
Adaptation and Validation of the Italian Version of the Diabetes Self-Management Questionnaire (I-DSMQ) with an Additional Focus on Patients with Type 2 Diabetes

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. DSMQ Questionnaire
2.2. Procedure
- Translation process: this involved four stages—translation, synthesis, back-translation, and the acquisition of a consensus version following review by committee specialists.
- Assessment: this focused on evaluating the clarity, difficulty, and relevance of each item, as well as their psychometric properties.
2.3. Data Collection
- Age ≥ 18 years.
- Ability to understand the questions.
- Proficiency in the Italian language.
- The exclusion criteria were:
- Age < 18 years.
- Cognitive impairment, dementia, or other conditions that hinder self-management.
2.4. Statistical Analysis
- Root mean square error of approximation (RMSEA) [21]: measures the estimated discrepancy between the population and model-implied population covariance matrices per degree of freedom. The closer the RMSEA is to 0, the better the fit. The threshold of 0.08 [22] is usually considered for discriminating between a good and poor fit [21].
3. Results
3.1. T1DM and T2DM
3.1.1. Reliability of the Instrument
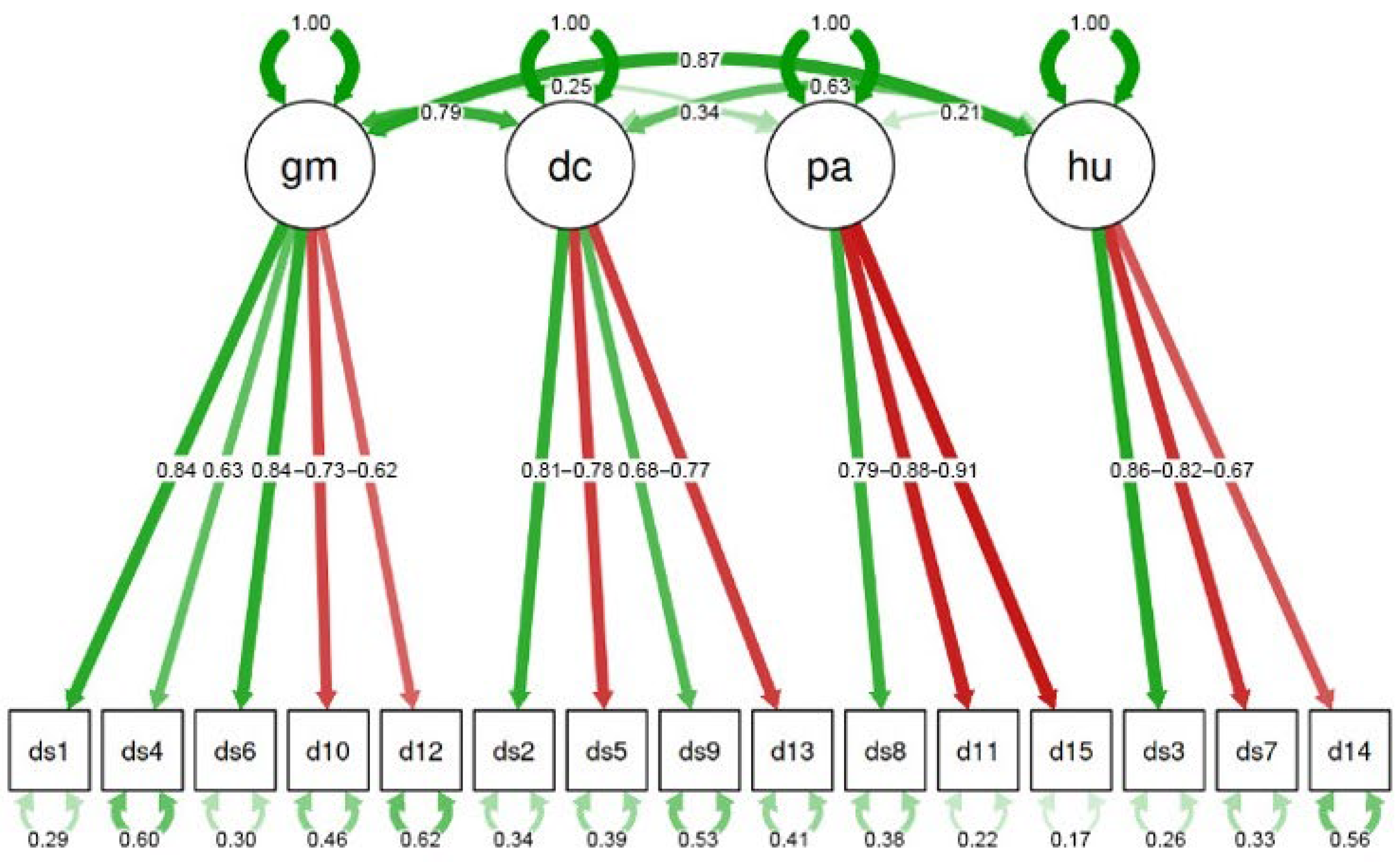
3.1.2. Confirmatory Factor Analysis
- CFI = 0.911;
- SRMR = 0.073;
- RMSEA = 0.096.
3.1.3. Test–Retest Analysis
3.2. T2DM
3.2.1. Reliability of the Instrument
3.2.2. Confirmatory Factor Analysis
- CFI = 0.816;
- SRMR = 0.095;
- RMSEA = 0.120.
3.2.3. Test–Retest Analysis
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Report of the WHO Discussion Group for People Living with Diabetes; World Health Organization: Geneva, Switzerland, 2023.
- World Health Organization. Diabetes. 2022. Available online: https://www.who.int/health-topics/diabetes#tab=tab_1 (accessed on 25 February 2022).
- Italian National Institute of Health-EpiCentro: Epicentro. Diabetes-PASSI Surveillance. Available online: https://www.epicentro.iss.it/passi/dati/diabete?tab-container-1=tab1 (accessed on 12 January 2025).
- Ballotari, P.; Caroli, S.; Ferrari, F.; Romani, G.; Marina, G.; Chiarenza, A.; Manicardi, V.; Rossi, P.G. Differences in diabetes prevalence and inequalities in disease management and glycaemic control by immigrant status: A population-based study (Italy). BMC Public Health 2015, 15, 87. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, A.; Gahr, A.; Hermanns, N.; Kulzer, B.; Huber, J.; Haak, T. The Diabetes Self-Management Questionnaire (DSMQ): Development and evaluation of an instrument to assess diabetes self-care activities associated with glycaemic control. Health Qual. Life Outcomes 2013, 11, 138. [Google Scholar] [CrossRef] [PubMed]
- Wee, P.J.L.; Kwan, Y.H.; Loh, D.H.F.; Phang, J.K.; Puar, T.H.; Østbye, T.; Thumboo, J.; Yoon, S.; Low, L.L. Measurement Properties of Patient-Reported Outcome Measures for Diabetes: Systematic Review. J. Med. Internet Res. 2021, 23, e25002. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, A.; Kulzer, B.; Ehrmann, D.; Haak, T.; Hermanns, N. A Self-Report Measure of Diabetes Self-Management for Type 1 and Type 2 Diabetes: The Diabetes Self-Management Questionnaire-Revised (DSMQ-R)-Clinimetric Evidence from Five Studies. Front Clin. Diabetes Healthc. 2021, 2, 823046. [Google Scholar] [CrossRef] [PubMed]
- Kaddech, N.; Guelmami, N.; Bonsaksen, T.; Doggui, R.; Beji, C.; El Ati, J. Adaptation and Psychometric Evidence of the ARABIC Version of the Diabetes Self-Management Questionnaire (A-DSMQ). Healthcare 2022, 10, 951. [Google Scholar] [CrossRef] [PubMed]
- Diaconu, L.; Gaita, L.; Timar, B.; Deaconu, L.; Lazar, S.; Timar, R.; Popescu, S. Validation and Cross-Cultural Adaptation of the Diabetes Self-Management Questionnaire (DSMQ) and the Social Phobia Inventory (SPIN) in Romanian Patients with Diabetes Mellitus. Medicina 2022, 58, 1823. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Statistics (Istat). Indicatori Demografici: Anno 2023 (Demographic indicators). Available online: https://esploradati.istat.it/databrowser/ (accessed on 12 January 2025).
- Cascini, F.; Gentili, A. National Recovery and Resilience Plan and Health: Qualitative analysis on the sustainability of the interventions on healthcare. Ann. Di Ig. Med. Prev. E Di Comunità 2023, 35, 602–610. [Google Scholar] [CrossRef]
- Capolongo, S.; Buffoli, M.; Gola, M.; Borghini, A.; Riano, F.; Arruzzoli, S.; Brusamolin, E.; Yu, Y.; Izzi, A.; Mantoan, D. The meta-projects of the new community health centers, community hospitals and local operative centers for the Italian country. Acta Bio-Medica de L’ateneo Parm. 2023, 94, e2023154. [Google Scholar] [CrossRef]
- Italian Government. Piano Nazionale di Ripresa e Resilienza (National Recovery and Resilience Plan). Available online: https://www.mimit.gov.it/it/pnrr/documenti (accessed on 12 January 2025).
- Ministry of Health. Decreto Ministeriale n. 77 del 2022. Available online: https://www.gazzettaufficiale.it/eli/id/2022/06/22/22G00085/SG (accessed on 12 January 2025).
- Floridia, G.; Grattagliano, I.; Greco, D.; Muzzetto, P.; Nicoli, F.; Petrini, C.; Gruppo di Lavoro Bioetica COVID-19. Il Medico di Medicina Generale e La Pandemia di COVID-19: ALCUNI Aspetti Di Etica e Di Organizzazione; Istituto Superiore di Sanità: Rome, Italy, 2020.
- Kercuku, A. Forgotten Italy: Spaces and identities of a changing geography. Trans. Assoc. Eur. Sch. Plan. 2022, 6, 41–54. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J. Multivariate Data Analysis: A Global Perspective; Pearson Education: London, UK, 2010. [Google Scholar]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative Fit Indexes in Structural Models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Byrne, B.M.; Byrne, B.M. Basic Concepts, Applications, and Programming. In Structural Equation Modeling With EQS, 2nd ed.; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Steiger, J.H. Notes on the Steiger–Lind (1980) Handout. Struct. Equ. Model. A Multidiscip. J. 2016, 23, 777–781. [Google Scholar] [CrossRef]
- Afthanorhan, W.M.A.W. A Handbook on SEM Overview of Structural Equation Modeling (SEM). Am. J. Humanit. Soc. Sci. Res. 2021, 5, 11–19. Available online: http://www.ajhssr.com (accessed on 12 January 2025).
- Kaiser, H.F. A second generation little jiffy. Psychometrika 1970, 35, 401–415. [Google Scholar] [CrossRef]
- Marzban, S.; Najafi, M.; Agolli, A.; Ashrafi, E. Impact of Patient Engagement on Healthcare Quality: A Scoping Review. J. Patient Exp. 2022, 9, 2022. [Google Scholar] [CrossRef] [PubMed]
- Rapporto Osservasalute. 2022 Osservatorio sulla Salute (Health Observatory Report). Available online: https://osservatoriosullasalute.it/osservasalute/rapporto-osservasalute-2022 (accessed on 12 January 2025).
- Italian Ministry of Health. Rapporto Annuale Sull’attività di Ricovero Ospedaliero (Dati SDO 2021) Annual Report on Hospitalization Activity SDO Data; Italian Ministry of Health: Rome, Italy, 2021.

{kind=link}
| Type 2 | Type 1 and 2 | Variable | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Re-Test | Test | Re-Test | Test | ||||||
| % | N | % | N | % | N | % | N | ||
| 99 | 99 | 62 | 70 | Sample size | |||||
| 49.5 | 49 | 49.5 | 49 | 43.5 | 27 | 44.3 | 31 | Male | Gender |
| 50.5 | 50 | 50.5 | 50 | 56.5 | 35 | 55.7 | 39 | Female | |
| 66.9 (7.9) | 66.9 (7.9) | 55.8 (16.6) | 55 (16.4) | Mean (S.D.) | Age | ||||
| Cronbach’s α [95% Confidence Intervals] | Cronbach’s α if the Item Is Dropped | Correlation | Items | Factors |
|---|---|---|---|---|
| 0.84 [0.78, 0.90] | 0.78 | 0.84 | DSMQ 1 | GM |
| 0.83 | 0.73 | DSMQ 4 | ||
| 0.79 | 0.82 | DSMQ 6 | ||
| 0.8 | 0.8 | DSMQ 10 (−) | ||
| 0.83 | 0.73 | DSMQ 12 (−) | ||
| 0.86 [0.81, 0.91] | 0.81 | 0.86 | DSMQ 2 | DC |
| 0.79 | 0.87 | DSMQ 5 (−) | ||
| 0.85 | 0.79 | DSMQ 9 | ||
| 0.82 | 0.83 | DSMQ 13 (−) | ||
| 0.90 [0.85, 0.94] | 0.89 | 0.89 | DSMQ 8 | PA |
| 0.83 | 0.92 | DSMQ 11 (−) | ||
| 0.83 | 0.92 | DSMQ 15 (−) | ||
| 0.82 [0.75, 0.90] | 0.77 | 0.85 | DSMQ 3 | HU |
| 0.66 | 0.9 | DSMQ 7 (−) | ||
| 0.83 | 0.82 | DSMQ 14 (−) |
| Loading | Factor | Kurtosis | Skewness | St.Dev. | Mean | Variable |
|---|---|---|---|---|---|---|
| 0.84 | GM | −1.07 | −0.32 | 0.91 | 1.99 | DSMQ 1 |
| 0.63 | −0.35 | −0.86 | 0.63 | 2.5 | DSMQ 4 | |
| 0.84 | −1.14 | −0.14 | 0.98 | 1.76 | DSMQ 6 | |
| −0.73 | −1.27 | −0.17 | 1.06 | 1.49 | DSMQ 10 (−) | |
| −0.62 | 0.8 | 0.44 | 0.93 | 1.06 | DSMQ 12 (−) | |
| 0.81 | DC | −1 | 0.05 | 0.94 | 1.63 | DSMQ 2 |
| −0.78 | −0.75 | 0 | 0.85 | 1.34 | DSMQ 5 (−) | |
| 0.68 | −0.43 | 0.01 | 0.75 | 1.59 | DSMQ 9 | |
| −0.77 | −0.58 | 0.56 | 0.86 | 0.91 | DSMQ 13 (−) | |
| 0.79 | PA | −0.7 | 0.28 | 0.9 | 1.33 | DSMQ 8 |
| −0.88 | −1.36 | 0.03 | 1.07 | 1.33 | DSMQ 11 (−) | |
| −0.91 | −1.21 | 0 | 1 | 1.33 | DSMQ 15 (−) | |
| 0.86 | HU | −1 | −0.46 | 0.95 | 2.03 | DSMQ 3 |
| −0.82 | −0.56 | 0.74 | 0.93 | 0.84 | DSMQ 7 (−) | |
| −0.67 | −1.04 | −0.01 | 0.95 | 1.34 | DSMQ 14 (−) |
| Cronbach’s α [95% Confidence Intervals] | Cronbach’s α if the Item Is Dropped | Correlation | Items | Factors |
|---|---|---|---|---|
| 0.79 [0.73, 0.86] | 0.8 | 0.65 | DSMQ 1 | GM |
| 0.75 | 0.76 | DSMQ 4 | ||
| 0.74 | 0.78 | DSMQ 6 | ||
| 0.75 | 0.78 | DSMQ 10 (−) | ||
| 0.76 | 0.75 | DSMQ 12 (−) | ||
| 0.84 [0.79, 0.89] | 0.82 | 0.8 | DSMQ 2 | DC |
| 0.78 | 0.86 | DSMQ 5 (−) | ||
| 0.81 | 0.82 | DSMQ 9 | ||
| 0.81 | 0.82 | DSMQ 13 (−) | ||
| 0.76 [0.68, 0.84] | 0.74 | 0.82 | DSMQ 8 | PA |
| 0.68 | 0.84 | DSMQ 11 (−) | ||
| 0.69 | 0.84 | DSMQ 15 (−) | ||
| 0.66 [0.55, 0.77] | 0.5 | 0.8 | DSMQ 3 | HU |
| 0.61 | 0.75 | DSMQ 7 (−) | ||
| 0.59 | 0.76 | DSMQ 14 (−) |
| Loading | Factor | Kurtosis | Skewness | St.Dev. | Mean | Variable |
|---|---|---|---|---|---|---|
| 0.64 | GM | −1.45 | −0.13 | 0.8 | 2.07 | DSMQ 1 |
| 0.61 | 0.28 | −0.86 | 0.78 | 2.26 | DSMQ 4 | |
| 0.67 | −1.04 | −0.03 | 0.77 | 1.94 | DSMQ 6 | |
| −0.73 | 0.19 | 0.71 | 0.68 | 0.67 | DSMQ 10 (−) | |
| −0.68 | −0.13 | 0.95 | 0.59 | 0.44 | DSMQ 12 (−) | |
| 0.71 | DC | −0.93 | −0.13 | 0.93 | 1.7 | DSMQ 2 |
| −0.83 | −0.3 | 0.63 | 0.83 | 0.89 | DSMQ 5 (−) | |
| 0.73 | −0.61 | −0.27 | 0.81 | 1.9 | DSMQ 9 | |
| −0.8 | 4.3 | 1.92 | 0.67 | 0.41 | DSMQ 13 (−) | |
| 0.73 | PA | −0.56 | −0.26 | 0.84 | 1.77 | DSMQ 8 |
| −0.74 | −0.64 | 0.18 | 0.59 | 0.71 | DSMQ 11 (−) | |
| −0.78 | −0.51 | 0.07 | 0.58 | 0.75 | DSMQ 15 (−) | |
| 0.73 | HU | −1.1 | −0.34 | 0.73 | 2.21 | DSMQ 3 |
| −0.56 | −0.24 | 0.89 | 0.57 | 0.43 | DSMQ 7 (−) | |
| −0.64 | −0.12 | −0.06 | 0.55 | 0.83 | DSMQ 14 (−) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardo, C.; Vittorini, P.; Fabiani, L.; Aleandri, A.R.; Ciogli, F.; Fiorenza, M.; Scatigna, M.; De Luca, A. Adaptation and Validation of the Italian Version of the Diabetes Self-Management Questionnaire (I-DSMQ) with an Additional Focus on Patients with Type 2 Diabetes. Healthcare 2025, 13, 475. https://doi.org/10.3390/healthcare13050475
Lombardo C, Vittorini P, Fabiani L, Aleandri AR, Ciogli F, Fiorenza M, Scatigna M, De Luca A. Adaptation and Validation of the Italian Version of the Diabetes Self-Management Questionnaire (I-DSMQ) with an Additional Focus on Patients with Type 2 Diabetes. Healthcare. 2025; 13(5):475. https://doi.org/10.3390/healthcare13050475
Chicago/Turabian StyleLombardo, Camilla, Pierpaolo Vittorini, Leila Fabiani, Anna Rita Aleandri, Francesco Ciogli, Marta Fiorenza, Maria Scatigna, and Assunta De Luca. 2025. "Adaptation and Validation of the Italian Version of the Diabetes Self-Management Questionnaire (I-DSMQ) with an Additional Focus on Patients with Type 2 Diabetes" Healthcare 13, no. 5: 475. https://doi.org/10.3390/healthcare13050475
APA StyleLombardo, C., Vittorini, P., Fabiani, L., Aleandri, A. R., Ciogli, F., Fiorenza, M., Scatigna, M., & De Luca, A. (2025). Adaptation and Validation of the Italian Version of the Diabetes Self-Management Questionnaire (I-DSMQ) with an Additional Focus on Patients with Type 2 Diabetes. Healthcare, 13(5), 475. https://doi.org/10.3390/healthcare13050475