
The Weekend Effect on In-Hospital Mortality—First 13-Year Retrospective Observational Study in Slovakia
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Data Sources
- -
- Demographic data: age, gender, and two age groups (under 65 and over 65).
- -
- Admission characteristics: day of admission (Monday–Sunday), length of hospital stay (LOS), and re-hospitalisations within 30 days.
- -
- Clinical information: primary diagnosis, principal diagnosis, admission diagnosis, and cause of death—all coded according to the International Classification of Diseases, 10th Revision (ICD-10)
- -
- Results: in-hospital mortality within 30 days of hospitalisation.
2.2. Study Objectives
2.3. Data Extraction
- (1)
- A comprehensive dataset of all hospitalisations from 2010 to 2022 in the 5th Department of Internal Medicine;
- (2)
- A detailed set of de-identified medical records of deceased patients.
- -
- ICD-10 codes for admission and cause of death;
- -
- Complete summaries of medical care;
- -
- Clinical and functional history;
- -
- Diagnostic investigations, including laboratory results (haematology, biochemistry, microbiology, urinalysis);
- -
- Imaging examinations (X-ray, CT, ultrasound);
- -
- Comorbidities and chronic diseases;
- -
- Medication history and treatment measures during hospitalization;
- -
- Specialist consultations (e.g., surgery, urology, rehabilitation);
- -
- Final clinical course and summary of the dying process.
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
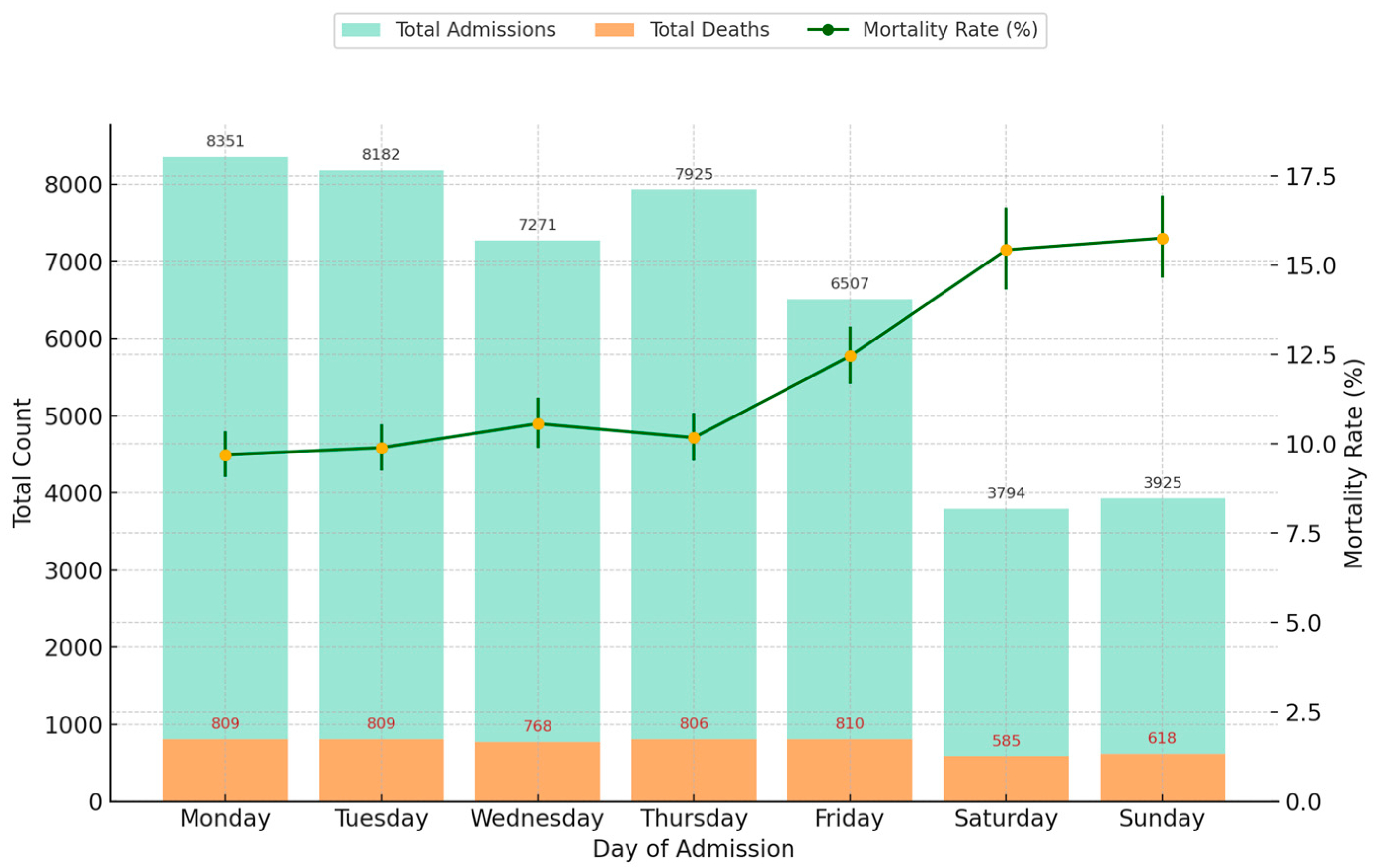
3.1. Patient Characteristics and Admission Patterns
- -
- Weekday admissions as those occurring from Monday to Friday
- -
- Weekend admissions as those occurring from Saturday to Sunday.
3.2. In-Hospital Mortality
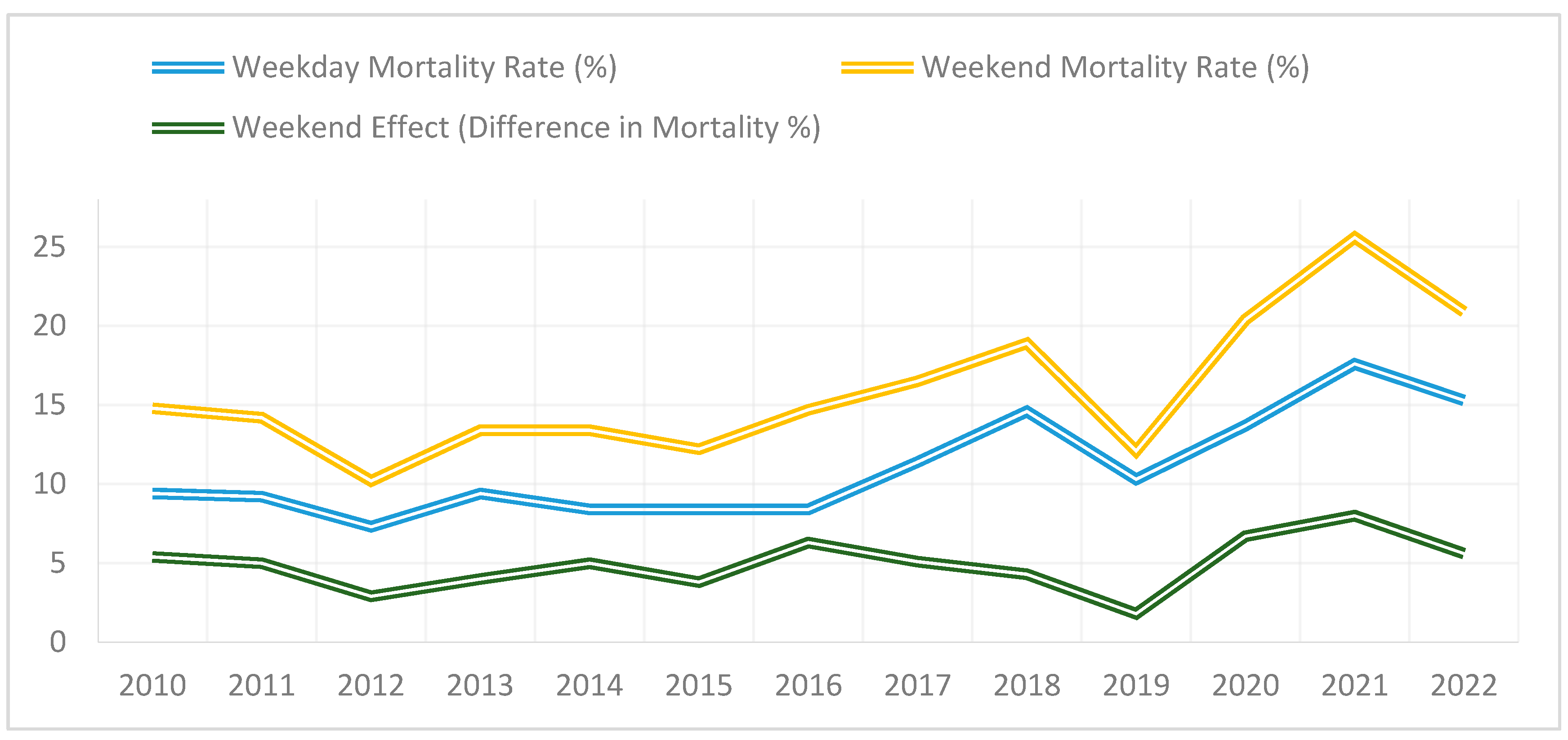
3.3. Mortality by Year
3.4. Unadjusted Analysis
3.5. Adjusted Analysis
3.6. Interaction Analysis
3.7. Cause-Specific Mortality and Weekend Admission Patterns
4. Discussion
4.1. Overview of Findings
4.2. Interaction Analysis Findings
4.3. Interpreation of Cause-Specific Mortality Patterns
4.4. Temporal Trends and Association with the COVID-19 Pandemic
4.5. Potential Mechanisms Behind the Weekend Effect
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AOR | Adjusted Odds Ratio |
| CI | Confidence Interval |
| COVID-19 | Coronavirus Disease 2019 |
| GLM | Generalised Linear Model |
| ICD-10 | International Classification of Diseases, 10th Revision |
| INESS | Institute of Economic and Social Studies |
| LOS | Length of Stay |
| OR | Odds Ratio |
| SD | Standard Deviation |
| V4 | Visegrad Group |
References
- Bell, C.M.; Redelmeier, D.A. Mortality among Patients Admitted to Hospitals on Weekends as Compared with Weekdays. N. Engl. J. Med. 2001, 345, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Ricciardi, R.; Nelson, J.; Francone, T.D.; Roberts, P.L.; Read, T.E.; Hall, J.F.; Schoetz, D.J.; Marcello, P.W. Do patient safety indicators explain increased weekend mortality? J. Surg. Res. 2016, 200, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Bressman, E.; Rowland, J.C.; Nguyen, V.-T.; Raucher, B.G. Severity of illness and the weekend mortality effect: A retrospective cohort study. BMC Health Serv. Res. 2020, 20, 169. [Google Scholar] [CrossRef] [PubMed]
- Pauls, L.A.; Johnson-Paben, R.; McGready, J.; Murphy, J.D.; Pronovost, P.J.; Wu, C.L. The Weekend Effect in Hospitalized Patients: A Meta—Analysis. J. Hosp. Med. 2017, 12, 760–766. [Google Scholar] [CrossRef]
- Ruiz, M.; Bottle, A.; Aylin, P.P. The Global Comparators project: International comparison of 30-day in-hospital mortality by day of the week. BMJ Qual. Saf. 2015, 24, 492–504. [Google Scholar] [CrossRef]
- Chen, Y.-F.; Lilford, R.; Sutton, E.; Wu, C.-W.; Boyal, A.; Armoiry, X.; Gosling, A.; Cowley, N.; Watson, S.I.; Higenbottam, C.; et al. Magnitude and modifiers of the weekend effect in hospital admissions: A systematic review and meta-analysis. BMJ Open 2019, 9, e025764. [Google Scholar] [CrossRef]
- Mathew, A.; Potluri, R.; Fyyaz, S.A.; Carter, P.R. The enigma of the weekend effect. J. Thorac. Dis. 2018, 10, 102–105. [Google Scholar] [CrossRef]
- Aylin, P. Making sense of the evidence for the “weekend effect”. BMJ 2015, 351, h4652. [Google Scholar] [CrossRef] [PubMed]
- Freemantle, N.; Wood, J.; Keogh, B.; Ray, D.; Richardson, M.; Khosla, S.; Shahian, D.; Roche, W.; Stephens, I.; Pagano, D. Weekend hospitalization and additional risk of death: An analysis of inpatient data. J. R. Soc. Med. 2012, 105, 74–84. [Google Scholar] [CrossRef]
- Honeyford, K.; Cecil, E.; Lo, M.; Bottle, A.; Aylin, P. The weekend effect: Does hospital mortality differ by day of the week? A systematic review and meta-analysis. BMC Health Serv. Res. 2018, 18, 870. [Google Scholar] [CrossRef]
- Walker, A.S.; Stoesser, N.; Crook, D.W.; Wyllie, D.H.; Peto, T.E.A.; Finney, J.; Quan, T.P.; Fawcett, N.J.; Davies, J.; Watkinson, P.; et al. Mortality risks associated with emergency admissions during weekends and public holidays: An analysis of electronic health records. Lancet 2017, 390, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Girling, A.J.; Aldridge, C.; Evison, F.; Beet, C.; Boyal, A.; Rudge, G.; Lilford, R.J.; Bion, J. Sicker patients account for the weekend mortality effect among adult emergency admissions to a large hospital trust. BMJ Qual. Saf. 2019, 28, 223–230. [Google Scholar] [CrossRef]
- He, F.; Mnatzaganian, G.; Rutherford, D.; Njovu, M.; Blackberry, I. Weekend/holiday effect on stroke mortality in regional Australia: A ten-year retrospective study, J. Stroke Cerebrovasc. Dis. 2024, 33, 8. [Google Scholar] [CrossRef]
- Concha, O.P.; Gallego, B.; Hillman, K.; Delaney, G.P.; Coiera, E. Do variations in hospital mortality patterns after weekend admission reflect reduced quality of care or different patient cohorts? A population-based study. BMJ Qual. Saf. 2014, 23, 215–222. [Google Scholar] [CrossRef]
- Wiedermann, C.J.; Adami, M.; Wiedermann, W. Weekend effects on health outcomes and operational efficiency in emergency admissions to general medicine services of the Central Hospital of the Autonomous Province of Bolzano, Italy. Ann. Igiene 2018, 30, 245–250. [Google Scholar] [CrossRef]
- Mikulich, O.; Callaly, E.; Bennett, K.; Silke, B.; Directorate, S.J.H.M.; O’rIordan, D. The increased mortality associated with a weekend emergency admission is due to increased illness severity and altered case-mix. Acute Med. J. 2011, 10, 182–187. [Google Scholar] [CrossRef]
- Barba, R.; Losa, J.; Velasco, M.; Guijarro, C.; de Casasola, G.G.; Zapatero, A. Mortality among adult patients admitted to the hospital on weekends. Eur. J. Intern. Med. 2006, 17, 322–324. [Google Scholar] [CrossRef]
- Amigo, F.; Dalmau-Bueno, A.; García-Altés, A. Do hospitals have a higher mortality rate on weekend admissions? An observational study to analyse weekend effect on urgent admissions to hospitals in Catalonia. BMJ Open 2021, 11, e047836. [Google Scholar] [CrossRef]
- Neuraz, A.; Guérin, C.; Payet, C.; Polazzi, S.; Aubrun, F.; Dailler, F.; Lehot, J.J.; Piriou, V.; Neidecker, J.; Rimmelé, T.; et al. Patient Mortality Is Associated With Staff Resources and Workload in the ICU: A multicenter observational study. Crit. Care Med. 2015, 43, 1587–1594. [Google Scholar] [CrossRef]
- Eindhoven, D.; Van Erkelens, J.; Cannegieter, S.; Schalij, M.; Borleffs, C. 259 Mortality differences in acute myocardial infarction in the Netherlands: “The Weekend-effect”. Eur. Heart J. 2017, 38, ehx501.259. [Google Scholar] [CrossRef]
- Tolvi, M.; Haukka, J.; Aaltonen, L.-M.; Mattila, K.; Lehtonen, L. Weekend effect on mortality by medical specialty in six secondary hospitals in the Helsinki metropolitan area over a 14-year period. BMC Health Serv. Res. 2020, 20, 323. [Google Scholar] [CrossRef] [PubMed]
- Nijland, L.M.; Vrouenraets, B.C.; Kerkhoffs, G.M.; Ultee, J.M.; Karres, J.; Simons, A.E. The weekend effect for hip fracture surgery. Injury 2017, 48, 1536–1541. [Google Scholar] [CrossRef] [PubMed]
- Tolvi, M.; Mattila, K.; Haukka, J.; Aaltonen, L.-M.; Lehtonen, L. Analysis of weekend effect on mortality by medical specialty in Helsinki University Hospital over a 14-year period. Health Policy 2020, 124, 1209–1216. [Google Scholar] [CrossRef]
- Hansen, K.W.; Sørensen, R.; Abildstrøm, S.Z.; Madsen, M.; Hvelplund, A.; Madsen, J.K.; Jensen, J.S.; Galatius, S.; Prescott, E. Prognosis and treatment in patients admitted with acute myocardial infarction on weekends and weekdays from 1997 to 2009. Int. J. Cardiol. 2013, 168, 1167–1173. [Google Scholar] [CrossRef]
- Kristiansen, N.S.; Kristensen, P.K.; Nørgård, B.M.; Johnsen, S.P.; Mainz, J. Off-hours admission and quality of hip fracture care: A nationwide cohort study of performance measures and 30-day mortality. Int. J. Qual. Health Care 2016, 28, 324–331. [Google Scholar] [CrossRef]
- Vest-Hansen, B.; Riis, A.H.; Sørensen, H.T.; Christiansen, C.F. Out-of-hours and weekend admissions to Danish medical departments: Admission rates and 30-day mortality for 20 common medical conditions. BMJ Open 2015, 5, e006731. [Google Scholar] [CrossRef]
- Bała, M.M.; Koperny, M.; Stefanoff, P. In-hospital mortality in Poland: What can we learn from administrative data? Pol. Arch. Intern. Med. 2020, 130, 264–265. [Google Scholar] [CrossRef]
- Walicka, M.; Tuszyńska, A.; Czech, M.; Rutkowski, D.; Śliwczyński, A.; Brzozowska, M.; Jacyna, A.; Puzianowska-Kuźnicka, M.; Franek, E.; Chlebus, M. Predictors of in-hospital mortality in nonsurgical departments: A multivariable regression analysis of 2 855 029 hospitalizations. Pol. Arch. Intern. Med. 2020, 130, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Lipiński, M.; Rydzewska, G. Acute pancreatitis and the weekend effect: Does weekend admission affect patient out-come? Prz. Gastroenterol. 2020, 15, 241–246. [Google Scholar] [CrossRef]
- Brinzaniuc, K.; Stan, A.; Suciu, H.; Neagu, N.; Al Hussein, H.; Szabo, D.A.; Puscas, A.; Harpa, M.; Cristutiu, D.; Halic, M.N.; et al. Weekend Effect and Mortality Outcomes in Aortic Dissection: A Prospective Analysis. J. Crit. Care Med. 2024, 10, 158–167. [Google Scholar] [CrossRef]
- Ferenci, T.; Jánosi, A. Diurnal and seasonal patterns in the incidence and mortality of acute myocardial infarction in Hungary A nationwide, registry-based study. Orvosi Hetil. 2021, 162, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Angerer, S.; Buttinger, K.; Stummer, H. The weekend effect revisited: Evidence from the Upper Austrian stroke registry. Eur. J. Health Econ. 2019, 20, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Bray, B.D.; Cloud, G.C.; James, M.A.; Hemingway, H.; Paley, L.; Stewart, K.; Tyrrell, P.J.; Wolfe, C.D.; Rudd, A.G. Weekly variation in healthcare quality by day and time of admission: A nationwide, registry-based, prospective cohort study of acute stroke care. Lancet 2016, 388, 170–177. [Google Scholar] [CrossRef] [PubMed]
- INESS. SLOVENSKÉ ZDRAVOTNÍCTVO 2023–2030: PROBLÉMY A ICH ZLEPŠENIA. Available online: https://iness.sk/sites/default/files/documents/pdf/other/slovenske_zdravotnictvo_2023-2030_iness.pdf (accessed on 27 April 2025).
- Univerzitná nemocnica Bratislava. (n.d.). V. Interná Klinika LF UK a UNB. Available online: https://www.unb.sk/v-interna-klinika-lf-uk-a-unb/ (accessed on 24 April 2025).
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004; Available online: https://iris.who.int/handle/10665/42980 (accessed on 27 April 2025).
- Univerzitná Nemocnica Bratislava. Štatút Etickej Komisie Univerzitnej Nemocnice Bratislava; Univerzitná Nemocnica Bratislava: Bratislava, Slovakia, 2015. [Google Scholar]
- Aly, H. A closer look at the weekend effect and COVID-19 mortalities. J. Neonatal-Perinat. Med. 2021, 14, 7–8. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | Weekday Admissions | Weekend Admissions | p-Value |
|---|---|---|---|
| Age (mean) | 68.77 | 69.96 | <0.0001 |
| Sex (female) | 19,632 | 4035 | — |
| Sex (male) | 18,604 | 3684 | 0.139 |
| All Hospitalisations (Within 30 Days of Admission) | Males, n (%) | Females, n (%) | |
| Total (n, %) | 45,955 | 22,288 (48.5) | 23,667 (51.5) |
| Age, mean ± SD, (years) Median [IQR] | 69.0 ± 16.2 72.1 [60.2–81.2] | 66.1 ± 15.9 66.1 [56.8–78.4] | 71.6 ± 16.0 70.4 [63.4–81.9] |
| LOS, mean ± SD, (days) Median [IQR] | 6.1 ± 5.2 5 [2–8] | 6.1 ± 5.3 5 [2–8] | 6.1 ± 5.1 5 [2–8] |
| Mon | 8351 (18.2) | 4039 (18.1) | 4312 (18.2) |
| Tue | 8182 (17.8) | 4049 (18.2) | 4133 (17.5) |
| Wed | 7271 (15.8) | 3536 (15.9) | 3735 (15.8) |
| Thu | 7925 (17.2) | 3894 (17.5) | 4031 (17.0) |
| Fri | 6507 (14.2) | 3086 (13.8) | 3421 (14.5) |
| Subtotal for Weekdays | 38,236 | 18,604 | 19,632 |
| Sat | 3794 (8.3) | 1772 (8.0) | 2022 (8.5) |
| Sun | 3925 (8.5) | 1912 (8.6) | 2013 (8.5) |
| Subtotal for Weekend | 7719 | 3684 | 4035 |
| In-Hospital Deaths (Within 30 Days of Admission) | Males, n (%) | Females, n (%) | |
| Total (n, %) | 5205 | 2491 (47.9) | 2714 (52.1) |
| Age, mean ± SD, (years) Median [IQR] | 77.0 ± 11.8 79.2 [70.1–85.8] | 74.6 ± 12.0 76.0 [67.1–83.5] | 79.2 ± 11.2 81.6 [73.2–87.1] |
| LOS, mean ± SD, (days) Median [IQR] | 6.5 ± 6.6 4 [1–10] | 6.7 ± 6.7 4 [1–10] | 6.4 ± 6.6 4 [1–10] |
| Mon | 809 (15.5) | 378 (15.2) | 431 (15.9) |
| Tue | 809 (15.5) | 383 (15.4) | 426 (15.7) |
| Wed | 768 (14.8) | 390 (15.7) | 378 (13.9) |
| Thu | 806 (15.5) | 385 (15.5) | 421 (15.5) |
| Fri | 810 (15.6) | 373 (15.0) | 437 (16.1) |
| Subtotal for Weekdays | 4002 | 1909 | 2093 |
| Sat | 585 (11.2) | 298 (12.0) | 287 (10.6) |
| Sun | 618 (11.9) | 284 (11.4) | 334 (12.3) |
| Subtotal for Weekend | 1203 | 582 | 621 |
| Admission Type | Weekday Admissions | Weekend Admissions | Total |
|---|---|---|---|
| Total admissions (n) | 38,236 | 7719 | 45,955 |
| In-hospital deaths (n) | 4002 | 1203 | 5205 |
| Mortality rate (%) | 10.47% | 15.58% | 11.32% |
| Chi-square (χ2) | 148.55 | ||
| p-value | <0.0001 | ||
| Risk difference | +5.12 | ||
| Relative risk | 1.49 | ||
| Odds ratio (unadjusted) | 1.58 | ||
| Year | Weekday Admissions (n) | Weekday Deaths (n) | Weekday Mortality Rate (%) | 95% CI | Weekend Admissions (n) | Weekend Deaths (n) | Weekend Mortality Rate (%) | 95% CI |
|---|---|---|---|---|---|---|---|---|
| 2010 | 3077 | 289 | 9.4% | 8.41–10.47% | 596 | 88 | 14.8% | 12.14–17.84% |
| 2011 | 3228 | 298 | 9.2% | 8.28–10.28% | 636 | 90 | 14.2% | 11.66–17.08% |
| 2012 | 3377 | 248 | 7.3% | 6.51–8.27% | 618 | 63 | 10.2% | 8.05–12.83% |
| 2013 | 3508 | 330 | 9.4% | 8.48–10.42% | 658 | 88 | 13.4% | 10.98–16.19% |
| 2014 | 3529 | 296 | 8.4% | 7.52–9.35% | 689 | 92 | 13.4% | 11.01–16.10% |
| 2015 | 3517 | 294 | 8.4% | 7.50–9.31% | 698 | 85 | 12.2% | 9.96–14.83% |
| 2016 | 3276 | 275 | 8.4% | 7.45–9.44% | 604 | 89 | 14.7% | 12.24–17.66% |
| 2017 | 3251 | 370 | 11.4% | 10.30–12.55% | 618 | 102 | 16.5% | 13.80–19.60% |
| 2018 | 2336 | 340 | 14.6% | 13.08–16.16% | 482 | 91 | 18.9% | 15.47–22.83% |
| 2019 | 2891 | 299 | 10.3% | 9.22–11.60% | 569 | 69 | 12.1% | 9.57–15.22% |
| 2020 | 2263 | 310 | 13.7% | 12.28–15.25% | 520 | 106 | 20.4% | 17.08–24.10% |
| 2021 | 1934 | 340 | 17.6% | 15.93–19.38% | 519 | 133 | 25.6% | 22.01–29.60% |
| 2022 | 2041 | 313 | 15.3% | 13.77–17.03% | 511 | 107 | 20.9% | 17.66–24.60% |
| Factor | AOR (Adjusted Odds Ratio) | Lower CI | Upper CI | Statistical Significance (p-Value) |
|---|---|---|---|---|
| Weekend admission | 1.31 | 1.22 | 1.41 | <0.001 |
| Age ≥ 65 | 2.88 | 2.73 | 3.05 | <0.001 |
| Male gender | 1.37 | 1.28 | 1.47 | <0.001 |
| Re-hospitalisation | 1 | 0.96 | 1.05 | 0.87 |
| Length of stay | 1.05 | 0.98 | 1.12 | 0.18 |
| Interaction Term | AOR | Lower CI | Upper CI | p-Value |
|---|---|---|---|---|
| Weekend × Age | 1.02 | 0.97 | 1.07 | 0.312 |
| Age < 65 (stratified) | 1.34 | - | - | - |
| Age ≥ 65 (stratified) | 1.60 | - | - | - |
| Weekend × Gender | 1.05 | 0.99 | 1.11 | 0.215 |
| Cause of Death | n (%) | Male, n (%) | Age, Mean ± SD (Years) | LOS ± SD (Days) | Weekday Deaths (n) | Weekend Deaths (n) | p-Value |
|---|---|---|---|---|---|---|---|
| Total deaths | 5205 | 2491 | 77.0 ± 11.8 | 6.5 ± 6.6 | 4002 | 1203 | - |
| Cardiovascular | 3664 (70.4) | 1734 (69.6) | 77.0 ± 11.3 | 6.5 ± 6.6 | 2811 (70.2) | 853 (70.9) | 0.683 |
| Respiratory | 701 (13.5) | 332 (13.3) | 77.9 ± 11.6 | 7.0 ± 6.8 | 543 (13.6) | 158 (13.1) | 0.735 |
| Sepsis and other infectious | 265 (5.1) | 137 (5.5) | 77.4 ± 11.0 | 6.7 ± 6.8 | 205 (5.1) | 59 (4.9) | 0.820 |
| Digestive | 162 (3.1) | 104 (4.2) | 64.0 ± 13.1 | 8.0 ± 7.5 | 129 (3.2) | 33 (2.7) | 0.455 |
| Cardiogenic shock | 138 (2.7) | 74 (3.0) | 73.9 ± 14.3 | 3.7 ± 5.3 | 105 (2.6) | 33 (2.7) | 0.901 |
| Malignancy | 121 (2.3) | 47 (1.9) | 71.7 ± 11.6 | 8.7 ± 7.8 | 94 (2.3) | 28 (2.3) | 0.968 |
| Endocrinous | 69 (1.3) | 27 (1.1) | 75.7 ± 11.4 | 4.6 ± 5.2 | 47 (1.2) | 22 (1.8) | 0.301 |
| Urogenital | 45 (0.9) | 21 (0.8) | 78.5 ± 9.5 | 5.2 ± 5.2 | 37 (0.9) | 8 (0.7) | 0.106 |
| Other | 40 (0.7) | 15 (0.6) | 73.0 ± 13.7 | 6.1 ± 5.2 | 30 (0.7) | 0 (0) | 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrubá, O.; Žigová, L.; Hrončová, M.; Valášková, S.; Smaha, J.; Jackuliak, P.; Kužma, M.; Mayer, A.; Dukat, A.; Payer, J.; et al. The Weekend Effect on In-Hospital Mortality—First 13-Year Retrospective Observational Study in Slovakia. Healthcare 2025, 13, 1412. https://doi.org/10.3390/healthcare13121412
Hrubá O, Žigová L, Hrončová M, Valášková S, Smaha J, Jackuliak P, Kužma M, Mayer A, Dukat A, Payer J, et al. The Weekend Effect on In-Hospital Mortality—First 13-Year Retrospective Observational Study in Slovakia. Healthcare. 2025; 13(12):1412. https://doi.org/10.3390/healthcare13121412
Chicago/Turabian StyleHrubá, Orsolya, Lucia Žigová, Michala Hrončová, Simona Valášková, Juraj Smaha, Peter Jackuliak, Martin Kužma, Alexander Mayer, Andrej Dukat, Juraj Payer, and et al. 2025. "The Weekend Effect on In-Hospital Mortality—First 13-Year Retrospective Observational Study in Slovakia" Healthcare 13, no. 12: 1412. https://doi.org/10.3390/healthcare13121412
APA StyleHrubá, O., Žigová, L., Hrončová, M., Valášková, S., Smaha, J., Jackuliak, P., Kužma, M., Mayer, A., Dukat, A., Payer, J., Kyselovic, J., & Gažová, A. (2025). The Weekend Effect on In-Hospital Mortality—First 13-Year Retrospective Observational Study in Slovakia. Healthcare, 13(12), 1412. https://doi.org/10.3390/healthcare13121412