
Efficacy and Predictability of Maxillary and Mandibular Dental Arch Expansion with Clear Aligners in Prepuberal Subjects: A Digital Retrospective Analysis


 ,
, 
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Treatment Protocol
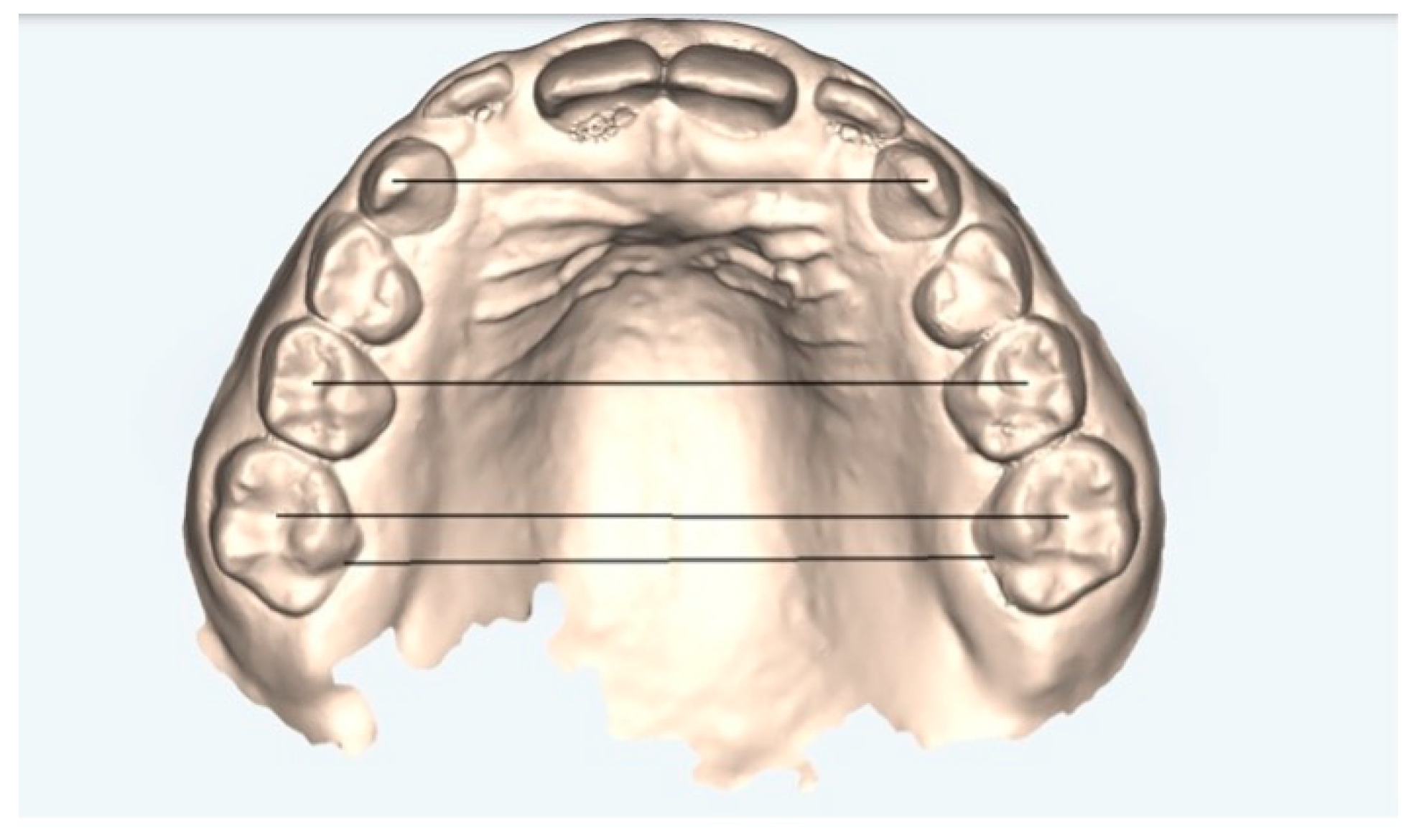
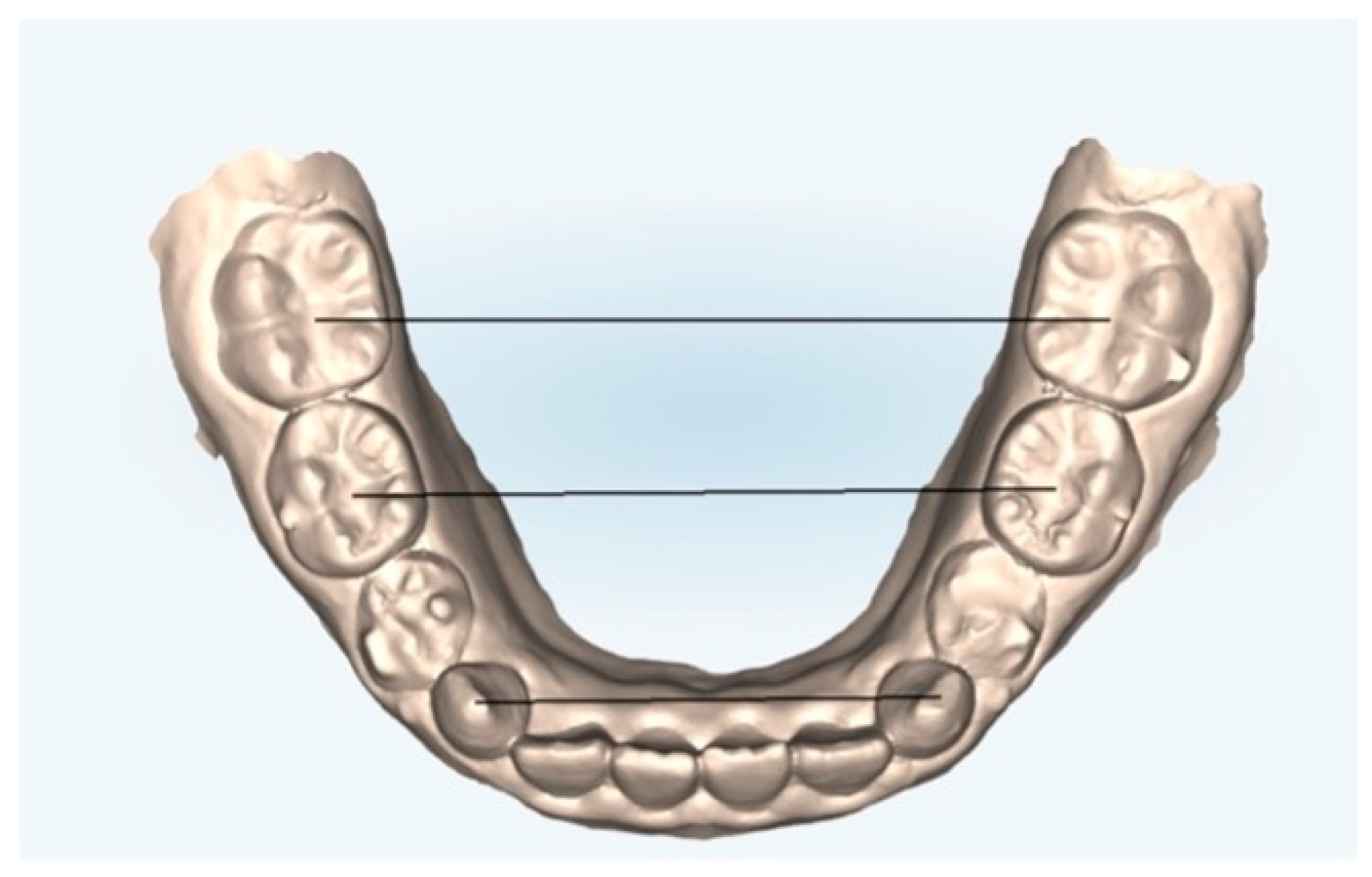
2.2. Measurement Protocol
- Canine cuspid width (CCW): linear distance between the tips of the cusps of the upper or lower canines;
- Canine gingival width (CGW): linear distance from the center of a palatal surface in contact with the gingival margin of one canine, upper or lower, to the other;
- First primary molar cuspid width (1PMWC): linear distance between the tips of the buccal cusps of the upper or lower first premolars;
- First primary molar gingival width (1PMWG): linear distance between the center of the palatal surface in contact with the gingival margin of the upper or lower first premolars;
- Second primary molar cuspid width (2PMWC): linear distance between the tips of the buccal cusps of the upper or lower second premolars;
- Second primary molar gingival width (2PMWG): linear distance between the center of the palatal surface in contact with the gingival margin of the upper or lower second premolars;
- First permanent molar cuspid width (MWC): linear distance between the tips of the buccal cusps of the upper or lower first permanent molars;
- First permanent molar gingival width (MWG): linear distance between the center of the palatal surface in contact with the gingival margin of the upper or lower first permanent molars.
2.3. Statistical Analysis
3. Results
3.1. Upper Arch
3.2. Lower Arch
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lione, R.; Paoloni, V.; Bartolommei, L.; Gazzani, F.; Meuli, S.; Pavoni, C.; Cozza, P. Maxillary arch development with Invisalign system. Angle Orthod. 2021, 91, 433–440. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Weinberg, M.; Sadowsky, C. Resolution of mandibular arch crowding in growing patients with Class I malocclusions treated nonextraction. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Giancotti, A.; Greco, M.; Mampieri, G. Clear aligner therapy in orthodontics: Treatment of complex cases with Invisalign. J. Clin. Orthod. 2008, 42, 679–688. [Google Scholar]
- Miller, D.B. Invisalign in TMD treatment. Int. J. Orthod. Milwaukee 2009, 20, 15–19. [Google Scholar] [PubMed]
- Caruso, S.; Nota, A.; Ehsani, S.; Gatto, R. The impact of clear aligners on periodontal health: A comprehensive review. J. Clin. Exp. Dent. 2019, 11, e896–e900. [Google Scholar]
- Nota, A.; Caruso, S.; Ehsani, S.; Tecco, S. Predictability of orthodontic clear aligner treatment in adult patients: A retrospective study. Prog. Orthod. 2021, 22, 36. [Google Scholar]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Anand, M.; Turpin, D.L.; Jumani, K.S.; Spiekerman, C.F.; Huang, G.J. Retrospective investigation of the effects and efficiency of self-ligating and conventional brackets. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 67–75. [Google Scholar] [CrossRef]
- Atik, E.; Akarsu-Guven, B.; Kocadereli, I.; Ciger, S. Evaluation of maxillary arch dimensional and inclination changes with self-ligating and conventional brackets using broad archwires. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 830–837. [Google Scholar] [CrossRef]
- Solano-Mendoza, B.; Sonnemberg, B.; Solano-Reina, E.; Iglesias-Linares, A. How effective is the Invisalign® system in expanding movement with Ex30′ aligners? Clin. Oral Investig. 2017, 21, 1475–1484. [Google Scholar] [CrossRef]
- Caruso, S.; De Felice, M.E.; Valenti, C.; Pagano, S.; Caruso, S.; Gatto, R.; Lombardo, G. An evaluation of the Invisalign® Aligner Technique and consideration of the force system: A systematic review. Syst. Rev. 2024, 13, 43. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mummolo, S.; Nota, A.; Tecco, S.; Marchetti, E.; Gatto, R.; Marzo, G. Orthodontic treatment with clear aligners in growing patients. Eur. J. Paediatr. Dent. 2020, 21, 112–116. [Google Scholar] [CrossRef]
- Mummolo, S.; Tieri, M.; Nota, A.; Caruso, S.; Darvizeh, A.; Albani, F.; Gatto, R.; Marzo, G.; Marchetti, E.; Quinzi, V.; et al. Salivary concentrations of Streptococcus mutans and Lactobacilli during an orthodontic treatment. An observational study comparing fixed and removable orthodontic appliances. Clin. Exp. Dent. Res. 2020, 6, 181–187. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caruso, S.; Nota, A.; Caruso, S.; Severino, M.; Gatto, R.; Meuli, S.; Mattei, A.; Tecco, S. Mandibular advancement with clear aligners in the treatment of skeletal Class II. A retrospective controlled study. Eur. J. Paediatr. Dent. 2021, 22, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, R.M. Occlusion--the medium of dentistry. J. Prosthet Dent. 1969, 21, 39–60. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.A. Maxillary transverse deficiency. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 567–570. [Google Scholar] [CrossRef]
- Marshall, S.D.; Southard, K.A.; Southard, T.E. Early transverse treatment. Semin. Orthod. 2005, 11, 130–139. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Grassia, V.; d’Apuzzo, F.; DiStasio, D.; Jamilian, A.; Lucchese, A.; Perillo, L. Upper and lower arch changes after Mixed Palatal Expansion protocol. Eur. J. Paediatr. Dent. 2014, 15, 375–380. [Google Scholar]
- Paradowska-Stolarz, A.M.; Wieckiewicz, M.; Mikulewicz, M.; Malysa, A.; Dus-Ilnicka, I.; Seweryn, P.; Laskowska, J.; Figueiredo Pollamann, M.C.; Adamska, M.; Wezgowiec, J. Comparison of the tensile modulus of three 3D-printable materials used in dentistry. Dent. Med. Probl. 2023, 60, 505–511. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.; Wezgowiec, J.; Malysa, A.; Wieckiewicz, M. Effects of Polishing and Artificial Aging on Mechanical Properties of Dental LT Clear® Resin. J. Funct. Biomater. 2023, 14, 295. [Google Scholar] [CrossRef] [PubMed]
- D’Antò, V.; Valletta, R.; Di Mauro, L.; Riccitiello, F.; Kirlis, R.; Rongo, R. The Predictability of Transverse Changes in Patients Treated with Clear Aligners. Materials 2023, 16, 1910. [Google Scholar] [CrossRef]
- Levrini, L.; Zecca, P.A.; Deppieri, A.; Caccia, M.; Scurati, E.I.; Legramandi, V.A.; Carganico, A. Predictability of Maxillary Expansion with Invisalign® First: Treatment Planning vs. Outcome. Appl. Sci. 2024, 14, 9871. [Google Scholar] [CrossRef]
- Rocha, A.S.; Gonçalves, M.; Oliveira, A.C.; Azevedo, R.M.S.; Pinho, T. Efficiency and Predictability of Coronal Maxillary Expansion Repercussion with the Aligners System: A Retrospective Study. Dent. J. 2023, 11, 258. [Google Scholar] [CrossRef]
- Staderini, E.; Patini, R.; Meuli, S.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Indication of clear aligners in the early treatment of anterior crossbite: A case series. Dent. Press J. Orthod. 2020, 25, 33–43. [Google Scholar] [CrossRef]
- Lione, R.; Cretella Lombardo, E.; Paoloni, V.; Meuli, S.; Pavoni, C.; Cozza, P. Upper arch dimensional changes with clear aligners in the early mixed dentition. J. Orofac. Orthop./Fortschritte Kieferorthopädie 2023, 84, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Guo, J. Efficiency of upper arch expansion with the Invisalign system. Angle Orthod. 2020, 90, 23–30. [Google Scholar] [CrossRef]
- Vidal-Bernárdez, M.; Vilches-Arenas, Á.; Sonnemberg, B.; Solano-Reina, E.; Solano-Mendoza, B. Efficacy and predictability of maxillary and mandibular expansion with the Invisalign® system. J. Clin. Exp. Dent. 2021, e669–e677. [Google Scholar] [CrossRef]
- Houle, J.-P.; Piedade, L.; Todescan, R.; Pinheiro, F.H.S.L. The predictability of transverse changes with Invisalign. Angle Orthod. 2017, 87, 19–24. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Upper Arch | Clinical Measuresments T0 | Clinical Measurements T1 | ΔClinical | Predicted Change T1 | ΔPredicted | % of Predictability | p-Value * ΔClinical vs. ΔPredicted |
|---|---|---|---|---|---|---|---|
| CCW | 31.83 ± 2.27 | 35.65 ± 1.04 | 3.81 ± 2.05 | 36.39 ± 0.78 | 4.56 ± 1.89 | 84% | 0.012 |
| 1PMWC | 39.68 ± 1.73 | 42.83 ± 1.71 | 3.15 ± 1.40 | 44.48 ± 1.64 | 4.80 ± 2.00 | 66% | 0.005 |
| MWC | 50.58 ± 1.86 | 53.89 ± 1.11 | 3.31 ± 1.70 | 54.91 ± 1.46 | 4.33 ± 2.16 | 76% | 0.017 |
| MWG | 32.89 ± 1.31 | 35.07 ± 1.99 | 2.18 ± 1.17 | 36.99 ± 2.41 | 4.10 ± 1.84 | 53% | 0.001 |
| Variables | Clinical Measurement T1 | Predicted Change T1 | Difference Between Clinical and Predicted Measurements at T1 | Mean (Clinical + Predicted)/2 |
|---|---|---|---|---|
| CCW | 35.65 ± 1.04 | 36.39 ± 0.78 | −0.74 | 36.02 |
| 1PMWC | 42.83 ± 1.71 | 44.48 ± 1.64 | −1.65 | 43.65 |
| MWC | 53.89 ± 1.11 | 54.91 ± 1.46 | −1.02 | 54.40 |
| MWG | 35.07 ± 1.99 | 36.99 ± 2.41 | −1.92 | 36.03 |
| ICC | 95% Interval Confidence | F Test with True Value 0 | |||
|---|---|---|---|---|---|
| Lower | Upper | Value | p Value | ||
| CCWMod-CCWCC | 4.89 | 0.013 | |||
| Single measures (intraclass) | 0.66 | 0.10 | 0.90 | ||
| Avarege measures (interclass) | 0.80 | 0.18 | 0.95 | ||
| 1PMWCMod-1PMWCCC | 4.51 | 0.018 | |||
| Single Measures (intraclass) | 0.64 | 0.06 | 0.90 | ||
| Avarege Measures (interclass) | 0.78 | 0.11 | 0.94 | ||
| MWCMod-MWCCC | 4.55 | 0.017 | |||
| Single measures (intraclass) | 0.64 | 0.06 | 0.90 | ||
| Avarege measures (interclass) | 0.78 | 0.12 | 0.95 | ||
| MWGMod-MWGCC | 9.87 | 0.001 | |||
| Single measures (intraclass) | 0.82 | 0.42 | 0.95 | ||
| Avarege measures (interclass) | 0.90 | 0.59 | 0.97 | ||
| Lower Arch | Clinical Measurements T0 | Clinical Measurements T1 | ΔClinical | Predicted Change | ΔPredicted | % of Predictability | p-Value * ΔClinical vs. ΔPredicted |
|---|---|---|---|---|---|---|---|
| CCW | 25.17 ±1.63 | 27.76 ±1.08 | 2.59 ± 2.03 | 28.50 ± 1.03 | 3.33 ± 2.07 | 78% | 0.009 |
| 1PMWC | 31.70 ± 1.71 | 35.29 ± 1.17 | 3.59 ± 1.57 | 36.28 ± 1.14 | 4.58 ± 1.68 | 78% | 0.037 |
| MWC | 44.43 ±1.56 | 47.36 ±2.31 | 2.94 ±1.80 | 47.78 ± 2.47 | 3.36 ± 1.57 | 88% | 0.227 |
| MWG | 32.69 ± 1.73 | 34.29 ± 2.36 | 1.60 ± 1.70 | 35.70 ± 2.52 | 3.02 ± 2.20 | 53% | 0.010 |
| Variables | Clinical Measurement T1 | Predicted Change T1 | Difference Between Clinical and Predicted Measurements at T1 | Mean (Clinical + Predicted)/2 |
|---|---|---|---|---|
| CCW | 27.76 ± 1.08 | 28.50 ± 1.03 | −0.74 | 28.13 |
| 1PMWC | 35.29 ± 1.17 | 36.28 ± 1.14 | −0.99 | 35.78 |
| MWC | 47.36 ± 2.31 | 47.78 ± 2.47 | −0.42 | 47.57 |
| MWG | 34.29 ± 2.36 | 35.70 ± 2.52 | −1.42 | 34.99 |
| ICC | 95% Interval Confidence | F Test with True Value 0 | |||
|---|---|---|---|---|---|
| Lower | Upper | Value | p Value | ||
| CCWMod-CCWCC | 7.73 | 0.003 | |||
| Single measures (intraclass) | 0.77 | 0.32 | 0.94 | ||
| Avarege measures (interclass) | 0.87 | 0.48 | 0.97 | ||
| 1PMWCMod-1PMWCCC | 2.21 | 0.126 | |||
| Single measures (intraclass) | 0.38 | −0.29 | 0.80 | ||
| Avarege measures (interclass) | 0.55 | −0.82 | 0.89 | ||
| MWCMod-MWCCC | 20.83 | <0.001 | |||
| Single measures (intraclass) | 0.91 | 0.68 | 0.98 | ||
| Avarege measures (interclass) | 0.95 | 0.81 | 0.99 | ||
| MWGMod-MWGCC | 11.78 | 0.001 | |||
| Single measures (intraclass) | 0.84 | 0.49 | 0.96 | ||
| Avarege measures (interclass) | 0.92 | 0.66 | 0.98 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, S.; Nota, A.; Tonelli, C.; Tai, S.K.; Baldini, G.; Fiasca, F.; Caruso, S.; Mattei, A. Efficacy and Predictability of Maxillary and Mandibular Dental Arch Expansion with Clear Aligners in Prepuberal Subjects: A Digital Retrospective Analysis. Healthcare 2025, 13, 1508. https://doi.org/10.3390/healthcare13131508
Caruso S, Nota A, Tonelli C, Tai SK, Baldini G, Fiasca F, Caruso S, Mattei A. Efficacy and Predictability of Maxillary and Mandibular Dental Arch Expansion with Clear Aligners in Prepuberal Subjects: A Digital Retrospective Analysis. Healthcare. 2025; 13(13):1508. https://doi.org/10.3390/healthcare13131508
Chicago/Turabian StyleCaruso, Silvia, Alessandro Nota, Chiara Tonelli, Sandra Khong Tai, Gianluca Baldini, Fabiana Fiasca, Sara Caruso, and Antonella Mattei. 2025. "Efficacy and Predictability of Maxillary and Mandibular Dental Arch Expansion with Clear Aligners in Prepuberal Subjects: A Digital Retrospective Analysis" Healthcare 13, no. 13: 1508. https://doi.org/10.3390/healthcare13131508
APA StyleCaruso, S., Nota, A., Tonelli, C., Tai, S. K., Baldini, G., Fiasca, F., Caruso, S., & Mattei, A. (2025). Efficacy and Predictability of Maxillary and Mandibular Dental Arch Expansion with Clear Aligners in Prepuberal Subjects: A Digital Retrospective Analysis. Healthcare, 13(13), 1508. https://doi.org/10.3390/healthcare13131508