
Five-Year Trends in SSRI Consumption: A Precision Medicine Approach to Comparative Analysis Between Serbia and European Countries



Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DDD | Defined daily doses |
| DDD/TID | Defined daily doses per 1000 inhabitants per day |
References
- Wu, Y.; Wang, L.; Tao, M.; Cao, H.; Yuan, H.; Ye, M.; Chen, X.; Wang, K.; Zhu, C. Changing Trends in the Global Burden of Mental Disorders from 1990 to 2019 and Predicted Levels in 25 Years. Epidemiol. Psychiatr. Sci. 2023, 32, e63. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Kalin, N.H. The Critical Relationship between Anxiety and Depression. Am. J. Psychiatry 2020, 177, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the True Global Burden of Mental Illness. Lancet Psychiatry 2016, 3, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Hock, R.S.; Or, F.; Kolappa, K.; Burkey, M.D.; Surkan, P.J.; Eaton, W.W. A New Resolution for Global Mental Health. Lancet 2012, 379, 1367–1368. [Google Scholar] [CrossRef]
- Jha, P.; Subedi, S.; Paudyal, S.; Panta, P.P. Suicidal Attempt among Psychiatry Patients Presented to the Department of Emergency of a Tertiary Care Centre: A Descriptive Cross-Sectional Study. JNMA J. Nepal Med. Assoc. 2023, 61, 442–445. [Google Scholar] [CrossRef]
- Alshaya, D.S. Genetic and Epigenetic Factors Associated with Depression: An Updated Overview. Saudi J. Biol. Sci. 2022, 29, 103311. [Google Scholar] [CrossRef]
- Javaid, S.F.; Hashim, I.J.; Hashim, M.J.; Stip, E.; Samad, M.A.; Ahbabi, A.A. Epidemiology of Anxiety Disorders: Global Burden and Sociodemographic Associations. Middle East Curr. Psychiatry 2023, 30, 44. [Google Scholar] [CrossRef]
- Luft, M.J.; Lamy, M.; DelBello, M.P.; McNamara, R.K.; Strawn, J.R. Antidepressant-Induced Activation in Children and Adolescents: Risk, Recognition and Management. Curr. Probl. Pediatr. Adolesc. Health Care 2018, 48, 50–62. [Google Scholar] [CrossRef]
- Gabriel, M.; Sharma, V. Antidepressant Discontinuation Syndrome. Can. Med Assoc. J. 2017, 189, E747. [Google Scholar] [CrossRef]
- Jing, E.; Straw-Wilson, K. Sexual Dysfunction in Selective Serotonin Reuptake Inhibitors (SSRIs) and Potential Solutions: A Narrative Literature Review. Ment. Health Clin. 2016, 6, 191–196. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, Y.; Yang, L.; Zhang, K.; Li, S. Safety Profile of Selective Serotonin Reuptake Inhibitors in Real-World Settings: A Pharmacovigilance Study Based on FDA Adverse Event Reporting System. Ann. Pharmacother. 2024, 58, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, N.; Damkier, P.; Pedersen, S.A. Serotonin Syndrome-A Focused Review. Basic Clin. Pharmacol. Toxicol. 2023, 133, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Grimsley, S.R.; Jann, M.W. Paroxetine, Sertraline, and Fluvoxamine: New Selective Serotonin Reuptake Inhibitors. Clin. Pharm. 1992, 11, 930–957. [Google Scholar] [PubMed]
- Nawaz, A.; Mamoon, B.; Batool, T.E.; Khattak, M.I.; Amir, F.; Akbar, A.; Khan, S. Advances in Antidepressant Therapy: Comparing the Efficacy of Selective Serotonin Reuptake Inhibitors (SSRIs), Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs), and Novel Agents. Cureus 2024, 16, e76318. [Google Scholar] [CrossRef]
- Milijašević, B.Ž.; Vlajankov, A.L.; Ubavić, M.B.; Rašković, A.L.; Martić, N.B.; Tomić, Z.S. Analysis of Antidepressant Use in Republic of Serbia from 2013 to 2015. Hosp. Pharmacol.-Int. Multidiscip. J. 2018, 5, 607–616. [Google Scholar] [CrossRef]
- Muijsers, R.B.R.; Plosker, G.L.; Noble, S. Spotlight on Sertraline in the Management of Major Depressive Disorder in Elderly Patients. CNS Drugs 2002, 16, 789–794. [Google Scholar] [CrossRef]
- Dwyer, J.B.; Bloch, M.H. Antidepressants for Pediatric Patients. Curr. Psychiatr. 2019, 18, 26–42. [Google Scholar]
- Pinheiro, E.; Bogen, D.L.; Hoxha, D.; Ciolino, J.D.; Wisner, K.L. Sertraline and Breastfeeding: Review and Meta-Analysis. Arch. Womens Ment. Health 2015, 18, 139–146. [Google Scholar] [CrossRef]
- Cuomo, A.; Maina, G.; Neal, S.M.; De Montis, G.; Rosso, G.; Scheggi, S.; Beccarini Crescenzi, B.; Bolognesi, S.; Goracci, A.; Coluccia, A.; et al. Using Sertraline in Postpartum and Breastfeeding: Balancing Risks and Benefits. Expert Opin. Drug Saf. 2018, 17, 719–725. [Google Scholar] [CrossRef]
- Edinoff, A.N.; Akuly, H.A.; Hanna, T.A.; Ochoa, C.O.; Patti, S.J.; Ghaffar, Y.A.; Kaye, A.D.; Viswanath, O.; Urits, I.; Boyer, A.G.; et al. Selective Serotonin Reuptake Inhibitors and Adverse Effects: A Narrative Review. Neurol. Int. 2021, 13, 387–401. [Google Scholar] [CrossRef]
- Huddart, R.; Hicks, J.K.; Ramsey, L.B.; Strawn, J.R.; Smith, D.M.; Bobonis Babilonia, M.; Altman, R.B.; Klein, T.E. PharmGKB Summary: Sertraline Pathway, Pharmacokinetics. Pharmacogenet. Genom. 2020, 30, 26–33. [Google Scholar] [CrossRef]
- Mauri, M.C.; Fiorentini, A.; Paletta, S.; Altamura, A.C. Pharmacokinetics of Antidepressants in Patients with Hepatic Impairment. Clin. Pharmacokinet. 2014, 53, 1069–1081. [Google Scholar] [CrossRef]
- Apseloff, G.; Wilner, K.D.; von Deutsch, D.A.; Henry, E.B.; Tremaine, L.M.; Gerber, N.; Lazar, J.D. Sertraline Does Not Alter Steady-State Concentrations or Renal Clearance of Lithium in Healthy Volunteers. J. Clin. Pharmacol. 1992, 32, 643–646. [Google Scholar] [CrossRef]
- Vaughn, S.E.; Strawn, J.R.; Poweleit, E.A.; Sarangdhar, M.; Ramsey, L.B. The Impact of Marijuana on Antidepressant Treatment in Adolescents: Clinical and Pharmacologic Considerations. J. Pers. Med. 2021, 11, 615. [Google Scholar] [CrossRef] [PubMed]
- Cavanah, L.R.; Ray, P.K.; Goldhirsh, J.L.; Huey, L.Y.; Piper, B.J. Patterns in (Es)Citalopram Prescriptions to Medicaid and Medicare Patients in the United States: The Potential Effects of Evergreening. Front. Psychiatry 2025, 16, 1450111. [Google Scholar] [CrossRef] [PubMed]
- Hyttel, J.; Bøgesø, K.P.; Perregaard, J.; Sánchez, C. The Pharmacological Effect of Citalopram Residues in the (S)-(+)-Enantiomer. J. Neural Transm. Gen. Sect. 1992, 88, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Rao, N. The Clinical Pharmacokinetics of Escitalopram. Clin. Pharmacokinet. 2007, 46, 281–290. [Google Scholar] [CrossRef]
- von Moltke, L.L.; Greenblatt, D.J.; Giancarlo, G.M.; Granda, B.W.; Harmatz, J.S.; Shader, R.I. Escitalopram (S-Citalopram) and Its Metabolites in Vitro: Cytochromes Mediating Biotransformation, Inhibitory Effects, and Comparison to R-Citalopram. Drug Metab. Dispos. 2001, 29, 1102–1109. [Google Scholar]
- Malling, D.; Poulsen, M.N.; Søgaard, B. The Effect of Cimetidine or Omeprazole on the Pharmacokinetics of Escitalopram in Healthy Subjects. Br. J. Clin. Pharmacol. 2005, 60, 287–290. [Google Scholar] [CrossRef]
- Molden, E.; Spigset, O. Interactions between metoprolol and antidepressants. Tidsskr. Nor. Laegeforen. 2011, 131, 1777–1779. [Google Scholar] [CrossRef]
- Zakaraya, Z.; Abu Assab, M.; Tamimi, L.N.; Karameh, N.; Hailat, M.; Al-Omari, L.; Abu Dayyih, W.; Alasasfeh, O.; Awad, M.; Awad, R. Pharmacokinetics and Pharmacodynamics: A Comprehensive Analysis of the Absorption, Distribution, Metabolism, and Excretion of Psychiatric Drugs. Pharmaceuticals 2024, 17, 280. [Google Scholar] [CrossRef]
- Laine, K.; Kytölä, J.; Bertilsson, L. Severe Adverse Effects in a Newborn with Two Defective CYP2D6 Alleles after Exposure to Paroxetine during Late Pregnancy. Ther. Drug Monit. 2004, 26, 685–687. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.B.; Soberman, J.E. Effects of Paroxetine on the Pharmacokinetics and Pharmacodynamics of Immediate-Release and Extended-Release Metoprolol. Pharmacotherapy 2011, 31, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Spina, E.; Avenoso, A.; Salemi, M.; Facciolá, G.; Scordo, M.G.; Ancione, M.; Madia, A. Plasma Concentrations of Clozapine and Its Major Metabolites during Combined Treatment with Paroxetine or Sertraline. Pharmacopsychiatry 2000, 33, 213–217. [Google Scholar] [CrossRef]
- Alderman, J.; Preskorn, S.H.; Greenblatt, D.J.; Harrison, W.; Penenberg, D.; Allison, J.; Chung, M. Desipramine Pharmacokinetics When Coadministered with Paroxetine or Sertraline in Extensive Metabolizers. J. Clin. Psychopharmacol. 1997, 17, 284–291. [Google Scholar] [CrossRef]
- Albers, L.J.; Reist, C.; Helmeste, D.; Vu, R.; Tang, S.W. Paroxetine Shifts Imipramine Metabolism. Psychiatry Res. 1996, 59, 189–196. [Google Scholar] [CrossRef]
- Bannister, S.J.; Houser, V.P.; Hulse, J.D.; Kisicki, J.C.; Rasmussen, J.G. Evaluation of the Potential for Interactions of Paroxetine with Diazepam, Cimetidine, Warfarin, and Digoxin. Acta Psychiatr. Scand. Suppl. 1989, 350, 102–106. [Google Scholar] [CrossRef]
- Hillhouse, T.M.; Porter, J.H. A Brief History of the Development of Antidepressant Drugs: From Monoamines to Glutamate. Exp. Clin. Psychopharmacol. 2015, 23, 1–21. [Google Scholar] [CrossRef]
- Stevens, J.C.; Wrighton, S.A. Interaction of the Enantiomers of Fluoxetine and Norfluoxetine with Human Liver Cytochromes P450. J. Pharmacol. Exp. Ther. 1993, 266, 964–971. [Google Scholar] [CrossRef]
- Mandrioli, R.; Forti, G.C.; Raggi, M.A. Fluoxetine Metabolism and Pharmacological Interactions: The Role of Cytochrome P450. Curr. Drug Metab. 2006, 7, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Deodhar, M.; Rihani, S.B.A.; Darakjian, L.; Turgeon, J.; Michaud, V. Assessing the Mechanism of Fluoxetine-Mediated CYP2D6 Inhibition. Pharmaceutics 2021, 13, 148. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriou, G.; Zandonella Callegher, R.; Butera, R.; De Santis, M.; Cavaliere, A.F.; Vecchio, S.; Lanzi, C.; Davanzo, R.; Mangili, G.; Bondi, E.; et al. Consensus Panel Recommendations for the Pharmacological Management of Breastfeeding Women with Postpartum Depression. Int. J. Environ. Res. Public Health 2024, 21, 551. [Google Scholar] [CrossRef]
- Vitale, S.G.; Laganà, A.S.; Muscatello, M.R.A.; La Rosa, V.L.; Currò, V.; Pandolfo, G.; Zoccali, R.A.; Bruno, A. Psychopharmacotherapy in Pregnancy and Breastfeeding. Obstet. Gynecol. Surv. 2016, 71, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Crosby, I.; Yip, V.; Maguire, P.; Pirmohamed, M.; Turner, R.M. A Review of the Important Role of CYP2D6 in Pharmacogenomics. Genes 2020, 11, 1295. [Google Scholar] [CrossRef]
- Sánchez, C.; Bøgesø, K.P.; Ebert, B.; Reines, E.H.; Braestrup, C. Escitalopram versus Citalopram: The Surprising Role of the R-Enantiomer. Psychopharmacology 2004, 174, 163–176. [Google Scholar] [CrossRef]
- Dackehag, M.; Ellegård, L.M.; Gerdtham, U.; Nilsson, T. Macroeconomic fluctuations and individual use of psychotropic medications: Evidence from Swedish administrative data. Eur. J. Public Health 2023, 33, 93–98. [Google Scholar] [CrossRef]
- Zivanovic, M.; Vukcevic Markovic, M.; Dimoski, J.; Gvozden, M. Mental Health in Serbia: Assessment of Needs, Risk Factors and Barriers to Obtaining Professional Help; Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH: Belgrade, Serbia, 2022. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SSRI | Depression | Panic Attacks | OCD | Social Phobia | GAD | PTSD | Bulimia Nervosa | PTSD |
|---|---|---|---|---|---|---|---|---|
| fluoxetine | X (8+) | X | X (7+) | X | X | X | X | |
| citalopram | X | |||||||
| paroxetine | X | X | X | X | X | X | X | |
| sertraline | X | X | X (6+) | X | X | X | ||
| escitalopram | X (12+) | X |
| SSRI | Time to Maximum Concentration | Bioavailability | Bound Fraction | Volume of Distribution | Half-Life |
|---|---|---|---|---|---|
| fluoxetine | 6–8 h | 60–80% | 94% | 20–40 L/kg | 96 h |
| citalopram | 2–4 h | 80% | 80% | 12–16 L/kg | 30–35 h |
| paroxetine | 5–6 h | 30–60% | 95% | 3–12 L/kg | 21 h |
| sertraline | 4–8 h | 44% | 98% | 25 L/kg | 22–36 h |
| escitalopram | 3–4 h | 80% | 56% | 12–26 L/kg | 27–33 h |
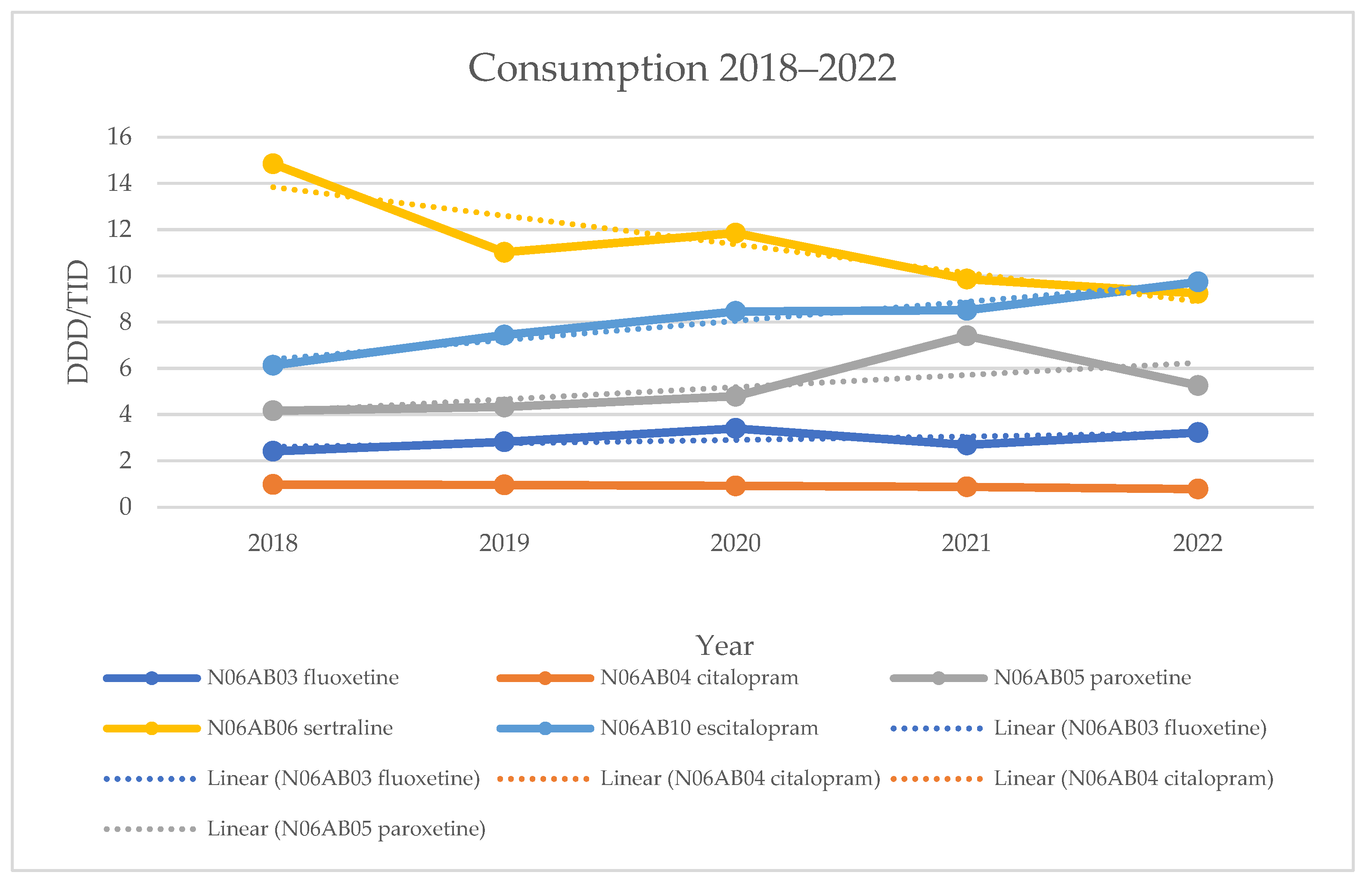
| Medicine | DID 2018 | DID 2019 | DID 2020 | DID 2021 | DID 2022 |
|---|---|---|---|---|---|
| fluoxetine | 2.40943 | 2.81899 | 3.40094 | 2.68469 | 3.22032 |
| citalopram | 0.97396 | 0.95170 | 0.91167 | 0.87061 | 0.78152 |
| paroxetine | 4.16225 | 4.32504 | 4.79192 | 7.40698 | 5.25851 |
| sertraline | 14.8493 | 11.0207 | 11.8468 | 9.85769 | 9.24536 |
| escitalopram | 6.13398 | 7.44041 | 8.46109 | 8.51289 | 9.73523 |
| Medicine | Trend Equation | R2 | Adjusted R2 | p-Value |
|---|---|---|---|---|
| fluoxetine | y = 0.1487x + 2.4606 | 0.342 | 0.1227 | 0.300 |
| citalopram | y = −0.0466x + 1.0377 | 0.9376 | 0.9168 | 0.007 * |
| paroxetine | y = 0.5274x + 3.6066 | 0.4042 | 0.2056 | 0.249 |
| sertraline | y = −1.2371x + 15.075 | 0.7948 | 0.7263 | 0.042 * |
| escitalopram | y = 0.8275x + 5.5742 | 0.9424 | 0.9233 | 0.006 * |
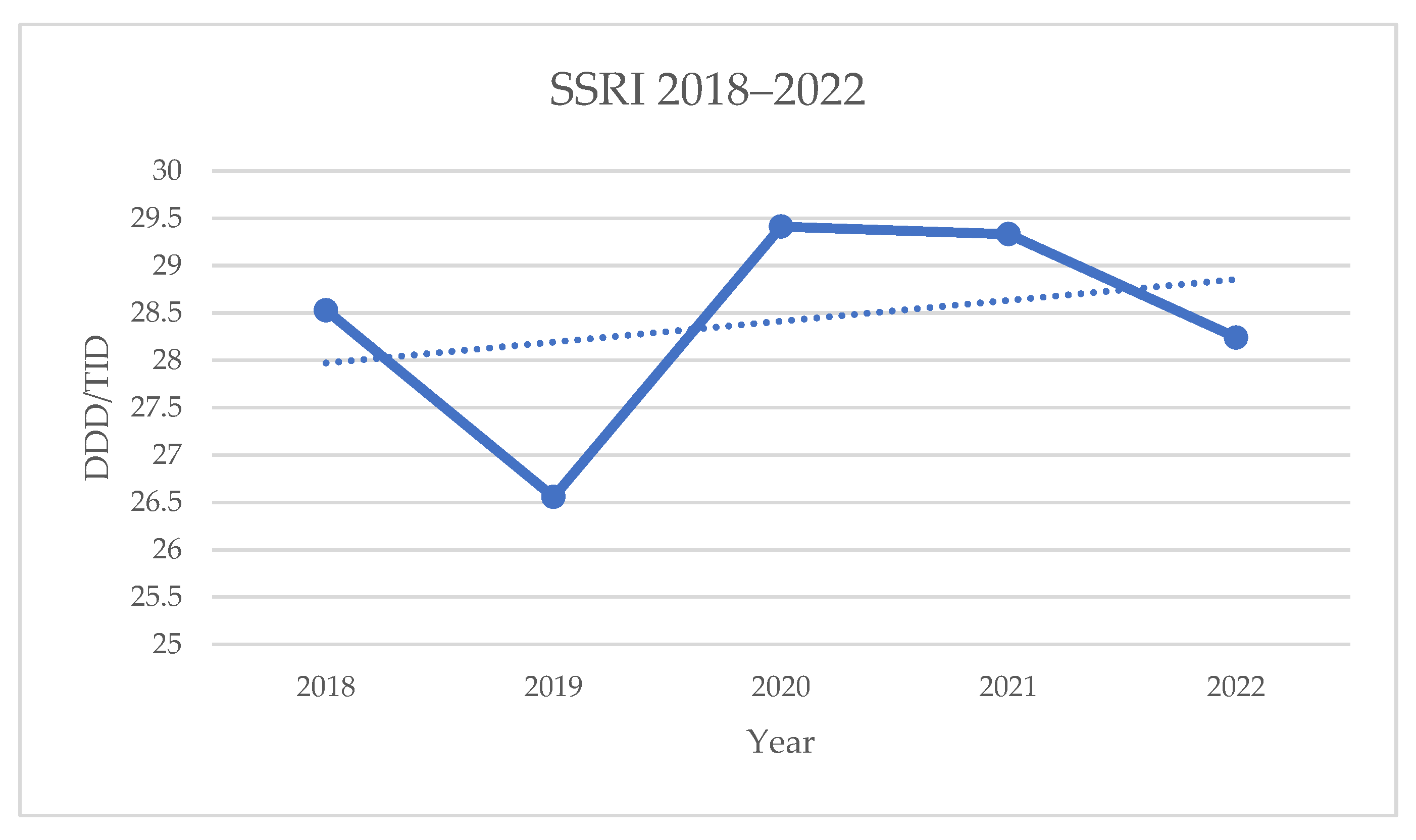
| SSRI | y = 0.22x + 27.754 | 0.0908 | −0.2123 | 0.622 |
| Year | DID SSRI |
|---|---|
| 2018 | 28.52887 |
| 2019 | 26.55683 |
| 2020 | 29.41245 |
| 2021 | 29.33288 |
| 2022 | 28.24096 |
| Country | DID 2018 | DID 2019 | DID 2020 | DID 2021 | DID 2022 |
|---|---|---|---|---|---|
| Serbia | 28.53 | 26.56 | 29.41 | 29.33 | 28.24 |
| Italy | 29.70 | 29.90 | 30.6 | 31.20 | 31.70 |
| Iceland | 103.3 | 106.3 | 111.7 | 118.9 | 116.3 |
| Spain | 49.09 | 50.27 | 52.11 | 55.07 | 57.71 |
| Croatia | 21.66 | 22.19 | 22.69 | 23.85 | 24.61 |
| Norway | 35.46 | 35.97 | 36.35 | 37.58 | / |
| The Netherlands | 42.35 | 44.41 | 46.5 | 48.21 | 49.71 |
| Estonia | 18.91 | 20.58 | 21.72 | 24.06 | 26.26 |
| Finland | 41.39 | 43.40 | 44.58 | 46.45 | / |
| Latvia | 10.42 | 11.45 | 13.17 | 14.26 | 15.76 |
| Lithuania | 20.127 | 22.50 | 23.22 | 23.86 | 25.74 |
| Slovenia | 40.30 | 41.00 | 41.30 | 42.90 | 44.20 |
| Denmark | 46.70 | 47.80 | 49.50 | 52.50 | 55.20 |
| Title 1 | Serbia | Denmark | Spain | Latvia | ||||
|---|---|---|---|---|---|---|---|---|
| 2019 | 2020 | 2019 | 2020 | 2019 | 2020 | 2019 | 2020 | |
| fluoxetine | 2.82 | 3.4 | 2 | 1.8 | 6.94 | 7.06 | 0.51 | 0.63 |
| citalopram | 0.95 | 0.91 | 13.9 | 13 | 6.11 | 6.09 | 0.86 | 0.94 |
| paroxetine | 4.33 | 4.79 | 2.2 | 2.1 | 8.8 | 8.9 | 3.1 | 3.52 |
| sertraline | 11.02 | 11.85 | 25.9 | 28.7 | 14.56 | 15.78 | 1.4 | 1.63 |
| escitalopram | 7.44 | 8.46 | 4.4 | 4.4 | 13.46 | 13.88 | 5.39 | 6.24 |
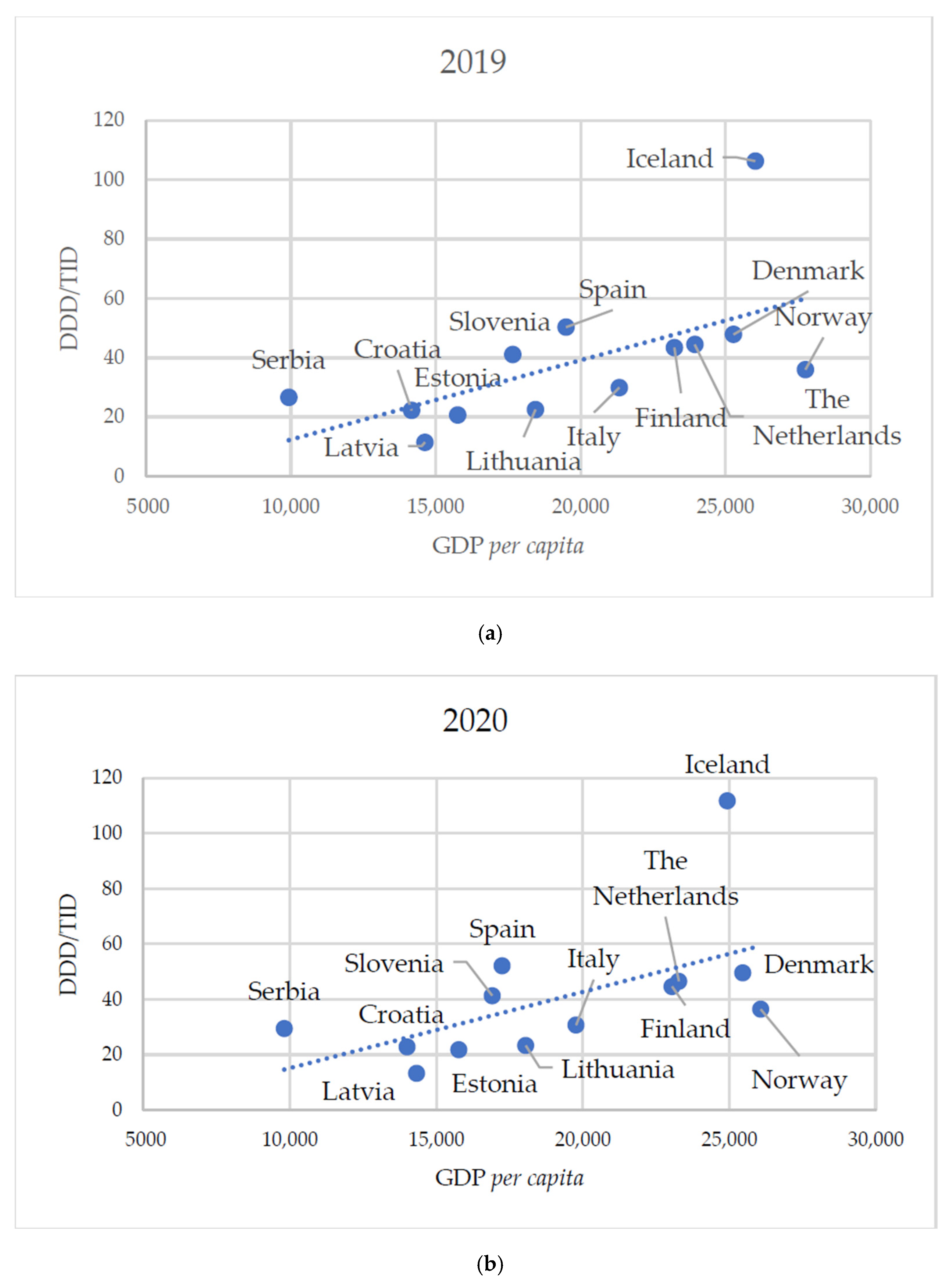
| Country | DID SSRI (2019) | GDP Per Capita (2019) | DID SSRI (2020) | GDP Per Capita (2020) |
|---|---|---|---|---|
| Serbia | 26.56 | 9927.1 | 29.41 | 9809.7 |
| Italy | 29.90 | 21,336.7 | 30.60 | 19,772.8 |
| Iceland | 106.3 | 26,029.8 | 111.7 | 24,937.5 |
| Spain | 50.27 | 19,497.2 | 52.11 | 17,253.5 |
| Croatia | 22.19 | 14,168.2 | 22.69 | 14,004.4 |
| Norway | 35.97 | 27,761.2 | 36.35 | 26,073.7 |
| The Netherlands | 44.41 | 23,939.2 | 46.50 | 23,281.6 |
| Estonia | 20.58 | 15,760.0 | 21.72 | 15,771.9 |
| Finland | 43.40 | 23,237.4 | 44.58 | 23,047.9 |
| Latvia | 11.45 | 14,628.4 | 13.17 | 14,325.5 |
| Lithuania | 22.50 | 18,444.7 | 23.22 | 18,053.4 |
| Slovenia | 41 | 17,652.1 | 41.30 | 16,907.5 |
| Denmark | 47.80 | 25,277.4 | 49.50 | 25,457.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samardžić, J.; Simović, F.; Sekanić, K.; Branković, M. Five-Year Trends in SSRI Consumption: A Precision Medicine Approach to Comparative Analysis Between Serbia and European Countries. Healthcare 2025, 13, 1174. https://doi.org/10.3390/healthcare13101174
Samardžić J, Simović F, Sekanić K, Branković M. Five-Year Trends in SSRI Consumption: A Precision Medicine Approach to Comparative Analysis Between Serbia and European Countries. Healthcare. 2025; 13(10):1174. https://doi.org/10.3390/healthcare13101174
Chicago/Turabian StyleSamardžić, Janko, Filip Simović, Kristina Sekanić, and Milica Branković. 2025. "Five-Year Trends in SSRI Consumption: A Precision Medicine Approach to Comparative Analysis Between Serbia and European Countries" Healthcare 13, no. 10: 1174. https://doi.org/10.3390/healthcare13101174
APA StyleSamardžić, J., Simović, F., Sekanić, K., & Branković, M. (2025). Five-Year Trends in SSRI Consumption: A Precision Medicine Approach to Comparative Analysis Between Serbia and European Countries. Healthcare, 13(10), 1174. https://doi.org/10.3390/healthcare13101174