




The Mediating Effect of Social Networks on the Impact of Health Perceptions on the Quality of Life in Older Adults

Abstract
1. Introduction
2. Materials and Methods
2.1. Purpose of the Study
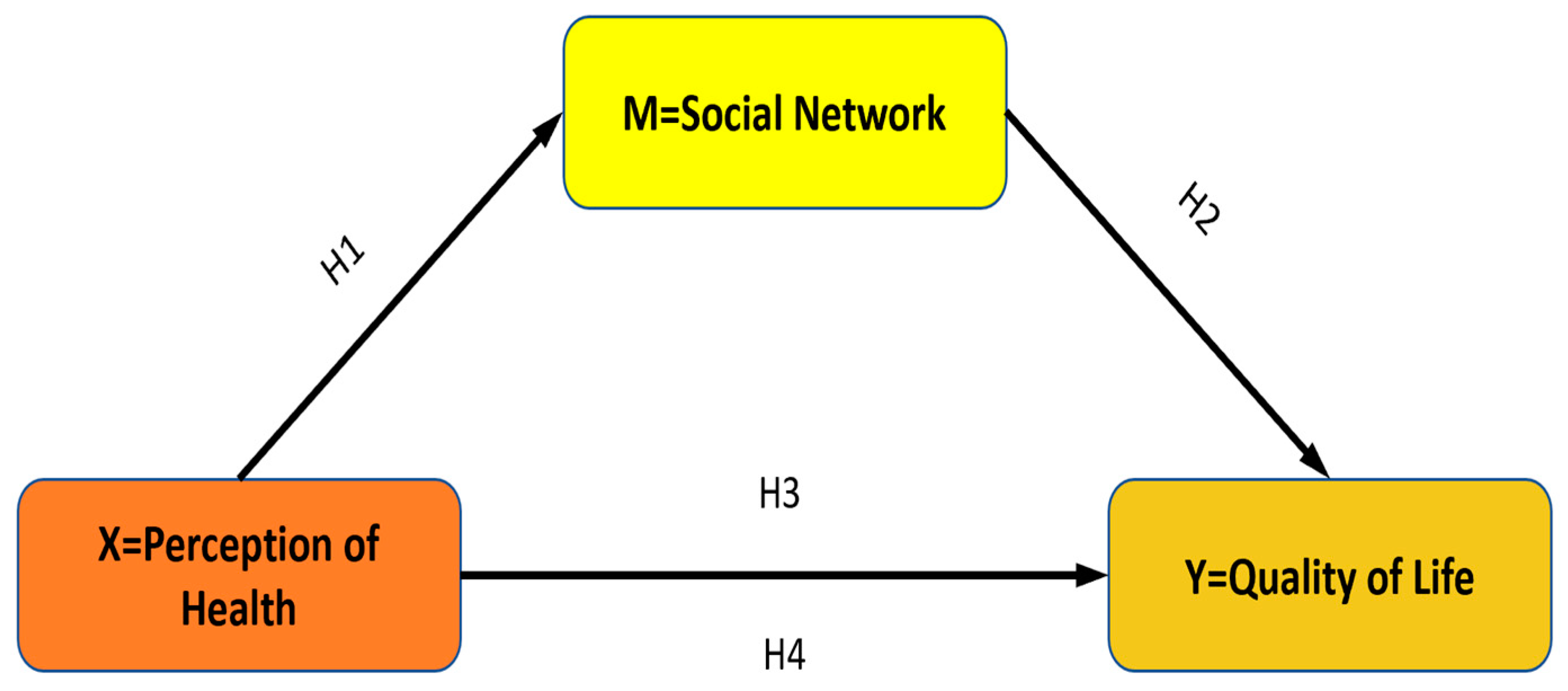
2.2. Study Design and Hypotheses
2.3. Sample of the Study
- Participants must be aged 65 and older.
- No communication barriers should be present.
- Willingness to participate in the study.
- The data collection forms contain incomplete or incorrect information.
- Wanting to leave the study at any stage of the study.
2.4. Data Collection Tools
2.4.1. Personal Information Form
2.4.2. Perception of Health Scale (PHS)
2.4.3. Lubben Social Network Scale (LSNS-6)
2.4.4. World Health Organization Quality of Life Instrument—Older Adults Module (WHOQOL-OLD)
2.5. Data Analysis
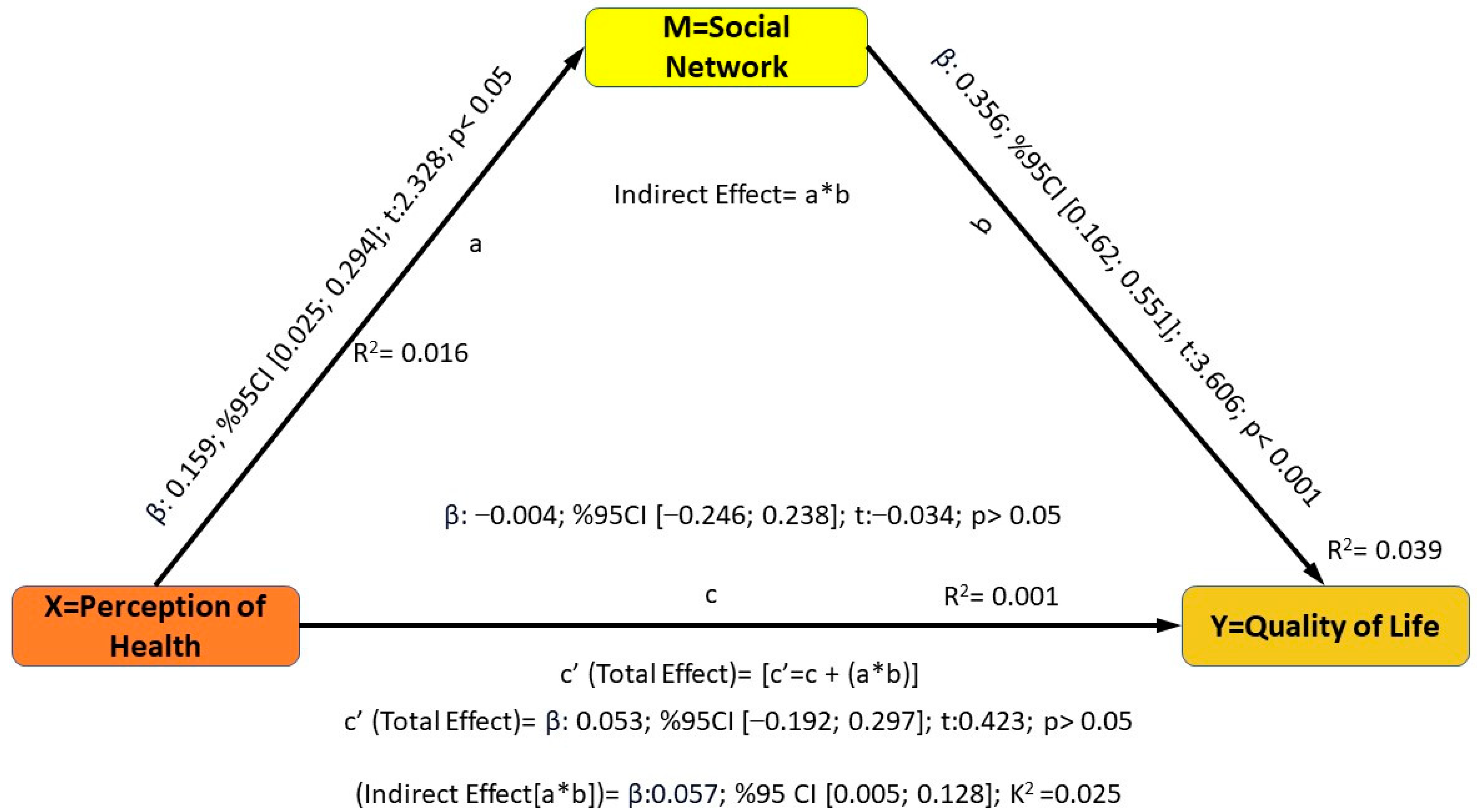
3. Results
4. Discussion
4.1. Limitations of the Study
4.2. Recommendations for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, M.; De Gagne, J.C.; Shin, H. Social networks, health promoting-behavior, and health-related quality of life in older Korean adults. Nurs. Health Sci. 2018, 20, 79–88. [Google Scholar] [CrossRef] [PubMed]
- TUİK Turkish Statistical Institute. 2023. Available online: https://data.tuik.gov.tr/Bulten/Index?p=Adrese-Dayali-Nufus-Kayit-Sistemi-Sonuclari-2023-49684 (accessed on 1 August 2024).
- Heiman, H.; Artiga, S. Issue Brief. Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity; Kaiser Family Foundation: San Francisco, CA, USA, 2015. [Google Scholar]
- Kim, B.J. Mediating effect of adult day health care (ADHC) and family network on quality of life among low-income older Korean immigrants. Res. Aging 2014, 36, 343–363. [Google Scholar] [CrossRef]
- Langford, C.P.H.; Bowsher, J.; Maloney, J.P.; Lillis, P.P. Social support: A conceptual analysis. J. Adv. Nursing. 1997, 25, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Cornwell, E.Y.; Waite, L.J. Social disconnectedness, perceived isolation, and health among older adults. J. Health Soc. Behav. 2009, 50, 31–48. [Google Scholar] [CrossRef]
- Moreno-Tamayo, K.; Manrique-Espinoza, B.; Ramírez-García, E.; Sánchez-García, S. Social isolation undermines quality of life in older adults. Int. Psychogeriatr. 2020, 32, 1283–1292. [Google Scholar] [CrossRef]
- Hussain, B.; Mirza, M.; Baines, R.; Burns, L.; Stevens, S.; Asthana, S.; Chatterjee, A. Loneliness and social networks of older adults in rural communities: A narrative synthesis systematic review. Front. Public Health 2023, 11, 1113864. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.C.; Donnelly, M.; Bhatnagar, P.; Carlin, A.; Kee, F.; Hunter, R.F. Peer social network processes and adolescent health behaviors: A systematic review. Prev. Med. 2020, 130, 105900. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Knowlton, A.R. Social network assessments and interventions for health behavior change: A critical review. Behav. Med. 2015, 41, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, N.R. A review of social isolation: An important but underassessed condition in older adults. J. Prim. Prev. 2012, 33, 137–152. [Google Scholar] [CrossRef]
- Stokes, J.E.; Moorman, S.M. Influence of the social network on married and unmarried older adults’ mental health. Gerontologist 2018, 58, 1109–1113. [Google Scholar] [CrossRef] [PubMed]
- Seeman, T.E. Health promoting effects of friends and family on health outcomes in older adults. Am. J. Health Promot. 2000, 14, 362–370. [Google Scholar] [CrossRef]
- Rowe, J.W.; Fulmer, T.; Fried, L. Preparing for better health and health care for an aging population. Jama 2016, 316, 1643–1644. [Google Scholar] [CrossRef]
- Shin, J.K.; Kim, K.W.; Park, J.H.; Lee, J.J.; Huh, Y.; Lee, S.B.; Choi, E.A.; Lee, D.Y.; Woo, J.I. Impacts of poor social support on general health status in community-dwelling Korean elderly: The results from the Korean longitudinal study on health and aging. Psychiatry Investig. 2008, 5, 155. [Google Scholar] [CrossRef] [PubMed]
- Ichida, Y.; Hirai, H.; Kondo, K.; Kawachi, I.; Takeda, T.; Endo, H. Does social participation improve self-rated health in the older population? A quasi-experimental intervention study. Soc. Sci. Med. 2013, 94, 83–90. [Google Scholar] [CrossRef]
- de Belvis, A.G.; Avolio, M.; Spagnolo, A.; Damiani, G.; Sicuro, L.; Cicchetti, A.; Ricciardi, W.; Rosano, A. Factors associated with health-related quality of life: The role of social relationships among the elderly in an Italian region. Public Health 2008, 122, 784–793. [Google Scholar] [CrossRef]
- Abu Hammattah, A.; Mohd Yunus, R.; Matthias Müller, A.; Bahyah Kamaruzzaman, S.; Naqiah Hairi, N. Association between structural social support and quality of life among urban older Malaysians. Australas. J. Ageing 2021, 40, 390–396. [Google Scholar] [CrossRef]
- Hamren, K.; Chungkham, H.S.; Hyde, M. Religion, spirituality, social support and quality of life: Measurement and predictors CASP-12 (v2) amongst older Ethiopians living in Addis Ababa. Aging Ment. Health 2015, 19, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Kooshiar, H.; Yahaya, N.; Hamid, T.A.; Abu Samah, A.; Sedaghat Jou, V. Living arrangement and life satisfaction in older Malaysians: The mediating role of social support function. PLoS ONE 2012, 7, e43125. [Google Scholar] [CrossRef]
- Mohamad Fuad, M.A.; Yacob, H.; Mohamed, N.; Wong, N.I. Association of sociodemographic factors and self-perception of health status on oral health-related quality of life among the older persons in Malaysia. Geriatr. Gerontol. Int. 2020, 20, 57–62. [Google Scholar] [CrossRef]
- Kim, B.-R.; Hwang, H.-H. Analysis of Major Factors Affecting the Quality of Life of the Elderly in Korea in Preparation for a Super-Aged Society. Int. J. Environ. Res. Public Health 2022, 19, 9618. [Google Scholar] [CrossRef]
- Altay, B.; Çavuşoğlu, F.; Çal, A. The factors affecting the perception of elderly patients towards health, quality of life and health-related quality of life. TAF Prev. Med. Bull. 2016, 15, 181–189. [Google Scholar] [CrossRef]
- Choi, H.J.; Lee, H.J. A study on factors affecting quality of life for the elderly: Focusing on socio-demographic, environmental, and institutional characteristics. J. Korean Soc. Wellness 2019, 14, 103–112. [Google Scholar] [CrossRef]
- Jung, J.P.; Lee, E.R.; Sin, M.S. The health of the elderly impact on quality of life. J. Korean Acad. Health Welf. Elder. 2012, 4, 51–61. [Google Scholar]
- Kim, J.Y.; Lee, S.G.; Lee, S.K. The relationship between health behaviors, health status, activities of daily living and health-related quality of life in the elderly. J. Korean Gerontol. Soc. 2010, 30, 471–484. [Google Scholar]
- Bhatia, R.; Hirsch, C.; Arnold, A.M.; Newman, A.B.; Mukamal, K.J. Social networks, social support, and life expectancy in older adults: The Cardiovascular Health Study. Arch. Gerontol. Geriatr. 2023, 111, 104981. [Google Scholar] [CrossRef] [PubMed]
- Schafer, M.H.; Sun, H.; Lee, J.A. Compensatory connections? Living alone, loneliness, and the buffering role of social connection among older American and European adults. J. Gerontol. Ser. B 2022, 77, 1550–1560. [Google Scholar] [CrossRef] [PubMed]
- Mancini, J.A.; Quinn, W.; Gavigan, M.A.; Franklin, H. Social network interaction among older adults: Implications for life satisfaction. Human Relat. 1980, 33, 543–554. [Google Scholar] [CrossRef]
- Raggi, A.; Corso, B.; Minicuci, N.; Quintas, R.; Sattin, D.; De Torres, L.; Chatterji, S.; Frisoni, G.B.; Haro, J.M.; Koskinen, S. Determinants of quality of life in ageing populations: Results from a cross-sectional study in Finland, Poland and Spain. PLoS ONE 2016, 11, e0159293. [Google Scholar] [CrossRef]
- Condello, G.; Capranica, L.; Migliaccio, S.; Forte, R.; Di Baldassarre, A.; Pesce, C. Energy balance and active lifestyle: Potential mediators of health and quality of life perception in aging. Nutrients 2019, 11, 2122. [Google Scholar] [CrossRef]
- Kalınkara, V. Population Aging and Its Social Dimensions, Sociology of Aging; Ceylan, H., Ed.; Nobel Publishing: Ankara, Turkey, 2016. [Google Scholar]
- Karasar, N. Scientific Research Methodology; Nobel Publishing: Ankara, Turkey, 2013. [Google Scholar]
- Diamond, J.J.; Becker, J.A.; Arenson, C.A.; Chambers, C.V.; Rosenthal, M.P. Development of a scale to measure adults’ perceptions of health: Preliminary findings. J. Community Psychol. 2007, 35, 557–561. [Google Scholar] [CrossRef]
- Lubben, J.E. Assessing social networks among elderly populations. Fam. Community Health 1988, 11, 42–52. [Google Scholar] [CrossRef]
- Power, M.; Quinn, K.; Schmidt, S.; Group, W.-O. Development of the WHOQOL-old module. Qual. Life Res. 2005, 14, 2197–2214. [Google Scholar] [CrossRef] [PubMed]
- Kadıoglu, H.; Yıldız, A. Validity and Reliability of Turkish Version of Perception of Health Scale. Türkiye Klinikleri. Tip Bilim. Derg. 2012, 32, 47. [Google Scholar]
- Demir Erbil, D.; Hazer, O.Y.A. Adaptation of “Lubben Social Network Scale-6 (LSSAS-6)” to Turkish Culture: Validity and Reliability Study. Soc. Ment. Res. Think. J. 2020, 6, 399–410. [Google Scholar]
- Eser, S.; Saatli, G.; Eser, E.; Baydur, H.; Fıdaner, C. The Reliability and Validity of the Turkish Version of the World Health Organization Quality of Life Instrument-Older adults Module (WHOQOL-Old). Turk. J. Psychiatry 2010, 21, 37–48. [Google Scholar]
- Bayram, N. Introduction to Structural Equation Modeling AMOS Applications; Ezgi Kitabevi: Isparta, Turkey, 2010. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Ward, M.; McGarrigle, C.A.; Kenny, R.A. More than health: Quality of life trajectories among older adults—Findings from The Irish Longitudinal Study of Ageing (TILDA). Qual. Life Res. 2019, 28, 429–439. [Google Scholar] [CrossRef]
- Keidser, G.; Seeto, M. The influence of social interaction and physical health on the association between hearing and depression with age and gender. Trends Hear. 2017, 21, 2331216517706395. [Google Scholar] [CrossRef] [PubMed]
- Santini, Z.I.; Koyanagi, A.; Tyrovolas, S.; Haro, J.M.; Fiori, K.L.; Uwakwa, R.; Thiyagarajan, J.A.; Webber, M.; Prince, M.; Prina, A.M. Social network typologies and mortality risk among older people in China, India, and Latin America: A 10/66 Dementia Research Group population-based cohort study. Soc. Sci. Med. 2015, 147, 134–143. [Google Scholar] [CrossRef]
- Park, N.S.; Jang, Y.; Chiriboga, D.A.; Chung, S. Social network types, health, and well-being of older Asian Americans. Aging Ment. Health 2019, 23, 1569–1577. [Google Scholar] [CrossRef]
- Condello, G.; Capranica, L.; Stager, J.; Forte, R.; Falbo, S.; Di Baldassarre, A.; Segura-Garcia, C.; Pesce, C. Physical activity and health perception in aging: Do body mass and satisfaction matter? A three-path mediated link. PLoS ONE 2016, 11, e0160805. [Google Scholar] [CrossRef]
- Ciaccioni, S.; Pesce, C.; Forte, R.; Presta, V.; Di Baldassarre, A.; Capranica, L.; Condello, G. The Interlink among age, functional fitness, and perception of Health and quality of life: A mediation analysis. Int. J. Environ. Res. Public Health 2022, 19, 6850. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | Total Participants (N = 327) | |
|---|---|---|
| Age (years) | 65–74 | 258 (78.9%) |
| 75–84 | 52 (15.9%) | |
| 85+ | 17 (5.2%) | |
| Gender | Male | 162 (49.5%) |
| Female | 165 (50.5%) | |
| Marital Status | Married | 295 (90.2) |
| Widowed/divorced/separated | 30 (9.2%) | |
| Single (never married) | 2 (0.6%) | |
| Educational Level | No formal education | 57 (17.4%) |
| Primary school | 213 (65.1%) | |
| Secondary school | 51 (15.6%) | |
| Higher education | 6 (1.8%) | |
| Living Arrangement | Alone | 26(8.0%) |
| With spouse | 272 (83.2%) | |
| With spouse and children | 16 (4.9%) | |
| With children | 8 (2.4%) | |
| Other (relatives, nursing home) | 5 (1.5) | |
| Employed | 18 (5.5%) | |
| Employment Status | Retired | 217 (66.4) |
| Unemployed | 92 (28.1%) | |
| Low | 2 (0.6%) | |
| Income Level | Medium | 188 (57.5%) |
| High | 137 (41.9%) | |
| Chronic Conditions (number of conditions) | 0 | 34 (10.4%) |
| 1–2 | 268 (82.0%) | |
| 3–4 | 25 (7.6%) | |
| Use of Assistive Devices | No | 133 (40.7%) |
| Yes | 194 (59.3%) |
| Variables | X | SD | Skewness | Kurtosis | 1 | 2 | 3 | Cronbach’s |
|---|---|---|---|---|---|---|---|---|
| 1. PHS | 46.32 | 3.4 | 0.242 | 0.334 | 1 | 0.023 | 0.128 * | 0.74 |
| 2. WHOQOL-OLD | 74.50 | 7.6 | −0.324 | 1056 | 1 | 0.198 ** | 0.80 | |
| 3. LSNS-6 | 16.43 | 4.2 | −0.372 | 0.620 | 1 | 0.73 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durmuş Sarıkahya, S.; Terzi, A.; Kanbay, Y.; Çınar Özbay, S. The Mediating Effect of Social Networks on the Impact of Health Perceptions on the Quality of Life in Older Adults. Healthcare 2025, 13, 122. https://doi.org/10.3390/healthcare13020122
Durmuş Sarıkahya S, Terzi A, Kanbay Y, Çınar Özbay S. The Mediating Effect of Social Networks on the Impact of Health Perceptions on the Quality of Life in Older Adults. Healthcare. 2025; 13(2):122. https://doi.org/10.3390/healthcare13020122
Chicago/Turabian StyleDurmuş Sarıkahya, Selma, Amine Terzi, Yalçın Kanbay, and Sevil Çınar Özbay. 2025. "The Mediating Effect of Social Networks on the Impact of Health Perceptions on the Quality of Life in Older Adults" Healthcare 13, no. 2: 122. https://doi.org/10.3390/healthcare13020122
APA StyleDurmuş Sarıkahya, S., Terzi, A., Kanbay, Y., & Çınar Özbay, S. (2025). The Mediating Effect of Social Networks on the Impact of Health Perceptions on the Quality of Life in Older Adults. Healthcare, 13(2), 122. https://doi.org/10.3390/healthcare13020122