
Effect of Manual Massage, Foam Rolling, and Strength Training on Hemodynamic and Autonomic Responses in Adults: A Scoping Review

 ,
,  ,
,  , , ,
, , ,  ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Stage 1: Identification of Relevant Studies
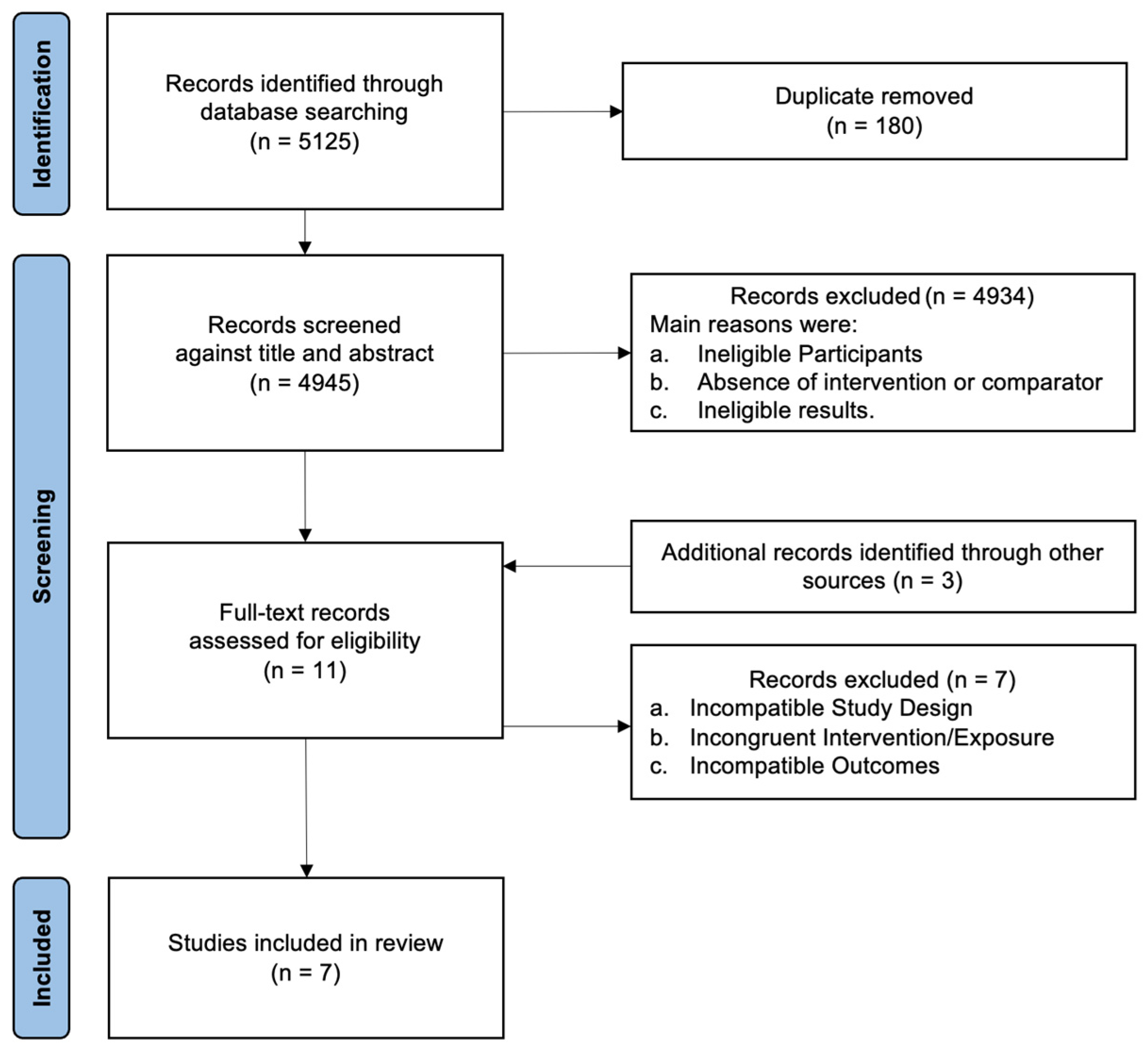
2.2. Stage 2: Study Selection
2.3. Stage 3: Data Mapping
2.4. Stage 4: Gathering, Summarizing, and Reporting the Results
3. Results
3.1. Study Quality
3.2. FR Alone
3.3. MM Alone
3.4. Combined Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BP | Blood pressure |
| PEH | Post-exercise hypotension |
| ST | Strength training |
| SBP | Systolic blood pressure |
| DBP | Diastolic blood pressure |
| MM | Manual massage |
| FR | Foam rolling |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews |
| CINAHL | Nursing and Allied Health |
| SS | Static stretching |
References
- Schiffrin, E.L. Immune mechanisms in hypertension and vascular injury. Clin. Sci. 2014, 126, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Hilmmerfab, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCN. A Guideline for the Prevention, Detection, Evaluation, and Management of high blood pressure in adults: Executive summary. A report of the American College of Cardiology/American Heart Association, Task Force on Clinical Practice Guidelines. Circulation 2018, 138, 426–483. [Google Scholar]
- Macdonald, H.V.; Johnson, B.T.; Huedo-Medina, T.B.; Livingston, J.; Forsyth, K.C.; Kraemer, W.J. Dynamic resistance training as stand-alone antihypertensive lifestyle therapy: A meta-analysis. J. Am. Heart Assoc. 2016, 5, e003231. [Google Scholar] [CrossRef]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Keaney, P.M.; Reynolds, K.; Chen, J.; He, J. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 countries. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Appes, L.J.; Rubenfire, M.; Ogedegbe, G.; Bisognano, J.D.; Elliott, W.J.; Fuchs, F.D.; Hughes, J.W.; Lacland, D.T.; Staffileno, B.A.; et al. Beyond medications and diet: Alternative approaches to lowering blood pressure: A scientific statement from the American Heart Association. Hypertension 2013, 61, 1360–1383. [Google Scholar] [CrossRef]
- Arnett, D.D.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J. ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar]
- Pescatello, L.S.; Buchner, D.M.; Jakicic, J.M.; Powell, K.E.; Kraus, W.E.; Bloodgood, B.; Campbell, W.W.; Dietz, S.; Dipietro, L.; George, S.M.; et al. Physical activity to prevent and treat hypertension: A systematic review. Med. Sci. Sports Exerc. 2019, 51, 1314–1323. [Google Scholar] [CrossRef]
- Fidalgo, A.S.F.; Farinatti, P.; Borges, J.P.; De Paula, T.; Monteiro, W. Institutional Guidelines for Resistance Exercise Training in Cardiovascular Disease: A Systematic Review. Sports Med. 2019, 49, 463–475. [Google Scholar] [CrossRef]
- Casonatto, J.; Goessler, K.F.; Cornelissen, V.A.; Cardoso, J.R.; Polito, M.D. The blood pressure-lowering effect of a single bout of resistance exercise: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Prev. Cardiol. 2016, 23, 1700–1714. [Google Scholar] [CrossRef]
- Hotfiel, T.; Swoboda, B.; Krinner, S.; Grim, C.; Engelhardt, M.; Uder, M.; Heiss, R.U. Acute effects of lateral thigh foam rolling on arterial tissue perfusion determined by spectral doppler and power doppler ultrasound. J. Strength. Cond. Res. 2017, 31, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Masuhara, M.; Ikuta, K. Acute effects of self-myofascial release using a foam roller on arterial function. J. Strength. Cond. Res. 2014, 28, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Liao, I.C.; Chen, S.L.; Wang, M.Y.; Tsai, P.S. Effects of massage on blood pressure in patients with hypertension and prehypertension: A meta-analysis of randomized controlled trials. J. Cardiovasc. Nurs. 2016, 31, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Beardsley, C.; Škarabot, J. Effects of self-myofascial release: A systematic review. J. Bodyw. Mov. Ther. 2015, 19, 747–758. [Google Scholar] [CrossRef]
- Fisher, M.M. The effect of resistance exercise on recovery blood pressure in normotensive and borderline hypertensive women. J. Strength. Cond. Res. 2001, 15, 210–216. [Google Scholar]
- Figueiredo, T.; Willardson, J.M.; Miranda, H.; Bentes, C.M.; Reis, V.M.; De Salles, B.F.; Simão, R. Influence of rest interval length between sets on blood pressure and heart rate variability after a strength training session performed by pre hypertensive men. J. Strength. Cond. Res. 2016, 30, 1813–1824. [Google Scholar] [CrossRef]
- Mayo, J.J.; Kravitz, L. A Review of the Acute Cardiovascular Responses to Resistance Exercise of Healthy Young and Older Adults. J. Strength. Cond. Res. 1999, 13, 90–96. [Google Scholar]
- Nobrega, A.C.; O′Leary, D.; Silva, B.M.; Marongiu, E.; Piepoli, M.F.; Crisafulli, A. Neural Regulation of Cardiovascular Response to Exercise: Role of Central Command and Peripheral Afferents. BioMed Res. Int. 2014, 2014, 478965. [Google Scholar] [CrossRef]
- Gladwell, V.F.; Coote, J.H. Heart rate at the onset of muscle contraction and during passive muscle stretch in humans: A role for mechanoreceptors. J. Physiol. 2002, 540, 1095–1102. [Google Scholar] [CrossRef]
- Inami, T.; Bara, R.; Nakagari, A.; Shimizu, T. Acute changes in peripheral vascular tonus and systemic circulation during static stretching. Res. Sports Med. 2015, 23, 167–178. [Google Scholar] [CrossRef]
- Monteiro, E.R.; Pescatello, L.S.; Winchester, J.B.; Corrêa Neto, V.G.; Brown, A.F.; Budde, H.; Marchetti, P.H.; Silva, J.G.; Vianna, J.M.; Novaes, J.S. Effects of manual therapies and resistance exercise on postexercise hypotension in women with normal blood pressure. J. Strength. Cond. Res. 2022, 36, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Brown, P.; Brunnhuber, K.; Chalkidou, K.; Chalmers, I.; Clarke, M.; Fenton, M.; Forbes, C.; Glanville, J.; Hickes, N.J.; Moody, J.; et al. How to formulate research recommendations. BMJ 2006, 333, 804–806. [Google Scholar] [CrossRef]
- Center for Evidence-Based Physiotherapy. Physiotherapy Evidence Database (PEDro). 2024. Available online: https://pedro.org.au/english/resources/pedro-scale/ (accessed on 29 January 2025).
- Lastova, K.; Nordvall, M.; Walters-Edwards, M.; Allnutt, A.; Wong, A. Cardiac autonomic and blood pressure responses to an acute foam rolling session. J. Strength. Cond. Res. 2018, 32, 2825–2830. [Google Scholar] [CrossRef]
- Monteiro, E.R.; Vingren, J.L.; Pescatello, L.S.; Corrêa Neto, V.G.; Brown, A.F.; Kingsley, J.D.; Silva, J.G.; Vianna, J.M.; Novaes, J.S. Effects of foam rolling and strength training on post exercise hypotension in normotensive women: A cross-over study. J. Bodyw. Mov. Ther. 2023, 34, 81–86. [Google Scholar] [CrossRef]
- Monteiro, E.R.; Pescatello, L.S.; Leitão, L.; De Miranda, M.J.C.; Marchetti, P.H.; Novaes, M.R.; Araújo, G.S.; Corrêa Neto, V.G.; Novaes, J.S. Muscular Performance and Blood Pressure After Different Pre-Strength Training Strategies in Recreationally Strength-Trained Women: Cross-Over Trial. J. Cardiovasc. Dev. Dis. 2025, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Ketelhut, S.; Oechslin, L.; Zehnder, C.; Kubica, C.; Nigg, C.R. Acute self-myofascial release modulates cardiac autonomic function and hemodynamic parameters at rest and reduces cardiovascular stress reaction. Eur. J. Appl. Physiol. 2024, 124, 1535–1545. [Google Scholar] [CrossRef]
- Walaszek, R. Impact of classic massage on blood pressure in patients with clinically diagnosed hypertension. J. Tradit. Chin. Med. 2015, 35, 396–401. [Google Scholar] [CrossRef]
- Givi, M.; Sadeghi, M.; Garakyaragui, M.; Eshghinezhad, A.; Moeini, M.; Ghasempour, Z. Long-term effect of massage therapy on blood pressure prehypertensive women. J. Educ. Health Promot. 2018, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Berkley, K.J.; Hubscher, C.H. Are there separate central nervous system pathways for touch and pain? Nat. Med. 1995, 1, 766–773. [Google Scholar] [CrossRef]
- McGlone, F.; Valbo, A.B.; Olausson, H.; Loken, L.; Wessberg, J. Discriminative touch and emotional touch. Can. J. Exp. Psychol. 2007, 61, 173–183. [Google Scholar] [CrossRef]
- Preusser, S.; Thiel, S.D.; Rook, C.; Roggenhofer, E.; Kosatschek, A.; Draganski, B.; Blankenburg, F.; Driver, J.; Villringer, A.; Pleger, B. The perception of touch and the ventral somatosensory pathway. Brain 2015, 138, 540–548. [Google Scholar] [CrossRef]
- White, D.W.; Raven, P.B. Autonomic neural control of heart rate during dynamic exercise: Revisited. J. Physiol. 2014, 592, 2491–2500. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Araújo, G.; Behm, D.G.; Monteiro, E.R.; De Melo Fiuza, A.G.F.; Gomes, T.M.; Vianna, J.M.; Reis, M.S.; Novaes, J.S. Order effects of resistance and stretching exercises on heart rate variability and blood pressure in healthy adults. J. Strength. Cond. Res. 2019, 33, 2684–2693. [Google Scholar] [CrossRef]
- Souza, A.C.; Gomes, T.M.; Sousa, M.S.; Saraiva, A.R.; Araújo, S.A.; Figueiredo, T.; Novaes, J.S. Static stretch performed after strength training session induces hypotensive response in trained men. J. Strength. Cond. Res. 2019, 33, 2981–2990. [Google Scholar] [CrossRef]
- Kruse, N.T.; Scheuermann, B.W. Cardiovascular responses to skeletal muscle stretching: “stretching” the truth or a new exercise paradigm for cardiovascular medicine? Sports Med. 2017, 47, 2507–2520. [Google Scholar] [CrossRef]

{kind=link}
| Studies | Sample Size (n = 95) | Sex | Age (Years) | Height | Body Mass (kg) | Training Status |
|---|---|---|---|---|---|---|
| Okamoto et al. [12] | 10 (7 men and 3 women) | Both sexes | 19.9 ± 0.3 | 162.7 ± 8.1 cm | 60.6 ± 11.2 | Recreational strength training |
| Hotfiel et al. [11] | 21 (12 men and 9 women) | Both sexes | 25 ± 2 | 177 ± 9 cm | 74 ± 9 | Recreational strength training |
| Lastova et al. [27] | 15 (8 men and 7 women) | Both sexes | 21.55 ± 0.52 | 1.72 ± 0.02 m | 74.79 ± 2.88 | N/A |
| Monteiro et al. [21] | 16 | Women | 25.1 ± 2.9 | 158.9 ± 4.1 cm | 59.5 ± 4.9 | Recreational strength training |
| Monteiro et al. [28] | 16 | Women | 25.5 ± 2.0 | 155.7 ± 4.4 cm | 61.2 ± 5.4 | Recreational strength training |
| Monteiro et al. [29] | 12 | Women | 27.2 ± 3.3 | 164.8 ± 5.5 cm | 69.8 ± 6.0 | Recreational strength training |
| Ketelhut et al. [30] | 20 | Men | 26 ± 2 | 182.6 ± 6.9 | 76.1 ± 7.2 | N/A |
| Studies | Objective | Interventions | Results | |
|---|---|---|---|---|
| Okamoto et al. [12] | To investigate the acute effect of FR on arterial stiffness and vascular endothelial function. | FR | FR condition was performed on the adductors, hamstrings, quadriceps, iliotibial band, and trapezius regions. Each participant practiced 2 or 3 times to learn the correct FR technique with the guidance of a coach and performed 20 repetitions in each region with 1 min intervals. The pressure was self-adjusted by applying body weight to the roller and using hands and feet to regulate pressure as needed. The roller was placed under the target tissue area, and the body was moved back and forth along the roller. | ↓ Ankle-brachial PWV (from 1202 ± 105 to 1074 ± 110 cm/s). ↑ Plasma nitric oxide concentration (from 20.4 ± 6.9 to 34.4 ± 17.2 μmol/L). Both after FR (p < 0.05), but neither of them differed significantly after the control condition. |
| CON | Rest in lying position in a quiet temperature-controlled room. | |||
| Hotfiel et al. [11] | To evaluate the effect of FR on arterial blood flow in the lateral thigh region. | ST + FR | The exercise protocol consisted of 3 sets, each with 45 s of FR on the lateral thigh region in the sagittal plane (with 20 s of rest between sets). | ↑ Arterial blood flow of the lateral thigh increased significantly after FR exercises compared with baseline (p ≤ 0.05). ↑ Vmax of 73.6% (0 min) and 52.7% (30 min) (p < 0.001), in TAMx of 53.2% (p < 0.001) and 38.3% (p = 0.002), and in TAMn of 84.4% (p < 0.001) and 68.2% (p < 0.001). |
| Lastova et al. [27] | To assess the effects of an acute FR session on HRV and BP in healthy individuals. | FR | In the FR condition, individuals completed 10 repetitions of FR per target area of the body (adductors, hamstrings, quadriceps, iliotibial band, gastrocnemius, and upper trapezius), followed by 1 min of rest. Each repetition involved moving the target tissue across the roller in a smooth motion at a rate of 2 s down and 2 s up, as determined by a metronome. | ↑ in vagal tone index (normalized high-frequency power) 30-min after FR (p < 0.01), while no changes were observed after the control condition. ↓ sympathetic activity (p < 0.05) (normalized low-frequency power) and sympathovagal balance (normalized low-frequency to high-frequency ratio). |
| CON | The control condition only involved measurements without the application of other experimental conditions. | |||
| Monteiro et al. [21] | To examine the acute effects of resistance exercise and different manual therapies (SS and MM) performed separately or combined on BP responses during recovery in normotensive women. | MM | The isolated SS and isolated MM conditions were applied unilaterally in two sets of 120 s for each quadriceps, hamstrings, and calf region. | ↓ Systolic BP in isolated strength training at Post-50 (p = 0.038; d = −2.24; ∆ = −4.0 mmHg), isolated SS at Post−50 (p = 0.021; d = −2.67; ∆ = −5.0 mmHg), and Post-60 (p = 0.008; d = −2.88; ∆ = −5.0 mmHg), and isolated MM at Post-50 (p = 0.011; d = −2.61; ∆ = −4.0 mmHg) and Post-60 (p = 0.011; d = −2.74; ∆ = −4.0 mmHg). ↓ Systolic BP in the combined of strength training and SS at Post-60 (p = 0.024; d = −3.12; ∆ = −5.0 mmHg). |
| SS | The isolated SS and isolated MM conditions were applied unilaterally in two sets of 120 s for each quadriceps, hamstrings, and calf region. | |||
| ST | Isolated strength training comprised three sets of bench press, back squat, and leg press at an intensity controlled to 80% of 10RM. | |||
| ST + MM | In the combined condition of strength training and MM, the massage was conducted immediately after strength training, following the same descriptions as above. | |||
| ST + SS | In the combined condition of strength training and SS, SS was performed immediately after strength training, following the same descriptions as above. | |||
| CON | The control condition consisted solely of measurements without applying any other experimental conditions. | |||
| Monteiro et al. [28] | Toexamine the acute effects of resistance exercise and FR performed separately or combined on BP responses during recovery in normotensive women. | FR | In the isolated FR condition, foam rolling was performed unilaterally in two sets of 120 s for each quadriceps, hamstrings, and calf region. | ↓ Systolic BP in isolated strength training at Post-50 (p < 0.001; d = −2.14) and Post-60 (p = 0.008; d = −2.88), and in isolated FR at Post-60 (p = 0.020; d = −2.14). ↓ Systolic BP in the combined condition of strength training and FR at Post-50 (p = 0.001; d = −2.03) and Post-60 (p < 0.001; d = −2.38). |
| ST | Isolated strength training comprised three sets of bench press, back squat, lateral pulldown, and leg press at an intensity controlled to 80% of 10RM. | |||
| ST + FR | In the combined condition of strength training and FR, FR was conducted immediately after strength training, following the same descriptions as above. | |||
| CON | The control condition consisted solely of measurements without applying any other experimental conditions. | |||
| Monteiro et al. [29] | To examine the acute effects of different pre-strength training strategies on total training volume, maximum repetition performance, fatigue index, and blood pressure responses in recreationally strength-trained women. | 10RM test and retest for bench press 45°, front squat, lat pulldown, leg press, shoulder press, and leg extension. Strength Training = 80% of 10RM load with self-suggested rest interval. FR and SS = Applied, unilaterally, in randomized order, in single set of 90 s to the lateral torso of the trunk, anterior and posterior thigh, and calf regions. Aerobic Exercise = Walking on the treadmill with intensity between 30% and 60% of the heart rate reserve. Specific Warm-Up = Two sets of 15 repetitions with 40%10RM with 90 s rest interval. BP was measured at baseline, Post-10, Post-20, Post-30, Post-40, Post-50, and Post-60 min. | No significant reductions were observed for systolic and diastolic BP with effect sizes magnitude ranging between trivial and large. | |
| Ketelhut et al. [30] | To evaluate the immediate effects of acute self-myofascial release on peripheral and central BP, HR, HRV, TPR, and PWV. Investigate whether self-myofascial release can influence hemodynamic reactivity and perceived pain during a cold pressor test. | FR Self-myofascial release was performed by two sets of 60 s with a 60 s rest interval between sets, targeting the calf, outer thigh, front thigh, inner thigh, and buttocks muscles regions. Hemodynamic and cardiac autonomic parameters were evaluated at rest (t0) and during a cold pressor test (CPT_t0). Following this, participants either engaged in a 20 min SMR exercise or a 20 min seated rest (CON). After each condition, outcomes were assessed again at rest (t1) and during a cold pressor test 2 min after the condition (CPT_t1), as well as after a 20 min period of supine rest (t2, CPT_t2). | ↓ Diastolic BP (p < 0.001) from t0 to t2 compared to the control condition (p < 0.001), resulting in a significantly lower at t2 (p = 0.027). ↓ Diastolic BP (p < 0.001) from t0 to t2 following the self-myofascial release (p < 0.001). This resulted in a significantly lower at t2 (p = 0.030). ↓ TPR from t0 to t2 (p = 0.017), resulting in a significantly lower TPR at t2 (p = 0.024). No time × condition interaction effects could be observed for systolic BP, PWV, and HRV (LF/HF parameters) (p > 0.05). ↓ HR (p = 0.043) from t0 to t1 (p 0.017), leading to a lower HR at t1 (p < 0.001) and t2 (p = 0.007). ↑ HRV (RMSSD index) from t0 to t1 was detected following the control condition (p = 0.047), leading to a significantly lower value after the control condition at t1 (p = 0.006). | |
| Studies | Eligibility Criteria | Random Allocation | Concealed Allocation | Baseline Comparability | Blind Subjects | Blind Therapists | Blind Assessors | Adequate Follow-Up | Intention-to-Treat Analysis | Between-Group Comparisons | Point Estimates and Variability |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Okamoto et al. [12] | No | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes |
| Hotfiel et al. [11] | No | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes |
| Lastova et al. [27] | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes |
| Monteiro et al. [21] | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes |
| Monteiro et al. [28] | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes |
| Monteiro et al. [29] | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes |
| Ketelhut et al. [30] | Yes | Yes | Yes | Yes | Yes | No | No | Yes | No | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monteiro, E.R.; Aguilera, L.M.; Ruá-Alonso, M.; Araújo, G.d.S.; Corrêa Neto, V.G.; Bentes, C.M.; Vilaça-Alves, J.; Reis, V.M.; Ferreira, A.d.S.; Marchetti, P.H.; et al. Effect of Manual Massage, Foam Rolling, and Strength Training on Hemodynamic and Autonomic Responses in Adults: A Scoping Review. Healthcare 2025, 13, 1371. https://doi.org/10.3390/healthcare13121371
Monteiro ER, Aguilera LM, Ruá-Alonso M, Araújo GdS, Corrêa Neto VG, Bentes CM, Vilaça-Alves J, Reis VM, Ferreira AdS, Marchetti PH, et al. Effect of Manual Massage, Foam Rolling, and Strength Training on Hemodynamic and Autonomic Responses in Adults: A Scoping Review. Healthcare. 2025; 13(12):1371. https://doi.org/10.3390/healthcare13121371
Chicago/Turabian StyleMonteiro, Estêvão Rios, Lavínia Martins Aguilera, Maria Ruá-Alonso, Gleisson da Silva Araújo, Victor Gonçalves Corrêa Neto, Cláudio Melibeu Bentes, José Vilaça-Alves, Victor Machado Reis, Arthur de Sá Ferreira, Paulo H. Marchetti, and et al. 2025. "Effect of Manual Massage, Foam Rolling, and Strength Training on Hemodynamic and Autonomic Responses in Adults: A Scoping Review" Healthcare 13, no. 12: 1371. https://doi.org/10.3390/healthcare13121371
APA StyleMonteiro, E. R., Aguilera, L. M., Ruá-Alonso, M., Araújo, G. d. S., Corrêa Neto, V. G., Bentes, C. M., Vilaça-Alves, J., Reis, V. M., Ferreira, A. d. S., Marchetti, P. H., & da Silva Novaes, J. (2025). Effect of Manual Massage, Foam Rolling, and Strength Training on Hemodynamic and Autonomic Responses in Adults: A Scoping Review. Healthcare, 13(12), 1371. https://doi.org/10.3390/healthcare13121371