IBE | 2 sess. × 15 min | Expectations ↑ Usability or utilization ↑ Usability or learning ↑ Usability or pleasantness ↑ Sense of presence or spatial presence ↑ Sense of presence or engagement× Sense of presence or realism ↑ Tolerability ↑ Use in the workplace ↑ |
| Rutkowski et al., 2020 [30] | n = 106 ♀ ♂ y = 60 ± 5 | Arm curl, Chair stand, Beck scratch, Chair sit and reach, Up and go, 6 min walk test | VA-ETPA-ET(TPR) | 5× 6 w | Arm curl ↑ Beck scratch ↑ Chair sit and reach ↑ 6 min walk test ↑ |
| Maden et al., 2022 [40] | n = 44 ♂ y = 18–28 | Height, Body mass, Body mass index, Smoking status, Gaming status, The nine item Internet Gaming Disorder Scale–Short Form, The International Physical Activity Questionnaire, Senior fitness test, Maximum oxygen uptake, Beck anxiety inventory | VR (XK36) PA-ATCG | 3 × 30 min 6 w | Body mass ↓ Physical activity ↑ Anxiety ↓ Repetition ↑ Flexibility ↑ |
| Irving et al., 2008 [41] | n = 27 ♀ y = 51 ± 9 | Weight, Body mass index, Fat free mass, Fat mass, Abdominal fat, Subcutaneous fat, Abdominal visceral fat, Mid-thigh fat area, Mid-thigh skeletal muscle, Waist circumference, Fasting blood glucose, High-density lipoprotein cholesterol, triglycerides, Systolic blood pressure, Diastolic blood pressure, Peak oxygen uptake, Oxygen uptake at lactate threshold, Tidal volume, Metabolic equivalent of task—heart work, Basal metabolic rate | NET LIET HIET | - 16 w | Waist circumference ↓ Systolic blood pressure ↓ Fasting blood glucose× High-density lipoprotein cholesterol× Triglycerides× Diastolic blood pressure× Subcutaneous fat ↓ Abdominal fat ↓ Abdominal visceral fat ↓ Mid-thigh fat area ↓ Body mass index ↓ Body fat× Fat free mass×Mid-thigh skeletal muscle×Fat mass×weight ↓ Peak oxygen uptake ↑ Oxygen uptake at lactate threshold× Tidal volume ↑ Metabolic equivalent of task—heart work× Basal metabolic rate× |
| Nitkiewicz et al., 2023 [17] | n = 4 ♀ ♂ y = 25 ± 1 | Accourity, Focus | VA-OQ2+HMD PA-OT, CT | - | Occasional training ↑ 1 week break ↑ Repetition ↑ Focus ↑ Continuous training ↓ Reflexes ↓ Focus ↓ |
| Wang, 2023 [31] | n = 78 ♀ n = 20 ♂ y = 72.16 ± 4.9 | Demographic characteristics of participants, Senior fitness test | E- VA+SFT CG-SFT | 1 w × 150 min 12 w | Upper body flexibility ↑ Lower body flexibility ↑ Upper body strength ↑ Lower body strength ↑ Cardiorespiratory ↑ Balance ↑ |
| Park et al., 2015 [42] | n = 30 ♀ ♂ y = 65+ | Gander, Age, Height, Weight, Sway length, Average sway speed, Timed up and go | VABE | 3 × 30 min 8 w | Balance sheets ↑ Sway length ↓ Average sway speed ↑ Timed up and go ↑ |
| Ross-Stewart et al., 2018 [43] | n = 27 ♂ y = 18–23 | Skill imagery, Goals imagery, Mastery imagery, Practicing automaticity, Practicing relaxation, Practicing self-talks, Practicing imagery, Self-talk competition, Competition automaticity, Imagery competition, Negative thinking competition, Strategy imagery ability, Affect imagery, Activation, Goal setting, Automaticity, Emotional control, Imagery, Relaxation | VA-SIAQ TPSQ | 2 × 15 min-1d (11 ses) 12 w | Goals imagery ↑ Skill imagery ↑ Imagery competition ↑ Practicing automaticity ↑ Practicing relaxation ↑ Practicing self-talks ↑ Practicing imagery ↑ Competition automaticity ↑ Self-talk competition ↑ Negative thinking competition ↑ Mastery imagery ↑ |
| Daveri et al., 2022 [44] | n = 21 ♂ y = 23.1 ± 1.5 | Weight, Height, Body mass index, Waist circumference, The sit and reach, Shoulders flexion and extension, One leg balance, Maximum push up, Maximal plank, Resting heart rate | LS VR WP | 1 w × 3 tm 5 w | Body mass index×Waist circumference ↓ Maximum push up ↑ Maximal plank ↑ Hand grip ↑ Shoulder flexion and extension ↑ Resting heart rate ↑ |
| Harris et al., 2020 [45] | n = 18 ♂ y = 29.2 | Virtual reality golf putting, Real-world golf putting, Eye tracking, Putting performance, Quiet eye period | VR-EX1-PWM VR-EX2-RWT | EX1-1d EX2-3d | E1: Real-world golf putting× Putting performance ↓ Quiet eye period× E2: Real world golf putting- Putting performance ↑ Quiet eye period× VR golf putting–Real-world golf putting× |
| Gani et al., 2023 [46] | n = 40 ♂ y = 19–24 | 20 m shuttle run, 30 m sprint run, Horizontal jump, Leg dynamometer, Subjective well-being, Social well-being, Psychological well-being | E-VA+TT CG-DTA | 8 w | Depression ↓, Accuracy ↓ 20 m shuttle run ↑, 30 m sprint run ↑ Horizontal jump ↑ Leg dynamometer ↑ Subjective well-being ↑ Social well-being ↑ Psychological well-being ↑ |
| Gray, 2017 [47] | n = 80 ♂ y = 17–18 | Total number of hits, % of swings at pitches inside the strike zone, % swings at pitches outside of strike zone | ATBVE ESBPVE EFSRB CCIAT | 2 × 45 min 6 w | % of swings at pitches outside of strike zone ↑ Total number of hits ↑ |
| McClure et al., 2019 [48] | n = 29 ♀ ♂ y = 18+ | Heart Rate, Body sensations, Video recording | VA-VRC PA-NVRC | 2 × 6–12 min 1 d | Heart rate ↑ Body sensations ↑ Video recording ↑ |
| Reference | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Oginni et al. (2022) [33] | + | + | + | + | − | − | + | − | − | + | + | 7 |
| Eckmann et al. (2021) [34] | + | + | + | − | − | − | + | + | − | + | + | 7 |
| de Melo Ghisi et al. (2024) [35] | + | + | + | + | − | − | − | − | − | + | + | 6 |
| Mokmin et al. (2021) [16] | + | − | − | + | − | − | − | − | + | + | + | 5 |
| Chau et al. (2021) [36] | + | + | + | − | − | − | − | − | + | + | + | 6 |
| McDaniel et al. (2022) [37] | − | + | − | + | − | − | + | − | + | + | + | 6 |
| Proffitt et al. (2015) [38] | + | + | − | − | − | − | − | − | − | + | + | 4 |
| Suderman et al. (2022) [39] | + | + | − | + | − | − | − | − | + | + | + | 6 |
| Seo et al. (2023) [14] | + | + | − | − | − | − | − | + | − | + | + | 5 |
| Touloudi et al. (2022) [15] | + | + | + | + | − | − | + | − | + | + | + | 8 |
| Rutkowski et al. (2020) [30] | + | + | + | − | + | − | − | − | + | + | + | 7 |
| Maden et al. (2022) [40] | + | + | − | + | − | − | − | − | + | + | + | 6 |
| Nitkiewicz et al. (2023) [17] | − | + | + | − | − | − | − | − | − | + | + | 4 |
| Irving et al. (2008) [41] | + | + | + | − | + | − | − | + | − | + | + | 7 |
| Wang (2023) [31] | + | + | + | + | − | + | − | − | − | + | + | 7 |
| Park et al. (2015) [42] | + | + | − | + | − | − | − | + | − | + | + | 6 |
| Daveri et al. (2022) [44] | + | − | − | + | − | − | − | + | − | + | + | 5 |
| Ross-Stewart et al. (2018) [43] | + | + | + | − | − | − | + | + | − | + | + | 7 |
| Harris et al. (2020) [45] | + | − | + | + | − | − | − | + | − | − | + | 5 |
| Gani et al. (2023) [46] | + | + | + | + | + | − | − | − | − | + | + | 7 |
| Gray (2017) [47] | + | + | − | − | − | − | − | + | + | + | + | 6 |
| McClure et al. (2019) [48] | + | + | − | + | − | − | − | − | − | − | + | 4 |
| Reference | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| Oginni et al. (2022) [33] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Eckmann et al. (2021) [34] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| de Melo Ghisi et al. (2024) [35] | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| Mokmin et al. (2021) [16] | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 2 |
| Chau et al. (2021) [36] | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| McDaniel et al. (2022) [37] | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| Proffitt et al. (2015) [38] | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 3 |
| Suderman et al. (2022) [39] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Seo et al. (2023) [14] | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 2 |
| Touloudi et al. (2022) [15] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Rutkowski et al. (2020) [30] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Maden et al. (2022) [40] | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Nitkiewicz et al. (2023) [17] | 0 | 0 | 1 | 0 | 0 | 2 | 0 | 3 |
| Irving et al. (2008) [41] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Wang (2023) [31] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Park et al. (2015) [42] | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| Daveri et al. (2022) [44] | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 2 |
| Ross-Stewart et al. (2018) [43] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Harris et al. (2020) [45] | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Gani et al. (2023) [46] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gray (2017) [47] | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| McClure et al. (2019) [48] | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 3 |
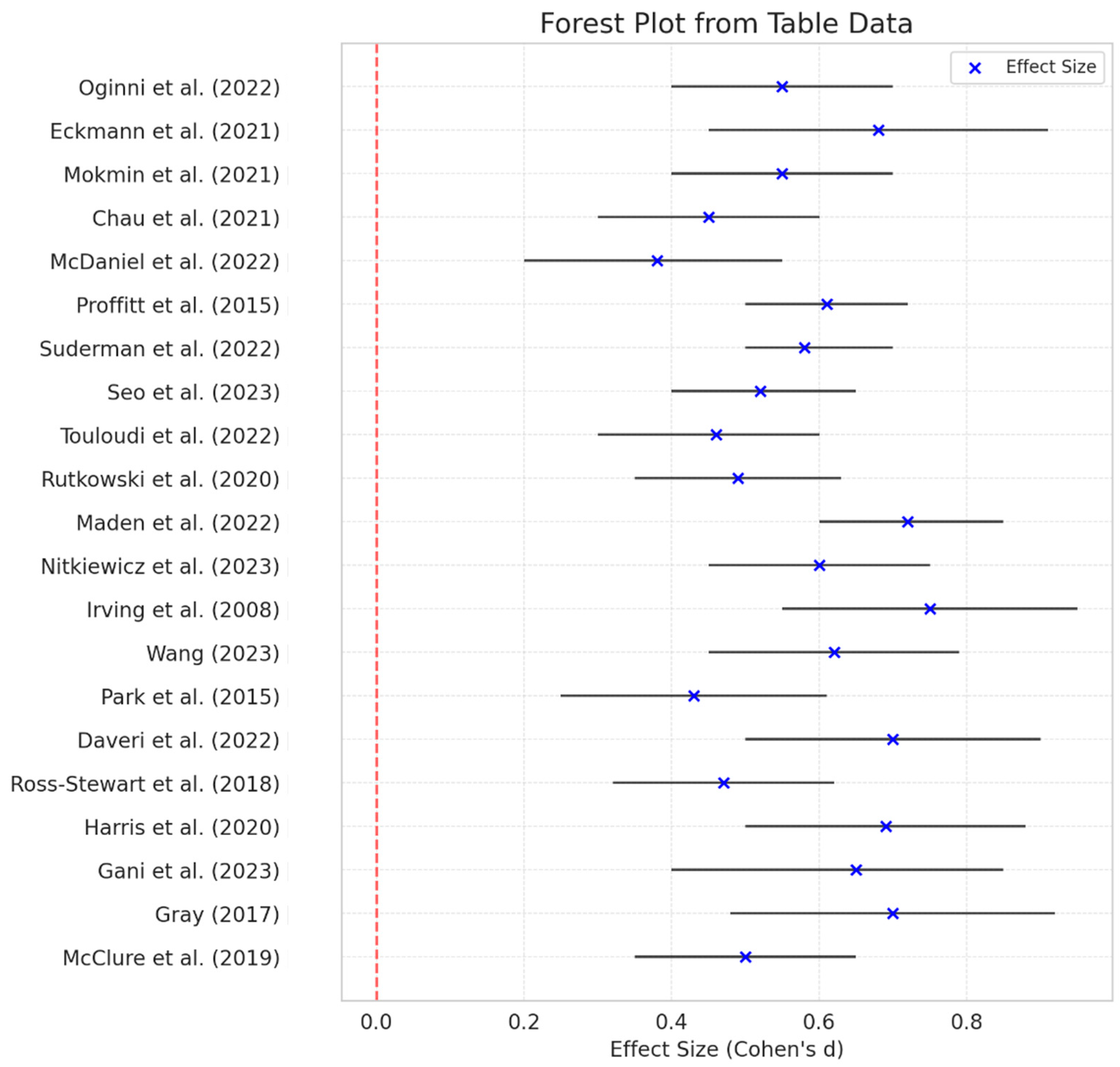
| Reference | Effect Size (Cohen’s d) | Lower CI | Upper CI |
|---|---|---|---|
| Oginni et al. (2022) [33] | 0.55 | 0.4 | 0.7 |
| Eckmann et al. (2021) [34] | 0.68 | 0.45 | 0.91 |
| de Melo Ghisi et al. (2024) [35] | / | / | / |
| Mokmin et al. (2021) [16] | 0.55 | 0.4 | 0.7 |
| Chau et al. (2021) [36] | 0.45 | 0.3 | 0.6 |
| McDaniel et al. (2022) [37] | 0.38 | 0.2 | 0.55 |
| Proffitt et al. (2015) [38] | 0.61 | 0.5 | 0.72 |
| Suderman et al. (2022) [39] | 0.58 | 0.5 | 0.7 |
| Seo et al. (2023) [14] | 0.52 | 0.4 | 0.65 |
| Touloudi et al. (2022) [15] | 0.46 | 0.3 | 0.6 |
| Rutkowski et al. (2020) [30] | 0.49 | 0.35 | 0.63 |
| Maden et al. (2022) [40] | 0.72 | 0.6 | 0.85 |
| Nitkiewicz et al. (2023) [17] | 0.6 | 0.45 | 0.75 |
| Irving et al. (2008) [41] | 0.75 | 0.55 | 0.95 |
| Wang (2023) [31] | 0.62 | 0.45 | 0.79 |
| Park et al. (2015) [42] | 0.43 | 0.25 | 0.61 |
| Daveri et al. (2022) [44] | 0.7 | 0.5 | 0.9 |
| Ross-Stewart et al. (2018) [43] | 0.47 | 0.32 | 0.62 |
| Harris et al. (2020) [45] | 0.69 | 0.5 | 0.88 |
| Gani et al. (2023) [46] | 0.65 | 0.4 | 0.85 |
| Gray (2017) [47] | 0.7 | 0.48 | 0.92 |
| McClure et al. (2019) [48] | 0.5 | 0.35 | 0.65 |
| Variable | Mean ± SD | p-Value | Effect Size |
|---|---|---|---|
| Physical Aspects | 74.3 ± 8.2 | 0.0029 | Very Large |
| Cognitive Aspects | 82.1 ± 6.7 | 0.0022 | Extremely Large |
| Health Aspects | 77.5 ± 7.9 | 0.0069 | Very Large |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hajder, Đ.; Bjelica, B.; Bubanj, S.; Aksović, N.; Marković, M.; Arsenijević, R.; Lupu, G.-S.; Gašić, T.; Sufaru, C.; Toskić, L.; et al. A Systematic Review and Meta-Analysis of Virtual and Traditional Physical Activity Programs: Effects on Physical, Health, and Cognitive Outcomes. Healthcare 2025, 13, 711. https://doi.org/10.3390/healthcare13070711
Hajder Đ, Bjelica B, Bubanj S, Aksović N, Marković M, Arsenijević R, Lupu G-S, Gašić T, Sufaru C, Toskić L, et al. A Systematic Review and Meta-Analysis of Virtual and Traditional Physical Activity Programs: Effects on Physical, Health, and Cognitive Outcomes. Healthcare. 2025; 13(7):711. https://doi.org/10.3390/healthcare13070711
Chicago/Turabian StyleHajder, Đorđe, Bojan Bjelica, Saša Bubanj, Nikola Aksović, Milan Marković, Radenko Arsenijević, Gabriel-Stănică Lupu, Tomislav Gašić, Constantin Sufaru, Lazar Toskić, and et al. 2025. "A Systematic Review and Meta-Analysis of Virtual and Traditional Physical Activity Programs: Effects on Physical, Health, and Cognitive Outcomes" Healthcare 13, no. 7: 711. https://doi.org/10.3390/healthcare13070711
APA StyleHajder, Đ., Bjelica, B., Bubanj, S., Aksović, N., Marković, M., Arsenijević, R., Lupu, G.-S., Gašić, T., Sufaru, C., Toskić, L., Dobreci, D.-L., Dobrescu, T., & Sava, M. A. (2025). A Systematic Review and Meta-Analysis of Virtual and Traditional Physical Activity Programs: Effects on Physical, Health, and Cognitive Outcomes. Healthcare, 13(7), 711. https://doi.org/10.3390/healthcare13070711