Abstract
Background: Solid organ transplant (SOT) recipients have an elevated risk of diabetes mellitus (DM). This study investigated the risk of posttransplant DM (PTDM) in a retrospective cohort study. Methods: We analyzed patients aged over 18 years who received an SOT between 2002 and 2013. Each patient was matched with four control individuals by age, sex, insured salary, urbanization level, Charlson’s comorbidity index (CCI), and year of inclusion in the study. After matching, the study comprised 6874 patients who underwent an SOT and 27,496 matched general patients as the comparison. The risk of DM among the SOT recipients was assessed using a Cox proportional hazards model after adjustment for all relevant variables. Results: The SOT cohort had a significantly higher risk of DM than general patients (adjusted hazard ratio [aHR], 1.61; 95% confidence interval [CI], 1.51–1.72). Kidney and liver recipients, respectively, had DM incidence rates 1.57 (95% CI, 1.46–1.70) and 1.73 (95% CI, 1.53–1.94) times that of the general patients. Conclusions: SOT recipients had an elevated risk of DM. Among various organ recipients, liver recipients had the highest PTDM risk. Kidney and liver recipients demonstrated the highest DM risk at 6 months after their SOT. The risk of PTDM following an SOT may result in long-term consequences. Hence, we advise the critical need for proper management to mitigate related complications after transplantation.
1. Introduction
A solid organ transplant (SOT) is a therapeutic option for patients with chronic disease resulting from end-stage organ dysfunction and improves survival and quality of life [1,2]. In 2014, the International Expert Panel recommended a shift in terminology from new onset diabetes after transplantation (NODAT) back to posttransplant diabetes mellitus (PTDM) [3]. NODAT was used routinely before 2014 [4]. However, PTDM refers to the time of diagnosis rather than the time of occurrence. Specifically, PTDM refers to DM newly diagnosed after a transplant, irrespective of timing and whether DM was undetected prior to the transplant [3].
PTDM is a common complication following an SOT [5], with metabolic disturbances associated with various adverse outcomes that may increase the risks of morbidity and mortality [6]. PTDM is associated with a gradual decline in organ function, particularly in patients with longer survival periods [7,8]. The prevalence of PTDM after an SOT differs depending on the type of organ transplanted [9,10,11,12]. The incidence of PTDM following an SOT may also vary depending on the duration of the follow-up period [3,13]. Clinicians need a thorough understanding of the risk of PTDM following an SOT to effectively prevent relative complications. To address this, we conducted a retrospective cohort study using data from Taiwan’s National Health Insurance Research Database (NHIRD) between 2001 and 2018. This study aimed to examine the risk of PTDM across different types of SOTs and assess how the risk varies over different follow-up periods.
2. Materials and Methods
2.1. Data Sources
This study was a secondary analysis of data from the NHIRD on patients who underwent transplants at any point between 2001 and 2018. The NHIRD is a nationally representative database maintained by the Health and Welfare Data Science Center (HWDC) of the Ministry of Health and Welfare and includes detailed clinical records from both the inpatient and outpatient claims of the beneficiaries of Taiwan’s National Health Insurance program. This program has provided coverage for up to 99% of the country’s population since 1995. The NHIRD can serve as a foundation for the procurement of real-world evidence to support clinical decisions and health-care policy-making [14,15]. Diagnostic data within the NHIRD from before 2016 and from 2016 or later are, respectively, coded using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes.
2.2. Ethics Statement
The work reported is in line with the STROCSS criteria [16]. Because the HWDC encrypts personally identifying data to protect the privacy of beneficiaries, this study was exempt from obtaining informed consent. This study protocol received an ethical review and approval by the Institutional Review Board of Chung Shan Medical University Hospital, Taiwan (No. CSMUH CS2-21134).
2.3. Study Participants
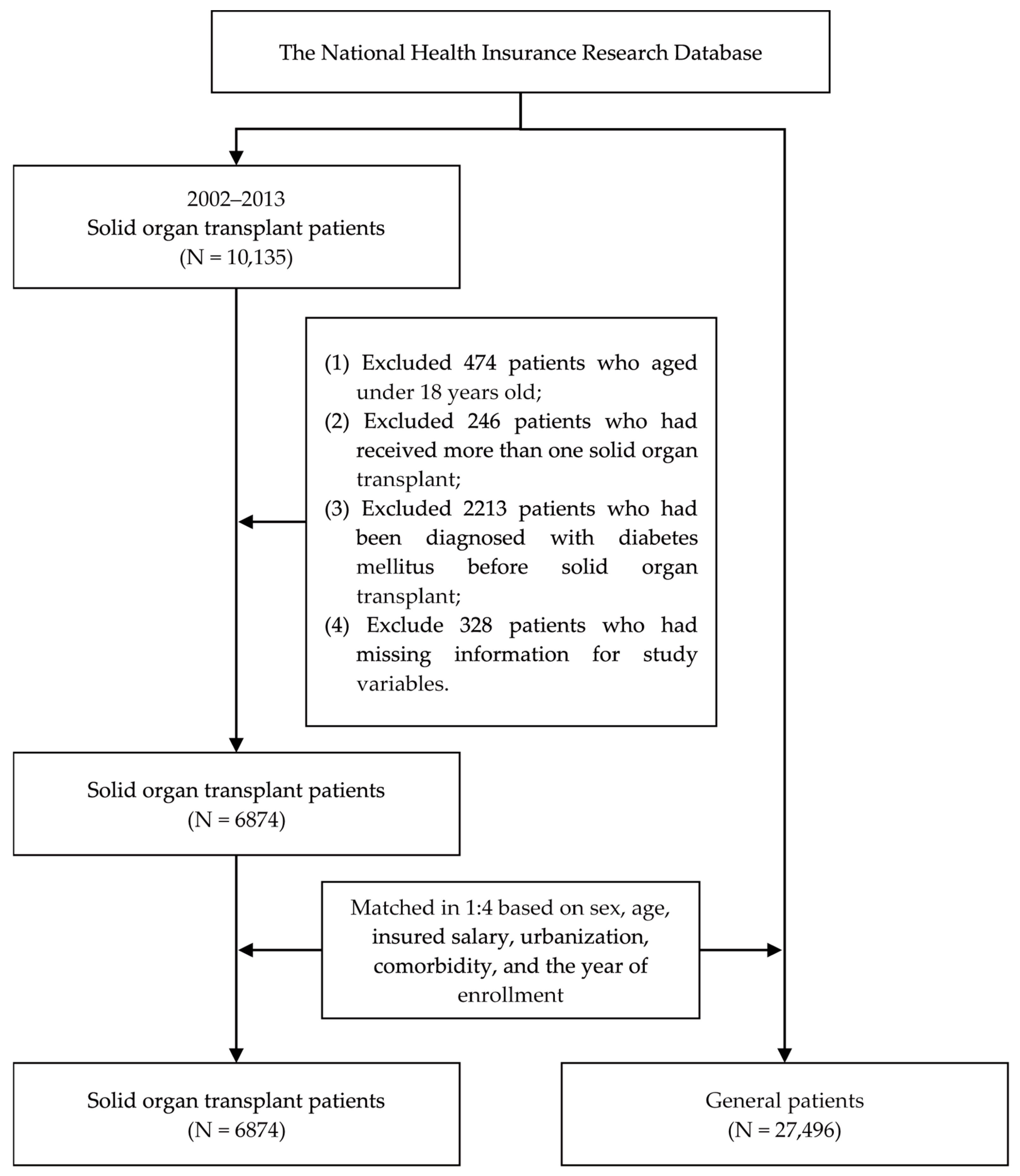
We enrolled patients aged over 18 years who underwent SOTs between 2002 and 2013, specifically, kidney (ICD-9-CM code V42.0), liver (ICD-9-CM code V42.7), or lung (ICD-9-CM code V42.6) transplants. Patients were excluded from our study if they received more than one SOT, had a DM diagnosis before their SOT, or had incomplete medical information in the NHIRD. This study used general patients without any DM diagnosis patients as the control group. To minimize potential selection bias resulting from the use of unbalanced covariates in observational studies, we employed 1:4 propensity score matching (PSM) to establish a matched cohort. PSM is a statistical matching technique that can be used to reduce potential confounding caused by unbalanced covariates in non-experimental settings. A propensity score is a probability that is calculated using a logistic regression model. The score is a unit of a certain characteristic assigned to a patient who received an SOT. These scores can help reduce or eliminate selection bias in observational studies by accounting for the characteristics of control individuals. We selected sex, age, insured salary, the urbanization level, Charlson’s comorbidity index (CCI), and the year of inclusion in the study as characteristics for matching. After matching, this study comprised 6874 patients who underwent an SOT and 27,496 matched general patients as the comparison. The patient selection process is presented in Figure 1.
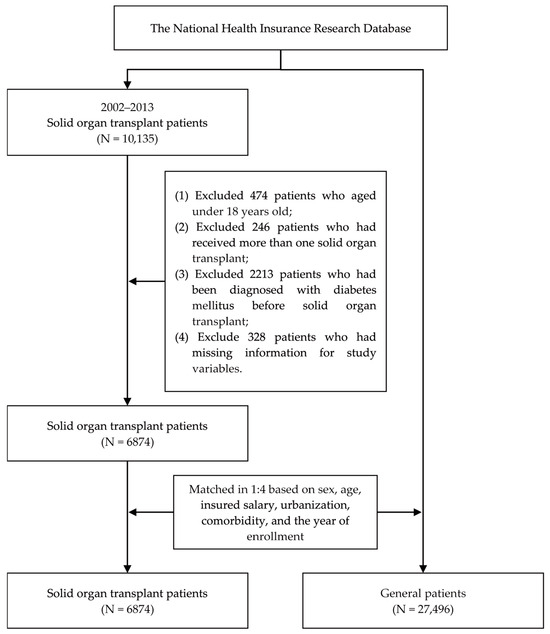
Figure 1.
Flowchart of the patient selection process.
2.4. Study Design
This retrospective cohort study investigated the risk of DM (ICD-9-CM code 250 or ICD-10-CM code E10–E14) by using data from the NHIRD of Taiwan. The date of an SOT was defined as the observation start date for SOT recipients, and the same date was assigned as the observation start date for corresponding members of the control group. To investigate the risk of DM, all participants were followed up until they were diagnosed with DM, died, or at the end of 2018, whichever occurred first. The comorbidities included in the analysis were hypertension (ICD-9-CM 401-405), hyperlipidemia (ICD-9-CM codes 272.0–272.4), obesity (ICD-9-CM code 287.0), rheumatoid arthritis (RA, ICD-9-CM code 714), inflammatory bowel disease (IBD, ICD-9-CM codes 555 and 556), hyperuricemia (ICD-9-CM code 790.6), cytomegalovirus (CMV, ICD-9-CM code 078.5), hepatitis B virus (HBV, ICD-9-CM codes 070.2 and 070.3), hepatitis C virus (HCV, ICD-9-CM codes 070.4, 070.5 and 070.70), sleep disturbance (ICD-9-CM code 780), and periodontitis (ICD-9-CM code 523).
2.5. Statistical Analysis
All statistical analyses in our study were conducted using SAS software version 9.4 (SAS Institute., Cary, NC, USA), with statistical significance indicated by p < 0.05. Chi-square tests were used to evaluate the distributions of baseline characteristics. In terms of multivariable analysis, given that our primary outcome (incident DM) is a time-to-event variable, a Cox proportional hazards model was employed to investigate the association between DM and undergoing an SOT after adjustment for all relevant variables. Results are presented as hazard ratios (HRs) with 95% confidence intervals (CIs). The sex, age, insured salary, urbanization, CCI, and comorbidities were the control variables to adjust the hazard ratio of the risk of incident DM. SOT recipients had an increased risk of DM at different periods after organ transplantation; thus, we conducted a sensitivity analysis at 6-month, 1-year, 3-year, and 5-year follow-ups [17]. A sensitivity analysis was also conducted to examine the risk of DM among SOT recipients after different follow-up periods, namely, 6 months and 1, 3, and 5 years.
3. Results
The mean follow-up period was 8.16 ± 3.41 years, and 5092 patients developed DM in 34,370 study individuals. Table 1 presents the baseline characteristics of the SOT recipients and matched control patients. Of the 34,370 study individuals, 19,732 were men and 14,638 were women. Of these patients, 6874 patients had undergone SOTs and 27,496 were matched controls. The average ages of the SOT recipients and matched controls were 47.52 ± 14.68 and 47.22 ± 11.73 years, respectively. Sex, age, insured salary, urbanization, and CCI did not differ significantly between the groups (p > 0.05). Among the 6874 SOT recipients, 3084 (44.86%) had hypertension, 874 (12.71%) had hyperlipidemia, 46 (0.67%) had RA, 28 (0.41%) had IBD, 201 had hyperuricemia (2.92%), 94 (1.37%) had CMV, 1493 (21.72%) had HBV, 663 (9.65%) had HCV, 1504 (21.88%) had sleep disturbance, and 44 (0.64%) had periodontitis. The distribution of each of the aforementioned comorbidities among the SOT cohort differed significantly from that of the matched cohort (p < 0.001).

Table 1.
Baseline characteristics of the study subjects after matching.
Table 2 presents the risks of incident DM in the SOT and matched cohorts. In total, 5092 patients (14.82%) developed DM, 1443 patients (20.99%) of whom underwent SOTs. The DM incidence rates were 1.34 and 2.24 per 1000 person-years in the matched and SOT cohorts, respectively. In total, 2128 women (14.54%) and 2964 men (15.02%) developed DM; the incidence rates were 1.44 and 1.57 per 1000 person-years, respectively. Among the recipients of a kidney, liver, or lung, 956 (21.05%), 480 (21.09%), and 7 (12.28%), respectively, developed DM, for respective incidence rates of 2.12, 2.56, and 1.25 per 1000 person-years. Patients with hypertension, hyperuricemia, HCV, or sleep disturbances were more likely to develop DM than those without comorbidities.
Table 2.
The multivariable analysis of the risk of incident diabetes mellitus via a Cox proportional hazard model.
With adjustments for confounding variables, the SOT cohort had a significantly higher risk of incident DM (adjusted HR [aHR], 1.61; 95% CI, 1.51–1.72) than the matched cohort. The incidence of DM among kidney and liver transplants was 1.57 times (95% CI, 1.46–1.70) and 1.73 (95% CI, 1.53–1.94) times that of the matched cohort, respectively. Patients with comorbid hypertension (aHR, 1.21; 95% CI, 1.13–1.28), hyperuricemia (aHR, 1.43; 95% CI, 1.20–1.71), HCV (aHR, 1.40; 95% CI, 1.24–1.58), or sleep disturbance (aHR, 1.10; 95% CI, 1.03–1.17) had a higher risk of incident DM after adjusting for relevant variables.
Table 3 presents the results of a sensitivity analysis conducted to investigate DM risk after various follow-up periods. Compared to the matched cohort, the SOT cohort had higher risks of incident DM after 6 months (aHR, 2.01; 95% CI, 1.67–2.42) and 1 (aHR, 1.83; 95% CI, 1.58–2.13), 3 (aHR, 1.94; 95% CI, 1.74–2.16), and 5 (aHR, 1.73; 95% CI, 1.58–1.90) years. Furthermore, kidney and liver recipients had higher risks of incident DM after 6 months and 1, 3, and 5 years.
Table 3.
Sensitivity analysis to investigate the risk of incident diabetes mellitus at different follow-up periods.
4. Discussion
Large-scale epidemiological studies have investigated the risk of DM after an SOT. In this large population-based study, we found that SOT recipients had a higher risk of DM. Among the recipients of different organs, liver transplant recipients had the highest DM risk, that is, a 1.72-fold likelihood of developing DM. Renal transplant recipients had a 1.57-fold likelihood of developing DM. However, lung transplant recipients did not exhibit an elevated risk of DM. SOT recipients with comorbid hypertension, HCV, hyperuricemia, or sleep disturbances had a higher risk of DM than those without these comorbidities. Kidney and liver transplant recipients had the highest risks of DM at 6 months after their transplants; this heightened risk persisted, even after 1, 3, and 5 years.
In the current study, people with SOTs had a higher risk of DM than matched controls. The pathogenesis of PTDM is multifactorial. The pathogenesis of PTDM mainly involves pancreatic β-cell dysfunction and insulin resistance [18]. However, a study indicated that β-cell dysfunction alone is the major factor contributing to DM in kidney recipients [19]. The pathogenesis of PTDM is similar to that of type 2 DM, sharing characteristics such as insulin resistance, hypertriglyceridemia, obesity, decompensated insulin release, hypertension, and low-grade inflammation [20,21]. However, the underlying mechanisms of the two conditions may differ [22]. Nevertheless, impairments in insulin-mediated glucose uptake in peripheral tissue [23,24], insulin-mediated suppression of hepatic glucose output [24], insulin release [25], and the incretin axis between the gut and pancreas [26] (reinforcing the impairment of β-cell function and enhancing glucagon production) are common to both T2DM and PTDM. Increased renal gluconeogenesis and proximal tubular sodium–glucose reabsorption are present in T2DM [27] but have not been observed in PTDM
In addition to the transplanted organ, factors that may affect the incidence of PTDM include age, race, body mass index, and immunosuppression regimen [22]. PTDM is associated with long-term graft function impairment, decreased graft survival, increased risks of cardiovascular disease and infection, and acute graft rejection [7,8].
Compared with cyclosporine A, tacrolimus can improve graft survival and prevent acute rejection after transplantation, but it contributes to an increase in the occurrence of PTDM [28,29]. Therefore, as the most commonly used immunosuppressants after transplantation, blood glucose concentrations should be closely monitored in recipients taking tacrolimus [28,30]. However, we did not analyze the relationship between immunosuppressive drugs and the occurrence of PTDM in SOT recipients.
The current study discovered that, among the recipients of different organs, liver recipients had the highest risk of PTDM, specifically a 1.72-fold likelihood of DM; prior studies have indicated that PTDM occurs in 12–45% of liver recipients [3,31,32]. Another study indicated that PTDM is a significant causal factor of morbidity and mortality in liver recipients [33]. Liver transplant recipients with sustained PTDM had significantly higher risks of death due to infection, graft failure resulting from chronic graft rejection, and late-onset thrombosis of the hepatic artery [34].
The current study found that kidney recipients had a 1.57-fold likelihood of developing DM. One study found that DM incidence after renal transplants ranges between 7.9% and 50% [35]; however, another study found that DM incidence after such transplants ranges between 10% and 20% [22]. PTDM has been associated with an increased mortality, which is well documented in recipients who have received kidney and heart transplants [22,36]. Furthermore, PTDM has been associated with decreased graft survival [37,38], premature cardiovascular disease, and death in renal transplant recipients [39].
The current study found no association between lung transplants and PTDM. Previous study indicated that DM is a significant concern for lung transplant recipients. Pre-existing DM diagnosed before lung transplantation adversely impacts posttransplant survival in patients with cystic fibrosis. Patients with cystic fibrosis and pre-existing DM experience reduced survival rates compared to those with cystic fibrosis who do not have pre-existing DM [40].
The risk factors for PTDM are complex and associated with numerous variables [18]. PTDM is more likely in patients with pre-existing risk factors for T2DM, including older age, male sex, a family history of T2DM, a high-risk ethnicity, and obesity [1,41]. In the current study, people with SOTs and aged 51–60 years had the highest DM risk. Additionally, male patients had a higher risk than female patients. PTDM is a common complication in lung transplant recipients taking tacrolimus-based immunosuppression [42].
Age is a major risk factor for PTDM. With advancing age, islet β cells age and undergo apoptosis, resulting in decreased insulin secretion, increased insulin resistance, and a 2.2-fold increase in PTDM risk for SOT recipients older than 45 years [22]. Another study indicated that an age of >55 years is a significant risk factor for PTDM [43]. Furthermore, older age is independently correlated with a higher risk of irreversible PTDM [18].
The current study also found that patients with higher CCIs, particularly those >2, had a higher PTDM risk. Age and CCI are the two primary risk factors for PTDM across all time periods [44]. Moreover, PTDM is more prevalent among male SOT recipients than among female SOT recipients [45].
The current study observed that SOT recipients with comorbid hypertension, HCV, hyperuricemia, or sleep disturbances had a higher PTDM risk than those without these comorbidities. Risk factors for PTDM, including insulin resistance, hypertension, hypertriglyceridemia, and obesity, are similar to those for T2DM, but PTDM is influenced by specific predisposing posttransplant factors [36]. Hypertension is a risk factor for DM after renal transplants [46]. High serum uric acid levels are associated with a higher PTDM risk in kidney recipients, independently of metabolic syndrome components and transplant-related variables, including immunosuppressive therapy, HCV, and CMV [47]. HCV is a PTDM risk factor [48] and has been associated with a 2.5- to 4-fold relative risk of PTDM after liver transplants [9,49,50,51]. HCV can induce posttransplant insulin resistance [52]. Several meta-analyses have indicated that patients with HCV have higher risks of mortality and graft loss after renal transplants than those without transplants [53,54]. CMV is another comorbidity associated with PTDM. Because of immunosuppression, CMV infection is a common complication of transplants [36]. CMV infection may also play a role in the pathogenesis of PTDM because it is associated with an increased PTDM risk [55]. CMV induces the secretion of proinflammatory cytokines and the destruction of pancreatic β cells [1]. However, we found that SOT recipients with comorbid CMV infection did not have a higher risk for PTDM. A systematic review and meta-analysis identified sleep disturbances as a risk factor for DM [56].
The current study discovered that kidney and liver recipients had the highest PTDM risk 6 months after their transplants, a risk that remained high even after 1, 3, and 5 years. The 2014 international consensus meeting on PTDM identified two critical periods for assessment: 46–365 days and >365 days after the procedure [3]. The incidence of PTDM follows a biphasic pattern, with the first peak occurring in the first few months and the second over the subsequent 2–3 years [13]. One study observed the highest PTDM incidence at 46–365 days after the SOT [44]. In addition, age and CCI were the two primary risk factors for PTDM for all investigated periods [44]. Another study observed the highest PTDM incidence within 6 months after the procedure [57]. Furthermore, the incidence of PTDM was discovered to be 20.5% at 6 months after renal transplants [58]. A Taiwanese population-based study indicated that the PTDM incidence was the highest within the first year after a renal transplant [59]. Among lung transplant recipients, 33% had PTDM after 3 months, 30% had PTDM after 1 year, and 24% had PTDM after 2 years [22]. However, the decline in PTDM could indicate a competing risk estimate, considering more recipients with PTDM died during the first year [22].
The current study suggests that patients with PTDM require regular glucose monitoring and the early intervention of the endocrinologist with timely treatment of hyperglycemia to improve long-term outcomes. An awareness and identification of PTDM are important. Thus, understanding PTDM would help in reducing severe complications and minimizing its impact following transplantation.
The present study has several strengths. First, it employed a nationwide population-based study design. Patients were selected from the entire population of Taiwan and followed for extended periods, thereby yielding a large, representative sample with high statistical utility. The population-based design may have minimized selection bias, which is common in observational studies. Second, we investigated the risk of DM in SOT recipients at different time points after their transplants at 6 months and 1, 3, and 5 years.
The current study also had limitations. First, some inherent flaws may be associated with retrospective cohort analysis, such as selective reporting bias and data errors. Second, we performed a retrospective cohort study using the NHIRD, which is a secondary database. The NHIRD does not include laboratory or medical examination data; thus, we could not assess diagnostic criteria per the consensus guidelines. Third, smoking habits, alcohol consumption, body mass index, HbA1c levels, personal history, physical activity, and dietary habits are associated with PTDM risk, but related data could not be accessed for this study. Although information such as smoking habits and alcohol consumption cannot be obtained from the NHIRD, this study includes the total population of the nation; thus, this large sample size study was representative, which may increase statistical precision. There is no doubt about the representativeness of this study. Fourth, all diagnoses in this study were based on ICD-9-CM or ICD-10-CM codes. However, the Bureau of the National Health Insurance in Taiwan randomly reviews charts and conducts patient interviews to ensure diagnostic accuracy, which bolsters the validity and accuracy of the analyzed NHIRD data. We acknowledge the possibility that we did not control for some confounding variables.
5. Conclusions
This study provides large-scale, population-based, longitudinal evidence that SOT recipients experience an elevated DM risk. Among the recipients of different organs, the liver recipients had the highest PTDM risk. The risk of PTDM following an SOT could have long-term consequences. Therefore, we emphasize the importance of effective management DM to reduce associated complications following transplantation.
Author Contributions
Conceptualization, C.-J.T., K.-H.H., C.-N.W. and C.-Y.L.; Formal analysis, S.-Y.G., S.-W.H., K.-Y.S. and T.-H.T.; Methodology, C.-J.T., K.-H.H., J.-Y.W., C.-N.W. and C.-Y.L.; Validation, J.-Y.W., S.-Y.G., C.-N.W. and C.-Y.L.; Writing—original draft, C.-J.T., K.-H.H., C.-N.W. and C.-Y.L.; Writing—review and editing, C.-J.T., K.-H.H., J.-Y.W., C.-N.W. and C.-Y.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Chung Shan Medical University Hospital, Taiwan (CSH-2023-C-049), China Medical University Taiwan (CMU113-ASIA-12), and the National Science and Technology Council Taiwan (MOST 111-2410-H-040-002). Funders had no role in the development or publication of this manuscript.
Institutional Review Board Statement
This study protocol received an ethical review and approval by the Institutional Review Board of Chung Shan Medical University Hospital, Taiwan (No. CSMUH CS2-21134, approval date: 6 September 2021).
Informed Consent Statement
Because the HWDC encrypts personally identifying data to protect the privacy of beneficiaries, this study was exempt from obtaining informed consent.
Data Availability Statement
The database used to support the findings of this study was provided by the Health and Welfare Data Science Center, Ministry of Health and Welfare (HWDC, MOHW) under license and cannot be made freely available. Requests for access to these data should be made to HWDC (https://dep.mohw.gov.tw/dos/cp-5119-59201-113.html, accessed on 20 October 2024).
Acknowledgments
We are grateful to Chung Shan Medical University Taiwan, Chung Shan Medical University Hospital Taiwan, China Medical University Taiwan, and Asia University Taiwan for providing administrative, technical, and funding support that has contributed to the completion of this study. This study is based, in part, on data released by the Health and Welfare Data Science Center, Ministry of Health and Welfare. The interpretation and conclusions contained herein do not represent those of the Ministry of Health and Welfare.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ahmed, S.H.; Biddle, K.; Augustine, T.; Azmi, S. Post-Transplantation Diabetes Mellitus. Diabetes Ther. 2020, 11, 779–801. [Google Scholar] [CrossRef]
- Black, C.K.; Termanini, K.M.; Aguirre, O.; Hawksworth, J.S.; Sosin, M. Solid organ transplantation in the 21(st) century. Ann. Transl. Med. 2018, 6, 409. [Google Scholar] [CrossRef] [PubMed]
- Sharif, A.; Hecking, M.; de Vries, A.P.; Porrini, E.; Hornum, M.; Rasoul-Rockenschaub, S.; Berlakovich, G.; Krebs, M.; Kautzky-Willer, A.; Schernthaner, G.; et al. Proceedings from an international consensus meeting on posttransplantation diabetes mellitus: Recommendations and future directions. Am. J. Transplant. 2014, 14, 1992–2000. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.A.; Wilkinson, A.; International Expert Panel on New-Onset Diabetes after Transplantation. New-Onset Diabetes After Transplantation 2003 International Consensus Guidelines: An endocrinologist’s view. Diabetes Care 2004, 27, 805–812. [Google Scholar] [CrossRef]
- Munshi, V.N.; Saghafian, S.; Cook, C.B.; Werner, K.T.; Chakkera, H.A. Comparison of post-transplantation diabetes mellitus incidence and risk factors between kidney and liver transplantation patients. PLoS ONE 2020, 15, e0226873. [Google Scholar] [CrossRef]
- Dong, M.; Parsaik, A.K.; Eberhardt, N.L.; Basu, A.; Cosio, F.G.; Kudva, Y.C. Cellular and physiological mechanisms of new-onset diabetes mellitus after solid organ transplantation. Diabet. Med. 2012, 29, e1–e12. [Google Scholar] [CrossRef]
- Kaposztas, Z.; Gyurus, E.; Kahan, B.D. New-onset diabetes after renal transplantation: Diagnosis, incidence, risk factors, impact on outcomes, and novel implications. Transplant. Proc. 2011, 43, 1375–1394. [Google Scholar] [CrossRef]
- Cosio, F.G.; Pesavento, T.E.; Kim, S.; Osei, K.; Henry, M.; Ferguson, R.M. Patient survival after renal transplantation: IV. Impact of post-transplant diabetes. Kidney Int. 2002, 62, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Baid, S.; Cosimi, A.B.; Farrell, M.L.; Schoenfeld, D.A.; Feng, S.; Chung, R.T.; Tolkoff-Rubin, N.; Pascual, M. Posttransplant diabetes mellitus in liver transplant recipients: Risk factors, temporal relationship with hepatitis C virus allograft hepatitis, and impact on mortality. Transplantation 2001, 72, 1066–1072. [Google Scholar] [CrossRef]
- Davidson, J.; Wilkinson, A.; Dantal, J.; Dotta, F.; Haller, H.; Hernández, D.; Kasiske, B.L.; Kiberd, B.; Krentz, A.; Legendre, C.; et al. New-onset diabetes after transplantation: 2003 International consensus guidelines. Proceedings of an international expert panel meeting. Barcelona, Spain, 19 February 2003. Transplantation 2003, 75 (Suppl. S10), SS3–SS24. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Kuo, H.T.; Sampaio, M.S.; Jiang, Y.; Bunnapradist, S. Risk factors for development of new-onset diabetes mellitus after transplant in adult lung transplant recipients. Clin. Transplant. 2011, 25, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Kuo, H.T.; Sampaio, M.S.; Jiang, Y.; Reddy, P.; Bunnapradist, S. Risk factors for development of new-onset diabetes mellitus in adult heart transplant recipients. Transplantation 2010, 89, 1526–1532. [Google Scholar] [CrossRef] [PubMed]
- Porrini, E.L.; Diaz, J.M.; Moreso, F.; Delgado Mallen, P.I.; Silva Torres, I.; Ibernon, M.; Bayes-Genis, B.; Benitez-Ruiz, R.; Lampreabe, I.; Lauzurrica, R.; et al. Clinical evolution of post-transplant diabetes mellitus. Nephrol. Dial. Transplant. 2016, 31, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.W.; Liao, K.F.; Lin, C.L.; Lin, C.C.; Lin, C.H. Longitudinal data of multimorbidity and polypharmacy in older adults in Taiwan from 2000 to 2013. Biomedicine 2020, 10, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Mathew, G.; Agha, R.; Albrecht, J.; Goel, P.; Mukherjee, I.; Pai, P.; D’Cruz, A.K.; Nixon, I.J.; Roberto, K.; Enam, S.A.; et al. STROCSS 2021: Strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int. J. Surg. 2021, 96, 106165. [Google Scholar] [CrossRef] [PubMed]
- Man Kim, J.; Hwang, S.; Lee, K.W.; Lee, J.G.; Ryu, J.H.; Kim, B.W.; Choi, D.L.; You, Y.K.; Kim, D.S.; Nah, Y.W.; et al. New-onset diabetes after adult liver transplantation in the Korean Organ Transplantation Registry (KOTRY) study. Hepatobiliary Surg. Nutr. 2020, 9, 425–439. [Google Scholar] [CrossRef]
- Zhang, Z.; Sun, J.; Guo, M.; Yuan, X. Progress of new-onset diabetes after liver and kidney transplantation. Front. Endocrinol. 2023, 14, 1091843. [Google Scholar] [CrossRef]
- Nam, J.H.; Mun, J.I.; Kim, S.I.; Kang, S.W.; Choi, K.H.; Park, K.; Ahn, C.W.; Cha, B.S.; Song, Y.D.; Lim, S.K.; et al. beta-Cell dysfunction rather than insulin resistance is the main contributing factor for the development of postrenal transplantation diabetes mellitus. Transplantation 2001, 71, 1417–1423. [Google Scholar] [CrossRef]
- Jenssen, T.; Hartmann, A. Emerging treatments for post-transplantation diabetes mellitus. Nat. Rev. Nephrol. 2015, 11, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Heldal, T.F.; Ueland, T.; Jenssen, T.; Hartmann, A.; Reisaeter, A.V.; Aukrust, P.; Michelsen, A.; Asberg, A. Inflammatory and related biomarkers are associated with post-transplant diabetes mellitus in kidney recipients: A retrospective study. Transpl. Int. 2018, 31, 510–519. [Google Scholar] [CrossRef]
- Jenssen, T.; Hartmann, A. Post-transplant diabetes mellitus in patients with solid organ transplants. Nat. Rev. Endocrinol. 2019, 15, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, A.V.; Eriksson, J.G.; Gronhagen-Riska, C.; Ahonen, P.J.; Groop, L.C. Insulin resistance and insulin deficiency in the pathogenesis of posttransplantation diabetes in man. Transplantation 1992, 53, 563–569. [Google Scholar] [CrossRef]
- Jorgensen, M.B.; Hornum, M.; van Hall, G.; Bistrup, C.; Hansen, J.M.; Mathiesen, E.R.; Feldt-Rasmussen, B. The impact of kidney transplantation on insulin sensitivity. Transpl. Int. 2017, 30, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Hecking, M.; Kainz, A.; Werzowa, J.; Haidinger, M.; Doller, D.; Tura, A.; Karaboyas, A.; Horl, W.H.; Wolzt, M.; Sharif, A.; et al. Glucose metabolism after renal transplantation. Diabetes Care 2013, 36, 2763–2771. [Google Scholar] [CrossRef]
- Halden, T.A.; Egeland, E.J.; Asberg, A.; Hartmann, A.; Midtvedt, K.; Khiabani, H.Z.; Holst, J.J.; Knop, F.K.; Hornum, M.; Feldt-Rasmussen, B.; et al. GLP-1 Restores Altered Insulin and Glucagon Secretion in Posttransplantation Diabetes. Diabetes Care 2016, 39, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Gerich, J.E. Role of the kidney in normal glucose homeostasis and in the hyperglycaemia of diabetes mellitus: Therapeutic implications. Diabet Med. 2010, 27, 136–142. [Google Scholar] [CrossRef]
- Webster, A.; Woodroffe, R.C.; Taylor, R.S.; Chapman, J.R.; Craig, J.C. Tacrolimus versus cyclosporin as primary immunosuppression for kidney transplant recipients. Cochrane Database Syst. Rev. 2005, CD003961. [Google Scholar] [CrossRef] [PubMed]
- Haddad, E.M.; McAlister, V.C.; Renouf, E.; Malthaner, R.; Kjaer, M.S.; Gluud, L.L. Cyclosporin versus tacrolimus for liver transplanted patients. Cochrane Database Syst. Rev. 2006, 2006, CD005161. [Google Scholar] [CrossRef] [PubMed]
- Muduma, G.; Saunders, R.; Odeyemi, I.; Pollock, R.F. Systematic Review and Meta-Analysis of Tacrolimus versus Ciclosporin as Primary Immunosuppression After Liver Transplant. PLoS ONE 2016, 11, e0160421. [Google Scholar] [CrossRef] [PubMed]
- Galindo, R.J.; Wallia, A. Hyperglycemia and Diabetes Mellitus Following Organ Transplantation. Curr. Diab. Rep. 2016, 16, 14. [Google Scholar] [CrossRef] [PubMed]
- Pirsch, J.D.; Henning, A.K.; First, M.R.; Fitzsimmons, W.; Gaber, A.O.; Reisfield, R.; Shihab, F.; Woodle, E.S. New-Onset Diabetes After Transplantation: Results From a Double-Blind Early Corticosteroid Withdrawal Trial. Am. J. Transplant. 2015, 15, 1982–1990. [Google Scholar] [CrossRef]
- Pelaez-Jaramillo, M.J.; Cardenas-Mojica, A.A.; Gaete, P.V.; Mendivil, C.O. Post-Liver Transplantation Diabetes Mellitus: A Review of Relevance and Approach to Treatment. Diabetes Ther. 2018, 9, 521–543. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.I.; Barbeito, R.; Faradji, R.N.; Gaynor, J.J.; Tzakis, A.G. Negative impact of new-onset diabetes mellitus on patient and graft survival after liver transplantation: Long-term follow up. Transplantation 2006, 82, 1625–1628. [Google Scholar] [CrossRef]
- Fabrizi, F.; Martin, P.; Dixit, V.; Bunnapradist, S.; Kanwal, F.; Dulai, G. Post-transplant diabetes mellitus and HCV seropositive status after renal transplantation: Meta-analysis of clinical studies. Am. J. Transplant. 2005, 5, 2433–2440. [Google Scholar] [CrossRef]
- Shivaswamy, V.; Boerner, B.; Larsen, J. Post-Transplant Diabetes Mellitus: Causes, Treatment, and Impact on Outcomes. Endocr. Rev. 2016, 37, 37–61. [Google Scholar] [CrossRef] [PubMed]
- Montori, V.M.; Basu, A.; Erwin, P.J.; Velosa, J.A.; Gabriel, S.E.; Kudva, Y.C. Posttransplantation diabetes: A systematic review of the literature. Diabetes Care 2002, 25, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Revanur, V.K.; Jardine, A.G.; Kingsmore, D.B.; Jaques, B.C.; Hamilton, D.H.; Jindal, R.M. Influence of diabetes mellitus on patient and graft survival in recipients of kidney transplantation. Clin. Transplant. 2001, 15, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Eide, I.A.; Halden, T.A.; Hartmann, A.; Asberg, A.; Dahle, D.O.; Reisaeter, A.V.; Jenssen, T. Mortality risk in post-transplantation diabetes mellitus based on glucose and HbA1c diagnostic criteria. Transpl. Int. 2016, 29, 568–578. [Google Scholar] [CrossRef]
- Belle-van Meerkerk, G.; van de Graaf, E.A.; Kwakkel-van Erp, J.M.; van Kessel, D.A.; Lammers, J.W.; Biesma, D.H.; de Valk, H.W. Diabetes before and after lung transplantation in patients with cystic fibrosis and other lung diseases. Diabet. Med. 2012, 29, e159–e162. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.D.; Chang, Y.H.; Aqel, B.A.; Byrne, T.J.; Chakkera, H.A.; Douglas, D.D.; Mulligan, D.C.; Rakela, J.; Vargas, H.E.; Carey, E.J. New Onset Diabetes Mellitus in Living Donor versus Deceased Donor Liver Transplant Recipients: Analysis of the UNOS/OPTN Database. J. Transplant. 2013, 2013, 269096. [Google Scholar] [CrossRef] [PubMed]
- Ollech, J.E.; Kramer, M.R.; Peled, N.; Ollech, A.; Amital, A.; Medalion, B.; Saute, M.; Shitrit, D. Post-transplant diabetes mellitus in lung transplant recipients: Incidence and risk factors. Eur. J. Cardio-Thorac. Surg. 2008, 33, 844–848. [Google Scholar] [CrossRef]
- Abe, T.; Onoe, T.; Tahara, H.; Tashiro, H.; Ishiyama, K.; Ide, K.; Ohira, M.; Ohdan, H. Risk factors for development of new-onset diabetes mellitus and progressive impairment of glucose metabolism after living-donor liver transplantation. Transplant. Proc. 2014, 46, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, Q.; Hornum, M.; Terrones-Campos, C.; Crone, C.G.; Wareham, N.E.; Soeborg, A.; Rasmussen, A.; Gustafsson, F.; Perch, M.; Soerensen, S.S.; et al. Posttransplantation Diabetes Mellitus Among Solid Organ Recipients in a Danish Cohort. Transpl. Int. 2022, 35, 10352. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, G.; Blohme, I.; Norden, G. Gender differences in a kidney transplant population. Nephrol. Dial. Transplant. 1997, 12, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Numakura, K.; Satoh, S.; Tsuchiya, N.; Horikawa, Y.; Inoue, T.; Kakinuma, H.; Matsuura, S.; Saito, M.; Tada, H.; Suzuki, T.; et al. Clinical and genetic risk factors for posttransplant diabetes mellitus in adult renal transplant recipients treated with tacrolimus. Transplantation 2005, 80, 1419–1424. [Google Scholar] [CrossRef] [PubMed]
- Sotomayor, C.G.; Oskooei, S.S.; Bustos, N.I.; Nolte, I.M.; Gomes-Neto, A.W.; Erazo, M.; Gormaz, J.G.; Berger, S.P.; Navis, G.J.; Rodrigo, R.; et al. Serum uric acid is associated with increased risk of posttransplantation diabetes in kidney transplant recipients: A prospective cohort study. Metabolism 2021, 116, 154465. [Google Scholar] [CrossRef] [PubMed]
- Naing, C.; Mak, J.W.; Ahmed, S.I.; Maung, M. Relationship between hepatitis C virus infection and type 2 diabetes mellitus: Meta-analysis. World J. Gastroenterol. 2012, 18, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Gane, E.J. The natural history of recurrent hepatitis C and what influences this. Liver Transpl. 2008, 14 (Suppl. S2), S36–S44. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Jia, H.; Li, J.; Chen, X.; Zhou, H.; Tian, H. New onset diabetes mellitus after liver transplantation and hepatitis C virus infection: Meta-analysis of clinical studies. Transpl. Int. 2009, 22, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, C.J.; Cashion, A.K.; Hathaway, D.K.; Thompson, C.; Conley, Y.; Gaber, O.; Vera, S.; Shokouh-Amiri, H. Posttransplant diabetes mellitus in liver transplant recipients. Prog. Transplant. 2006, 16, 110–116. [Google Scholar] [CrossRef]
- Veldt, B.J.; Poterucha, J.J.; Watt, K.D.; Wiesner, R.H.; Hay, J.E.; Rosen, C.B.; Heimbach, J.K.; Janssen, H.L.; Charlton, M.R. Insulin resistance, serum adipokines and risk of fibrosis progression in patients transplanted for hepatitis C. Am. J. Transplant. 2009, 9, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Fabrizi, F.; Martin, P.; Dixit, V.; Messa, P. Meta-analysis of observational studies: Hepatitis C and survival after renal transplant. J. Viral Hepat. 2014, 21, 314–324. [Google Scholar] [CrossRef]
- Fabrizi, F.; Martin, P.; Dixit, V.; Bunnapradist, S.; Dulai, G. Hepatitis C virus antibody status and survival after renal transplantation: Meta-analysis of observational studies. Am. J. Transplant. 2005, 5, 1452–1461. [Google Scholar] [CrossRef] [PubMed]
- Einollahi, B.; Motalebi, M.; Salesi, M.; Ebrahimi, M.; Taghipour, M. The impact of cytomegalovirus infection on new-onset diabetes mellitus after kidney transplantation: A review on current findings. J. Nephropathol. 2014, 3, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Anothaisintawee, T.; Reutrakul, S.; Van Cauter, E.; Thakkinstian, A. Sleep disturbances compared to traditional risk factors for diabetes development: Systematic review and meta-analysis. Sleep Med. Rev. 2016, 30, 11–24. [Google Scholar] [CrossRef]
- Sinangil, A.; Celik, V.; Barlas, S.; Koc, Y.; Basturk, T.; Sakaci, T.; Akin, E.B.; Ecder, T. The incidence of new onset diabetes after transplantation and related factors: Single center experience. Nefrologia 2017, 37, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Vincenti, F.; Friman, S.; Scheuermann, E.; Rostaing, L.; Jenssen, T.; Campistol, J.M.; Uchida, K.; Pescovitz, M.D.; Marchetti, P.; Tuncer, M.; et al. Results of an international, randomized trial comparing glucose metabolism disorders and outcome with cyclosporine versus tacrolimus. Am. J. Transplant. 2007, 7, 1506–1514. [Google Scholar] [CrossRef]
- Yeh, H.; Lin, C.; Li, Y.R.; Yen, C.L.; Lee, C.C.; Chen, J.S.; Chen, K.H.; Tian, Y.C.; Liu, P.H.; Hsiao, C.C. Temporal trends of incident diabetes mellitus and subsequent outcomes in patients receiving kidney transplantation: A national cohort study in Taiwan. Diabetol. Metab. Syndr. 2020, 12, 34. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).