
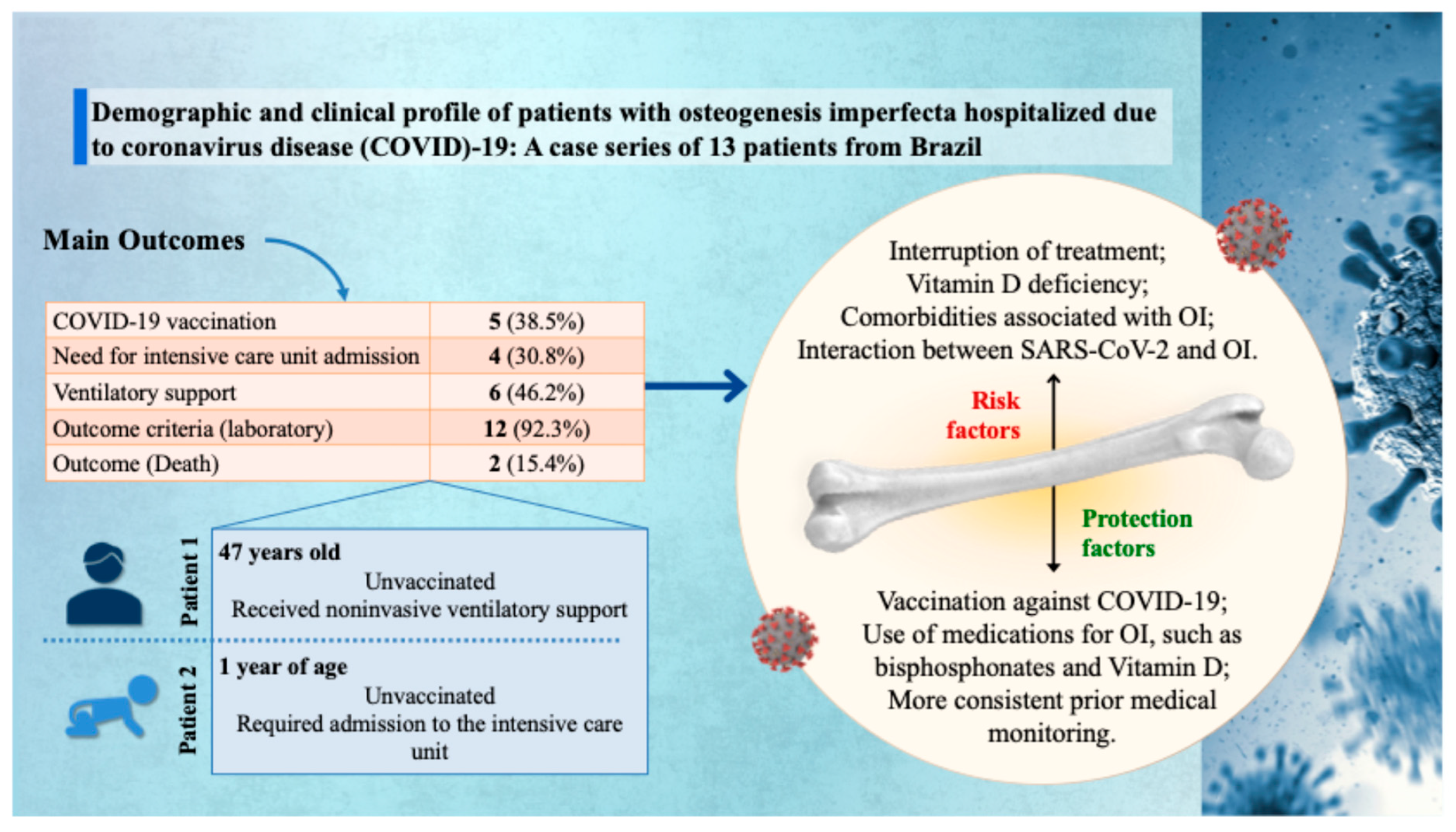
Demographic and Clinical Profile of Patients with Osteogenesis Imperfecta Hospitalized Due to Coronavirus Disease (COVID)-19: A Case Series of 13 Patients from Brazil

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| % | Percentage |
| 25(OH)D | 25-hydroxyvitamin D |
| 95% CI | 95% confidence interval |
| ACE2 | Angiotensin-converting enzyme |
| AL | Alagoas |
| B | Black |
| BBS | Brittle Bones Society |
| C | Clinic |
| COL1A1 | Collagen Type I Alpha 1 Chain |
| COL1A2 | Collagen Type I Alpha 2 Chain |
| COVID-19 | Coronavirus disease-19 |
| ERN BOND | European Reference Network on Rare Bone Diseases |
| F | Female |
| FD | Federal District |
| ICU | Intensive care unit |
| IQR | Interquartile range |
| L | Laboratory |
| M | Male |
| MG | Minas Gerais |
| MI | Mixed individuals |
| MS | Mato Grosso do Sul |
| NF-κB | Nuclear factor kappa B |
| ng/mL | Nanograms per milliliter |
| NI | No Invasive |
| OI | Osteogenesis imperfecta |
| P | Patients |
| PE | Pernambuco |
| PLS3 | Plastin-3 |
| PR | Paraná |
| OR | Odds ratio |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SIVEP-Gripe | Sistema de Informação da Vigilância Epidemiológica da Gripe |
| SPSS | Statistical Package for the Social Sciences |
| SUS | Sistema Único de Saúde |
| RANKL | Receptor Activator of Nuclear Factor Kappa-B Ligand |
| RS | Rio Grande do Sul |
| S | Spike |
| SC | Santa Catarina |
| SP | São Paulo |
| U | Urban |
| W | White |
| WHO | World Health Organization |
References
- Subramanian, S.; Anastasopoulou, C.; Viswanathan, V.K. Osteogenesis Imperfecta. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Warman, M.L.; Cormier-Daire, V.; Hall, C.; Krakow, D.; Lachman, R.; LeMerrer, M.; Mortier, G.; Mundlos, S.; Nishimura, G.; Rimoin, D.L.; et al. Nosology and Classification of Genetic Skeletal Disorders: 2010 Revision. Am. J. Med. Genet. A 2011, 155A, 943–968. [Google Scholar] [CrossRef] [PubMed]
- Aliyeva, L.; Ongen, Y.D.; Eren, E.; Sarisozen, M.B.; Alemdar, A.; Temel, S.G.; Sag, S.O. Genotype and Phenotype Correlation of Patients with Osteogenesis Imperfecta. J. Mol. Diagn. 2024, 26, 754–769. [Google Scholar] [CrossRef] [PubMed]
- Byrd, J.J.; White, A.C.; Nissen, C.G.; Schissel, M.; Van Ormer, M.; Velasco, D.; Wallace, M. Genotype-Phenotype Correlations in 294 Pediatric Patients with Osteogenesis Imperfecta. JBMR Plus 2024, 8, ziae125. [Google Scholar] [CrossRef] [PubMed]
- Rossi, V.; Lee, B.; Marom, R. Osteogenesis Imperfecta: Advancements in Genetics and Treatment. Curr. Opin. Pediatr. 2019, 31, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, F.S.; Sillence, D.O. Osteogenesis Imperfecta: Clinical Diagnosis, Nomenclature and Severity Assessment. Am. J. Med. Genet. A 2014, 164A, 1470–1481. [Google Scholar] [CrossRef] [PubMed]
- Botor, M.; Fus-Kujawa, A.; Uroczynska, M.; Stepien, K.L.; Galicka, A.; Gawron, K.; Sieron, A.L. Osteogenesis Imperfecta: Current and Prospective Therapies. Biomolecules 2021, 11, 1493. [Google Scholar] [CrossRef] [PubMed]
- Santili, C.; Akkari, M.; Waisberg, G.; Bastos Júnior, J.O.C.; Ferreira, W.M. Avaliação clínica, radiográfica e laboratorial de pacientes com osteogênese imperfeita. Rev. Assoc. Med. Bras. 2005, 51, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Deguchi, M.; Tsuji, S.; Katsura, D.; Kasahara, K.; Kimura, F.; Murakami, T. Current Overview of Osteogenesis Imperfecta. Medicina 2021, 57, 464. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.M.; Rocha-Braz, M.G.M.; França, M.M.; Lerario, A.M.; Simões, V.R.F.; Zanardo, E.A.; Kulikowski, L.D.; Martin, R.M.; Mendonca, B.B.; Ferraz-de-Souza, B. The Molecular Landscape of Osteogenesis Imperfecta in a Brazilian Tertiary Service Cohort. Osteoporos. Int. 2020, 31, 1341–1352. [Google Scholar] [CrossRef] [PubMed]
- Holtz, A.P.; Souza, L.T.; Ribeiro, E.M.; Acosta, A.X.; Lago, R.M.R.S.; Simoni, G.; Llerena, J.C.; Félix, T.M. Genetic Analysis of Osteogenesis Imperfecta in a Large Brazilian Cohort. Bone 2023, 169, 116683. [Google Scholar] [CrossRef] [PubMed]
- Reis, F.C.; Alexandrino, F.; Steiner, C.E.; Norato, D.Y.J.; Cavalcanti, D.P.; Sartorato, E.L. Molecular Findings in Brazilian Patients with Osteogenesis Imperfecta. J. Appl. Genet. 2005, 46, 105–108. [Google Scholar] [PubMed]
- Martins, J.P.; Siqueira, B.A.; Sansone, N.M.S.; Marson, F.A.L. COVID-19 in Brazil: A Three-Year Update. Diagn. Microbiol. Infect. Dis. 2023, 107, 116074. [Google Scholar] [CrossRef] [PubMed]
- Lauwers, M.; Au, M.; Yuan, S.; Wen, C. COVID-19 in Joint Ageing and Osteoarthritis: Current Status and Perspectives. Int. J. Mol. Sci. 2022, 23, 720. [Google Scholar] [CrossRef] [PubMed]
- Puig-Domingo, M.; Marazuela, M.; Yildiz, B.O.; Giustina, A. COVID-19 and Endocrine and Metabolic Diseases. An Updated Statement from the European Society of Endocrinology. Endocrine 2021, 72, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Mung, S.M.; Jude, E.B. Interplay between Endocrinology, Metabolism and COVID-19 Infection. Clin. Med. 2021, 21, e499–e504. [Google Scholar] [CrossRef] [PubMed]
- di Filippo, L.; Frara, S.; Doga, M.; Giustina, A. The Osteo-Metabolic Phenotype of COVID-19: An Update. Endocrine 2022, 78, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Sapra, L.; Saini, C.; Garg, B.; Gupta, R.; Verma, B.; Mishra, P.K.; Srivastava, R.K. Long-Term Implications of COVID-19 on Bone Health: Pathophysiology and Therapeutics. Inflamm. Res. 2022, 71, 1025–1040. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Creecy, A.; Awosanya, O.D.; McCune, T.; Ozanne, M.V.; Toepp, A.J.; Kacena, M.A.; Qiao, X. SARS-CoV-2 and Its Multifaceted Impact on Bone Health: Mechanisms and Clinical Evidence. Curr. Osteoporos. Rep. 2024, 22, 135–145. [Google Scholar] [CrossRef] [PubMed]
- di Filippo, L.; Doga, M.; Frara, S.; Giustina, A. Hypocalcemia in COVID-19: Prevalence, Clinical Significance and Therapeutic Implications. Rev. Endocr. Metab. Disord. 2022, 23, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Giustina, A.; Bouillon, R.; Binkley, N.; Sempos, C.; Adler, R.A.; Bollerslev, J.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Heijboer, A.; et al. Controversies in Vitamin D: A Statement from the Third International Conference. JBMR Plus 2020, 4, e10417. [Google Scholar] [CrossRef] [PubMed]
- Coccia, F.; Pietrobelli, A.; Zoller, T.; Guzzo, A.; Cavarzere, P.; Fassio, A.; Flodmark, C.-E.; Gatti, D.; Antoniazzi, F. Vitamin D and Osteogenesis Imperfecta in Pediatrics. Pharmaceuticals 2023, 16, 690. [Google Scholar] [CrossRef] [PubMed]
- Gnoli, M.; Brizola, E.; Tremosini, M.; Di Cecco, A.; Sangiorgi, L. Vitamin D and Bone Fragility in Individuals with Osteogenesis Imperfecta: A Scoping Review. Int. J. Mol. Sci. 2023, 24, 9416. [Google Scholar] [CrossRef] [PubMed]
- Abdrabbo, M.; Birch, C.M.; Brandt, M.; Cicigoi, K.A.; Coffey, S.J.; Dolan, C.C.; Dvorak, H.; Gehrke, A.C.; Gerzema, A.E.L.; Hansen, A.; et al. Vitamin D and COVID-19: A Review on the Role of Vitamin D in Preventing and Reducing the Severity of COVID-19 Infection. Protein Sci. 2021, 30, 2206–2220. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.; Wang, Y.; Dreischulte, T.; Barreiro, O.; Gonzalez, R.J.; Hanč, P.; Matysiak, C.; Neely, H.R.; Rottenkolber, M.; Haskell, T.; et al. Association between Bisphosphonate Use and COVID-19 Related Outcomes. Elife 2023, 12, e79548. [Google Scholar] [CrossRef] [PubMed]
- Argano, C.; Mallaci Bocchio, R.; Natoli, G.; Scibetta, S.; Lo Monaco, M.; Corrao, S. Protective Effect of Vitamin D Supplementation on COVID-19-Related Intensive Care Hospitalization and Mortality: Definitive Evidence from Meta-Analysis and Trial Sequential Analysis. Pharmaceuticals 2023, 16, 130. [Google Scholar] [CrossRef] [PubMed]
- Alshukairi, A.N.; Doar, H.; Al-Sagheir, A.; Bahasan, M.A.; Sultan, A.A.; Al Hroub, M.K.; Itani, D.; Khalid, I.; Saeedi, M.F.; Bakhamis, S.; et al. Outcome of COVID19 in Patients with Osteogenesis Imperfecta: A Retrospective Multicenter Study in Saudi Arabia. Front. Endocrinol. 2022, 12, 800376. [Google Scholar] [CrossRef] [PubMed]
- Bandeira, F.; Bilezikian, J.P. Bone Diseases and the COVID-19 Pandemic. Arch. Endocrinol. Metab. 2022, 66, 589–590. [Google Scholar] [CrossRef] [PubMed]
- Tahtabasi, M.; Kilicaslan, N.; Akin, Y.; Karaman, E.; Gezer, M.; Icen, Y.K.; Sahiner, F. The Prognostic Value of Vertebral Bone Density on Chest CT in Hospitalized COVID-19 Patients. J. Clin. Densitom. 2021, 24, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Kong, G. Changes in Vitamin D Status among Adults from the COVID-19 Pandemic to Post-Pandemic Normality. Front. Nutr. 2024, 11, 1407890. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.P.; Sciani, J.M.; Marson, F.A.L. Huntington’s Disease in Hospitalized Patients Infected with SARS-CoV-2 in Brazil: Three-Year Update. Neurodegener. Dis. 2025, 25, 88–105. [Google Scholar] [CrossRef] [PubMed]
- Boschiero, M.N.; Palamim, C.V.C.; Ortega, M.M.; Marson, F.A.L. Clinical Characteristics and Comorbidities of COVID-19 in Unvaccinated Patients with Down Syndrome: First Year Report in Brazil. Hum. Genet. 2022, 141, 1887–1904. [Google Scholar] [CrossRef] [PubMed]
- Sansone, N.M.; Boschiero, M.N.; Valencise, F.E.; Palamim, C.V.; Marson, F.A. Characterization of Demographic Data, Clinical Signs, Comorbidities, and Outcomes According to the Race in Hospitalized Individuals with COVID-19 in Brazil: An Observational Study. J. Glob. Health 2022, 12, 05027. [Google Scholar] [CrossRef] [PubMed]
- Sansone, N.M.S.; Mello, L.S.; Martins, J.P.; Marson, F.A.L. Impact of Coronavirus Disease (COVID)-19 on the Indigenous Population of Brazil: A Systematic Review. J. Racial Ethn. Health Disparities 2025. [Google Scholar] [CrossRef] [PubMed]
- Boschiero, M.N.; Sansone, N.M.S.; Marson, F.A.L. Hospitalized Patients with X-Linked Disease and Infected with SARS-CoV-2 in Brazil: A Serial Case Report from the First Two Years of the Pandemic. Respir. Investig. 2023, 61, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, J.H.; Zhang, H.; Issa, H.; Wu, J.; Hama, T.; Phiho-Gomes, A.-C.; Groza, T.; Khalid, S.; Lumbers, T.R.; Hocaoglu, M.; et al. Prevalence and Demographics of 331 Rare Diseases and Associated COVID-19-Related Mortality among 58 Million Individuals: A Nationwide Retrospective Observational Study. Lancet Digit. Health 2025, 7, e145–e156. [Google Scholar] [CrossRef] [PubMed]
- Conti, P.B.M.; Ribeiro, M.Â.G.O.; Gomez, C.C.S.; Souza, A.P.; Borgli, D.S.P.; Sakano, E.; Pascoa, M.A.; Severino, S.D.; Castilho, T.; Marson, F.A.L.; et al. Pulmonary and Functional Hallmarks after SARS-CoV-2 Infection across Three WHO Severity Level-Groups: An Observational Study. Front. Med. 2025, 12, 1561387. [Google Scholar] [CrossRef] [PubMed]
- Palamim, C.V.C.; Siqueira, B.A.; Boschiero, M.N.; Marson, F.A.L. Increase in COVID-19 Underreporting among 3,282,337 Brazilian Hospitalized Patients Due to SARS: A 3-Year Report and a Major Concern for Health Authorities. Travel. Med. Infect. Dis. 2023, 54, 102616. [Google Scholar] [CrossRef] [PubMed]
- Marques, L.S.; Boschiero, M.N.; Sansone, N.M.S.; Brienze, L.R.; Marson, F.A.L. Epidemiological Profile of Hospitalized Patients with Cystic Fibrosis in Brazil Due to Severe Acute Respiratory Infection during the COVID-19 Pandemic and a Systematic Review of Worldwide COVID-19 in Those with Cystic Fibrosis. Healthcare 2023, 11, 1936. [Google Scholar] [CrossRef] [PubMed]
- Palamim, C.V.C.; Camargo, T.M.; Valencise, F.E.; Marson, F.A.L. Evaluation of the Case Fatality Rate in 2 031 309 Hospitalised Brazilian Patients Due to COVID-19: An Observational Study of the First 3 Years of the Pandemic in Brazil. BMJ Public Health 2025, 3, e000724. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.E.F.; Costa, P.T.; Mello, L.S.; Marques, L.F.A.; Dos Santos, V.S.; Marson, F.A.L. A Serial Case Report of Hospitalized Patients with Creutzfeldt-Jakob Disease Due to Coronavirus Disease (COVID)-19 in Brazil: A Four-Year Profile. J. Neurol. Sci. 2025, 469, 123380. [Google Scholar] [CrossRef] [PubMed]
- Sansone, N.M.S.; Valencise, F.E.; Bredariol, R.F.; Peixoto, A.O.; Marson, F.A.L. Profile of Coronavirus Disease Enlightened Asthma as a Protective Factor against Death: An Epidemiology Study from Brazil during the Pandemic. Front. Med. 2022, 9, 953084. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Varna, V.P.; Sharma, U.; Mavalankar, D. Does Vitamin D Supplementation Reduce COVID-19 Severity?: A Systematic Review. QJM 2022, 115, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Nguengang Wakap, S.; Lambert, D.M.; Olry, A.; Rodwell, C.; Gueydan, C.; Lanneau, V.; Murphy, D.; Le Cam, Y.; Rath, A. Estimating Cumulative Point Prevalence of Rare Diseases: Analysis of the Orphanet Database. Eur. J. Hum. Genet. 2020, 28, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Zybarth, D.; Brandt, M.; Mundlos, C.; Inhestern, L. Impact of the COVID-19 Pandemic on Health Care and Daily Life of Patients with Rare Diseases from the Perspective of Patient Organizations—A Qualitative Interview Study. Orphanet J. Rare Dis. 2023, 18, 154. [Google Scholar] [CrossRef] [PubMed]
- Smyth, D.; Hytiris, M.; Kelday, C.; McDonnell, C.; Burren, C.; Gardner, A.; Mills, L.; Parekh, S.; Semler, O.; Stewart, A.; et al. Patient-Reported Experience of Clinical Care of Osteogenesis Imperfecta (OI) during the COVID-19 Pandemic. Front. Public Health 2022, 10, 951569. [Google Scholar] [CrossRef] [PubMed]
- Boschiero, M.N.; Palamim, C.V.C.; Marson, F.A.L. The Hindrances to Perform the COVID-19 Vaccination in Brazil. Hum. Vaccin. Immunother. 2021, 17, 3989–4004. [Google Scholar] [CrossRef] [PubMed]
- Brizola, E.; Adami, G.; Baroncelli, G.I.; Bedeschi, M.F.; Berardi, P.; Boero, S.; Brandi, M.L.; Casareto, L.; Castagnola, E.; Fraschini, P.; et al. Providing High-Quality Care Remotely to Patients with Rare Bone Diseases during COVID-19 Pandemic. Orphanet J. Rare Dis. 2020, 15, 228. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | P1 | P2 | P3 | P4 | P5 | P6 | P7 | P8 | P9 | P10 | P11 | P12 | P13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Notification date | 02/23 | 07/21 | 02/21 | 12/22 | 01/21 | 11/21 | 08/20 | 09/20 | 04/21 | 05/21 | 03/22 | 03/22 | 05/23 |
| Notification state | MG | FD | MS | MG | RS | PE | SC | PE | SP | MG | PR | MG | AL |
| Sex | M | F | F | F | M | M | M | F | F | F | M | M | M |
| Age (years) | 50 | 58 | 31 | 22 | 47 | 60 | 47 | <1 | 25 | 58 | 1 | 2 | <1 |
| Race | B | W | W | W | W | MI | W | MI | W | W | W | MI | W |
| Housing region | U | U | U | U | U | U | U | U | U | U | U | U | U |
| Nosocomial infection | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Clinical signs and symptoms | |||||||||||||
| Fever | Yes | Yes | No | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes |
| Cough | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Sore throat | No | No | No | Yes | Yes | No | No | No | No | No | No | No | No |
| Dyspnea | No | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Respiratory discomfort | No | Yes | No | No | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes |
| Peripheral oxygen saturation <95% | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes |
| Diarrhea | No | No | No | No | No | No | No | No | No | Yes | No | No | No |
| Vomiting | No | No | No | No | Yes | No | No | No | No | No | Yes | Yes | No |
| Fatigue | No | No | No | No | No | No | No | No | No | Yes | No | No | No |
| Another symptom | No | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | No | No | No |
| Comorbidities | |||||||||||||
| Heart diseases | No | Yes | No | No | No | No | Yes | No | No | No | No | No | No |
| Hematological disorders | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Down syndrome | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Liver diseases | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Asthma | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Diabetes mellitus | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Neurological disorders | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Chronic respiratory diseases | No | No | No | No | No | No | No | No | No | No | No | Yes | No |
| Immunosuppressive disorders | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Kidney diseases | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Obesity | No | No | No | No | Yes | No | No | No | No | No | No | No | No |
| Vaccinated against COVID-19 | No | Yes | Yes | Yes | No | Yes | No | No | No | No | No | No | Yes |
| Antiviral for the treatment of flu-like symptoms | No | No | No | No | No | No | No | No | No | No | No | No | No |
| Required admission to the intensive care unit | No | Yes | No | No | No | No | No | No | No | No | Yes | Yes | Yes |
| Received ventilatory support | No | NI | No | No | No | NI | NI | No | NI | NI | No | No | NI |
| Outcome criteria | L | C | L | L | L | L | L | L | L | L | L | L | L |
| Outcome | Cure | Cure | Cure | Cure | Cure | Cure | Death | Cure | Cure | Cure | Death | Cure | Cure |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morikawa, L.L.; Marques, L.F.A.; Silva, A.E.F.; Costa, P.T.; Mello, L.S.; Fraga, A.d.M.A.; Marson, F.A.L. Demographic and Clinical Profile of Patients with Osteogenesis Imperfecta Hospitalized Due to Coronavirus Disease (COVID)-19: A Case Series of 13 Patients from Brazil. Healthcare 2025, 13, 1779. https://doi.org/10.3390/healthcare13151779
Morikawa LL, Marques LFA, Silva AEF, Costa PT, Mello LS, Fraga AdMA, Marson FAL. Demographic and Clinical Profile of Patients with Osteogenesis Imperfecta Hospitalized Due to Coronavirus Disease (COVID)-19: A Case Series of 13 Patients from Brazil. Healthcare. 2025; 13(15):1779. https://doi.org/10.3390/healthcare13151779
Chicago/Turabian StyleMorikawa, Luana Lury, Luiz Felipe Azevedo Marques, Adriele Evelyn Ferreira Silva, Patrícia Teixeira Costa, Lucas Silva Mello, Andrea de Melo Alexandre Fraga, and Fernando Augusto Lima Marson. 2025. "Demographic and Clinical Profile of Patients with Osteogenesis Imperfecta Hospitalized Due to Coronavirus Disease (COVID)-19: A Case Series of 13 Patients from Brazil" Healthcare 13, no. 15: 1779. https://doi.org/10.3390/healthcare13151779
APA StyleMorikawa, L. L., Marques, L. F. A., Silva, A. E. F., Costa, P. T., Mello, L. S., Fraga, A. d. M. A., & Marson, F. A. L. (2025). Demographic and Clinical Profile of Patients with Osteogenesis Imperfecta Hospitalized Due to Coronavirus Disease (COVID)-19: A Case Series of 13 Patients from Brazil. Healthcare, 13(15), 1779. https://doi.org/10.3390/healthcare13151779