
Mindfulness-Oriented Professional Resilience (MOPR) Training to Reduce Compassion Fatigue in Healthcare Workers: A Pilot Study



Abstract
1. Introduction
2. Materials and Methods
2.1. The Program
2.2. Study Design
2.3. Setting and Participants
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Demographics and Work-Related Backgrounds
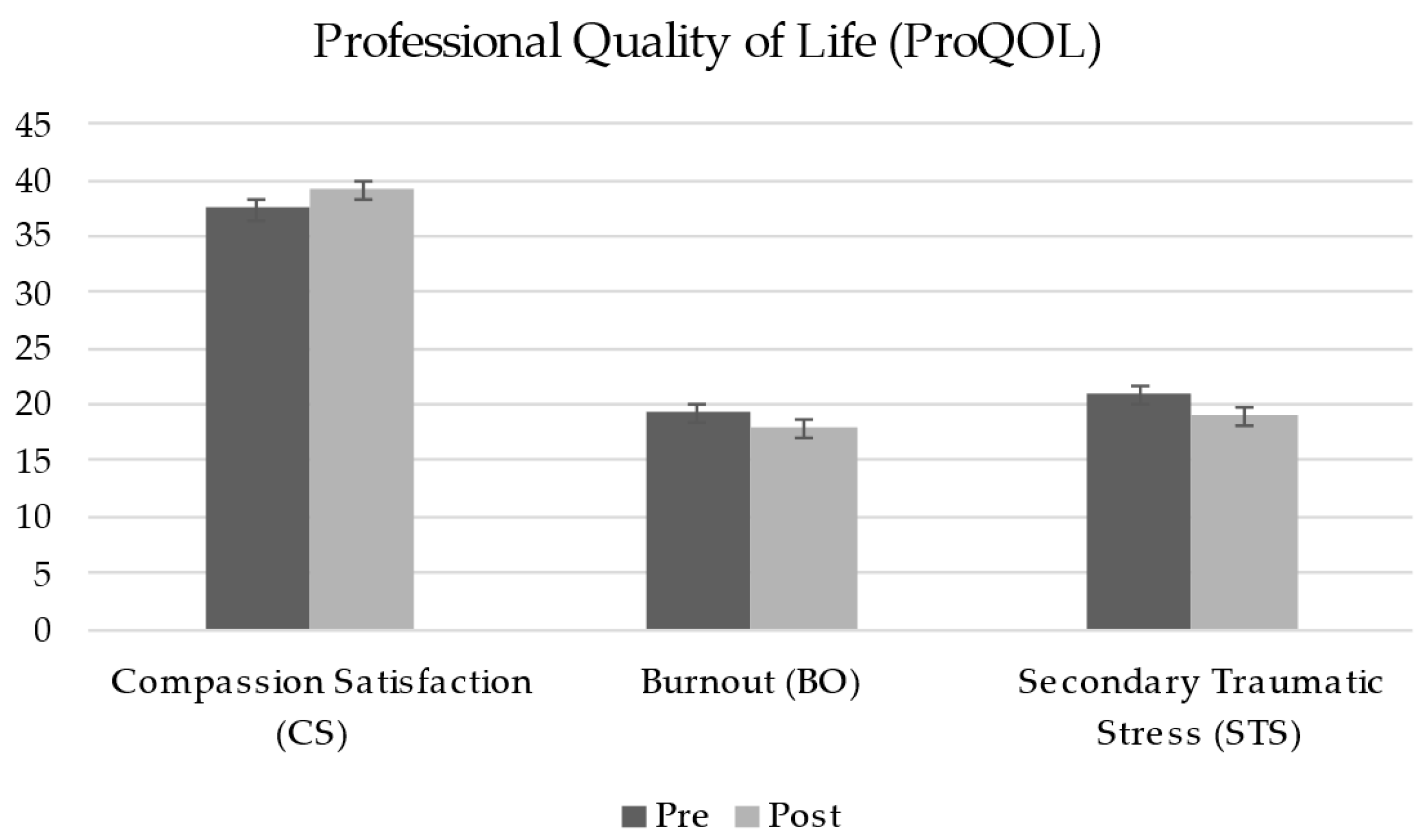
3.2. Professional Quality of Life
3.3. Mindfulness
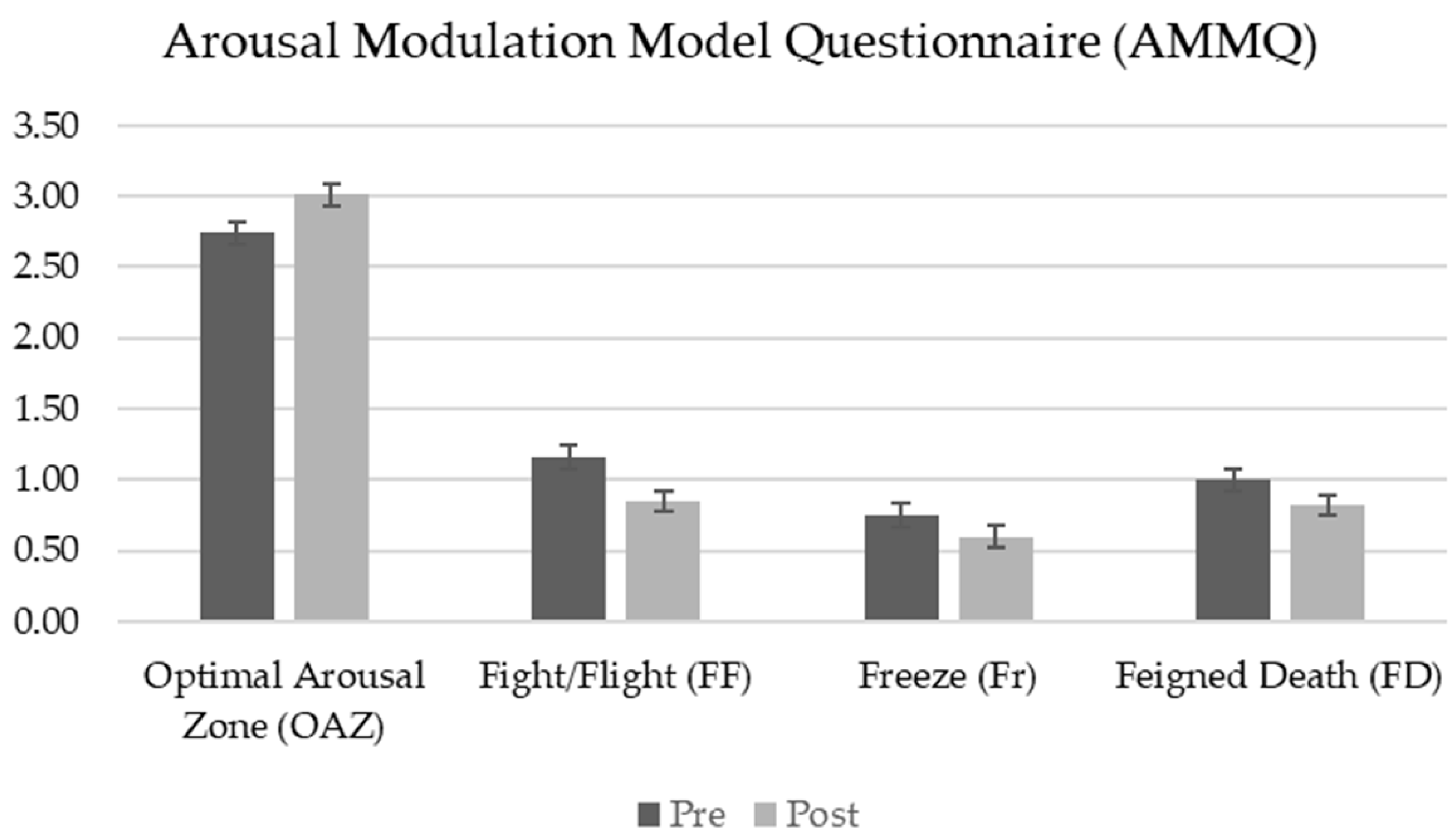
3.4. Arousal Modulation
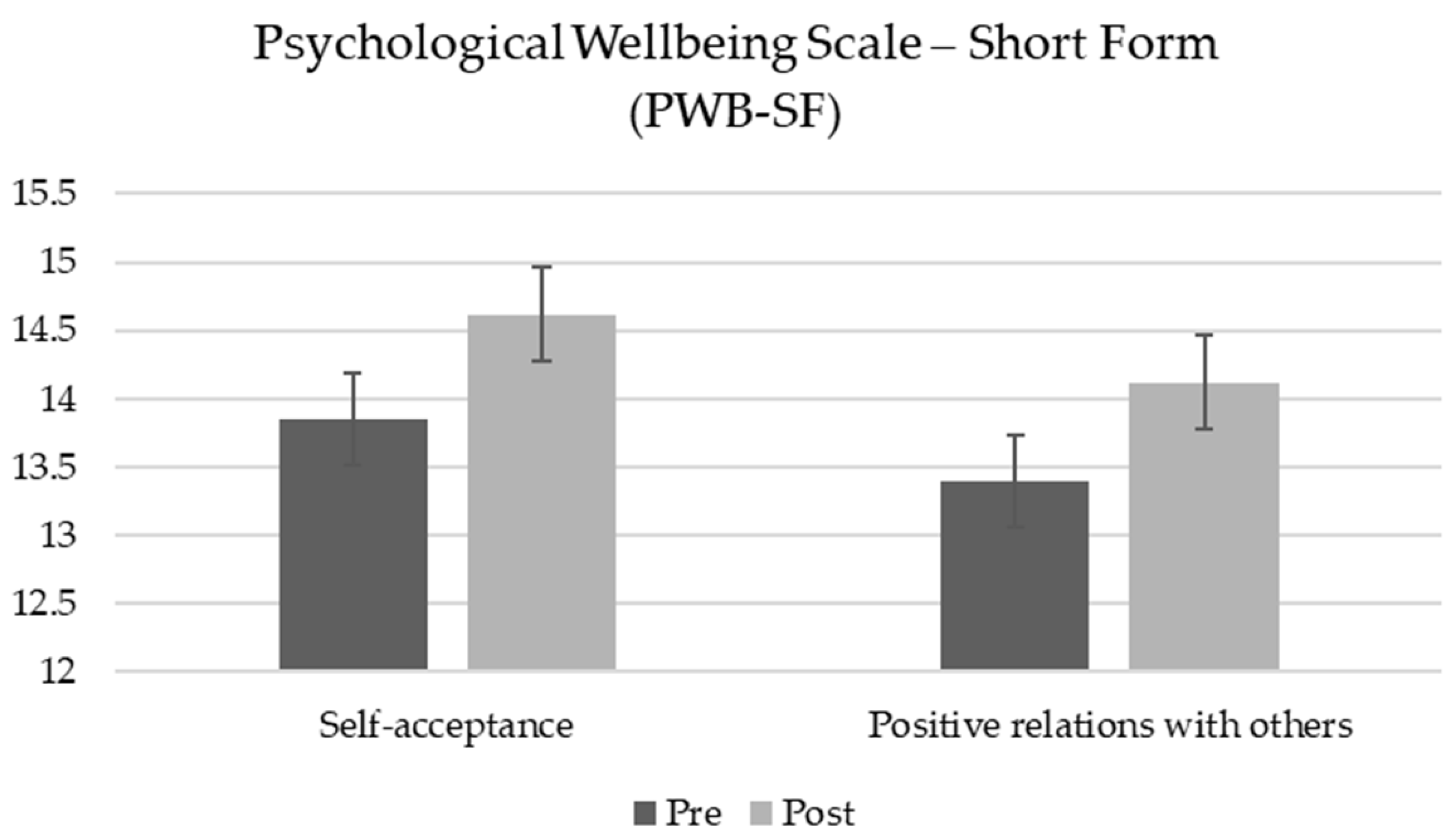
3.5. Psychological Well-Being
3.6. Relations Between Arousal Regulation and Professional Quality of Life
3.6.1. Compassion Satisfaction
3.6.2. Burnout
3.6.3. Secondary Traumatic Stress
3.7. Summary of Key Findings
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joinson, C. Coping with compassion fatigue. Nursing 1992, 22, 116–121. [Google Scholar] [PubMed]
- Patole, S.; Pawale, D.; Rath, C. Interventions for Compassion Fatigue in Healthcare Providers—A Systematic Review of Randomised Controlled Trials. Healthcare 2024, 12, 171. [Google Scholar] [CrossRef]
- Figley, C.R. Compassion fatigue: Toward a new understanding of the costs of caring. In Secondary Traumatic Stress: Self-Care Issues for Clinicians, Researchers, and Educators, 2nd ed.; Stamm, B.H., Ed.; The Sidran Press: Baltimore, MD, USA, 1999; pp. 3–28. [Google Scholar]
- Figley, C.R. Compassion fatigue as secondary traumatic stress disorder: An overview. In Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized; Psychosocial Stress Series; Figley, C.R., Ed.; Routledge Taylor and Francis Group: New York, NY, USA, 1995; pp. 1–20. [Google Scholar]
- Figley, C.R.; Kleber, R.J. Beyond the “victim”: Secondary traumatic stress. In Beyond Trauma: Cultural and Societal Dynamics; Kleber, R.J., Figley, C.R., Gersons, B.P.R., Eds.; Plenum Press: New York, NY, USA, 1995; pp. 75–98. [Google Scholar]
- Stamm, B.H. Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL). 2009. Available online: https://proqol.org/proqol-measure (accessed on 19 October 2024).
- Stamm, B.H. The Concise ProQOL Manual. 2010. Available online: https://proqol.org/proqol-manual (accessed on 19 October 2024).
- De Luca, R.; Bonanno, M.; Maggio, M.G.; Todaro, A.; Rifici, C.; Mento, C.; Muscatello, M.R.A.; Castorina, M.V.; Tonin, P.; Quartarone, A.; et al. Compassion Fatigue in a Cohort of South Italian Nurses and Hospital-Based Clinical Social Workers Following COVID-19: A Cross-Sectional Survey. J. Clin. Med. 2024, 13, 4200. [Google Scholar] [CrossRef]
- Rayani, A.; Hannan, J.; Alreshidi, S.; Aboshaiqah, A.; Alodhailah, A.; Hakamy, E. Compassion Satisfaction, Burnout, and Secondary Traumatic Stress among Saudi Nurses at Medical City: A Cross-Sectional Study. Healthcare 2024, 12, 847. [Google Scholar] [CrossRef] [PubMed]
- Lobo, R.; Kumar, S.P.; Tm, R. Professional Quality of Life Among Mental Health Nurses: A Systematic Review and Meta-Analysis. Int. J. Ment. Health Nurs. 2024, 33, 2005–2025. [Google Scholar] [CrossRef]
- Algamdi, M. Prevalence of Oncology Nurses’ Compassion Satisfaction and Compassion Fatigue: Systematic Review and Meta-Analysis. Nurs. Open 2022, 9, 44–56. [Google Scholar] [CrossRef]
- Alharbi, J.; Jackson, D.; Usher, K. Compassion Fatigue in Critical Care Nurses: An Integrative Review of the Literature. Saudi Med. J. 2019, 40, 1087–1097. [Google Scholar] [CrossRef]
- Alipio, J.; Florendo, M.G.; Montilla, M.G.; Narvaez, R.A. Compassion Fatigue in Oncology Nurses: An Integrative Review. World J. Cancer Oncol. Res. 2023, 2, 85–101. Available online: https://www.scipublications.com/journal/index.php/wjcor/article/view/732 (accessed on 19 October 2024). [CrossRef]
- Hooper, C.; Craig, J.; Janvrin, D.R.; Wetsel, M.A.; Reimels, E. Compassion Satisfaction, Burnout, and Compassion Fatigue Among Emergency Nurses Compared With Nurses in Other Selected Inpatient Specialties. J. Emerg. Nurs. 2010, 36, 420–427. [Google Scholar] [CrossRef]
- Ortega-Campos, E.; Vargas-Román, K.; Velando-Soriano, A.; Suleiman-Martos, N.; Cañadas-de la Fuente, G.A.; Albendín-García, L.; Gómez-Urquiza, J.L. Compassion Fatigue, Compassion Satisfaction, and Burnout in Oncology Nurses: A Systematic Review and Meta-Analysis. Sustainability 2020, 12, 72. [Google Scholar] [CrossRef]
- Garnett, A.; Hui, L.; Oleynikov, C.; Boamah, S. Compassion Fatigue in Healthcare Providers: A Scoping Review. BMC Health Serv. Res. 2023, 23, 1336. [Google Scholar] [CrossRef] [PubMed]
- Gribben, J.L.; Kase, S.M.; Waldman, E.D.; Weintraub, A.S. A Cross-Sectional Analysis of Compassion Fatigue, Burnout, and Compassion Satisfaction in Pediatric Critical Care Physicians in the United States. Pediatr. Crit. Care Med. 2019, 20, 213–222. [Google Scholar] [CrossRef]
- Ruiz-Fernández, M.D.; Pérez-García, E.; Ortega-Galán, Á.M. Quality of Life in Nursing Professionals: Burnout, Fatigue, and Compassion Satisfaction. Int. J. Environ. Res. Public Health 2020, 17, 1253. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.E.; Boscarino, J.A.; Figley, C.R. Compassion Fatigue and Psychological Distress Among Social Workers: A Validation Study. Am. J. Orthopsychiatry 2006, 76, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Casado, T.; Rosselló, M.V.; Cañas-Lerma, A. Changes in Social Interventions after COVID-19: The Experience of Front-Line Social Workers. Soc. Sci. 2023, 12, 41. [Google Scholar] [CrossRef]
- Craig, C.D.; Sprang, G. Compassion Satisfaction, Compassion Fatigue, and Burnout in a National Sample of Trauma Treatment Therapists. Anxiety Stress Coping 2010, 23, 319–339. [Google Scholar] [CrossRef]
- Dehlin, M.; Lundh, L.G. Compassion Fatigue and Compassion Satisfaction Among Psychologists: Can Supervision and a Reflective Stance Be of Help? J. Pers.-Oriented Res. 2018, 4, 95–107. [Google Scholar] [CrossRef]
- Watson, V.C.; Begun, S. Burnout in Social Work: A Review of the Literature within the Context of COVID-19. Soc. Work Public Health 2025, 40, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Campos i Arnal, A.; Galiana, L.; Sánchez-Ruiz, J.; Sansó, N. Cross-Sectional Study of the Professional Quality of Life of Palliative Care Professionals during the COVID-19 Pandemic. Healthcare 2024, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Han, S.-J.; Lee, S.-Y.; Kim, S.-E. An Exploratory Study of Psychological Distress, Professional Quality of Life, Effort-Reward Imbalance, and Turnover Intention of Hospital Nurses during the COVID-19 Pandemic. Healthcare 2023, 11, 2695. [Google Scholar] [CrossRef] [PubMed]
- Rania, N.; Coppola, I.; Brucci, M. Mental Health and Quality of Professional Life of Healthcare Workers: One Year after the Outbreak of the COVID-19 Pandemic. Sustainability 2023, 15, 2977. [Google Scholar] [CrossRef]
- Romito, B.T.; Okoro, E.N.; Ringqvist, J.R.B.; Goff, K.L. Burnout and Wellness: The Anesthesiologist’s Perspective. Am. J. Lifestyle Med. 2020, 15, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Vittori, A.; Marinangeli, F.; Bignami, E.G.; Simonini, A.; Vergallo, A.; Fiore, G.; Petrucci, E.; Cascella, M.; Pedone, R. Analysis on Burnout, Job Conditions, Alexithymia, and Other Psychological Symptoms in a Sample of Italian Anesthesiologists and Intensivists, Assessed Just before the COVID-19 Pandemic: An AAROI-EMAC Study. Healthcare 2022, 10, 1370. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician Burnout: Contributors, Consequences, and Solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef]
- Lee, T.; Becerra, B.J.; Becerra, M.B. “Seems Like There Is No Stopping Point at All Whatsoever”: A Mixed-Methods Analysis of Public Health Workforce Perception on COVID-19 Pandemic Management and Future Needs. Int. J. Environ. Res. Public Health 2023, 20, 6350. [Google Scholar] [CrossRef]
- Armstrong, J.W.; Turne, L.N. Mindfulness-based interventions to reduce stress and burnout in nurses: An integrative review. Br. J. Ment. Health Nurs. 2022, 11, 1–11. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; Martínez-Arriaga, R.J.; Herdoiza-Arroyo, P.E.; Bautista-Valerio, E.; de la Rosa-Gómez, A.; Castellanos Vargas, R.O.; Lacomba-Trejo, L.; Mateu-Mollá, J.; Lupercio Ramírez, M.d.J.; Figueroa González, J.A.; et al. E-Health Psychological Intervention for COVID-19 Healthcare Workers: Protocol for its Implementation and Evaluation. Int. J. Environ. Res. Public Health 2022, 19, 12749. [Google Scholar] [CrossRef]
- Katzman, J.W.; Tomedi, L.E.; Pandey, N.; Richardson, K.; Xenakis, S.N.; Heines, S.; Grabbe, L.; Magdaleno, Y.; Mehta, A.; Welton, R.; et al. Caring for the Caregivers: Improving Mental Health among Health Professionals Using the Behavioral Health Professional Workforce Resilience ECHO Program. Healthcare 2024, 12, 1741. [Google Scholar] [CrossRef] [PubMed]
- Benavides-Gil, G.; Martínez-Zaragoza, F.; Fernández-Castro, J.; García-Campayo, J.; Demarzo, M.; Miralles, C.; Pascual, A.; Oliván-Blázquez, B. Mindfulness-Based Interventions for Improving Mental Health of Frontline Healthcare Professionals during the COVID-19 Pandemic: A Systematic Review. Syst. Rev. 2024, 13, 160. [Google Scholar] [CrossRef]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Fu, C.H.; Hart, R.; Eiroa-Orosa, F.J. A Systematic Review and Meta-Analysis of the Impact of Mindfulness-Based Interventions on the Well-Being of Healthcare Professionals. Mindfulness 2019, 10, 1193–1216. [Google Scholar] [CrossRef]
- Ong, N.Y.; Teo, F.J.J.; Ee, J.Z.Y.; Yau, C.E.; Thumboo, J.; Tan, H.K.; Ng, Q.X. Effectiveness of Mindfulness-Based Interventions on the Well-Being of Healthcare Workers: A Systematic Review and Meta-Analysis. Gen. Psychiatry 2024, 37, e101115. [Google Scholar] [CrossRef] [PubMed]
- Lalani, K.; O’Neal, M.; Joannou, S.L.; Gopal, B.; Champagne-Langabeer, T. Helping Frontline Workers in Texas—A Framework for Resource Development. Int. J. Environ. Res. Public Health 2023, 20, 6935. [Google Scholar] [CrossRef] [PubMed]
- Pérez, V.; Menéndez-Crispín, E.J.; Sarabia-Cobo, C.; de Lorena, P.; Fernández-Rodríguez, A.; González-Vaca, J. Mindfulness-Based Intervention for the Reduction of Compassion Fatigue and Burnout in Nurse Caregivers of Institutionalized Older Persons with Dementia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 11441. [Google Scholar] [CrossRef] [PubMed]
- Sulosaari, V.; Unal, E.; Cinar, F.I. The effectiveness of mindfulness-based interventions on the psychological well-being of nurses: A systematic review. Appl. Nurs. Res. 2022, 64, 151565. [Google Scholar] [CrossRef] [PubMed]
- Lipsa, J.M.; Rajkumar, E.; Gopi, A.; Romate, J. Effectiveness of Psychological Interventions for Compassion Fatigue: A Systematic Review and Meta-Analysis. J. Occup. Health 2024, 66, uiae061. [Google Scholar] [CrossRef] [PubMed]
- Lluch, C.; Galiana, L.; Doménech, P.; Sansó, N. The Impact of the COVID-19 Pandemic on Burnout, Compassion Fatigue, and Compassion Satisfaction in Healthcare Personnel: A Systematic Review of the Literature Published during the First Year of the Pandemic. Healthcare 2022, 10, 364. [Google Scholar] [CrossRef] [PubMed]
- Gentry, J.E. Compassion Fatigue: A Crucible of Transformation. J. Trauma Pract. 2002, 1, 37–61. [Google Scholar] [CrossRef]
- Gentry, J.E.; Baggerly, J.; Baranowsky, A. Training-as-Treatment: Effectiveness of the Certified Compassion Fatigue Specialist Training. Int. J. Emerg. Ment. Health 2004, 6, 147–155. [Google Scholar] [PubMed]
- Orrù, G.; Marzetti, F.; Conversano, C.; Vagheggini, G.; Miccoli, M.; Ciacchini, R.; Panait, E.; Gemignani, A. Secondary Traumatic Stress and Burnout in Healthcare Workers during COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2021, 18, 337. [Google Scholar] [CrossRef]
- Kriakous, S.A.; Elliott, K.A.; Lamers, C.; Owen, R. The Effectiveness of Mindfulness-Based Stress Reduction on the Psychological Functioning of Healthcare Professionals: A Systematic Review. Mindfulness 2021, 12, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Campanella, F.; Crescentini, C.; Urgesi, C.; Fabbro, F. Mindfulness-Oriented Meditation Improves Self-Related Character Scales in Healthy Individuals. Compr. Psychiatry 2014, 55, 1269–1278. [Google Scholar] [CrossRef]
- Gentry, J.E.; Baranowsky, A.B.; Dunning, K. The Accelerated Recovery Program (ARP) for Compassion Fatigue. In Treating Compassion Fatigue; Figley, C.R., Ed.; Brunner-Routledge: New York, NY, USA, 2002; pp. 123–137. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Delacorte: New York, NY, USA, 1990. [Google Scholar]
- Fabbro, F.; Crescentini, C. La meditazione orientata alla mindfulness (MOM) nella ricerca psicologica. Ricerche di Psicologia 2016, 4, 457–472. [Google Scholar] [CrossRef]
- Hayes, S.C.; Lillis, J. Acceptance and Commitment Therapy; American Psychological Association: Washington, DC, USA, 2012. [Google Scholar] [CrossRef]
- Polk, K.L.; Schoendorff, B. (Eds.) The ACT Matrix: A New Approach to Building Psychological Flexibility across Settings and Populations; Context Press/New Harbinger Publications: Oakland, CA, USA, 2014. [Google Scholar]
- Neff, K.D. The Science of Self-Compassion. In Wisdom and Compassion in Psychotherapy: Deepening Mindfulness in Clinical Practice; Germer, C.K., Siegel, R.D., Eds.; The Guilford Press: New York, NY, USA, 2012; pp. 79–92. [Google Scholar]
- Ogden, P.; Minton, K.; Pain, C. Trauma and the Body: A Sensorimotor Approach to Psychotherapy; W.W. Norton & Company: New York, NY, USA, 2006. [Google Scholar]
- Porges, S.W. The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation; W.W. Norton & Co.: New York, NY, USA, 2011. [Google Scholar]
- Khazan, I. Biofeedback and Mindfulness in Everyday Life: Practical Solutions for Improving Your Health and Performance; W.W. Norton & Company: New York, NY, USA, 2019. [Google Scholar]
- Lehrer, P.M.; Gevirtz, R. Heart rate variability biofeedback: How and why does it work? Front. Psychol. 2014, 5, 756. [Google Scholar] [CrossRef] [PubMed]
- Palestini, L.; Prati, G.; Pietrantoni, L.; Cicognani, E. La Qualità della Vita Professionale nel Lavoro di Soccorso: Un Contributo alla Validazione Italiana della Professional Quality of Life Scale (ProQOL). Psicoter. Cogn. Comport. 2009, 15, 205–227. [Google Scholar]
- Iani, L.; Lauriola, M.; Cafaro, V. The Assessment of Mindfulness Skills: The “What” and the “How”. J. Ment. Health 2020, 29, 144–151. [Google Scholar] [CrossRef]
- Ruini, C.; Ottolini, F.; Rafanelli, C.; Ryff, C.D.; Fava, G.A. Italian Validation of Psychological Well-Being Scales (PWB). Riv. Psichiatr. 2003, 38, 117–130. [Google Scholar]
- Sirigatti, S.; Stefanile, C.; Giannetti, E.; Iani, L.; Penzo, I.; Mazzeschi, A. Assessment of Factor Structure of Ryff’s Psychological Well-Being Scales in Italian Adolescents. Giunti Organ. Spec. 2009, 259, 30–50. [Google Scholar]
- Cocker, F.; Joss, N. Compassion Fatigue among Healthcare, Emergency and Community Service Workers: A Systematic Review. Int. J. Environ. Res. Public Health 2016, 13, 618. [Google Scholar] [CrossRef] [PubMed]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A Systematic Review of the Impact of Mindfulness on the Well-Being of Healthcare Professionals. J. Clin. Psychol. 2018, 74, 319–355. [Google Scholar] [CrossRef]
- Tripathi, S.K.; Mulkey, D.C. Implementing Brief Mindfulness-Based Interventions to Reduce Compassion Fatigue. Crit. Care Nurse 2023, 43, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Burton, A.; Burgess, C.; Dean, S.; Koutsopoulou, G.Z.; Hugh-Jones, S. How Effective are Mindfulness-Based Interventions for Reducing Stress Among Healthcare Professionals? A Systematic Review and Meta-Analysis. Stress Health 2017, 33, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.C.; Thompson, D.R.; Jenkins, Z.M.; Ski, C.F. Mindfulness Mediates the Physiological Markers of Stress: Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2017, 95, 156–178. [Google Scholar] [CrossRef] [PubMed]
- Steffen, P.R.; Austin, T.; DeBarros, A.; Brown, T. The Impact of Resonance Frequency Breathing on Measures of Heart Rate Variability, Blood Pressure, and Mood. Front. Public Health 2017, 5, 222. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, L.; Fisher, Z.; Kemp, A.H. The Complex Construct of Wellbeing and the Role of Vagal Function. Front. Integr. Neurosci. 2022, 16, 925664. [Google Scholar] [CrossRef] [PubMed]
- Nykliček, I.; Vingerhoets, A.; Zeelenberg, M. (Eds.) Emotion Regulation and Well-Being; Springer Science + Business Media: New York, NY, USA, 2011. [Google Scholar] [CrossRef]
- Paiva-Salisbury, M.L.; Schwanz, K.A. Building Compassion Fatigue Resilience: Awareness, Prevention, and Intervention for Pre-Professionals and Current Practitioners. J. Health Serv. Psychol. 2022, 48, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Rushforth, A.; Durk, M.; Rothwell-Blake, G.A.A.; Kirkman, A.; Ng, F.; Kotera, Y. Self-Compassion Interventions to Target Secondary Traumatic Stress in Healthcare Workers: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 6109. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Core Themes | Theoretical Frameworks and Intervention Models |
|---|---|
| Mindfulness meditation |
|
| Mindfulness-based approaches |
|
| Compassion satisfaction (CS) and Compassion fatigue (CF) |
|
| Psychological trauma | |
| Vagal stimulation and autoregulation | Heart Rate Variability (HRV) Biofeedback [55,56] |
| Session | Title | Psychoeducation | Guided Work Reflection | Mindfulness Practices | Self-Regulation Exercises |
|---|---|---|---|---|---|
| 1 | Breath | Mindfulness; Resonance frequency breathing | Professional values | Mindful breathing meditation | Diaphragmatic breathing at resonance frequency |
| 2 | Body | Compassion fatigue; Arousal modulation model | Professional goals | Body scan meditation | Stretching (eyes and neck) |
| 3 | Mind | Psychological trauma; Polyvagal theory | Committed action at work | Mind awareness meditation | Stretching (sternocleidomastoid and trapezius) |
| 4 | Equanimity | From reaction to response | Work-related obstacles | Comprehensive meditation (breath, body scan, mind awareness) | Stretching (psoas) |
| 5 | Relationships | Compassion; Self-compassion | Experiential avoidance loops at work | Loving-kindness exercises | Soothing touch |
| 6 | Integration | Resilience; Medically unexplained symptoms; Lifestyle | Individual resilience plan | ||
| Variable | Category | N 1 | Percentage (%) |
|---|---|---|---|
| Gender | Male | 10 | 14% |
| Female | 63 | 86% | |
| Educational level | |||
| Degree | High school | 10 | 14% |
| Bachelor’s degree | 15 | 21% | |
| Master’s degree | 19 | 26% | |
| PhD or Postgraduate diploma | 29 | 40% | |
| Professional background | |||
| Healthcare professionals | Medical doctor | 6 | 8% |
| (M = 2, F = 4; Age 52.33, SD = 10.23) | |||
| Psychologist | 38 | 52% | |
| (M = 4, F = 34; Age 49.24, SD = 7.78) | |||
| Nurse | 18 | 25% | |
| (M = 3, F = 15; Age 49.61, SD = 10.79) | |||
| Healthcare assistant | 2 | 3% | |
| (M = 0, F = 2; Age 45.50, SD = 14.85) | |||
| Rehabilitation therapist | 8 | 11% | |
| (M = 1, F = 7; Age 40.50, SD = 10.28) | |||
| Biomedical laboratory technician | 1 | 1% | |
| (M = 1, F = 0; Age 54) | |||
| Health and wellness characteristics | |||
| Physical Activity Level | Physically Active Person | 22 | 30% |
| Partially Active Person | 37 | 51% | |
| Sedentary Person | 14 | 19% | |
| Meditation | Yes | 16 | 22% |
| No | 57 | 78% | |
| Breathing Exercises | Yes | 18 | 25% |
| No | 55 | 75% | |
| Mental Health Diagnosis | Yes | 4 | 5% |
| No | 69 | 95% | |
| Psychotropic Medication Use | Yes | 4 | 5% |
| No | 69 | 95% | |
| Scale | Time Point | M | SD | ANOVA F | p-Value 1 | ηp2 |
|---|---|---|---|---|---|---|
| Professional Quality of Life (ProQOL) | ||||||
| Compassion satisfaction | Pre | 37.47 | 5.85 | 16.84 | <0.001 | 0.19 |
| Post | 39.18 | 5.84 | ||||
| Burnout | Pre | 19.43 | 4.83 | 9.21 | 0.003 | 0.11 |
| Post | 18.06 | 4.92 | ||||
| Secondary traumatic stress | Pre | 21.01 | 5.12 | 22.57 | <0.001 | 0.24 |
| Post | 19.08 | 5.43 | ||||
| Five Facet Mindfulness Questionnaire—Short Form (FFMQ-SF) | ||||||
| Observing | Pre | 14.08 | 3.59 | 9.13 | 0.003 | 0.11 |
| Post | 15.36 | 3.44 | ||||
| Describing | Pre | 17.78 | 3.90 | 7.04 | 0.01 | 0.09 |
| Post | 18.90 | 3.85 | ||||
| Acting with awareness | Pre | 17.21 | 4.18 | 13.83 | <0.001 | 0.16 |
| Post | 19.11 | 3.86 | ||||
| Non-judging | Pre | 16.69 | 4.64 | 0.57 | 0.454 | 0.01 |
| Post | 17.10 | 4.82 | ||||
| Non-reacting | Pre | 15.01 | 3.44 | 10.77 | 0.002 | 0.13 |
| Post | 16.14 | 3.20 | ||||
| Arousal Modulation Model Questionnaire (AMMQ) | ||||||
| Optimal arousal zone | Pre | 2.74 | 0.69 | 22.28 | <0.001 | 0.24 |
| Post | 3.01 | 0.65 | ||||
| Fight/flight | Pre | 1.16 | 0.90 | 11.20 | 0.001 | 0.14 |
| Post | 0.85 | 0.77 | ||||
| Freeze | Pre | 0.75 | 0.66 | 4.71 | 0.033 | 0.06 |
| Post | 0.60 | 0.62 | ||||
| Feigned death | Pre | 1.00 | 0.73 | 5.98 | 0.017 | 0.08 |
| Post | 0.82 | 0.72 | ||||
| Psychological Well-Being Scale—Short Form (PWB-SF) | ||||||
| Self-acceptance | Pre | 13.85 | 3.17 | 6.35 | 0.014 | 0.08 |
| Post | 14.62 | 2.90 | ||||
| Autonomy | Pre | 12.16 | 3.38 | 0.46 | 0.500 | 0.01 |
| Post | 12.47 | 3.39 | ||||
| Personal growth | Pre | 16.21 | 2.20 | 0.99 | 0.324 | 0.01 |
| Post | 16.44 | 2.15 | ||||
| Positive relations with others | Pre | 13.40 | 2.91 | 4.34 | 0.041 | 0.06 |
| Post | 14.12 | 2.87 | ||||
| Purpose in life | Pre | 14.32 | 3.34 | 1.55 | 0.218 | 0.02 |
| Post | 14.73 | 3.11 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Antoni, F.; Matiz, A.; Crescentini, C. Mindfulness-Oriented Professional Resilience (MOPR) Training to Reduce Compassion Fatigue in Healthcare Workers: A Pilot Study. Healthcare 2025, 13, 92. https://doi.org/10.3390/healthcare13020092
D’Antoni F, Matiz A, Crescentini C. Mindfulness-Oriented Professional Resilience (MOPR) Training to Reduce Compassion Fatigue in Healthcare Workers: A Pilot Study. Healthcare. 2025; 13(2):92. https://doi.org/10.3390/healthcare13020092
Chicago/Turabian StyleD’Antoni, Fabio, Alessio Matiz, and Cristiano Crescentini. 2025. "Mindfulness-Oriented Professional Resilience (MOPR) Training to Reduce Compassion Fatigue in Healthcare Workers: A Pilot Study" Healthcare 13, no. 2: 92. https://doi.org/10.3390/healthcare13020092
APA StyleD’Antoni, F., Matiz, A., & Crescentini, C. (2025). Mindfulness-Oriented Professional Resilience (MOPR) Training to Reduce Compassion Fatigue in Healthcare Workers: A Pilot Study. Healthcare, 13(2), 92. https://doi.org/10.3390/healthcare13020092