
The Implementation of a Blended Counseling Intervention in Undergraduate Engineering Students: The Effect on Mental Health




Abstract
1. Introduction
1.1. Student Mental Health Issues
1.2. Positive Psychology Interventions to Students
1.3. Cognitive Therapy Interventions to Students
1.4. Integration of Cognitive and Positive Psychology Interventions
1.5. The Purpose of the Present Study
2. Materials and Methods
2.1. Study Sample
2.2. Survey Tools
2.3. Ethics
2.4. Procedure
2.5. Design and Statistical Analysis
3. Results
3.1. Independent t-Tests Comparing the Intervention Group and the Control Group on Student Satisfaction Questionnaire Items
3.2. Two-Way Repeated-Measures ANOVAs
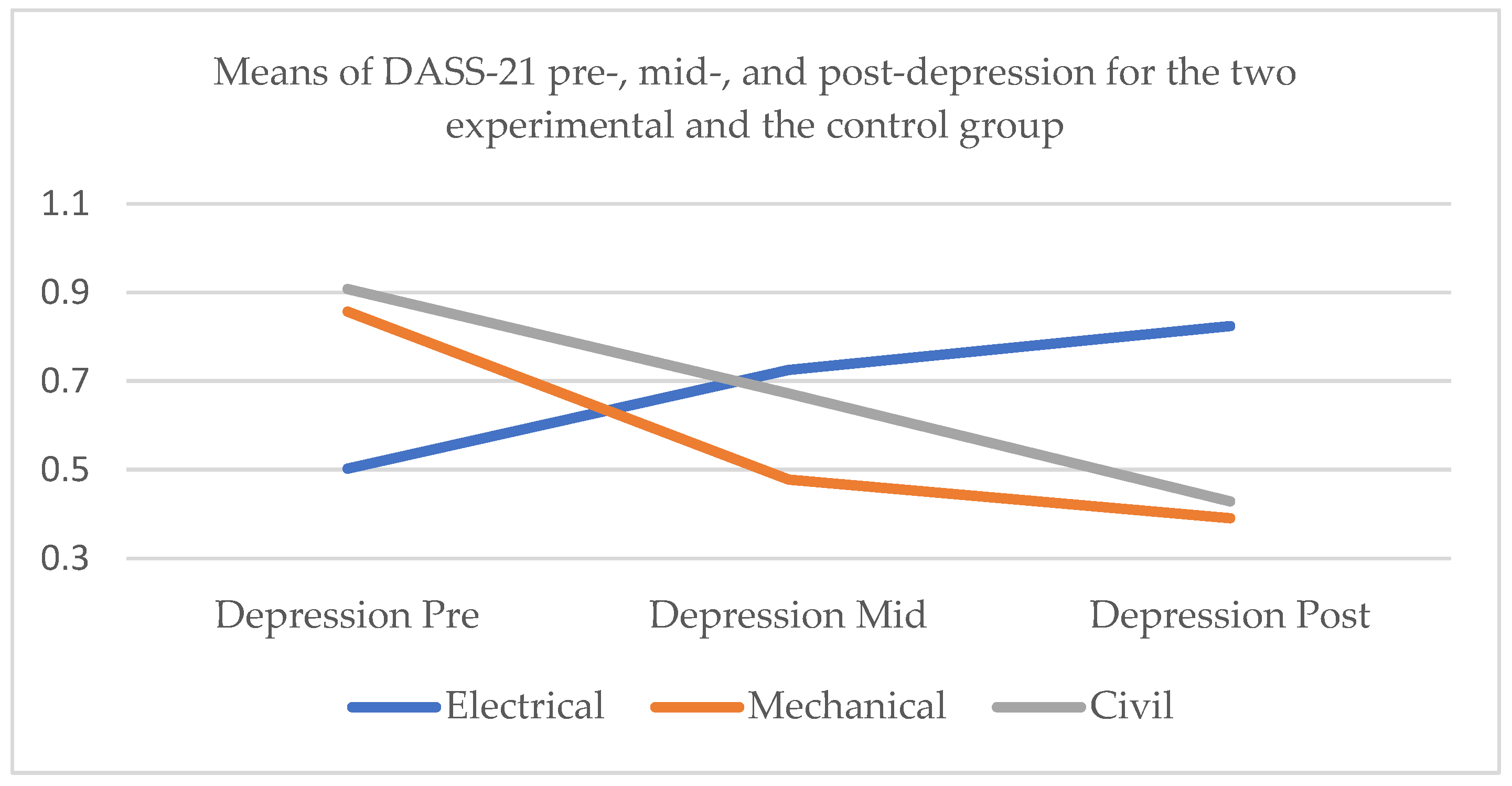
3.2.1. DASS-21 Depression
- Whole sample
- 2.
- Electrical engineers
- 3.
- Mechanical engineers
- 4.
- Civil engineers
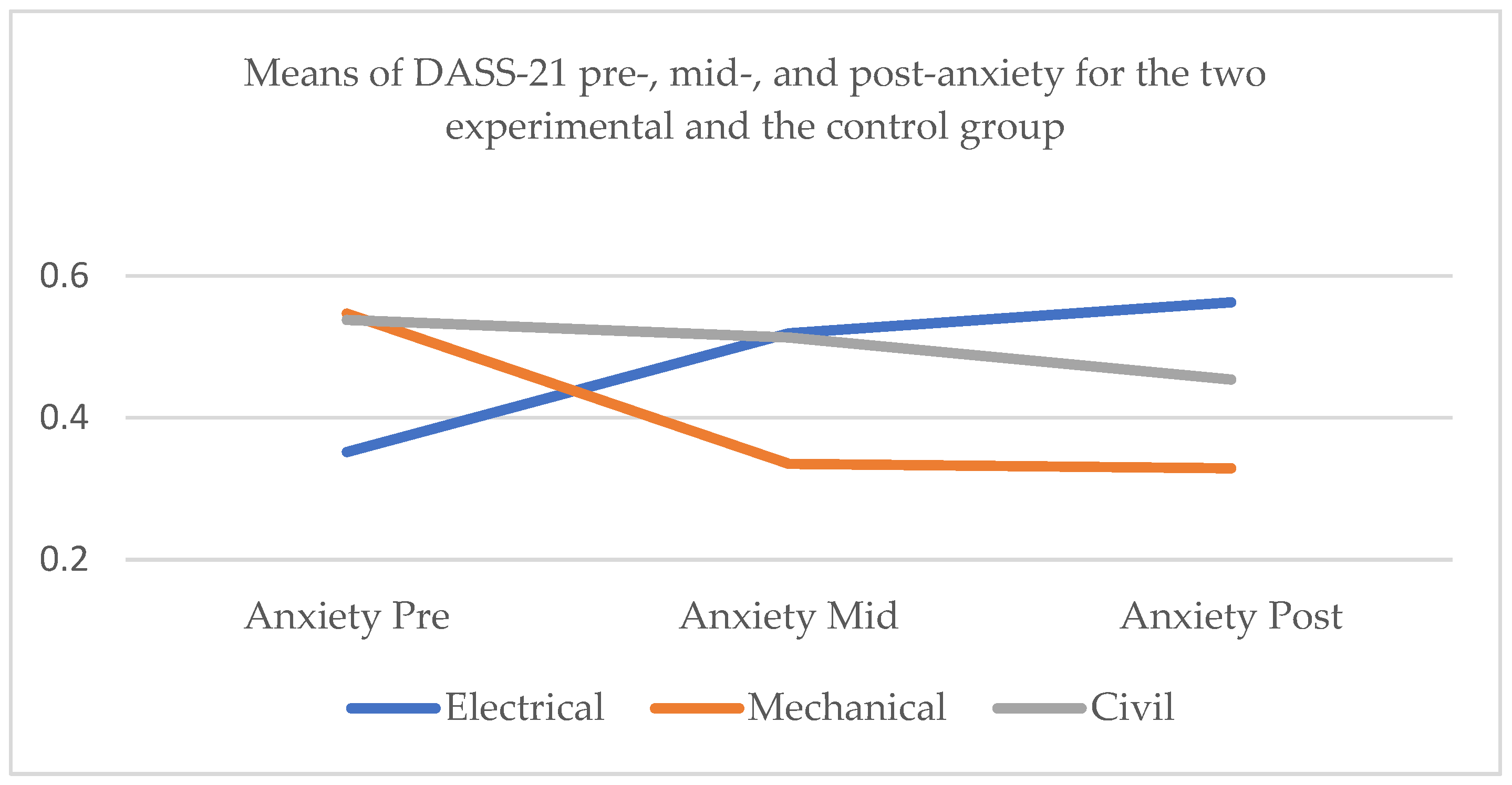
3.2.2. DASS-21 Anxiety
- Whole sample
- 2.
- Electrical engineers
- 3.
- Mechanical engineers
- 4.
- Civil engineers
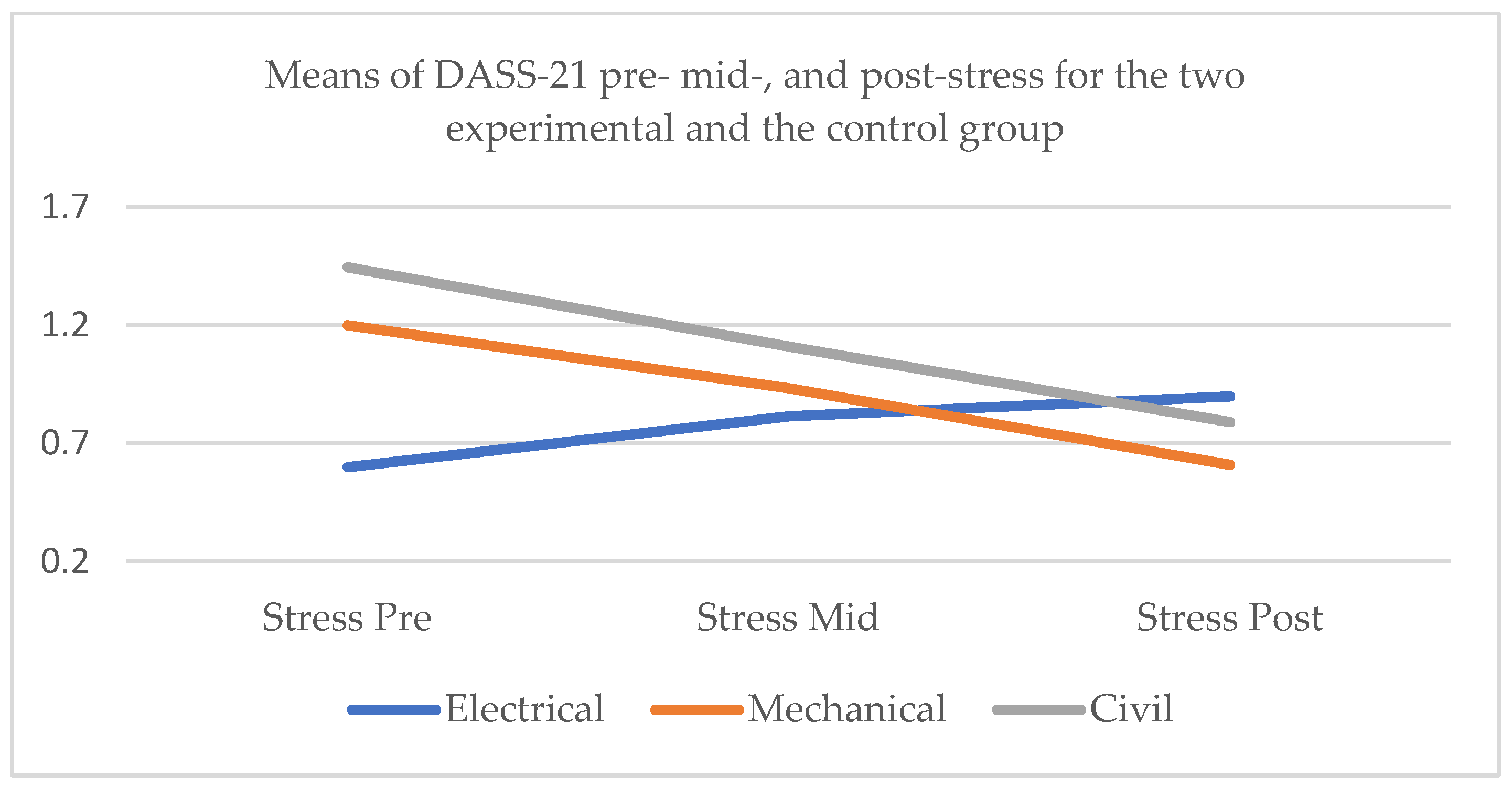
3.2.3. DASS-21 Stress
- Whole sample
- 2.
- Electrical engineers
- 3.
- Mechanical engineers
- 4.
- Civil engineers
3.3. Independent t-Tests Comparing the Two Experimental Subgroups on DASS-21 Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hicks, T.; Heastie, S. High School to college transition: A profile of the stressors, physical and psychological health issues that affect the first-year on-campus college student. J. Cult. Divers. 2008, 15, 143–147. [Google Scholar] [PubMed]
- Kessler, R.; Bergland, P.; Demler, O.; Jin, R.; Walters, E.E. Lifetime prevalence and age-of onset distributions of DSM-IV disorders in the National comorbidity survey replication. Arch. Gen. Psychiat. 2005, 62, 593–602. [Google Scholar] [CrossRef]
- MacKean, G. Mental health and well-being in postsecondary education settings: A literature and environmental scan to support planning and action in Canada. In Proceedings of the CACUSS Pre-Conference Workshop: Student Mental Health: A Call to Action, Toronto, ON, Canada, 6 June 2011. [Google Scholar]
- Verger, P.; Combes, J.B.; Kovess-Masfety, V.; Choquet, M.; Guagliardo, V.; Rouillon, F.; Peretti-Watel, P. Psychological distress in first year university students: Socioeconomic and academic stressors, mastery and social support in young men and women. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M.; Auerbach, R.P. Stress and its sequelae: Depression, Suicide, and Physical Illness. In American Psychological Association Handbook of Psychopathology; Butcher, J.N., Hooley, J., Kendall, P.C., Eds.; American Psychological Association: Washington, DC, USA, 2018; Volume 3, pp. 375–402. [Google Scholar]
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. WHO world mental health surveys international college student project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar] [CrossRef] [PubMed]
- Bayram, N.; Bilgel, N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Kavvadas, D.; Kavvada, A.; Karachrysafi, S.; Papaliagkas, V.; Chatzidimitriou, M.; Papamitsou, T. Stress, anxiety, and depression levels among university students: Three years from the beginning of the pandemic. Clin. Pract. 2023, 13, 596–609. [Google Scholar] [CrossRef] [PubMed]
- Aldiabat, K.M.; Matani, N.A.; Navenec, N.C.L. Mental health among undergraduate university students: A background paper for administrators, educators and healthcare providers. Univers. J. Public Health 2014, 2, 209–214. [Google Scholar] [CrossRef]
- Wang, X.; Hegde, S.; Son, C.; Keller, B.; Smith, A.; Sasangohar, F. Investigating mental health of US college students during the COVID-19 pandemic: Cross-sectional survey study. J. Med. Internet Res. 2020, 22, e22817. [Google Scholar] [CrossRef]
- Campbell, F.; Blank, L.; Cantrell, A.; Baxter, S.; Blackmore, C.; Dixon, J.; Goyder, E. Factors that influence mental health of university and college students in the UK: A systematic review. BMC Public Health 2022, 22, 1778. [Google Scholar] [CrossRef]
- Osborn, T.G.; Li, S.; Saunders, R.; Fonagy, P. University students’ use of mental health services: A systematic review and meta-analysis. Int. J. Ment. Health Syst. 2022, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- DeLucia-Waack, J.L.; Kalodner, C.R.; Riva, M.T. Handbook of Group Counseling and Psychotherapy, 2nd ed.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Samson, J.E.; Tanner-Smith, E.E. Single-session alcohol interventions for heavy drinking college students: A systematic review and meta-analysis. J. Stud. Alcohol Drugs 2015, 76, 530–543. [Google Scholar] [CrossRef] [PubMed]
- Ward, H.E.; Wheaton, M.G. Targeting perfectionism in college students. Grad. Stud. J. Psychol. 2022, 19, 98–113. [Google Scholar]
- Gable, S.L.; Haidt, J. What (and why) is positive psychology? Rev. Gen. Psychol. 2005, 9, 103–110. [Google Scholar] [CrossRef]
- Keyes, C.L.; Fredrickson, B.L.; Park, N. Positive psychology and the quality of life. In Handbook of Social Indicators and Quality of Life Research; Land, K.C., Michalos, A.C., Sirgy, M.J., Eds.; Springer: Dordrecht, The Netherlands; New York, NY, USA, 2012; pp. 99–112. [Google Scholar]
- Carr, A.; Cullen, K.; Keeney, C.; Canning, C.; Mooney, O.; Chinseallaigh, E.; O’Dowd, A. Effectiveness of positive psychology interventions: A systematic review and meta-analysis. J. Posit. Psychol. 2020, 16, 749–769. [Google Scholar] [CrossRef]
- Hammill, J.; Nguyen, T.; Henderson, F. Student engagement: The impact of positive psychology interventions on students. Act. Learn. High. Educ. 2022, 23, 129–142. [Google Scholar] [CrossRef]
- Hobbs, C.; Armitage, J.; Hood, B.; Jelbert, S. A systematic review of the effect of university positive psychology courses on student psychological wellbeing. Front. Psychol. 2022, 13, 1023140. [Google Scholar] [CrossRef]
- Biber, D.; Davis, A. A digital positive psychology intervention for college student mental health and health behaviors. Ment. Health Digit. Technol. 2024, 1, 228–239. [Google Scholar] [CrossRef]
- Kotsoni, A.; Mertika, A.; Stalikas, A. Be Your Best You: An evaluation of a positive psychology intervention programme in Greece. Psychology 2020, 11, 1021–1036. [Google Scholar] [CrossRef]
- Dimitropoulou, C.; Leontopoulou, S. A positive psychological intervention to promote well-being in a multicultural school setting in Greece. Eur. J. Couns. Psychol. 2017, 6, 113–137. [Google Scholar] [CrossRef]
- Karakasidou, E.; Raftopoulou, G.; Stalikas, A. A self-compassion intervention program for children in Greece. Psychology 2021, 12, 1990–2008. [Google Scholar] [CrossRef]
- Kotsoni, A.; Kanellakis, K.; Stalikas, A. Be Your Best You: A pilot study of a positive psychology programme for people with depression, anxiety or stress in Greece. Psychology 2020, 11, 13–29. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.; Sawyer, A.T.; Fang, A. The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognit. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Peterson, A.L.; Halstead, T.S. Group cognitive behavior therapy for depression in a community setting: A clinical replication series. Behav. Ther. 1998, 29, 3–18. [Google Scholar] [CrossRef]
- Dugas, M.J.; Ladouceur, R.; Léger, E.; Freeston, M.H.; Langolis, F.; Provencher, M.D.; Boisvert, J.-M. Group cognitive-behavioral therapy for generalized anxiety disorder: Treatment outcome and long-term follow-up. J. Consult. Clin. Psychol. 2003, 71, 821–825. [Google Scholar] [CrossRef]
- Wolgensinger, L. Cognitive behavioral group therapy for anxiety: Recent developments. Dialogues Clin. Neurosci. 2015, 17, 347–351. [Google Scholar] [CrossRef]
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disord. 2013, 148, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Irie, T.; Yokomitsu, K.; Sakano, Y. Relationship between cognitive behavioral variables and mental health status among university students: A meta-analysis. PLoS ONE 2019, 14, e0223310. [Google Scholar] [CrossRef]
- Buschmann, T.; Horn, R.A.; Blankenship, V.R.; Garcia, Y.E.; Bohan, K.B. The relationship between automatic thoughts and irrational beliefs predicting anxiety and depression. J. Ration.-Emot. Cogn.-Behav. Ther. 2018, 36, 137–162. [Google Scholar] [CrossRef]
- Ksiksou, J.; Maskour, L.; Alaoui, S. Effects of cognitive-behavioral group therapy on reducing levels of internet addiction, depression, anxiety, and stress among nursing students in Morocco. Iran J. Psychiatry Behav. Sci. 2023, 17, e136425. [Google Scholar] [CrossRef]
- Fava, G.A.; Cosci, F.; Guidi, J.; Tomba, E. Well-being therapy in depression: New insights into the role of psychological well-being in the clinical process. Depress. Anxiety 2017, 34, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Bannink, F.P. Positive CBT in practice. In Positive Psychology Interventions in Practice; Proctor, C., Ed.; Springer International Publishing: Guernsey, UK, 2017; pp. 15–28. [Google Scholar]
- Karwoski, L.; Garratt, G.M.; Ilardi, S.S. On the integration of cognitive-behavioral therapy for depression and positive psychology. J. Cogn. Psychother. 2006, 20, 159–170. [Google Scholar] [CrossRef]
- Chaves, C.; Lopez-Gomez, I.; Hervas, G.; Vazquez, C. A comparative study on the efficacy of a positive psychology intervention and a cognitive behavioral therapy for clinical depression. Cogn. Ther. Res. 2017, 41, 417–433. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Steen, T.A.; Park, N.; Peterson, C. Positive psychology progress: Empirical validation of interventions. Am. Psychol. 2005, 60, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Sin, N.L.; Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. J. Clin. Psychol. 2009, 65, 467–487. [Google Scholar] [CrossRef] [PubMed]
- van Aalderen, J.R.; Donders, A.R.; Giommi, F.; Spinhoven, P.; Barendregt, H.P.; Speckens, A.E. The efficacy of mindfulness-based cognitive therapy in recurrent depressed patients with and without a current depressive episode: A randomized controlled trial. Psychol. Med. 2012, 42, 989–1001. [Google Scholar] [CrossRef] [PubMed]
- Geschwind, N.; Bosgraaf, E.; Bannink, F.; Peeters, F. Positivity pays off: Clients’ perspectives on positive compared with traditional cognitive behavioral therapy for depression. Psychotherapy 2020, 57, 366–378. [Google Scholar] [CrossRef]
- Bannink, F.P.; Geschwind, N. Positive CBT: Individual and Group Treatment Protocols for Positive Cognitive Behavioral Therapy; Hogrefe Publishing: Boston, MA, USA, 2021. [Google Scholar]
- Utami, M.S.; Shalihah, M.; Adhiningtyas, N.P.; Rahmah, S.; Ningrum, W.K. Gratitude cognitive behavior therapy (G-CBT) to reduce college students’ academic stress. J. Psikol. 2020, 47, 137–150. [Google Scholar] [CrossRef]
- Geschwind, N.; Arntz, A.; Bannink, F.; Peeters, F. Positive cognitive behavior therapy in the treatment of depression: A randomized order within-subject comparison with traditional cognitive behavior therapy. Behav. Res. Ther. 2019, 116, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Padesky, C.; Mooney, K. Strengths-based cognitive-behavioural therapy: A four-step model to build resilience. Clin. Psychol. Psychother. 2012, 19, 283–290. [Google Scholar] [CrossRef]
- Johnson, J.; Wood, A.M. Integrating positive and clinical psychology: Viewing human functioning as continua from positive to negative can benefit clinical assessment, interventions and understandings of resilience. Cognit. Ther. Res. 2017, 41, 335–349. [Google Scholar] [CrossRef]
- Neimeyer, R.A.; Robinson, L.A.; Berman, J.S.; Haykal, R.F. Clinical outcome of group therapies for depression. Group Anal. 1989, 22, 73–86. [Google Scholar] [CrossRef]
- Marrero, R.-J.; Carballeira, M.; Martín, S.; Mejías, M.; Hernández, J.-A. Effectiveness of a positive psychology intervention combined with cognitive behavioral therapy in university students. An. Psicol. 2016, 32, 728–740. [Google Scholar] [CrossRef]
- Kocsis, Z.; Alter, E.; Pusztai, G. The role of student employment in persistence and efficiency in STEM higher education. Int. J. Educ. Math. Sci. Technol. 2022, 10, 831–848. [Google Scholar] [CrossRef]
- Stylianou, T.; Milidis, A. The socioeconomic determinants of university dropouts: The case of Greece. J. Infras. Policy Dev. 2024, 8, 3729. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck depression and anxiety inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Pezirkianidis, C.; Karakasidou, E.; Lakioti, A.; Stalikas, A.; Galanakis, M. Psychometric properties of the Depression, Anxiety, Stress Scales-21 (DASS-21) in a Greek sample. Psychology 2018, 9, 2933–2950. [Google Scholar] [CrossRef]
- Parks, A.C.; Seligman, M.E.P. 8-week group Positive Psychotherapy (PPT) manual. In Unpublished Manual; University of Pennysylvania: Philadelphia, PA, USA, 2007. [Google Scholar]
- Cunha, L.F.; Pellanda, L.C.; Reppold, C.T. Positive psychology and gratitude interventions: A randomized clinical trial. Front. Psychol. 2019, 10, 584. [Google Scholar] [CrossRef] [PubMed]
- Parks, A.C.; Biswas-Diener, R. Positive interventions: Past, present and future. In Mindfulness, Acceptance, and Positive Psychology: The Seven Foundations of Well-Being; Kashdan, T.B., Ciarrochi, J.V., Eds.; Context Press: Oakland, CA, USA, 2013; pp. 140–165. [Google Scholar]
- Linley, P.A.; Joseph, S. Positive Psychology in Practice; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004. [Google Scholar]
- Smith, B.W.; deCruz-Dixon, N.; Erickson, K.; Guzman, A.; Phan, A.; Schodt, K. The effects of an online positive psychology course on happiness, health, and well-being. J. Happiness Stud. 2023, 24, 1145–1167. [Google Scholar] [CrossRef] [PubMed]
- Neimeyer, R.A.; Feixas, G. The role of homework and skill acquisition in the outcome of group cognitive therapy for depression—Republished article. Behav. Ther. 2016, 47, 747–754. [Google Scholar] [CrossRef]
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef]
- Mishra, P.; Pandey, C.M.; Singh, U.; Gupta, A.; Sahu, C.; Keshri, A. Descriptive statistics and normality tests for statistical data. Ann. Card. Anaesth. 2019, 22, 67–72. [Google Scholar] [PubMed]
- Peterson, C.; Seligman, M.E.P. Character Strengths and Virtues: A Handbook and Classification; American Psychological Association, Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Barth, J.; Munder, T.; Gerger, H.; Nüesch, E.; Trelle, S.; Znoj, H.; Jüni, P.; Cuijpers, P. Comparative efficacy of seven psychotherapeutic interventions for patients with depression: A network meta-analysis. PLoS Med. 2013, 10, e1001454. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P. Are all psychotherapies equally effective in the treatment of adult depression? The lack of statistical power of comparative outcome studies. Evid. Based Ment. Health 2016, 19, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Gomez, I.; Chaves, C.; Hervas, G.; Vazquez, C. Pattern of changes during treatment: A comparison between a positive psychology intervention and a cognitive behavioral treatment for clinical depression. Span. J. Psychol. 2017, 20, e52. [Google Scholar] [CrossRef]
- Whitfield, G. Group cognitive-behavioural therapy for anxiety and depression. Adv. Psychiatr. Treat. 2010, 16, 219–227. [Google Scholar] [CrossRef]
- Wright, C.J.; Wilson, S.A.; Hammer, J.H.; Hargis, L.E.; Miller, M.E.; Usher, E.L. Mental health in undergraduate engineering students: Identifying facilitators and barriers to seeking help. J. Eng. Educ. 2023, 112, 963–986. [Google Scholar] [CrossRef]
- Beddoes, K.; Danowitz, A. In their own words: How aspects of engineering education undermine students’ mental health. In Proceedings of the ASEE Annual Conference and Exposition, Minneapolis, MN, USA, 23 August 2022. [Google Scholar]
- Johansson, F.; Rozental, A.; Edlund, K.; Côté, P.; Sundberg, T.; Onell, C.; Rudman, A.; Skillgate, E. Associations between procrastination and subsequent health outcomes among university students in Sweden. JAMA Netw. Open 2023, 6, e2249346. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Johri, A.; Rangwala, H. Running out of stem: A comparative study across stem majors of college students at-risk of dropping out early. In Proceedings of the 8th International Conference on Learning Analytics and Knowledge, Sydney, Australia, 7 March 2018. [Google Scholar]
- Trusty, W.T.; Scofield, B.E.; Christensen, A.E.; White, T.D.; Murphy, Y.E.; Janis, R.A.; Tan, H.; Hernandez, N.M.; Hochstedt, K.S. Psychological symptoms and academic dropout in higher education: A six-year cohort study. J. Coll. Stud. Ment. Health 2025, 1–21. [Google Scholar] [CrossRef]
- Cully, J.A.; Teten, A.L. A Therapist’s Guide to Brief Cognitive Behavioral Therapy; Department of Veterans Affairs South Central MIRECC: Houston, DX, USA, 2008.
- Ma, L.; Huang, C.; Cui, Z. A meta-analysis of cognitive-behavioral therapy for depressive symptoms among college students, alone and in comparison with other interventions. J. Behav. Cogn. Ther. 2020, 30, 127–139. [Google Scholar] [CrossRef]
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health 2013, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- Juul, S.; Jakobsen, J.C.; Jørgensen, C.K.; Poulsen, S.; Sørensen, P.; Simonsen, S. The difference between shorter-versus longer-term psychotherapy for adult mental health disorders: A systematic review with meta-analysis. BMC Psychiatry 2023, 23, 438. [Google Scholar] [CrossRef] [PubMed]
- Kulandaiammal, R.; Neelakantan, M. Character strengths interventions in higher education students: A literature review. Hell. J. Psychol. 2024, 21, 67–97. [Google Scholar]
- Borja-Gil, J.; Verdugo, M.C.; Oviedo-García, M.Á. Engagement and commitment in higher education: Looking at the role of identification and perception of performance. Eur. J. Educ. 2024, 59, e12642. [Google Scholar] [CrossRef]
- Marra, R.M.; Rodgers, K.A.; Shen, D.; Bogue, B. Leaving Engineering: A multi-year single institution study. J. Eng. Educ. 2012, 101, 6–27. [Google Scholar] [CrossRef]
- Flinchbaugh, C.L.; Moore, E.G.; Chang, Y.K.; May, D.R. Student well-being interventions: The effects of stress management techniques and gratitude journaling in the management education classroom. J. Manag. Educ. 2012, 36, 191–219. [Google Scholar] [CrossRef]
- Kerr, S.L.; O’Donovan, A.; Pepping, C.A. Can gratitude and kindness interventions enhance well-being in a clinical sample? J. Happiness Stud. 2014, 16, 17–36. [Google Scholar] [CrossRef]
- Sheldon, K.M.; Lyubomirsky, S. How to increase and sustain positive emotion: The effects of expressing gratitude and visualizing best possible selves. J. Posit. Psychol. 2006, 1, 73–82. [Google Scholar] [CrossRef]
- Emmons, R.A.; McCullough, M.E. Counting blessings versus burdens: An experimental investigation of gratitude and subjective well-being in daily life. J. Pers. Soc. Psychol. 2003, 84, 377–389. [Google Scholar] [CrossRef]
- Niemiec, R.M. Mindfulness and Character Strengths: A Practical Guide to Flourishing; Hogrefe: Boston, MA, USA, 2014. [Google Scholar]
- Seligman, M.E.P. Learned Optimism: How to Change Your Mind and Your Life; Nicholas Brealey Publishing: London, UK, 2006. [Google Scholar]
- Bannink, F.P. Practicing Positive CBT: From Reducing Distress to Building Success; Wiley-Blackwell: Chichester, UK, 2012. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Session Civil Engineers | Topic | Content | Tasks/Exercises | Homework |
|---|---|---|---|---|
| 1 | Initial measurement—introduction in positive psychology | Administration of questionnaires, information about the goal of the intervention—aim of the Three Good Things | Three Good Things | Three good things every day in a weekly span |
| 2 | Character strengths, gratitude | Presentation of virtues and character strengths, theory about gratitude | Everyday use of character strengths and new ways of application, future goals and character strengths that can help achieve them | List of accomplishments and achievements, journal of gratitude |
| 3 | Gratitude—middle measurement—introduction in cognitive psychotherapy | Theory about gratitude and its benefits—administration of questionnaires—theory about the errors in thinking | Letter of gratitude, personal motto—examples of cognitive distortions | Matching types of cognitive distortions with their examples |
| 4 | Recognizing negative automatic thoughts | Theory about negative thoughts and ways of discovering them | Identifying cognitive distortions and associating them with provoking situations | Journal of negative automatic thoughts |
| 5 | Dismantling negative automatic thoughts—ending and final measurement | Theory about challenging negative thoughts and finding alternatives—administration of questionnaires | Challenging negative automatic thinking and reframing it into alternative rational one, personal motto | |
| Session Mechanical Engineers | ||||
| 1 | Initial measurement—introduction in cognitive psychotherapy | Administration of questionnaires—information about the goal of the intervention—theory about the errors in thinking | Examples of cognitive distortions | Matching types of cognitive distortions with their examples |
| 2 | Recognizing negative automatic thoughts | Theory about negative thoughts and ways of discovering them | Identifying cognitive distortions and associating them with provoking situations | Journal of negative automatic thoughts |
| 3 | Dismantling negative automatic thoughts—middle measurement—introduction in positive psychology | Theory about challenging negative thoughts and finding alternatives—administration of questionnaires—aim of the Three Good Things | Challenging negative automatic thinking and reframing it into alternative rational one, personal motto—Three Good Things | Three good things every day in a weekly span |
| 4 | Character strengths, gratitude | Presentation of virtues and character strengths, theory about gratitude | Everyday use of character strengths and new ways of application, future goals and character strengths that can help achieve them | List of accomplishments and achievements, journal of gratitude |
| 5 | Gratitude—ending and final measurement | Theory about gratitude and its benefits—administration of questionnaires | Letter of gratitude, personal motto |
| Student Satisfaction with University Services Items | Experimental | Control | df | t | p | ||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Class organization | 2.85 | 1.099 | 2.54 | 0.874 | 90 | 1.515 | 0.133 |
| Secretary assistance | 2.25 | 1.056 | 2.08 | 0.987 | 90 | 0.809 | 0.421 |
| E-platform | 2.13 | 1.305 | 2.21 | 0.871 | 90 | −0.381 | 0.704 |
| Technical services | 1.95 | 1.131 | 2.04 | 0.969 | 90 | −0.403 | 0.688 |
| Teaching quality | 3.55 | 1.061 | 2.94 | 1.037 | 90 | 2.759 | <0.01 |
| Teachers’ knowledge | 3.83 | 0.931 | 3.35 | 1.046 | 90 | 2.283 | <0.05 |
| University notes | 3.30 | 1.067 | 2.79 | 1.073 | 90 | 2.273 | <0.05 |
| Testing mode | 3.58 | 0.874 | 2.52 | 1.000 | 90 | 5.300 | <0.001 |
| Grading mode | 3.43 | 1.059 | 2.54 | 1.056 | 90 | 3.985 | <0.001 |
| DASS-21 Factors | Departments | M | SD |
|---|---|---|---|
| Depression Pre | Electrical | 0.503 | 0.629 |
| Mechanical | 0.857 | 0.383 | |
| Civil | 0.908 | 0.766 | |
| Depression Mid | Electrical | 0.725 | 0.611 |
| Mechanical | 0.478 | 0.396 | |
| Civil | 0.672 | 0.717 | |
| Depression Post | Electrical | 0.824 | 0.612 |
| Mechanical | 0.391 | 0.398 | |
| Civil | 0.429 | 0.505 | |
| Anxiety Pre | Electrical | 0.352 | 0.503 |
| Mechanical | 0.547 | 0.394 | |
| Civil | 0.538 | 0.514 | |
| Anxiety Mid | Electrical | 0.519 | 0.540 |
| Mechanical | 0.335 | 0.403 | |
| Civil | 0.513 | 0.503 | |
| Anxiety Post | Electrical | 0.563 | 0.587 |
| Mechanical | 0.329 | 0.427 | |
| Civil | 0.454 | 0.423 | |
| Stress Pre | Electrical | 0.599 | 0.557 |
| Mechanical | 1.199 | 0.604 | |
| Civil | 1.445 | 0.654 | |
| Stress Mid | Electrical | 0.813 | 0.623 |
| Mechanical | 0.932 | 0.489 | |
| Civil | 1.109 | 0.588 | |
| Stress Post | Electrical | 0.898 | 0.658 |
| Mechanical | 0.609 | 0.476 | |
| Civil | 0.790 | 0.438 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalamatianos, A.; Kounenou, K.; Pezirkianidis, C. The Implementation of a Blended Counseling Intervention in Undergraduate Engineering Students: The Effect on Mental Health. Healthcare 2025, 13, 511. https://doi.org/10.3390/healthcare13050511
Kalamatianos A, Kounenou K, Pezirkianidis C. The Implementation of a Blended Counseling Intervention in Undergraduate Engineering Students: The Effect on Mental Health. Healthcare. 2025; 13(5):511. https://doi.org/10.3390/healthcare13050511
Chicago/Turabian StyleKalamatianos, Antonios, Kalliope Kounenou, and Christos Pezirkianidis. 2025. "The Implementation of a Blended Counseling Intervention in Undergraduate Engineering Students: The Effect on Mental Health" Healthcare 13, no. 5: 511. https://doi.org/10.3390/healthcare13050511
APA StyleKalamatianos, A., Kounenou, K., & Pezirkianidis, C. (2025). The Implementation of a Blended Counseling Intervention in Undergraduate Engineering Students: The Effect on Mental Health. Healthcare, 13(5), 511. https://doi.org/10.3390/healthcare13050511