Abstract
Background/Objectives: Engaging in regular physical activity (PA) and reducing sedentary behaviors benefits youth health, especially for those with disabilities. However, two-thirds of European children remain insufficiently active. In schools, Active Breaks, brief 5–15 min PA sessions led by teachers during or between lessons, offer a feasible strategy to increase movement. This study investigated teachers’ perceptions of ABs by comparing implementers and non-implementers, examining facilitators and barriers to implementation, and exploring their potential to support the inclusion of students with disabilities. Methods: An observational cross-sectional study was conducted among primary and secondary school teachers in the Emilia-Romagna region (Italy), all of whom had completed a 6 h training course on the implementation of ABs. Data were collected using an ad hoc questionnaire consisting of four sections: sociodemographic data, an adapted Attitudes Toward Physical Activity scale, ABs’ practicality/sustainability, and inclusiveness. Results: Overall, 65% of teachers reported implementing ABs, with higher adoption in primary (69.5%) than secondary schools (58.6%). Implementers reported more positive perceptions and attitudes across individual, classroom, and school-support domains (p < 0.05). In addition, primary teachers consistently scored higher than their secondary counterparts, particularly in terms of class characteristics and benefit perceptions (p < 0.001). Most teachers, especially in primary schools (84.2%), reported no difficulties, although one-third of secondary teachers reported challenges. Exploratory factor analysis on barrier items identified two dimensions (practical/logistical feasibility; institutional/procedural difficulties), but internal consistency was low. Teachers mainly reported using motor activities, with sessions lasting 5–10 min, typically scheduled mid-morning. Inclusion analysis revealed that 60% of teachers had students with disabilities in their classes. While most students participated without adjustments, 25% required occasional or consistent modifications. Conclusions: ABs are a practical and inclusive strategy to reduce SBs in schools. However, not all teachers are currently able to implement them, due to varying contextual constraints, levels of support, and perceived barriers. Primary school settings appear more conducive to their integration, whereas secondary schools may require more tailored support. Fostering teacher confidence, peer collaboration, and inclusive planning can enhance both the implementation and long-term sustainability of educational initiatives.
1. Introduction
Engaging in regular physical activity (PA) and reducing sedentary behaviors (SBs) are widely recognized as beneficial for the physical and mental health of children and adolescents [1,2], especially for those with disabilities [3,4]. Specifically, PA offers advantages across multiple health domains, including improved physical fitness (cardiorespiratory and muscular fitness), enhanced cardiometabolic health (blood pressure, dyslipidemia, glucose regulation, and insulin sensitivity), stronger bone health, better cognitive outcomes (academic performance and executive function), improved mental health (reduced symptoms of depression), and decreased adiposity [1,5]. Conversely, higher levels of SB in this population are associated with adverse health outcomes, such as increased adiposity, poorer cardiometabolic health and fitness, reduced sleep duration, and negative impacts on behavioral regulation and prosocial functioning [5].
Alarmingly, two-thirds of European children and adolescents are not sufficiently active, with a clear trend of lower activity levels in Southern compared to Northern regions [6]. This highlights the need for policymakers, governments, and stakeholders at both local and national levels to implement structural and political changes to promote PA and reduce SB among European youth [6]. Although SBs and physical inactivity are sometimes used interchangeably, they are distinct constructs that are necessarily correlated, and both carry significant health risks [7,8]. Physical inactivity, defined as not achieving the recommended average of 60 min per day of moderate-to-vigorous intensity physical activity for children and adolescents aged 5–17 years, has often been referred to as a 21st-century epidemic [9,10,11]. By contrast, SBs refer to any waking behavior characterized by an energy expenditure ≤ 1.5 metabolic equivalents (METs), while in a sitting, reclining, or lying posture, such as TV viewing, video game playing, computer use (collectively termed “screen time”), or sitting in a car [12]. Identifying opportunities for children and adolescents to achieve the recommended 60 min of moderate-to-vigorous PA daily is crucial for enhancing fitness, developing movement skills, and preventing chronic diseases [13]. These challenges are even more pronounced among children with disabilities (e.g., intellectual and/or physical), who often fail to achieve sufficient PA, accumulate most of their activity at school, and show limited moderate-to-vigorous physical activity (MVPA) during physical education and recess [14,15]. High levels of overweight and obesity, poorer motor skills, and reduced participation in structured activities further hinder their engagement in PA [3,16,17]. Similarly, children with autism spectrum disorder (ASD) and/or attention-deficit/hyperactivity disorder (ADHD) face additional barriers such as motor coordination, sensory, and attentional difficulties, which contribute to higher SB and lower PA levels [18,19,20].
Schools play a key role in promoting health by interrupting SBs and integrating PA into daily routines through before- and after-school programs, physical education classes, and active breaks during recess and lunch [21]. While integrating PA helps to reduce sedentary time, its implementation often competes with academic demands, limiting widespread adoption. Efficient and adaptable strategies are therefore needed to balance these competing priorities and to support the integration of physical activity within the school setting [22,23].
In this regard, School Active Breaks (ABs) have emerged as a practical and effective strategy for incorporating PA into educational settings. ABs are short sessions of PA, typically lasting 5 to 15 min, led by appropriately trained teachers, and conducted during daily educational settings [24]. These short bursts of movement help interrupt prolonged sitting while fitting seamlessly into the curricular schedule [25]. Evidence shows that ABs can increase PA levels, improve classroom behavior (e.g., on-task behavior [26,27,28,29]) and working memory, and encourage a positive attitude toward movement and exercise [30]. Moreover, a recent systematic review indicated that ABs help children and adolescents to rediscover the pleasure of moving and reach the minimum level of PA recommended for health [31,32].
Significantly, the effectiveness of ABs is reinforced by teachers’ positive perceptions [22,33,34]. This favorable outlook underscores the importance of teacher engagement and training in successfully implementing ABs within educational settings. However, previous studies have emphasized that, for ABs to be effective, they must be brief, quick to execute, adaptable to the limited space available in classrooms, and easy to implement without requiring sophisticated equipment [33,35]. When properly designed and implemented, ABs are strongly supported by teachers. ABs are often perceived as a valuable tool for enhancing students’ physical activity, focus, and conflict management in the class within the constraints of the school day [30,36]. Despite these benefits and their importance within the educational community, ABS are still underutilized in schools [30,36]. The potential of ABs may be particularly relevant for children with disabilities, who often face lower PA levels, higher sedentary behavior, and additional barriers to participation compared to their typically developing peers. For example, children with intellectual disabilities (ID) often exhibit deficits in working memory, especially in the phonological loop [37], while children with ASD or ADHD may experience motor coordination, sensory, or attentional difficulties that limit their engagement in PA. In these populations, ABs could serve not only to interrupt sedentary time but also as a supportive educational practice with potential cognitive and social-behavioral benefits [3].
In Italy, the National Prevention Plan 2020–2025 promotes health-enhancing school environments, particularly via the Program “Schools that Promote Health” [38]. Within this framework, the Emilia-Romagna region has identified a list of recommended practices for schools promoting health, including ABs, as practical tools to counteract sedentary behavior in children and adolescents. While previous literature supports the positive effects of ABs, questions remain regarding the facilitators and barriers that influence teachers’ decisions to implement these breaks. Further research is needed to understand the factors that shape teachers’ ability and willingness to adopt ABs. Identifying these factors could foster greater acceptance among teachers and stakeholders, leading to more widespread adoption.
The present study aims to explore how teachers across different school levels perceive the role of ABs in terms of their benefits, facilitators, and barriers, by comparing implementers and non-implementers. It also investigates the potential of ABs to support the inclusion of pupils with disabilities. The findings are intended to inform strategies for effective and sustainable implementation. We hypothesized that teachers would generally view ABs as beneficial and feasible within the school environment. However, secondary school teachers might face greater challenges in implementation compared to primary school teachers. Additionally, we anticipated the identification of specific barriers that could affect the applicability and sustainability of ABs, and we expected ABs to emerge as a supportive practice for fostering more inclusive educational settings for students with disabilities.
2. Materials and Methods
2.1. Sampling
A total of 481 teachers (447 females) were recruited across different school grades. Of the full sample, 300 teachers (293 females) worked in primary schools, and 181 (154 females) in secondary schools (middle and high school combined). Participants taught a variety of subjects, including mathematics, sciences, geography, chemistry, and informatics.
Teachers expressed their willingness to participate by contacting their school managers and subsequently attending a 6 h training program on implementing ABs. The training was delivered in one session of six hours each and systematically integrated theoretical foundations with practical application. The first part introduced the scientific rationale and benefits of ABs, providing participants with principles and guidance for their implementation The second was dedicated to hands-on practice, with instructors modeling simple, adaptable strategies to foster teachers’ skill-building, confidence, and self-efficacy. Following the training phase, each school formally agreed to participate in the project. Teachers were asked to implement ABs at least three times per day in each class, with complete discretion over content, timing, and pedagogical style. These elements were intentionally kept flexible to allow adaptation to class context, student needs, and time constraints.
2.2. Study Design
The study was an observational cross-sectional study conducted in accordance with the Survey Reporting Guideline (SURGE, [39]). Local Emilia-Romagna health agencies organized the training sessions by coordinating with school managers. The survey was conducted 3 to 6 months after the training session, allowing teachers sufficient time to decide whether to implement and integrate ABs in their classrooms.
Data collection was carried out via a census between 1 May 2024, and 31 July 2024. Participation in the survey was voluntary and pseudo-anonymous. Respondents were informed about the study’s objectives and provided informed consent prior to participation. No directly identifying information was collected, and unique codes were used to protect individual identities while allowing linkage of responses. This approach enhanced data reliability for sensitive topics while ensuring participant confidentiality [40]. Consent to participate was obtained in electronic format before survey administration. Participants had to read, understand, and accept all the information reported on the introduction page of the online survey.
The study was approved by the Ethics Committee of the University of Bologna (Ref. 0126773, 7 May 2024) and conducted in accordance with the Declaration of Helsinki.
2.3. Survey Questionnaire and Administration
The questionnaire named “The schools promoting health through ABs: teachers’ perceptions” was developed ad hoc with items organized into five sections:
- Teacher sociodemographic characteristics (4 items collecting data such as gender, teaching role, years of experience, and school level).
- Adapted version of the Attitudes Towards Physical Activity (ATPA) questionnaire evaluating teachers’ perceptions and attitudes toward ABs (11 items) and additional items assessing potential barriers (8 items) [41,42].
- Practicability, applicability, sustainability of ABs (9 items) and perceived benefits experienced during their use (7 items).
- Inclusion and disability (3 items, including those with special educational needs or diverse abilities).
Section 1 and Section 2 were completed by all teachers, including both implementers and non-implementers of ABs. Section 3 and Section 4 were specifically designed for teachers who had implemented ABs in the classroom. The items were selected through a critical review of the literature to define the specific items of each section [21,41,43]. After the initial development, cognitive interviews were conducted with a subsample of teachers to verify the clarity and interpretation of the item [44]. Based on their feedback, some items were revised to improve comprehension. The survey included multiple-choice questions rated on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree).
The survey was promoted via email through Local health agencies and School representatives of the Emilia-Romagna region (Italy) and was administered using a dedicated online survey platform. This survey was accessible from both mobile devices and computers. A designated researcher monitored data collection and maintained access to the anonymized dataset. The study respected the anonymity and privacy of data in accordance with the General Data Protection Regulation (GDPR Regulation EU 2016/679) [45]. Answers were anonymized, and IP addresses were not visible to the researcher.
2.4. Statistical Analysis
Data were analyzed using R (v. 4.5.1) through the RStudio platform (v. 2025.09.0+38). Descriptive statistics were computed to summarize the variables. Dichotomous and categorical data were presented as frequencies and percentages, whereas continuous variables were expressed as means and standard deviations.
For the questionnaire data, items were grouped according to the three main sections of the survey. The internal consistency of each section was assessed using Cronbach’s α, which evaluates how consistently the items within a section measure the same construct.
Items related to barriers were examined through an exploratory factor analysis (EFA) to identify potential latent variables. Composite scores for each section were then computed by summing the respective items.
Linear mixed-effects models, suitable for non-parametric data (using the ARToolpackage, v. 0.11.2), were used to analyze associations. Data normality was assessed using the Shapiro–Wilk test. Independent variables of the models were “school grade” (primary vs. secondary) and the “implementation of ABs” (ABs; Implementers vs. Non-Implementers). When appropriate, post hoc analyses with Tukey corrections were conducted using the emmeans package (v. 1.11.2-8). Results are reported as F values with associated degrees of freedom, F(df1, df2), where df1 represents the numerator degrees of freedom and df2 the denominator degrees of freedom.
3. Results
3.1. Sociodemographic Characteristics
Of the 481 teachers who completed the training, 140 completed the questionnaire, and five refused to sign the consent form (Figure 1). Therefore, the present analysis is based on a subsample of 140 teachers. The characteristics of teachers are shown in Table 1.
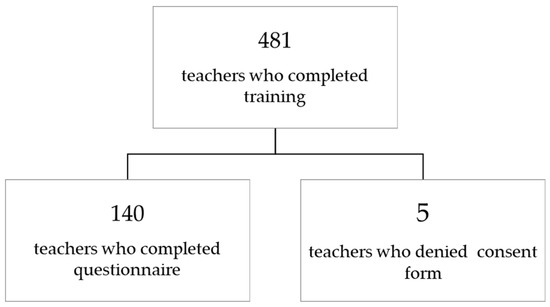
Figure 1.
Participant flow diagram.

Table 1.
Characteristics of teachers.
Although the response rate in the present study was approximately 30%, this value is within the acceptable range reported in educational and organizational research, where typical rates range from 34% to 53% [46].
3.2. Teacher ABs Implementation
Ninety-one teachers (65%) reported implementing ABs during the school year. Specifically, 57 (69.5%) primary school teachers stated they regularly integrated ABs into their teaching practice, compared to 34 (58.6%) secondary school teachers. Despite these encouraging numbers, a non-negligible portion of teachers reported not implementing ABs (see Figure A1 in Appendix A).
3.2.1. Teachers’ Perceptions and Attitudes Toward ABs in the Classroom
Cronbach’s α for the Individual Perception variable was 0.91. The linear regression indicated that the AB factor was significant (F(1,136) = 41.78, p < 0.001, ƞ2 = 0.24). A higher score for Implementers compared to Non-Implementers was found (see Table 2). The “school grade” factor was also significant (F(1,136) = 8.83, p = 0.004, ƞ2 = 0.06) with primary school teachers reporting higher scores than secondary school teachers (M = 16.15, SD = 3.40 vs. M = 15.22, SD = 2.58 points). Interaction “ABs” × “school grade” was non-significant (F(1,136) = 0.17, p > 0.05, ƞ2 = 0.00).
Table 2.
Teacher perceptions and attitudes.
Cronbach’s α for the Class Characteristics variable was 0.79. Linear regression indicated the “ABs” factor was significant (F(1,136) = 35.35, p < 0.001, ƞ2 = 0.21), with a higher score for Implementers compared to Non-implementers (Table 2). “School grade” factor was also significant (F(1,136) = 18.26, p > 0.001, ƞ2 = 0.12). The score was higher for primary school teachers than for secondary school teachers (M = 11.72, SD = 2.22 vs. M = 10.52, SD = 1.95 points). The interaction “ABs” × “school grade” was nonsignificant (F(1,136) = 0.27, p > 0.05, ƞ2 = 0.00) see Figure 2.
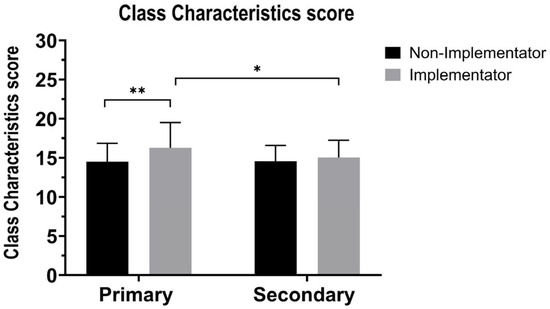
Figure 2.
Class characteristics scores in primary and secondary classes for Implementers (gray bars) and Non-Implementers (black bars). Y-axis: class characteristics score; X-axis: school level. Class characteristics scores were calculated as the sum of responses within the domain. Mean (±SD) values are shown for Primary vs. Secondary students and for Implementors vs. Non-Implementors. Significant differences are indicated as follows: * p < 0.05; ** p < 0.01.
Cronbach’s α for the Supporting the School Education variable was 0.88. Linear regression highlighted that the “ABs” factor was significant (F(1,136) = 9.16, p = 0.003, ƞ2 = 0.06). Analysis showed that Implementers had a higher score compared to Non-implementers (Table 2). The “School grade” factor was also significant (F(1,136) = 5.39, p > 0.001, ƞ2 = 0.04). Primary school teachers had a higher score than secondary school teachers (M = 15.75, SD = 3.07 vs. M = 14.86, SD = 2.13 points). The interaction “ABs” × “school grade” was significant (F(1,136) = 3.93, p > 0.04, ƞ2 = 0.03). Post hoc analyses revealed a significant difference between the primary school teachers who did not implement ABs and the primary school teachers who implemented ABs (t(136) = 3.55, p = 0.003, d = 0.61). No significant difference was observed between the primary school teachers who did not implement ABs and the secondary school teachers who did not implement ABs (t(136) = 0.07, p > 0.05, d = 0.01) or between the Non-Implementer primary school teachers and the Implementer secondary school teachers (t(136) = 0.72, p > 0.05, d = 0.12). No significant difference was found between Implementers and Non-Implementers of secondary school (t(136) = 0.79, p > 0.05, d = 0.14).
3.2.2. Perceived Difficulties and Barriers to ABs
The analysis of perceived difficulties in implementing ABs revealed differences between primary and secondary school teachers. Most primary teachers reported no difficulties (84.2%), compared with 64.7% of secondary teachers, among whom 35.3% experienced challenges (Figure 3).
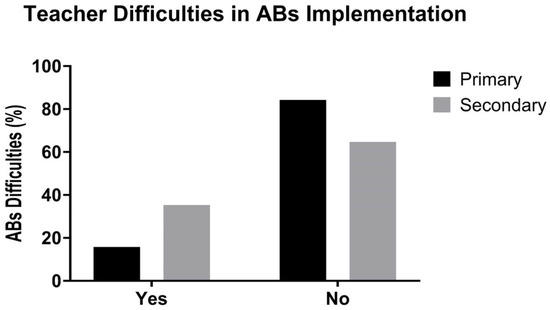
Figure 3.
Teacher difficulties in ABs implementation in Primary (black bars) and Secondary (gray bars) schools. The y-axis represents the percentage of teachers reporting difficulties with ABs implementation, while the x-axis indicates whether teachers reported experiencing difficulties (Yes vs. No). Data are reported as percentages.
Items related to barriers associated with the implementation of ABs; an EFA was conducted on the six items assessing barriers to the implementation of ABs (Table 3). The internal consistency of the items was low (Cronbach’s α = 0.35), and the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy indicated a poor overall fit (KMO = 0.56), although all individual Measure of Sampling Adequacy values were above the 0.50 threshold. Bartlett’s test of sphericity was significant (χ2(15) = 97.11, p < 0.001), indicating that the correlation matrix was suitable for factor analysis. Parallel analysis suggested the extraction of two factors. The two-factor model with varimax rotation showed good model fit (χ2(4) = 1.21, p = 0.877) and accounted for 45% of the total variance (Factor 1 = 28%; Factor 2 = 17%). Factor 1 was strongly defined by BARR3 (0.82) and BARR7 (1.00), whereas Factor 2 was characterized by BARR6 (0.67), BARR2 (0.48), and BARR5 (–0.47), with BARR1 showing a weaker loading (0.31). The uniqueness values indicated that BARR1 (0.90) and BARR5 (0.78) contributed less to the overall factor structure. Overall, these results suggest a two-factor solution, reflecting practical/logistical feasibility and institutional/procedural challenges as the main latent dimensions of perceived barriers. However, the relatively low internal consistency highlights the need to refine and validate the barrier items in future research, possibly by clarifying wording or developing additional items to strengthen each dimension.
Table 3.
Teacher barriers.
Cronbach’s α for Factor 1 was 0.90. The linear regressions did not highlight any significant differences for all the factors and the possible interaction (F < 2.95, p > 0.05). Cronbach’s α for Factor 2 was 0.04, and the linear regressions did not highlight any significant differences for all the factors and the possible interaction (F < 0.55, p > 0.05).
3.3. Practicability, Benefits, Applicability, and Sustainability of ABs in the Classroom
The profile of teachers who implemented ABs varied between primary and secondary school levels (see Table A1 in Appendix A). Among primary school teachers, 44 (77.19%) reported “Definitely Yes” about whether they were comfortable suggesting ABs, compared to 24 (70.59%) secondary school teachers. In contrast, only 1 (1.75%) primary school teacher indicated discomfort (i.e., “More NO than YES”), compared to 2 (5.88%) at the secondary level. Winter (December–February) was the most common starting period for ABs in both groups, reported by 23 teachers in each group (40.35% of primary and 67.65% of secondary teachers). Among primary school teachers, 29 (50.88%) performed ABs a few times a week, while 11 (19.30%) reported doing so several times a day and 12 (21.05%) once daily. In contrast, among secondary school teachers, 22 (64.71%) reported performing ABs a few times a week, and only 5 (14.71%) managed to conduct them once a day. Regarding duration, 34 (59.65%) of primary school teachers and 14 (41.18%) of secondary school teachers reported that ABs typically lasted 10 min, followed by 5 min sessions, reported by 20 (35.09%) and 15 (44.12%) teachers, respectively. Teachers identified mid-morning as the most helpful time for ABs, with 25 (43.86%) primary and 26 (76.47%) secondary teachers selecting this period. In terms of content, “Motor” activities were the most frequently used in both groups: 39 (68.42%) in primary and 23 (67.65%) in secondary. Mixed content was used by 14 (24.56%) primary and 6 (17.65%) secondary teachers, while cognitive content was used exclusively in secondary schools by two teachers (5.88%). Leadership of ABs was most commonly assumed by the teacher, with 38 (66.67%) primary and 14 (41.18%) secondary school teachers leading the breaks. However, secondary schools involved pupils more frequently, with 8 (23.53%) ABs led entirely by students and 9 (26.47%) co-led by teachers and students. The use of digital tools, particularly interactive whiteboards, was limited. Among primary school teachers, 8 (14.04%) reported using the interactive whiteboard during ABs, compared to 6 (17.65%) of secondary teachers. YouTube was the most used application, cited by four teachers in primary (7.02%) and six in secondary (17.65%), followed by “mixed tools” (7.02% and 5.88%, respectively). These findings highlight some differences between school levels in terms of frequency, modality, leadership, and technological support for ABs, with greater challenges and variability reported in secondary school settings.
Cronbach’s α for the teachers’ perceptions of the benefit of ABs was 0.92. Linear regression showed that “school grade” factor was significant (F(1,89) = 13.73, p < 0.001, ƞ2 = 0.13), highlighting a higher score for primary school teachers compared to secondary school teachers (Figure 4 and Table 4).
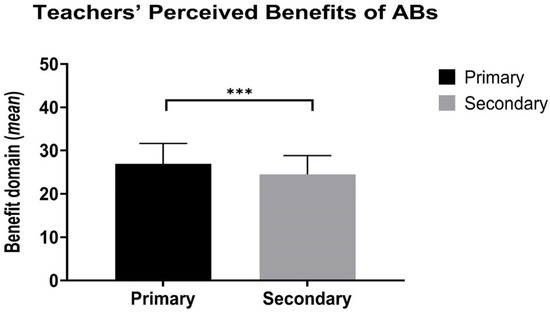
Figure 4.
Teachers’ perceived benefits of ABs in Primary (black bars) and Secondary (gray bars) schools. The y-axis represents the mean score of perceived benefits, while the x-axis indicates school level (Primary vs. Secondary). Data are reported as mean values of the benefit domain score (±standard deviation). Significant differences are marked as follows: *** p < 0.001.
Table 4.
Teachers’ perceptions of the benefits of ABs.
3.4. Inclusion and Disability
The survey revealed that the majority of teachers had students with disabilities in their classrooms, with 34 (59.65%) primary school teachers and 22 (64.71%) secondary school teachers confirming their presence (see Table A2 in Appendix A). A small proportion of respondents preferred not to disclose this information (5.26% in primary and 5.88% in secondary schools). Among those who specified the type of disability, cognitive disabilities were the most frequently reported, noted by 27 (47.37%) primary and 15 (44.12%) secondary school teachers. Physical disabilities were reported by 2 (5.88%) teachers in secondary schools only, while sensory disabilities were mentioned by 2 (3.51%) primary school teachers. Combined disabilities, such as cognitive and physical, were reported by one teacher in each school level (1.75% in primary and 2.94% in secondary), whereas cognitive and sensory disabilities were reported by 2 (3.51%) teachers in primary school only. A small group of respondents (3.51% primary and 11.76% secondary) preferred not to specify the type of disability. Regarding the need to adjust the timing, rhythms, or scheduling of ABs to meet the needs of students with disabilities, responses were varied. In primary schools, 11 teachers (32.25%) reported that adjustments were never needed, while 10 (29.41%) indicated that they were sometimes required. Smaller proportions reported adjusting almost never (23.53%), always (11.76%), or rarely (2.94%). In secondary schools, 10 teachers (45.45%) stated that no adjustments were needed, 6 (27.27%) reported adjusting sometimes, and only 2 (9.09%) indicated constantly adjusting ABs. The responses “almost never” and “rarely” were each selected by two secondary teachers (9.09%). These findings highlight the relevance of inclusive planning when designing and implementing active breaks. Although the need for adjustments was not universal, a non-negligible proportion of teachers reported modifying ABs to support students with disabilities, underscoring the importance of flexibility and responsiveness in school-based physical activity interventions.
4. Discussion
This study examined the relationship between teachers’ self-reported implementation of ABs, their perceptions and attitudes, perceived barriers and benefits, and school levels, in order to identify strategies that support effective and sustainable adoption.
The sociodemographic profile of the sample offers insights into the profile of teachers engaged in ABs. The predominance of female respondents, typical in the Italian school system due to the high proportion of female teachers, reflects demographic trends observed in previous European studies, where teaching staff is often predominantly female and highly experienced [47,48]. These characteristics may influence attitudes and practices related to the promotion of PA in the classroom.
Our analysis revealed important differences in AB implementation between primary and secondary school teachers. While the majority of teachers reported integrating ABs into their teaching routines, implementation rates were higher in primary schools. This pattern suggests that curriculum flexibility and pedagogical approaches may facilitate integration at this educational level. Primary school curricula often emphasize holistic child development, incorporating PA and playing embedded in daily learning experiences [48]. In contrast, secondary school teachers reported greater challenges, likely due to subject-specific instructional demands, time-stricter lesson schedules, and limited curricular flexibility [49,50].
Perceptions, attitudes, beliefs, and self-efficacy regarding ABs implementation, assessed through a modified version of the ATPA [41,42], showed that teachers who implemented ABs reported more positive perceptions and attitudes across individual, classroom, and school support domains. This finding suggests a possible increase in self-efficacy and the perceived feasibility of applying ABs in everyday teaching practice [25,50,51], corroborating previous evidence that teacher confidence and motivation are critical facilitators of classroom-based physical activity interventions [48,52]. Classroom-level factors, such as students’ behavior and perceived time availability, also influenced the implementation of ABs, in line with literature identifying classroom management and time constraints as recurrent determinants of PA adoption [53]. Notably, primary school teachers consistently scored higher across domains than secondary school teachers, reinforcing the idea that contextual and organizational differences strongly shape implementation feasibility.
The last social–ecological dimension of school support further emerged as a key facilitator. Teachers who perceived strong institutional and peer support were more likely to adopt ABs, supporting previous findings that highlight the importance of leadership and school culture in sustaining classroom-based practices [22,33].
Despite these generally favorable perceptions, some barriers were reported. Most primary school teachers described few or no difficulties, whereas more than one-third of secondary teachers perceived challenges, reflecting the contextual differences between the two educational levels. Exploratory factor analysis of the barrier items indicated two main dimensions: practical/logistical feasibility (e.g., space, materials, class size, and time) and institutional/procedural challenges (e.g., bureaucracy, training, and organizational support). Although the internal consistency of the barrier scale was low, these categories align with established literature that identifies a lack of time, limited space, and classroom management as common barriers [35,53]. Interestingly, in our sample, perceptions of training adequacy did not differ between implementers and non-implementers, suggesting that the training provided may have equipped teachers with sufficient knowledge and confidence to deliver ABs effectively.
Overall, teachers perceived ABs as feasible and beneficial in classroom practice, although implementation patterns varied between primary and secondary schools. Primary school teachers tended to deliver ABs more frequently, whereas secondary school teachers provided shorter and less frequent sessions, likely constrained by organizational and time-related factors. Across both levels, motor-based activities were the most frequently adopted, indicating a preference for simple movement tasks over cognitively integrated ones. Interestingly, secondary schools more often involve students in leading ABs, a strategy that may enhance engagement and sustainability in older age groups [50]. Benefit scores were significantly higher among primary school teachers, reinforcing the notion that primary education contexts are more conducive to the integration of ABs.
The potential of ABs as an inclusive practice also emerged as a key finding. Students with disabilities typically engage in lower levels of PA during school hours [54]. ABs can help address this gap by offering accessible opportunities for movement. Previous research, such as that conducted by Mazzoli et al. [3], has shown that ABs can provide moderate cognitive benefits and reduce sedentary behavior among students with intellectual disabilities, while also highlighting potential challenges, such as overstimulation in students with ASD. These findings underscore the importance of teacher training and tailored support, including the use of visual aids and adapted instructional strategies.
Our survey further confirmed the potential of ABs for inclusion. A substantial proportion of teachers reported having students with disabilities in their classes (59.65% in primary and 64.71% in secondary schools), primarily with cognitive impairments. While some students participated without adjustments (19.30% in primary, 29.41% in secondary), others required occasional (17.5%) or consistent (7%) modifications. In many secondary schools, the presence of physical education teachers with a degree in Sports Science may have facilitated adaptation. These findings suggest the importance of a flexible, tailored approach to ensure ABs are accessible to all students. While cognitively demanding motor tasks can enhance engagement among typically developing students, they may pose challenges for students with neurodevelopmental disorders [55]. This emphasized the need for balanced task design, guided instructions, adapted equipment, and peer-assisted activities [55,56]. By ensuring that ABs accommodate diverse needs, schools can foster more inclusive environments, promote PA, and reduce disparities in movement opportunities and health outcomes [56]. This aligns with broader educational equity goals and supports the development of healthier, more inclusive school cultures. Research on the intersection of ABs and inclusivity remains limited, and our findings provide valuable new perspectives. While ABs can foster inclusion and cognitive engagement, their effectiveness depends heavily on thoughtful design and implementation. Future studies should incorporate qualitative and observational approaches to better understand the real-world adaptability of ABs and to develop evidence-based strategies that maximize accessibility and engagement for all students.
Several limitations of this study should be acknowledged. The relatively low response rate, influenced by formal recruitment and distribution procedures, may limit the generalizability of the findings. The self-reported nature of the data could also introduce response bias, as perceptions and reported practices may not fully reflect actual implementation. Additionally, although preliminary analyses supported the reliability of the questionnaire (e.g., internal consistency and exploratory factor analysis), the tool has not been fully validated and should be refined in future research. Finally, the cross-sectional design captures only a snapshot of teachers’ practices and perceptions, precluding conclusions about longitudinal trends or causal relationships. Future research should employ representative, longitudinal designs, validate the questionnaire through robust psychometric testing, and examine contextual factors that influence the adoption and sustainability of ABs.
5. Conclusions
ABs represent a promising and accessible strategy to foster PA, cognitive engagement, and inclusion within school settings. When thoughtfully designed and adequately supported, ABs can offer significant benefits for all students, particularly those with disabilities, by promoting participation, reducing sedentary behavior, and enhancing classroom learning environments. To unlock their full potential, comprehensive teacher training, strong institutional commitment, and inclusive, adaptable implementation strategies are essential across all educational levels.
Author Contributions
Conceptualization: L.D.; methodology: A.C., A.M., R.S. and M.P.; formal analysis: M.P. and G.R.; data curation: G.R.; investigation: G.R., G.S. and L.B.; writing—original draft preparation: M.P.; supervision: L.D., A.C., R.S. and A.M.; project administration: R.S. and A.M.; funding acquisition: M.M. and A.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study received financial support from the Local Health Agency of Romagna (ID: 1129 –21/21/2023). One of the authors is employed by the same agency. No other external funding was received for this work.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Bologna (Ref. 0126773, 7 May 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are not publicly available due to privacy or ethical restrictions. Data may be available from the corresponding author upon reasonable request and subject to approval by the relevant ethics committee.
Conflicts of Interest
One author reports that financial support for this study was provided by a local health agency. Another author reports on an employment relationship with the same agency. All other authors declare that they have no known competing financial interest or personal relationships that could have appeared to influence the work reported in this study.
Abbreviations
The following abbreviations are used in this manuscript:
| ABs | Active Breaks |
| ASD | Autism Spectrum Disorder |
| ATPA | Attitudes Towards Physical Activity |
| EFA | Exploratory Factor Analysis |
| GDPR | General Data Protection Regulation |
| IPAQ | International Physical Activity Questionnaire |
| KMO | Kaiser–Meyer–Olkin |
| METs | Metabolic Equivalents |
| PA | Physical Activity |
| SBs | Sedentary Behavior |
| SURGE | Survey Reporting Guideline |
Appendix A

Figure A1.
Implementation of ABs by teachers. Percentage of primary and secondary school teachers who implemented active breaks (ABs) during the school year.
Table A1.
Teachers’ perceptions of the practicality, benefits, applicability and sustainability of ABs.
Table A1.
Teachers’ perceptions of the practicality, benefits, applicability and sustainability of ABs.
| Primary (N = 57) | Secondary (N = 34) | |||
|---|---|---|---|---|
| Did you feel comfortable suggesting active breaks? | N. | % | N. | % |
| Definitely YES | 44 | 77.19 | 24 | 70.59 |
| More YES than NO | 12 | 21.05 | 8 | 23.53 |
| More NO than YES | 1 | 1.75 | 2 | 5.88 |
| In which month did you start performing active breaks? | ||||
| Autumn (September–November) | 19 | 33.33 | 4 | 11.76 |
| Winter (December–January–February) | 23 | 40.35 | 23 | 67.65 |
| Spring (March–April–May) | 15 | 26.32 | 7 | 20.59 |
| How often did you perform active breaks? | ||||
| A few times a week | 29 | 50.88 | 22 | 64.71 |
| A few times a month | 5 | 8.77 | 7 | 20.59 |
| Every day once a day | 12 | 21.05 | 5 | 14.71 |
| Every day several times a day | 11 | 19.30 | 0 | 0.00 |
| How long does an active break usually last? | ||||
| 15 min | 2 | 3.51 | 1 | 2.94 |
| 10 min | 34 | 59.65 | 14 | 41.18 |
| 5 min | 20 | 35.09 | 15 | 44.12 |
| Others | 1 | 1.75 | 4 | 11.76 |
| At what time of the school day is the active break most useful? | ||||
| Early morning | 16 | 28.07 | 4 | 11.76 |
| Midmorning | 25 | 43.86 | 26 | 76.47 |
| After lunch break | 6 | 10.53 | 0 | 0.00 |
| Afternoon | 8 | 14.04 | 0 | 0.00 |
| Other | 2 | 3.51 | 4 | 11.76 |
| What type of content did you use most frequently in active breaks? | ||||
| Cognitive | 0 | 0.00 | 2 | 5.88 |
| Disciplinary | 3 | 5.26 | 1 | 2.94 |
| Motor | 39 | 68.42 | 23 | 67.65 |
| Relational | 1 | 1.75 | 2 | 5.88 |
| Mixed Content | 14 | 24.56 | 6 | 17.65 |
| Who led the active breaks? | ||||
| Teacher | 38 | 66.67 | 14 | 41.18 |
| Expert on educational project | 1 | 1.75 | 0 | 0.00 |
| Pupils | 0 | 0.00 | 8 | 23.53 |
| Special needs teacher | 5 | 8.77 | 1 | 2.94 |
| Teacher and Pupils | 6 | 10.53 | 9 | 26.47 |
| Mixed Figures | 7 | 12.28 | 2 | 5.88 |
| During the active break did you use the interactive whiteboard? | ||||
| No | 49 | 85.96 | 28 | 82.35 |
| Yes | 8 | 14.04 | 6 | 17.65 |
| What digital teaching tools/applications have you used with the interactive whiteboard? * | ||||
| YouTube | 4 | 7.02 | 6 | 17.65 |
| Mixed tools | 4 | 7.02 | 2 | 5.88 |
| None | 49 | 85.96 | 28 | 82.36 |
Number of observations n. and percentage % across school levels. * multiple choice question.
Table A2.
Inclusion and disability.
Table A2.
Inclusion and disability.
| Primary (N = 57) | Secondary (N = 34) | |||
|---|---|---|---|---|
| Were there pupils with disabilities in your class this year? | N. | % | N. | % |
| No | 20 | 35.09 | 10 | 29.41 |
| Yes | 34 | 59.65 | 22 | 64.71 |
| I prefer not to answer | 3 | 5.26 | 2 | 5.88 |
| Teachers who taught pupils with disabilities | (N = 34) | (N = 22) | ||
| Can you specify the type of disability referred to the pupils in your class? * | ||||
| Cognitive | 27 | 79.41 | 15 | 68.18 |
| Physical | 0 | 0 | 2 | 9.09 |
| Sensory | 2 | 5.88 | 0 | 0 |
| Cognitive and Physical | 1 | 2.94 | 1 | 4.55 |
| Cognitive and Sensory | 2 | 5.88 | 0 | 0 |
| I prefer not to answer | 2 | 5.88 | 4 | 18.18 |
| Was it necessary to adjust the timing/rhythms/scheduling of the ABs to meet the needs of the students with disabilities? * | ||||
| Never | 11 | 32.25 | 10 | 45.45 |
| Almost never | 8 | 23.53 | 2 | 9.09 |
| Rarely | 1 | 2.94 | 2 | 9.09 |
| Sometimes | 10 | 29.41 | 6 | 27.27 |
| Always | 4 | 11.76 | 2 | 9.09 |
Number of observations n. and percentage %. Questions * were provided by a subset of participants only.
References
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour, 1st ed.; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-001512-8. [Google Scholar]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic Review of the Relationships between Objectively Measured Physical Activity and Health Indicators in School-Aged Children and Youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Mazzoli, E.; Salmon, J.; Pesce, C.; Teo, W.-P.; Rinehart, N.; May, T.; Barnett, L.M. Effects of Classroom-based Active Breaks on Cognition, Sitting and On-task Behaviour in Children with Intellectual Disability: A Pilot Study. J. Intellect. Disabil. Res. 2021, 65, 464–488. [Google Scholar] [CrossRef] [PubMed]
- Sit, C.; Li, R.; McKenzie, T.L.; Cerin, E.; Wong, S.; Sum, R.; Leung, E. Physical Activity of Children with Physical Disabilities: Associations with Environmental and Behavioral Variables at Home and School. Int. J. Environ. Res. Public Health 2019, 16, 1394. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO Guidelines on Physical Activity and Sedentary Behaviour for Children and Adolescents Aged 5–17 Years: Summary of the Evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- Steene-Johannessen, J.; Hansen, B.H.; Dalene, K.E.; Kolle, E.; Northstone, K.; Møller, N.C.; Grøntved, A.; Wedderkopp, N.; Kriemler, S.; Page, A.S.; et al. Variations in Accelerometry Measured Physical Activity and Sedentary Time across Europe—Harmonized Analyses of 47,497 Children and Adolescents. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Baumann, H.; Fiedler, J.; Wunsch, K.; Woll, A.; Wollesen, B. mHealth Interventions to Reduce Physical Inactivity and Sedentary Behavior in Children and Adolescents: Systematic Review and Meta-Analysis of Randomized Controlled Trials. JMIR mHealth uHealth 2022, 10, e35920. [Google Scholar] [CrossRef]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S.; et al. Systematic Review of Sedentary Behaviour and Health Indicators in School-Aged Children and Youth: An Update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Rivière, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 288. [Google Scholar] [CrossRef]
- Hall, G.; Laddu, D.R.; Phillips, S.A.; Lavie, C.J.; Arena, R. A Tale of Two Pandemics: How Will COVID-19 and Global Trends in Physical Inactivity and Sedentary Behavior Affect One Another? Prog. Cardiovasc. Dis. 2021, 64, 108–110. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Aubert, S.; Barnes, J.D.; Abdeta, C.; Abi Nader, P.; Adeniyi, A.F.; Aguilar-Farias, N.; Andrade Tenesaca, D.S.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis From 49 Countries. J. Phys. Act. Health 2018, 15, S251–S273. [Google Scholar] [CrossRef]
- Einarsson, I.Þ.; Jóhannsson, E.; Daly, D.; Arngrímsson, S.Á. Physical Activity during School and after School among Youth with and without Intellectual Disability. Res. Dev. Disabil. 2016, 56, 60–70. [Google Scholar] [CrossRef]
- Sit, C.H.P.; McManus, A.; McKenzie, T.L.; Lian, J. Physical Activity Levels of Children in Special Schools. Prev. Med. 2007, 45, 424–431. [Google Scholar] [CrossRef]
- Maïano, C. Prevalence and Risk Factors of Overweight and Obesity among Children and Adolescents with Intellectual Disabilities. Obes. Rev. 2011, 12, 189–197. [Google Scholar] [CrossRef]
- Wouters, M.; Evenhuis, H.M.; Hilgenkamp, T.I.M. Physical Fitness of Children and Adolescents with Moderate to Severe Intellectual Disabilities. Disabil. Rehabil. 2020, 42, 2542–2552. [Google Scholar] [CrossRef] [PubMed]
- Levit-Binnun, N.; Davidovitch, M.; Golland, Y. Sensory and Motor Secondary Symptoms as Indicators of Brain Vulnerability. J. Neurodev. Disord. 2013, 5, 26. [Google Scholar] [CrossRef]
- Jones, R.A.; Downing, K.; Rinehart, N.J.; Barnett, L.M.; May, T.; McGillivray, J.A.; Papadopoulos, N.V.; Skouteris, H.; Timperio, A.; Hinkley, T. Physical Activity, Sedentary Behavior and Their Correlates in Children with Autism Spectrum Disorder: A Systematic Review. PLoS ONE 2017, 12, e0172482. [Google Scholar] [CrossRef]
- Tandon, P.S.; Sasser, T.; Gonzalez, E.S.; Whitlock, K.B.; Christakis, D.A.; Stein, M.A. Physical Activity, Screen Time, and Sleep in Children With ADHD. J. Phys. Act. Health 2019, 16, 416–422. [Google Scholar] [CrossRef]
- Macdonald, K.; Milne, N.; Pope, R.; Orr, R. Factors Influencing the Provision of Classroom-Based Physical Activity to Students in the Early Years of Primary School: A Survey of Educators. Early Child. Educ. J. 2021, 49, 361–373. [Google Scholar] [CrossRef]
- McMullen, J.; Kulinna, P.; Cothran, D. Chapter 5 Physical Activity Opportunities During the School Day: Classroom Teachers’ Perceptions of Using Activity Breaks in the Classroom. J. Teach. Phys. Educ. 2014, 33, 511–527. [Google Scholar] [CrossRef]
- Reyes-Amigo, T.; Ibarra-Mora, J.; Aguilar-Farías, N.; Gómez-Álvarez, N.; Carrasco-Beltrán, H.; Zapata-Lamana, R.; Hurtado-Almonácid, J.; Páez-Herrera, J.; Yañez-Sepulveda, R.; Cortés, G.; et al. An Active Break Program (ACTIVA-MENTE) at Elementary Schools in Chile: Study Protocol for a Pilot Cluster Randomized Controlled Trial. Front. Public Health 2024, 11, 1243592. [Google Scholar] [CrossRef] [PubMed]
- Dallolio, L.; Gallè, F.; Masini, A. Active Breaks: A Strategy to Counteract Sedentary Behaviors for Health Promoting Schools. A Discussion on Their Implementation in Italy. Ann. Ig. Med. Prev. E Comunità 2023, 35, 202–212. [Google Scholar] [CrossRef]
- Carlson, J.A.; Engelberg, J.K.; Cain, K.L.; Conway, T.L.; Mignano, A.M.; Bonilla, E.A.; Geremia, C.; Sallis, J.F. Implementing Classroom Physical Activity Breaks: Associations with Student Physical Activity and Classroom Behavior. Prev. Med. 2015, 81, 67–72. [Google Scholar] [CrossRef]
- Mavilidi, M.F.; Drew, R.; Morgan, P.J.; Lubans, D.R.; Schmidt, M.; Riley, N. Effects of Different Types of Classroom Physical Activity Breaks on Children’s On-task Behaviour, Academic Achievement and Cognition. Acta Paediatr. 2020, 109, 158–165. [Google Scholar] [CrossRef]
- Masini, A.; Marini, S.; Ceciliani, A.; Barone, G.; Lanari, M.; Gori, D.; Bragonzoni, L.; Toselli, S.; Stagni, R.; Bisi, M.C.; et al. The Effects of an Active Breaks Intervention on Physical and Cognitive Performance: Results from the I-MOVE Study. J. Public Health 2023, 45, 919–929. [Google Scholar] [CrossRef]
- Reyes-Amigo, T.; Salinas-Gallardo, G.; Mendoza, E.; Ovalle-Fernández, C.; Ibarra-Mora, J.; Gómez-Álvarez, N.; Carrasco-Beltrán, H.; Páez-Herrera, J.; Hurtado-Almonácid, J.; Yañez-Sepúlveda, R.; et al. Effectiveness of School-Based Active Breaks on Classroom Behavior, Executive Functions and Physical Fitness in Children and Adolescent: A Systematic Review. Front. Public Health 2025, 13, 1469998. [Google Scholar] [CrossRef]
- Infantes-Paniagua, Á.; Silva, A.F.; Ramirez-Campillo, R.; Sarmento, H.; González-Fernández, F.T.; González-Víllora, S.; Clemente, F.M. Active School Breaks and Students’ Attention: A Systematic Review with Meta-Analysis. Brain Sci. 2021, 11, 675. [Google Scholar] [CrossRef]
- Mullins, N.M.; Michaliszyn, S.F.; Kelly-Miller, N.; Groll, L. Elementary School Classroom Physical Activity Breaks: Student, Teacher, and Facilitator Perspectives. Adv. Physiol. Educ. 2019, 43, 140–148. [Google Scholar] [CrossRef]
- Masini, A.; Ceciliani, A.; Dallolio, L.; Gori, D.; Marini, S. Evaluation of Feasibility, Effectiveness, and Sustainability of School-Based Physical Activity “Active Break” Interventions in Pre-Adolescent and Adolescent Students: A Systematic Review. Can. J. Public Health 2022, 113, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, N.; Mantilla, A.; Bussey, K.; Emonson, C.; Olive, L.; McGillivray, J.; Pesce, C.; Lewis, S.; Rinehart, N. Understanding the Benefits of Brief Classroom-Based Physical Activity Interventions on Primary School-Aged Children’s Enjoyment and Subjective Wellbeing: A Systematic Review. J. Sch. Health 2022, 92, 916–932. [Google Scholar] [CrossRef]
- Van Den Berg, V.; Salimi, R.; De Groot, R.; Jolles, J.; Chinapaw, M.; Singh, A. “It’s a Battle… You Want to Do It, but How Will You Get It Done?”: Teachers’ and Principals’ Perceptions of Implementing Additional Physical Activity in School for Academic Performance. Int. J. Environ. Res. Public Health 2017, 14, 1160. [Google Scholar] [CrossRef]
- Barcelona, J.; Centeio, E.; Phillips, S.; Gleeson, D.; Mercier, K.; Foley, J.; Simonton, K.; Garn, A. Comprehensive School Health: Teachers’ Perceptions and Implementation of Classroom Physical Activity Breaks in US Schools. Health Promot. Int. 2022, 37, daac100. [Google Scholar] [CrossRef]
- Campbell, A.L.; Lassiter, J.W. Teacher Perceptions of Facilitators and Barriers to Implementing Classroom Physical Activity Breaks. J. Educ. Res. 2020, 113, 108–119. [Google Scholar] [CrossRef]
- McKown, H.B.; Centeio, E.E.; Barcelona, J.M.; Pedder, C.; Moore, E.W.G.; Erwin, H.E. Exploring Classroom Teachers’ Efficacy towards Implementing Physical Activity Breaks in the Classroom. Health Educ. J. 2022, 81, 585–596. [Google Scholar] [CrossRef]
- Schuchardt, K.; Gebhardt, M.; Mäehler, C. Working Memory Functions in Children with Different Degrees of Intellectual Disability. J. Intellect. Disabil. Res. 2010, 54, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute Piano Nazionale Della Prevenzione 2020–2025. Available online: https://www.salute.gov.it/imgs/C_17_notizie_5029_0_file.pdf (accessed on 25 September 2025).
- Bennett, C.; Khangura, S.; Brehaut, J.C.; Graham, I.D.; Moher, D.; Potter, B.K.; Grimshaw, J.M. Reporting Guidelines for Survey Research: An Analysis of Published Guidance and Reporting Practices. PLoS Med. 2011, 8, e1001069. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.; Hwang, H.-J. The Importance of Anonymity and Confidentiality for Conducting Survey Research. J. Res. Publ. Ethics 2023, 4, 1–7. [Google Scholar] [CrossRef]
- Martyn, L.; Bigelow, H.; Graham, J.D.; Ogrodnik, M.; Chiodo, D.; Fenesi, B. A Mixed Method Investigation of Teacher-Identified Barriers, Facilitators and Recommendations to Implementing Daily Physical Activity in Ontario Elementary Schools. BMC Public Health 2022, 22, 1986. [Google Scholar] [CrossRef]
- Mok, M.M.C.; Chin, M.K.; Chen, S.; Emeljanovas, A.; Mieziene, B.; Bronikowski, M.; Laudanska-Krzeminska, I.; Milanovic, I.; Pasic, M.; Balasekaran, G.; et al. Psychometric Properties of the Attitudes toward Physical Activity Scale: A Rasch Analysis Based on Data From Five Locations. J. Appl. Meas. 2015, 16, 379–400. [Google Scholar]
- Kuhn, A.P.; Parker, E.A.; Lane, H.G.; Deitch, R.; Wang, Y.; Turner, L.; Hager, E.R. Physical Activity, Confidence, and Social Norms Associated With Teachers’ Classroom Physical Activity Break Implementation. Health Promot. Pract. 2024, 25, 358–367. [Google Scholar] [CrossRef]
- Draugalis, J.R.; Plaza, C.M. Best Practices for Survey Research Reports Revisited: Implications of Target Population, Probability Sampling, and Response Rate. Am. J. Pharm. Educ. 2009, 73, 142. [Google Scholar] [CrossRef]
- General Data Protection Regulation (GDPR). (EU 2016/679). Available online: https://gdpr-info.eu (accessed on 20 May 2020).
- Wilson, A.B.; Brooks, W.S.; Edwards, D.N.; Deaver, J.; Surd, J.A.; Pirlo, O.J.; Byrd, W.A.; Meyer, E.R.; Beresheim, A.; Cuskey, S.L.; et al. Survey Response Rates in Health Sciences Education Research: A 10-year Meta-analysis. Anat. Sci. Educ. 2024, 17, 11–23. [Google Scholar] [CrossRef]
- European Education and Culture Executive Agency. Eurydice. In The European Higher Education Area in 2024: Bologna Process Implementation Report; Publications Office: Luxembourg, 2024. [Google Scholar]
- Dinkel, D.; Schaffer, C.; Snyder, K.; Lee, J.M. They Just Need to Move: Teachers’ Perception of Classroom Physical Activity Breaks. Teach. Teach. Educ. 2017, 63, 186–195. [Google Scholar] [CrossRef]
- Webster, C.A.; Russ, L.; Vazou, S.; Goh, T.L.; Erwin, H. Integrating Movement in Academic Classrooms: Understanding, Applying and Advancing the Knowledge Base. Obes. Rev. 2015, 16, 691–701. [Google Scholar] [CrossRef]
- Masini, A.; Longo, G.; Ricci, M.; Scheier, L.M.; Sansavini, A.; Ceciliani, A.; Dallolio, L. Investigating Facilitators and Barriers for Active Breaks among Secondary School Students: Formative Evaluation of Teachers and Students. Children 2024, 11, 155. [Google Scholar] [CrossRef]
- Masini, A.; Marini, S.; Gori, D.; Leoni, E.; Rochira, A.; Dallolio, L. Evaluation of School-Based Interventions of Active Breaks in Primary Schools: A Systematic Review and Meta-Analysis. J. Sci. Med. Sport 2020, 23, 377–384. [Google Scholar] [CrossRef]
- Martin, R.; Murtagh, E.M. Teachers’ and Students’ Perspectives of Participating in the ‘Active Classrooms’ Movement Integration Programme. Teach. Teach. Educ. 2017, 63, 218–230. [Google Scholar] [CrossRef]
- Michael, R.D.; Webster, C.A.; Egan, C.A.; Nilges, L.; Brian, A.; Johnson, R.; Carson, R.L. Facilitators and Barriers to Movement Integration in Elementary Classrooms: A Systematic Review. Res. Q. Exerc. Sport 2019, 90, 151–162. [Google Scholar] [CrossRef]
- Sit, C.H.P.; Mckenzie, T.L.; Cerin, E.; Chow, B.C.; Huang, W.Y.; Yu, J. Physical Activity and Sedentary Time among Children with Disabilities at School. Med. Sci. Sports Exerc. 2017, 49, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Mazzoli, E.; Koorts, H.; Salmon, J.; Pesce, C.; May, T.; Teo, W.-P.; Barnett, L.M. Feasibility of Breaking up Sitting Time in Mainstream and Special Schools with a Cognitively Challenging Motor Task. J. Sport Health Sci. 2019, 8, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Carroll, D.D.; Courtney-Long, E.A.; Stevens, A.C.; Sloan, M.L.; Lullo, C.; Visser, S.N.; Fox, M.H.; Armour, B.S.; Campbell, V.A.; Brown, D.R.; et al. Vital Signs: Disability and Physical Activity--United States, 2009–2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 407–413. [Google Scholar] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).