
Psychometric Evaluation of the German Version of the Perceived Access to Healthcare Questionnaire in a Sample of Individuals with Rare Chronic Diseases



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Measures
2.2.1. Diagnostic Information
2.2.2. Access to Healthcare
2.2.3. Ability to Perceive—Health Literacy
2.2.4. Ability to Seek—Patient Activation
2.2.5. Ability to Reach—Mobility/Physical Functioning
2.2.6. Ability to Engage—Autonomy Preference
2.2.7. Ability to Pay—Socioeconomic Status
2.3. Statistical Analysis
3. Results
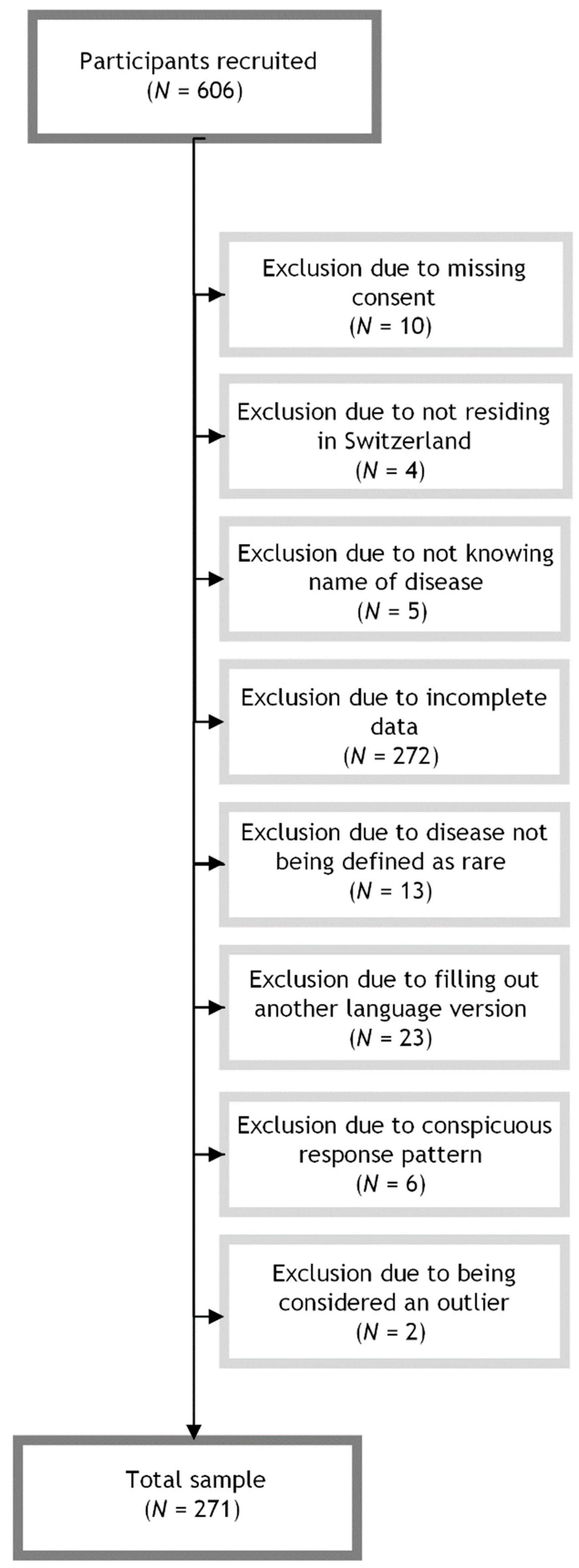
3.1. Sample Characteristics
3.2. Confirmatory Factor Analysis (Global Goodness of Fit)
3.3. Confirmatory Factor Analysis (Local Goodness of Fit)
3.4. Internal Consistency
3.5. Criterion-Related Validity
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gopal-Srivastava, R.; Kaufmann, P. Facilitating clinical studies in rare diseases. In Rare Diseases Epidemiology: Update and Overview; Posada de la Paz, M., Taruscio, D., Groft, S.C., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 125–140. [Google Scholar]
- Orphanet. About Rare Diseases. Available online: http://www.orpha.net/consor/cgi-bin/Education_AboutRareDiseases.php?lng=EN (accessed on 25 May 2023).
- EURORDIS Resolution4Rare: Global Campaign for the First UN Resolution on Persons Living with a Rare Disease. Available online: https://www.eurordis.org/resolution4rare-global-campaign-for-the-first-un-resolution-on-persons-living-with-a-rare-disease/#:~:text=The%20Resolution%20is%20an%20important,living%20with%20a%20rare%20disease (accessed on 25 May 2023).
- Nguengang Wakap, S.; Lambert, D.M.; Olry, A.; Rodwell, C.; Gueydan, C.; Lanneau, V.; Murphy, D.; Le Cam, Y.; Rath, A. Estimating cumulative point prevalence of rare diseases: Analysis of the Orphanet database. Eur. J. Hum. Genet. 2020, 28, 165–173. [Google Scholar] [CrossRef]
- Valdez, R.; Ouyang, L.; Bolen, J. Public Health and Rare Diseases: Oxymoron No More. Prev. Chronic Dis. 2016, 13, E05. [Google Scholar] [CrossRef]
- Von der Lippe, C.; Diesen, P.S.; Feragen, K.B. Living with a rare disorder: A systematic review of the qualitative literature. Mol. Genet. Genomic Med. 2017, 5, 758–773. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.C.Y.; Hong Kong Genome Project; Chu, A.T.W.; Chung, B.H.Y. Rare disease emerging as a global public health priority. Front. Public Health 2022, 10, 1028545. [Google Scholar] [CrossRef]
- Nguyen, A. Accessing Health Care in Global Public Health: The History of Conceptual Frameworks. In Handbook of Social Sciences and Global Public Health; Springer International Publishing: Cham, Switzerland, 2022; pp. 1–14. [Google Scholar]
- Ricketts, T.C.; Goldsmith, L.J. Access in health services research: The battle of the frameworks. Nurs. Outlook. 2005, 53, 274–280. [Google Scholar] [CrossRef]
- Andersen, R.M. A Behavior Model of Families’ Use of Health Services; Center for Health Administration Studies: Chicago, IL, USA, 1968. [Google Scholar]
- Penchansky, R.; Thomas, J.W. The concept of access: Definition and relationship to consumer satisfaction. Med. Care. 1981, 19, 127–140. [Google Scholar] [CrossRef]
- Shengelia, B.; Murray, C.J.; Adams, O.B. Beyond access and utilization: Defining and measuring health system coverage. In Health Systems Performance Assessment: Debates, Methods and Empiricism; World Health Organization: Geneva, Switzerland, 2003; pp. 221–235. [Google Scholar]
- Saurman, E. Improving access: Modifying Penchansky and Thomas’s Theory of Access. J. Health Serv. Res. Policy 2016, 21, 36–39. [Google Scholar] [CrossRef]
- Levesque, J.F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualizing access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Cu, A.; Meister, S.; Lefebvre, B.; Ridde, V. Assessing healthcare access using Levesque’s conceptual framework—A scoping review. Int. J. Equity Health 2021, 20, 116. [Google Scholar] [CrossRef]
- Frahsa, A.; Farquet, R.; Bayram, T.; De Araujo, L.; Meyer, S.; Sakarya, S.; Cattacin, S.; Abel, T. Experiences With Health Care Services in Switzerland Among Immigrant Women with Chronic Illnesses. Front. Public Health 2020, 8, 553438. [Google Scholar] [CrossRef] [PubMed]
- Hicks, P.M.; Kang, L.; Armstrong, M.L.; Pongrac, J.R.; Stagg, B.C.; Saylor, K.M.; Newman-Casey, P.A.; Woodward, M.A. A scoping review of patients’ barriers to eye care for glaucoma and keratitis. Surv. Ophthalmol. 2023, 68, 567–577. [Google Scholar] [CrossRef]
- Song, H.J.; Dennis, S.; Levesque, J.F.; Harris, M.F. What matters to people with chronic conditions when accessing care in Australian general practice? A qualitative study of patient, carer, and provider perspectives. BMC Fam. Pract. 2019, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Souliotis, K.; Hasardzhiev, S.; Agapidaki, E. A Conceptual Framework of Mapping Access to Health Care across EU Countries: The Patient Access Initiative. Public Health Genom. 2016, 19, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Quinn, M.; Robinson, C.; Forman, J.; Krein, S.L.; Rosland, A.M. Survey Instruments to Assess Patient Experiences With Access and Coordination Across Health Care Settings: Available and Needed Measures. Med. Care 2017, 55, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Hoseini-Esfidarjani, S.S.; Negarandeh, R.; Delavar, F.; Janani, L. Psychometric evaluation of the perceived access to health care questionnaire. BMC Health Serv. Res. 2021, 21, 638. [Google Scholar] [CrossRef] [PubMed]
- European Parliament and the Council of the European Union. Regulation (EC) No 141/2000 of the European Parliament and of the Council of 16 December 1999 on orphan medicinal products. Off. J. Eur. Communities 2000, 18, 1–5. [Google Scholar]
- Wood, D.; Harms, P.D.; Lowman, G.H.; DeSimone, J.A. Response speed and response consistency as mutually validating indicators of data quality in online samples. Soc. Psych. Pers. Sci. 2017, 8, 454–464. [Google Scholar] [CrossRef]
- Bakker, M.; Wicherts, J.M. Outlier removal, sum scores, and the inflation of the type I error rate in independent samples t tests: The power of alternatives and recommendations. Psychol. Methods 2014, 19, 409–427. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th ed.; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Uhlenbusch, N.; Löwe, B.; Härter, M.; Schramm, C.; Weiler-Normann, C.; Depping, M.K. Depression and anxiety in patients with different rare chronic diseases: A cross-sectional study. PLoS ONE 2019, 14, e0211343. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P.; ISPOR Task Force for Translation and Cultural Adaptation. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef]
- Cyr, M.E.; Etchin, A.G.; Guthrie, B.J.; Benneyan, J.C. Access to specialty healthcare in urban versus rural US populations: A systematic literature review. BMC Health Serv. Res. 2019, 19, 974. [Google Scholar] [CrossRef] [PubMed]
- Finbråten, H.S.; Wilde-Larsson, B.; Nordström, G.; Pettersen, K.S.; Trollvik, A.; Guttersrud, Ø. Establishing the HLS-Q12 short version of the European Health Literacy Survey Questionnaire: Latent trait analyses applying Rasch modeling and confirmatory factor analysis. BMC Health Serv. Res. 2018, 18, 506. [Google Scholar] [CrossRef] [PubMed]
- Ilic, A.; Roser, K.; Sommer, G.; Baenziger, J.; Mitter, V.R.; Mader, L.; Dyntar, D.; Michel, G. COVID-19 Information-Seeking, Health Literacy, and Worry and Anxiety During the Early Stage of the Pandemic in Switzerland: A Cross-Sectional Study. Int. J. Public Health 2022, 67, 1604717. [Google Scholar] [CrossRef] [PubMed]
- Vincent, C.; Staines, A. Enhancing the Quality and Safety of Swiss Healthcare; Federal Office of Public Health: Bern, Switzerland, 2019. [Google Scholar]
- Hibbard, J.H.; Stockard, J.; Mahoney, E.R.; Tusler, M. Development of the Patient Activation Measure (PAM): Conceptualizing and measuring activation in patients and consumers. Health Serv. Res. 2004, 39, 1005–1026. [Google Scholar] [CrossRef] [PubMed]
- Brenk-Franz, K.; Hibbard, J.H.; Herrmann, W.J.; Freund, T.; Szecsenyi, J.; Djalali, S.; Steurer-Stey, C.; Sönnichsen, A.; Tiesler, F.; Storch, M.; et al. Validation of the German version of the patient activation measure 13 (PAM13-D) in an international multicentre study of primary care patients. PLoS ONE 2013, 8, e74786. [Google Scholar] [CrossRef] [PubMed]
- Zill, J.M.; Dwinger, S.; Kriston, L.; Rohenkohl, A.; Härter, M.; Dirmaier, J. Psychometric evaluation of the German version of the patient activation measure (PAM13). BMC Public Health 2013, 13, 1027. [Google Scholar] [CrossRef]
- Wirtz, M.A.; Morfeld, M.; Glaesmer, H.; Brähler, E. Normierung des SF-12 Version 2.0 zur Messung der gesundheitsbezogenen Lebensqualität in einer deutschen bevölkerungsrepräsentativen Stichprobe [Standardization of the SF-12 version 2.0 assessing health-related quality of life in a representative German sample]. Diagnostica 2018, 64, 215–226. [Google Scholar]
- Scholz, C. Personalmanagement: Informationsorientierte und Verhaltenstheoretische Grundlagen; Vahlen: Löbnitz, Germany, 2014. [Google Scholar]
- Kuhl, J.; Kaschel, R. Entfremdung als Krankheitsursache: Selbstregulation von Affekten und integrative Kompetenz [Alienation as a determinant of symptom formation: Self-regulation of affect and integrative competence]. Psychol. Rundsch. 2004, 55, 61–71. [Google Scholar] [CrossRef]
- Simon, D.; Kriston, L.; Loh, A.; Spies, C.; Scheibler, F.; Wills, C.; Härter, M. Confirmatory factor analysis and recommendations for improvement of the Autonomy-Preference-Index (API). Health Expect 2010, 13, 234–243. [Google Scholar] [CrossRef]
- Giersdorf, N.; Loh, A.; Härter, M. Messung der partizipativen Entscheidungsfindung [Measuring shared decision making]. Z. Fur Arztl. Fortbild. Und Qual. 2004, 98, 135–141. [Google Scholar]
- R: A Language and Environment for Statistical Computing (4.1.2). The R Foundation for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 2 August 2023).
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Allyn & Bacon: New York, NY, USA; Pearson Education: Harlow, UK, 2007. [Google Scholar]
- Hu, L.-T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Cortina, J.M. What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 1993, 78, 98–104. [Google Scholar] [CrossRef]
- Revelle, W.R. psych: Procedures for Personality and Psychological Research. 2017. Available online: https://www.scholars.northwestern.edu/en/publications/psych-procedures-for-personality-and-psychological-research (accessed on 2 August 2023).
- George, D.; Mallery, P. Cronbach’s Alpha. SPSS for Windows Step by Step: A Simple Guide and Reference; Allyn & Bacon: New York, NY, USA, 2003; Volume 11, p. 231. [Google Scholar]
- Baumbusch, J.; Mayer, S.; Sloan-Yip, I. Alone in a Crowd? Parents of Children with Rare Diseases’ Experiences of Navigating the Healthcare System. J. Genet. Couns. 2018, 28, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Molster, C.; Urwin, D.; Di Pietro, L.; Fookes, M.; Petrie, D.; van der Laan, S.; Dawkins, H. Survey of healthcare experiences of Australian adults living with rare diseases. Orphanet J. Rare Dis. 2016, 11, 30. [Google Scholar] [CrossRef]
- Navarrete-Opazo, A.A.; Singh, M.; Tisdale, A.; Cutillo, C.M.; Garrison, S.R. Can you hear us now? The impact of health-care utilization by rare disease patients in the United States. Genet. Med. 2021, 23, 2194–2201. [Google Scholar] [CrossRef]
- Chaufan, C. Is the Swiss health care system a model for the United States? Int. J. Health Serv. 2014, 44, 255–267. [Google Scholar] [CrossRef]
- Herzlinger, R.E.; Parsa-Parsi, R. Consumer-driven health care: Lessons from Switzerland. JAMA 2004, 292, 1213–1220. [Google Scholar] [CrossRef]
- Crutzen, R.; Peters, G.Y. Scale quality: Alpha is an inadequate estimate and factor-analytic evidence is needed first of all. Health Psychol. Rev. 2017, 11, 242–247. [Google Scholar] [CrossRef]
- Vaske, J.J.; Beaman, J.; Sponarski, C.C. Rethinking internal consistency in Cronbach’s alpha. Leis. Sci. 2017, 39, 163–173. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Sociodemographic & Disease-Related Variables | 1 N (%) | 2 M (SD) |
|---|---|---|
| Age (in years) | 48.15 (15.32) | |
| Gender | ||
| Female | 162 (59.78) | |
| Male | 108 (39.85) | |
| Non-binary | 1 (0.37) | |
| Education | ||
| Less than nine years of education/special needs education | 2 (0.74) | |
| Mandatory schooling time (nine years) | 16 (5.90) | |
| Middle school/junior high school | 99 (36.53) | |
| Senior high school/university of applied sciences | 104 (38.378) | |
| University | 50 (18.45) | |
| Marital Status | ||
| Single | 84 (31.00) | |
| Married | 127 (46.86) | |
| Cohabiting or in a partnership | 47 (17.34) | |
| Separated or divorced | 15 (5.54) | |
| Widowed | 4 (1.48) | |
| ICD-10 3 disease type | ||
| C00–D49, neoplasms | 6 (2.21) | |
| D50–D89, diseases of the blood and blood-forming organs, and certain disorders involving the immune mechanism | 23 (8.49) | |
| E00–E90, endocrine, nutritional, and metabolic diseases | 58 (21.40) | |
| G00–G99, diseases of the nervous system | 46 (16.97) | |
| H00–H59, diseases of the eye and adnexa | 21 (7.75) | |
| I00–I99, diseases of the circulatory system | 9 (3.21) | |
| K00–K93, diseases of the digestive system | 28 (10.33) | |
| L00–L99, diseases of the skin and subcutaneous tissue | 1 (0.37) | |
| M00–M99, diseases of the musculoskeletal system and connective tissue | 11 (4.06) | |
| N00–N99, diseases of the genitourinary system | 1 (0.37) | |
| Q00–Q99, congenital malformations, deformations, and chromosomal abnormalities | 51 (18.82) | |
| S00–T98, injury, poisoning, and certain other consequences of external causes | 9 (3.32) | |
| Disease type (according to ICD-11 3) | ||
| Developmental anomalies | 7 (2.58) | |
| Disease course | ||
| Stable | 103 (38.01) | |
| Progressive | 64 (23.62) | |
| Relapsing | 67 (24.72) | |
| Improving | 12 (4.43) | |
| Unknown | 25 (9.23) |
| Model | df 1 | χ2 4 | χ2 Difference 4 | p | AIC 2 | BIC 3 |
|---|---|---|---|---|---|---|
| Six-factor model | 429 | 1087.014 | 19,841.15 | 20,194.16 | ||
| Five-factor model | 430 | 1556.793 | 92.70 | <0.001 | 20,308.93 | 20,658.34 |
| Unidimensional-factor model | 435 | 4184.625 | 753.98 | <0.001 | 22,926.76 | 23,258.16 |
| Reduced Six-Factor Model | Original Six-Factor Model | |
|---|---|---|
| Latent Factor | α | α |
| Accessibility | 0.91 | 0.83 |
| Item 1 | 0.91 | |
| Item 2 | 0.83 | 0.74 |
| Item 3 | 0.80 | 0.72 |
| Item 4 | 0.96 | 0.75 |
| Availability | 0.64 | 0.64 |
| Item 5 | 0.60 | 0.60 |
| Item 6 | 0.35 | 0.35 |
| Item 7 | 0.64 | 0.64 |
| Acceptability | 0.89 | 0.86 |
| Item 8 | 0.88 | 0.84 |
| Item 9 | 0.87 | 0.83 |
| Item 10 | 0.86 | 0.82 |
| Item 11 | 0.87 | 0.83 |
| Item 12 | 0.88 | 0.84 |
| Item 13 | 0.87 | |
| Item 14 | 0.88 | |
| Item 15 | 0.88 | 0.84 |
| Item 16 | 0.89 | 0.85 |
| Affordability | 0.75 | 0.45 |
| Item 17 | 0.70 | −0.041 |
| Item 18 | 0.52 | 0.101 |
| Item 19 | 0.749 | |
| Adequacy | 0.77 | 0.76 |
| Item 20 | 0.69 | 0.70 |
| Item 21 | 0.69 | 0.70 |
| Item 22 | 0.77 | 0.76 |
| Item 23 | 0.74 | 0.73 |
| Item 24 | 0.71 | 0.71 |
| Item 25 | 0.77 | |
| Awareness | 0.84 | 0.82 |
| Item 26 | 0.79 | 0.77 |
| Item 27 | 0.82 | 0.79 |
| Item 28 | 0.80 | 0.78 |
| Item 29 | 0.77 | 0.76 |
| Item 30 | 0.84 | 0.80 |
| Item 31 | 0.84 |
| Latent Factor | Floor Effect, % | Ceiling Effect, % |
|---|---|---|
| Accessibility | 1.11 | 21.77 |
| Availability | 0.37 | 8.12 |
| Acceptability | 1.48 | 6.64 |
| Affordability | 0.74 | 25.46 |
| Adequacy | 0.37 | 3.32 |
| Awareness | 0.37 | 5.90 |
| Variable | M 1 | SD 2 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Accessibility | 11.45 | 2.92 | ||||||||||
| 2. Availability | 11.24 | 2.22 | 0.43 ** | |||||||||
| [0.32, 0.52] | ||||||||||||
| 3. Acceptability | 27.04 | 4.92 | 0.32 ** | 0.66 ** | ||||||||
| [0.21, 0.42] | [0.59, 0.72] | |||||||||||
| 4. Affordability | 7.93 | 1.88 | 0.12 * | 0.17 ** | 0.14 * | |||||||
| [0.00, 0.24] | [0.05, 0.28] | [0.02, 0.25] | ||||||||||
| 5. Adequacy | 17.86 | 3.46 | 0.38 ** | 0.59 ** | 0.64 ** | 0.22 ** | ||||||
| [0.27, 0.47] | [0.50, 0.66] | [0.56, 0.71] | [0.11, 0.33] | |||||||||
| 6. Awareness | 18.92 | 3.59 | 0.25 ** | 0.45 ** | 0.68 ** | 0.07 | 0.61 ** | |||||
| [0.14, 0.36] | [0.35, 0.54] | [0.61, 0.74] | [−0.05, 0.19] | [0.53, 0.68] | ||||||||
| 7. API 3 | 11.14 | 4.01 | 0.11 | 0.25 ** | 0.25 ** | 0.24 ** | 0.19 ** | 0.13 * | ||||
| [−0.00, 0.23] | [0.14, 0.36] | [0.13, 0.35] | [0.13, 0.35] | [0.08, 0.31] | [0.02, 0.25] | |||||||
| 8. HLS-Q12 4 | 33.90 | 4.87 | 0.13 * | 0.25 ** | 0.26 ** | 0.07 | 0.25 ** | 0.38 ** | 0.01 | |||
| [0.01, 0.24] | [0.13, 0.36] | [0.14, 0.36] | [−0.05, 0.19] | [0.13, 0.35] | [0.28, 0.48] | [−0.11, 0.13] | ||||||
| 9. PAM13 5 | 41.12 | 5.39 | 0.17 ** | 0.21 ** | 0.22 ** | 0.18 ** | 0.27 ** | 0.26 ** | 0.05 | 0.46 ** | ||
| [0.06, 0.29] | [0.10, 0.32] | [0.10, 0.33] | [0.06, 0.29] | [0.16, 0.38] | [0.15, 0.37] | [−0.07, 0.17] | [0.36, 0.55] | |||||
| 10. SF-12 PCS 6 | 359.50 | 176.15 | 0.36 ** | 0.32 ** | 0.23 ** | 0.05 | 0.19 ** | 0.18 ** | 0.14 * | 0.22 ** | 0.22 ** | |
| [0.25, 0.46] | [0.20, 0.42] | [0.11, 0.34] | [−0.07, 0.16] | [0.08, 0.30] | [0.07, 0.30] | [0.02, 0.25] | [0.10, 0.33] | [0.10, 0.33] | ||||
| 11. Education | 4.54 | 1.10 | 0.05 | −0.03 | −0.07 | −0.12 * | −0.07 | 0.08 | −0.20 ** | 0.13 * | 0.00 | 0.11 |
| [−0.07, 0.17] | [−0.14, 0.09] | [−0.19, 0.05] | [−0.24, −0.00] | [−0.19, 0.05] | [-0.04, 0.20] | [−0.31, −0.08] | [0.02, 0.25] | [−0.12, 0.12] | [−0.01, 0.23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wehrli, S.; Dwyer, A.A.; Landolt, M.A. Psychometric Evaluation of the German Version of the Perceived Access to Healthcare Questionnaire in a Sample of Individuals with Rare Chronic Diseases. Healthcare 2024, 12, 661. https://doi.org/10.3390/healthcare12060661
Wehrli S, Dwyer AA, Landolt MA. Psychometric Evaluation of the German Version of the Perceived Access to Healthcare Questionnaire in a Sample of Individuals with Rare Chronic Diseases. Healthcare. 2024; 12(6):661. https://doi.org/10.3390/healthcare12060661
Chicago/Turabian StyleWehrli, Susanne, Andrew A. Dwyer, and Markus A. Landolt. 2024. "Psychometric Evaluation of the German Version of the Perceived Access to Healthcare Questionnaire in a Sample of Individuals with Rare Chronic Diseases" Healthcare 12, no. 6: 661. https://doi.org/10.3390/healthcare12060661
APA StyleWehrli, S., Dwyer, A. A., & Landolt, M. A. (2024). Psychometric Evaluation of the German Version of the Perceived Access to Healthcare Questionnaire in a Sample of Individuals with Rare Chronic Diseases. Healthcare, 12(6), 661. https://doi.org/10.3390/healthcare12060661