
Reducing Sample Size While Improving Equity in Vaccine Clinical Trials: A Machine Learning-Based Recruitment Methodology with Application to Improving Trials of Hepatitis C Virus Vaccines in People Who Inject Drugs

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Preparation
2.1.1. Longitudinal Data
2.1.2. Survival Analysis Models
- Age;
- Sex assigned at birth;
- Syringe source (harm reduction program or other);
- The number of PWID who gave the candidate drugs/injection equipment in the last 30 days;
- The number of PWID who the candidate gave drugs/injection equipment to in the last 30 days;
- The total number of people in the candidate’s drug use network;
- The number of daily injections;
- The fraction of injections that involve receiving drugs or injection equipment from another person in the network.
2.1.3. Demographic Targets
2.2. The PREDICTEE Workflow
2.2.1. Candidate Scoring Equations
2.3. Evaluating PREDICTEE HCV Vaccine Trial in Chicago PWID Population
2.3.1. Design of Simulation Experiments
2.3.2. Software Modeling Platform and Tools
3. Results
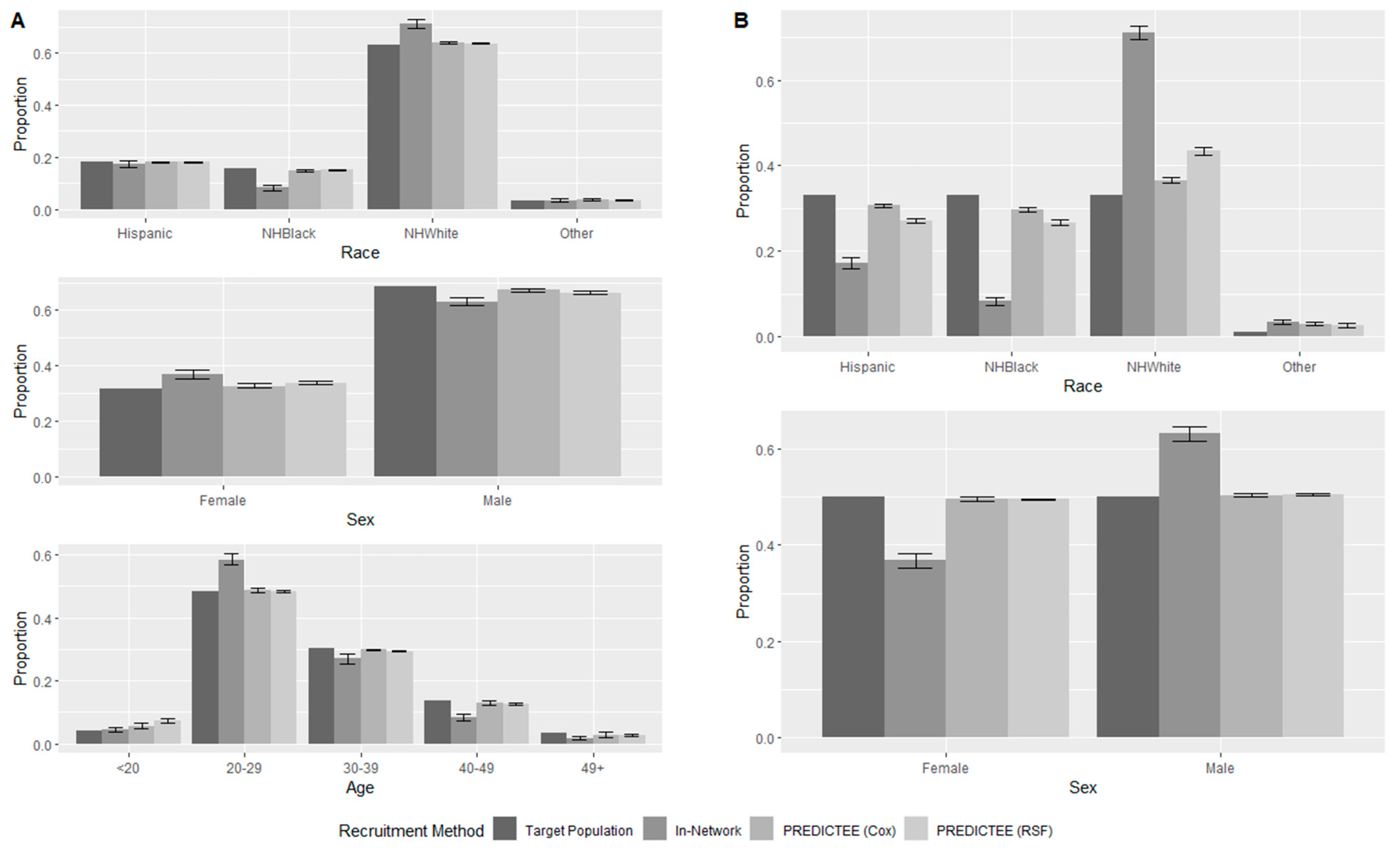
3.1. Matching the Chicago PWID Population
3.2. Targeting Arbitrary Demographics
4. Discussion
4.1. Implications
4.2. Limitations
4.3. Extensions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Lancet Gastroenterology & Hepatology. The Hunt for a Vaccine for Hepatitis C Virus Continues. Lancet Gastroenterol. Hepatol. 2021, 6, 253. [Google Scholar] [CrossRef] [PubMed]
- Page, K.; Melia, M.T.; Veenhuis, R.T.; Winter, M.; Rousseau, K.E.; Massaccesi, G.; Osburn, W.O.; Forman, M.; Thomas, E.; Thornton, K.; et al. Randomized Trial of a Vaccine Regimen to Prevent Chronic HCV Infection. N. Engl. J. Med. 2021, 384, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, E.S.; Rosenthal, E.M.; Hall, E.W.; Barker, L.; Hofmeister, M.G.; Sullivan, P.S.; Dietz, P.; Mermin, J.; Ryerson, A.B. Prevalence of Hepatitis C Virus Infection in US States and the District of Columbia, 2013 to 2016. JAMA Netw. Open 2018, 1, e186371. [Google Scholar] [CrossRef]
- Hofmeister, M.G.; Rosenthal, E.M.; Barker, L.K.; Rosenberg, E.S.; Barranco, M.A.; Hall, E.W.; Edlin, B.R.; Mermin, J.; Ward, J.W.; Ryerson, A.B. Estimating Prevalence of Hepatitis C Virus Infection in the United States, 2013–2016. Hepatology 2019, 69, 1020–1031. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, M.L. Hepatitis C Virus Therapy in the Direct Acting Antiviral Era. Curr. Opin. Gastroenterol. 2014, 30, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Bethea, E.D.; Chen, Q.; Hur, C.; Chung, R.T.; Chhatwal, J. Should We Treat Acute Hepatitis C? A Decision and Cost-Effectiveness Analysis. Hepatology 2018, 67, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Bruggmann, P.; Litwin, A.H. Models of Care for the Management of Hepatitis C Virus among People Who Inject Drugs: One Size Does Not Fit All. Clin. Infect. Dis. 2013, 57 (Suppl. S2), S56–S61. [Google Scholar] [CrossRef]
- Hellard, M.; Doyle, J.S.; Sacks-Davis, R.; Thompson, A.J.; McBryde, E. Eradication of Hepatitis C Infection: The Importance of Targeting People Who Inject Drugs. Hepatology 2014, 59, 366–369. [Google Scholar] [CrossRef]
- Carlisle, B.; Kimmelman, J.; Ramsay, T.; MacKinnon, N. Unsuccessful Trial Accrual and Human Subjects Protections: An Empirical Analysis of Recently Closed Trials. Clin. Trials 2015, 12, 77–83. [Google Scholar] [CrossRef]
- Huang, G.D.; Bull, J.; Johnston McKee, K.; Mahon, E.; Harper, B.; Roberts, J.N. Clinical Trials Recruitment Planning: A Proposed Framework from the Clinical Trials Transformation Initiative. Contemp. Clin. Trials 2018, 66, 74–79. [Google Scholar] [CrossRef]
- Goldberg, A.; Bakhireva, L.N.; Page, K.; Henrie, A.M. A Qualitative Scoping Review of Early-Terminated Clinical Trials Sponsored by the Department of Veterans Affairs Cooperative Studies Program From 2010 to 2020. Epidemiol. Rev. 2022, 44, 110–120. [Google Scholar] [CrossRef]
- Matheny, J.G. The Economics of Pharmaceutical Development: Costs, Risks, and Incentives. Ph.D. Thesis, Johns Hopkins University, Baltimore, MD, USA, 2013. [Google Scholar]
- Battelle Technology Partnership Practice. Biopharmaceutical Industry-Sponsored Clinical Trials: Impact on State Economies; Battelle: Columbus, OH, USA, 2015. [Google Scholar]
- Wilder, J.; Saraswathula, A.; Hasselblad, V.; Muir, A. A Systematic Review of Race and Ethnicity in Hepatitis C Clinical Trial Enrollment. J. Natl. Med. Assoc. 2016, 108, 24–29. [Google Scholar] [CrossRef]
- Grebely, J.; Raffa, J.D.; Lai, C.; Krajden, M.; Conway, B.; Tyndall, M.W. Factors Associated with Spontaneous Clearance of Hepatitis C Virus among Illicit Drug Users. Can. J. Gastroenterol. 2007, 21, 447–451. [Google Scholar] [CrossRef]
- van den Berg, C.H.B.S.; Grady, B.P.X.; Schinkel, J.; van de Laar, T.; Molenkamp, R.; van Houdt, R.; Coutinho, R.A.; van Baarle, D.; Prins, M. Female Sex and IL28B, a Synergism for Spontaneous Viral Clearance in Hepatitis C Virus (HCV) Seroconverters from a Community-Based Cohort. PLoS ONE 2011, 6, e27555. [Google Scholar] [CrossRef]
- Bakr, I.; Rekacewicz, C.; Hosseiny, M.E.; Ismail, S.; Daly, M.E.; El-Kafrawy, S.; Esmat, G.; Hamid, M.A.; Mohamed, M.K.; Fontanet, A. Higher Clearance of Hepatitis C Virus Infection in Females Compared with Males. Gut 2006, 55, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Piasecki, B.A.; Lewis, J.D.; Reddy, K.R.; Bellamy, S.L.; Porter, S.B.; Weinrieb, R.M.; Stieritz, D.D.; Chang, K.-M. Influence of Alcohol Use, Race, and Viral Coinfections on Spontaneous HCV Clearance in a US Veteran Population. Hepatology 2004, 40, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.; Price, J.C.; Tien, P.C. Hepatitis C Virus Infection in the Older Patient. Infect. Dis. Clin. North Am. 2017, 31, 827–838. [Google Scholar] [CrossRef] [PubMed]
- FDA Office of Minority Health and Health Equity. Enhance EQUITY in Clinical Trials. Available online: https://www.fda.gov/consumers/enhance-equity-initiative/enhance-equity-clinical-trials (accessed on 27 July 2022).
- National Institutes of Health. Inclusion of Women and Minorities as Participants in Research Involving Human Subjects. Available online: https://grants.nih.gov/policy/inclusion/women-and-minorities.htm (accessed on 27 July 2022).
- Kerr, K.F.; Roth, J.; Zhu, K.; Thiessen-Philbrook, H.; Meisner, A.; Wilson, F.P.; Coca, S.; Parikh, C.R. Evaluating Biomarkers for Prognostic Enrichment of Clinical Trials. Clin. Trials 2017, 14, 629–638. [Google Scholar] [CrossRef]
- Irazabal, M.V.; Abebe, K.Z.; Bae, K.T.; Perrone, R.D.; Chapman, A.B.; Schrier, R.W.; Yu, A.S.; Braun, W.E.; Steinman, T.I.; Harris, P.C.; et al. Prognostic Enrichment Design in Clinical Trials for Autosomal Dominant Polycystic Kidney Disease: The HALT-PKD Clinical Trial. Nephrol. Dial. Transplant. 2017, 32, 1857–1865. [Google Scholar] [CrossRef] [PubMed]
- Heitjan, D.F.; Ge, Z.; Ying, G. Real-Time Prediction of Clinical Trial Enrollment and Event Counts: A Review. Contemp. Clin. Trials 2015, 45, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Stevens, V.W.; Russo, E.M.; Young-Xu, Y.; Leecaster, M.; Zhang, Y.; Zhang, C.; Yu, H.; Cai, B.; Gonzalez, E.N.; Gerding, D.N.; et al. Identification of Patients at Risk of Clostridioides Difficile Infection for Enrollment in Vaccine Clinical Trials. Vaccine 2021, 39, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Kahn, J.M.; Gray, D.M., II; Oliveri, J.M.; Washington, C.M.; DeGraffinreid, C.R.; Paskett, E.D. Strategies to Improve Diversity, Equity, and Inclusion in Clinical Trials. Cancer 2022, 128, 216–221. [Google Scholar] [CrossRef]
- Kang, M.; Nicolay, U. Evaluation of Operational Chronic Infection Endpoints for HCV Vaccine Trials. Contemp. Clin. Trials 2008, 29, 671–678. [Google Scholar] [CrossRef][Green Version]
- Young, A.M.; Stephens, D.B.; Khaleel, H.A.; Havens, J.R. Hepatitis C Vaccine Clinical Trials among People Who Use Drugs: Potential for Participation and Involvement in Recruitment. Contemp. Clin. Trials 2015, 41, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.; Al-Zoubi, T.; El Naqa, I.; Saeed, H. The Role of Artificial Intelligence in Hastening Time to Recruitment in Clinical Trials. BJR Open 2023, 5, 20220023. [Google Scholar] [CrossRef] [PubMed]
- Harrer, S.; Shah, P.; Antony, B.; Hu, J. Artificial Intelligence for Clinical Trial Design. Trends Pharmacol. Sci. 2019, 40, 577–591. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Thangaraj, P.M.; Bhatt, D.L.; Ross, J.S.; Young, L.H.; Krumholz, H.M.; Suchard, M.A.; Khera, R. An Explainable Machine Learning-Based Phenomapping Strategy for Adaptive Predictive Enrichment in Randomized Clinical Trials. npj Digit. Med. 2023, 6, 217. [Google Scholar] [CrossRef]
- Gutfraind, A.; Boodram, B.; Prachand, N.; Hailegiorgis, A.; Dahari, H.; Major, M.E. Agent-Based Model Forecasts Aging of the Population of People Who Inject Drugs in Metropolitan Chicago and Changing Prevalence of Hepatitis C Infections. PLoS ONE 2015, 10, e0137993. [Google Scholar] [CrossRef]
- Tatara, E.; Collier, N.T.; Ozik, J.; Gutfraind, A.; Cotler, S.J.; Dahari, H.; Major, M.; Boodram, B. Multi-Objective Model Exploration of Hepatitis C Elimination in an Agent-Based Model of People Who Inject Drugs. Proc. Winter Simul. Conf. 2019, 2019, 1008–1019. [Google Scholar] [CrossRef]
- Cox, D.; Oakes, D. Analysis of Survival Data; CRC Press: Boca Raton, FL, USA, 1984; ISBN 978-0-412-24490-2. [Google Scholar]
- Ishwaran, H.; Kogalur, U.B.; Blackstone, E.H.; Lauer, M.S. Random Survival Forests. Ann. Appl. Stat. 2008, 2, 841–860. [Google Scholar] [CrossRef]
- Genuer, R.; Poggi, J.-M.; Tuleau, C. Random Forests: Some Methodological Insights. arXiv 2008, arXiv:0811.3619. [Google Scholar]
- Goldstein, B.A.; Polley, E.C.; Briggs, F.B.S. Random Forests for Genetic Association Studies. Stat. Appl. Genet. Mol. Biol. 2011, 10, 32. [Google Scholar] [CrossRef]
- Oshiro, T.M.; Perez, P.S.; Baranauskas, J.A. How Many Trees in a Random Forest? In Machine Learning and Data Mining in Pattern Recognition—Proceedings of the 8th International Conference, MLDM 2012, Berlin, Germany, 13–20 July 2012; Perner, P., Ed.; Springer: Berlin/Heidelberg, 2012; pp. 154–168. [Google Scholar]
- Probst, P.; Boulesteix, A.-L. To Tune or Not to Tune the Number of Trees in Random Forest? J. Mach. Learn. Res. 2017, 18, 1–18. [Google Scholar]
- Tatara, E.; Gutfraind, A.; Collier, N.T.; Echevarria, D.; Cotler, S.J.; Major, M.E.; Ozik, J.; Dahari, H.; Boodram, B. Modeling Hepatitis C Micro-Elimination among People Who Inject Drugs with Direct-Acting Antivirals in Metropolitan Chicago. PLoS ONE 2022, 17, e0264983. [Google Scholar] [CrossRef]
- Mackesy-Amiti, M.E.; Gutfraind, A.; Tatara, E.R.; Collier, N.T.; Cotler, S.J.; Page, K.; Ozik, J.T.; Boodram, B.; Major, M.E.; Dahari, H. Simulations of HCV Vaccine Trials Demonstrate Effects of Background Incidence and Unbalanced Exposure That Can Impact Vaccine Efficacy. Hepatology 2021, 74, 604A. [Google Scholar]
- Gutfraind, A.; Mackesy-Amiti, M.E.; Tatara, E.R.; Collier, N.T.; Cotler, S.J.; Page, K.; Ozik, J.T.; Boodram, B.; Major, M.E.; Dahari, H. Simulations of HCV Vaccine Trials Reveal Opportunities to Re-Evaluate Vaccine Efficacy. J. Hepatol. 2021, 75, S768. [Google Scholar]
- Harrell, F.E., Jr.; Califf, R.M.; Pryor, D.B.; Lee, K.L.; Rosati, R.A. Evaluating the Yield of Medical Tests. JAMA 1982, 247, 2543–2546. [Google Scholar] [CrossRef]
- Uno, H.; Cai, T.; Pencina, M.J.; D’Agostino, R.B.; Wei, L.J. On the C-Statistics for Evaluating Overall Adequacy of Risk Prediction Procedures with Censored Survival Data. Stat. Med. 2011, 30, 1105–1117. [Google Scholar] [CrossRef]
- Hartman, N.; Kim, S.; He, K.; Kalbfleisch, J.D. Pitfalls of the Concordance Index for Survival Outcomes. Stat. Med. 2023, 42, 2179–2190. [Google Scholar] [CrossRef]
- Steyerberg, E. Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating; Springer: New York, NY, USA, 2009. [Google Scholar]
- DeMaris, A.; Selman, S. Converting Data into Evidence: A Statistics Primer for the Medical Practitioner; Springer: New York, NY, USA, 2013. [Google Scholar]
- Centers for Disease Control and Prevention Principles of Epidemiology. Available online: https://www.cdc.gov/csels/dsepd/ss1978/lesson3/section6.html (accessed on 1 July 2023).
- Friede, T.; Pohlmann, H.; Schmidli, H. Blinded sample size reestimation in event-driven clinical trials: Methods and an application in multiple sclerosis. Pharm. Stat. 2019, 18, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Li, J.; Shu, M. Use of Participation to Prevalence Ratio for Evaluating the Representation Status of Women in Oncology Clinical Trials. JAMA Oncol. 2022, 8, 479–480. [Google Scholar] [CrossRef]
- Khan, S.U.; Khan, M.Z.; Raghu Subramanian, C.; Riaz, H.; Khan, M.U.; Lone, A.N.; Khan, M.S.; Benson, E.-M.; Alkhouli, M.; Blaha, M.J.; et al. Participation of Women and Older Participants in Randomized Clinical Trials of Lipid-Lowering Therapies: A Systematic Review. JAMA Netw. Open 2020, 3, e205202. [Google Scholar] [CrossRef]
- Saltzman, R.G.; Jayaweera, D.T.; Caceres, L.V.; Tovar, J.A.; Vidro-Casiano, M.; Karakeshishyan, V.; Soto, J.; Khan, A.; Mitrani, R.D.; Schulman, I.H.; et al. Demographic Representation in Clinical Trials for Cell-Based Therapy. Contemp. Clin. Trials Commun. 2021, 21, 100702. [Google Scholar] [CrossRef]
- Scott, P.E.; Unger, E.F.; Jenkins, M.R.; Southworth, M.R.; McDowell, T.-Y.; Geller, R.J.; Elahi, M.; Temple, R.J.; Woodcock, J. Participation of Women in Clinical Trials Supporting FDA Approval of Cardiovascular Drugs. J. Am. Coll. Cardiol. 2018, 71, 1960–1969. [Google Scholar] [CrossRef]
- Jin, X.; Chandramouli, C.; Allocco, B.; Gong, E.; Lam, C.S.P.; Yan, L.L. Women’s Participation in Cardiovascular Clinical Trials From 2010 to 2017. Circulation 2020, 141, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T.M.; Lumley, T.; Atkinson, E.; Crowson, C. A Package for Survival Analysis in R. Available online: https://CRAN.R-project.org/package=survival (accessed on 20 July 2022).
- Ishwaran, H.; Kogalur, U.B. Fast Unified Random Forests for Survival, Regression, and Classification (RF-SRC). Available online: https://cran.r-project.org/web/packages/randomForestSRC/index.html (accessed on 20 July 2022).
- R Core Team R. A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2019. [Google Scholar]
- Simon, N.; Simon, R. Adaptive Enrichment Designs for Clinical Trials. Biostatistics 2013, 14, 613–625. [Google Scholar] [CrossRef] [PubMed]
- Mehta, C.R.; Pocock, S.J. Adaptive Increase in Sample Size When Interim Results Are Promising: A Practical Guide with Examples. Stat. Med. 2011, 30, 3267–3284. [Google Scholar] [CrossRef]
- Uozumi, R.; Yada, S.; Kawaguchi, A. Patient Recruitment Strategies for Adaptive Enrichment Designs with Time-to-Event Endpoints. BMC Med. Res. Methodol. 2019, 19, 159. [Google Scholar] [CrossRef]
- Rosenblum, M.; Hanley, D.F. Adaptive Enrichment Designs for Stroke Clinical Trials. Stroke 2017, 48, 2021–2025. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, A.L.; Hudgens, M.G.; Cole, S.R.; Mollan, K.R.; Sax, P.E.; Daar, E.S.; Adimora, A.A.; Eron, J.J.; Mugavero, M.J. Generalizing Evidence from Randomized Trials Using Inverse Probability of Sampling Weights. J. R. Stat. Soc. Ser. A Stat. Soc. 2018, 181, 1193–1209. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Buchanan, A.L.; Cole, S.R. Generalizing Trial Evidence to Target Populations in Non-Nested Designs: Applications to AIDS Clinical Trials. J. R. Stat. Soc. Ser. C Appl. Stat. 2022, 71, 669–697. [Google Scholar] [CrossRef]
- Mansournia, M.A.; Altman, D.G. Inverse Probability Weighting. BMJ 2016, 352, i189. [Google Scholar] [CrossRef]
- Kasereka, S.K.; Zohinga, G.N.; Kiketa, V.M.; Ngoie, R.-B.M.; Mputu, E.K.; Kasoro, N.M.; Kyandoghere, K. Equation-Based Modeling vs. Agent-Based Modeling with Applications to the Spread of COVID-19 Outbreak. Mathematics 2023, 11, 253. [Google Scholar] [CrossRef]
- Paquette, D.; Bryant, J.; de Wit, J. Respondent-Driven Sampling and the Recruitment of People with Small Injecting Networks. AIDS Behav. 2012, 16, 890–899. [Google Scholar] [CrossRef]
- Harris, M.; Rhodes, T. Hepatitis C Treatment Access and Uptake for People Who Inject Drugs: A Review Mapping the Role of Social Factors. Harm Reduct. J. 2013, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.; Johnson, T.; Collins, J.; Corby-Lee, G.; Thacker, J.; White, C.; Hoven, A.; Thornton, A. Risk Factors for Loss to Follow-up of Persons Who Inject Drugs Enrolled at Syringe Services Programs in Kentucky. Int. J. Drug Policy 2021, 95, 103255. [Google Scholar] [CrossRef] [PubMed]
- Darvishian, M.; Wong, S.; Binka, M.; Yu, A.; Ramji, A.; Yoshida, E.M.; Wong, J.; Rossi, C.; Butt, Z.A.; Bartlett, S.; et al. Loss to Follow-up: A Significant Barrier in the Treatment Cascade with Direct-Acting Therapies. J. Viral Hepat. 2020, 27, 243–260. [Google Scholar] [CrossRef]
- Levy, V.; Evans, J.L.; Stein, E.S.; Davidson, P.J.; Lum, P.J.; Hahn, J.A.; Page, K. Are Young Injection Drug Users Ready and Willing to Participate in Preventive HCV Vaccine Trials? Vaccine 2010, 28, 5947–5951. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Bosch, R.J.; Hudgens, M.G. Sensitivity Analysis for the Assessment of Causal Vaccine Effects on Viral Load in HIV Vaccine Trials. Biometrics 2003, 59, 531–541. [Google Scholar] [CrossRef]
- Mewhirter, J.; Sagir, M.; Sanders, R. Towards a Predictive Model of COVID-19 Vaccine Hesitancy among American Adults. Vaccine 2022, 40, 1783–1789. [Google Scholar] [CrossRef]
- Tempalski, B.; Pouget, E.R.; Cleland, C.M.; Brady, J.E.; Cooper, H.L.F.; Hall, H.I.; Lansky, A.; West, B.S.; Friedman, S.R. Trends in the Population Prevalence of People Who Inject Drugs in US Metropolitan Areas 1992–2007. PLoS ONE 2013, 8, e64789. [Google Scholar] [CrossRef]
- Lansky, A.; Abdul-Quader, A.S.; Cribbin, M.; Hall, T.; Finlayson, T.J.; Garfein, R.S.; Lin, L.S.; Sullivan, P.S. Developing an HIV Behavioral Surveillance System for Injecting Drug Users: The National HIV Behavioral Surveillance System. Public Health Rep. 2007, 122, 48–55. [Google Scholar] [CrossRef]
- Huo, D.; Ouellet, L.J. Needle Exchange and Injection-Related Risk Behaviors in Chicago: A Longitudinal Study. JAIDS J. Acquir. Immune Defic. Syndr. 2007, 45, 108–114. [Google Scholar] [CrossRef]
- Boodram, B.; Hotton, A.L.; Shekhtman, L.; Gutfraind, A.; Dahari, H. High-Risk Geographic Mobility Patterns among Young Urban and Suburban Persons Who Inject Drugs and Their Injection Network Members. J. Urban Health 2018, 95, 71–82. [Google Scholar] [CrossRef]
- Boodram, B.; Mackesy-Amiti, M.-E.; Latkin, C. The Role of Social Networks and Geography on Risky Injection Behaviors of Young Persons Who Inject Drugs. Drug Alcohol Depend. 2015, 154, 229–235. [Google Scholar] [CrossRef]
- Temple, R. Enrichment of Clinical Study Populations. Clin. Pharmacol. Ther. 2010, 88, 774–778. [Google Scholar] [CrossRef]
- Ferguson, T.S. Who Solved the Secretary Problem? Stat. Sci. 1989, 4, 282–289. [Google Scholar] [CrossRef]
- Camidge, D.R.; Park, H.; Smoyer, K.E.; Jacobs, I.; Lee, L.J.; Askerova, Z.; McGinnis, J.; Zakharia, Y. Race and Ethnicity Representation in Clinical Trials: Findings from a Literature Review of Phase I Oncology Trials. Future Oncol. 2021, 17, 3271–3280. [Google Scholar] [CrossRef]
- Ma, M.A.; Gutiérrez, D.E.; Frausto, J.M.; Al-Delaimy, W.K. Minority Representation in Clinical Trials in the United States: Trends Over the Past 25 Years. Mayo Clin. Proc. 2021, 96, 264–266. [Google Scholar] [CrossRef] [PubMed]
- Kennedy-Martin, T.; Curtis, S.; Faries, D.; Robinson, S.; Johnston, J. A Literature Review on the Representativeness of Randomized Controlled Trial Samples and Implications for the External Validity of Trial Results. Trials 2015, 16, 495. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Stark, M.; Hesse, M.; Brannath, W.; Zapf, A. Blinded Sample Size Re-Estimation in a Comparative Diagnostic Accuracy Study. BMC Med. Res. Methodol. 2022, 22, 115. [Google Scholar] [CrossRef] [PubMed]
- Venn, M.L.; Knowles, C.H.; Li, E.; Glasbey, J.; Morton, D.G.; Hooper, R. ESCP EAGLE Safe Anastomosis Collaborative Implementation of a Batched Stepped Wedge Trial Evaluating a Quality Improvement Intervention for Surgical Teams to Reduce Anastomotic Leak after Right Colectomy. Trials 2023, 24, 329. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Attia, Z.I.; Behnken, E.M.; Walvatne, K.; Giblon, R.E.; Liu, S.; Siontis, K.C.; Gersh, B.J.; Graff-Radford, J.; Rabinstein, A.A.; et al. Batch Enrollment for an Artificial Intelligence-Guided Intervention to Lower Neurologic Events in Patients with Undiagnosed Atrial Fibrillation: Rationale and Design of a Digital Clinical Trial. Am. Heart J. 2021, 239, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Wermuth, P. Participant Recruitment, Screening, and Enrollment. In Principles and Practice of Clinical Trials; Piantadosi, S., Meinert, C.L., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 257–278. ISBN 978-3-319-52636-2. [Google Scholar]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Attribute | 2018 Chicago PWID Population | Susceptible Population with Receptive Network | HCV-Susceptible Population |
|---|---|---|---|
| Demographic Attributes | |||
| Location (by ZIP Code) | City: 45.4% | City: 27.5% | City: 36.5% |
| Suburbs: 54.6% | Suburbs: 72.5% | Suburbs: 63.5% | |
| Race/Ethnicity | Hispanic: 18.7% | Hispanic: 17.5% | Hispanic: 18.1% |
| NH Black: 20.8% | NH Black: 10.0% | NH Black: 15.5% | |
| NH White: 57.2% | NH White: 69.3% | NH White: 63.2% | |
| Other: 3.2% | Other: 3.2% | NH Other: 3.2% | |
| Sex | Female: 30.6% | Female: 37.8% | Female: 31.5% |
| Male: 69.4% | Male: 62.2% | Male: 68.5% | |
| Age, mean (IQR) | 35.2 (26.0–43.0) | 29.8 (24.0–34.0) | 31.4 (24.9–37.0) |
| Elapsed years of injection drug use, mean (IQR) | 11.3 (3.4–15.6) | 6.3 (2.0–8.6) | 7.2 (2.5–9.9) |
| Enrollment in any harm-reduction (HR) program | HR: 48.4% | HR: 33.1% | HR: 45.5% |
| Non-HR: 51.6% | Non-HR: 66.9% | Non-HR: 54.5% | |
| HCV Infection State | Infected (acute or chronic): 28.1% | 0%—all susceptible | 0%—all susceptible |
| Recovered (antibody-positive): 12.3% | |||
| Behavioral Attributes | |||
| Daily Drug Injections, mean (IQR) | 2.5 (0.9–3.3) | 2.6 (0.9–3.6) | 2.4 (0.8–3.2) |
| Probability of Receptible Sharing, mean (IQR) | 19.4% (0.0–37.3%) | 30.3% (5.0–50.0%) | 21.3% (0.0–40.6%) |
| Network Attributes | |||
| In Degree (Receptive Network Size) | 0 (no network)–68.0% | 0 (no network)–0% | 0 (no network)–68.0% |
| 1–23.5% | 1–75.7% | 1–23.5% | |
| ≥2–8.5% | ≥2–24.3% | ≥2–8.5% | |
| Out Degree (Giving Network Size) | 0 (no network)–72.0% | 0 (no network)–45.0% | 0 (no network)–69.4% |
| 1–20.6% | 1–40.5% | 1–22.7% | |
| ≥2–7.4% | ≥2–14.5% | ≥2–7.9% | |
| Random Sample | In-Network Recruitment | PREDICTEE (Cox Model) | PREDICTEE (RSF Model) | |
|---|---|---|---|---|
| (a) | Matching Chicago’s Susceptible PWID | |||
| Cohort Incidence | 0.024 (0.018–0.033) | 0.055 (0.044–0.068) | 0.097 (0.090–0.104) | 0.149 (0.141–0.155) |
| Required Sample Size (Calculated Using Cohort Incidence) | 1876 (1356–2512) | 802 (642–1010) | 444 (408–480) | 278 (264–294) |
| Expected Number of Candidates Screened Before Achieving Required Sample Size * | 2207 (1595–2955) | 4648 (3721–5853) | 5224 (4800–5647) | 3271 (3106–3459) |
| Post Hoc Power if 800 Recruited | 49.2% (40.5–60.5%) | 80.0% (71.5–87.1%) | 95.5% (94.2–96.7%) | 99.5% (99.3–99.6%) |
| PPRmin ** | - | 0.475 (0.356–0.568) | 0.764 (0.593–0.934) | 0.754 (0.685–0.834) |
| (b) | Matching Arbitrary Balanced Demographics | |||
| Cohort Incidence | 0.024 (0.018–0.033) | 0.055 (0.044–0.068) | 0.085 (0.079–0.095) | 0.137 (0.130–0.144) |
| Required Sample Size (Calculated Using Cohort Incidence) | 1876 (1356–2512) | 802 (642–1010) | 506 (452–550) | 304 (288–322) |
| Expected Number of Candidates Screened Before Achieving Required Sample Size * | 2207 (1595–2955) | 4648 (3721–5853) | 5953 (5318–6471) | 3576 (3388–3788) |
| Post Hoc Power if 800 Recruited | 49.2% (40.5–60.5%) | 80.0% (71.5–87.1%) | 93.1% (91.3–95.2%) | 99.2% (98.9–99.4%) |
| PPRmin *** | 0.433 (0.396–0.472) | 0.250 (0.221–0.280) | 0.903 (0.889–0.918) | 0.807 (0.792–0.821) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, R.; Tatara, E.; Mackesy-Amiti, M.E.; Page, K.; Ozik, J.; Boodram, B.; Dahari, H.; Gutfraind, A. Reducing Sample Size While Improving Equity in Vaccine Clinical Trials: A Machine Learning-Based Recruitment Methodology with Application to Improving Trials of Hepatitis C Virus Vaccines in People Who Inject Drugs. Healthcare 2024, 12, 644. https://doi.org/10.3390/healthcare12060644
Chiu R, Tatara E, Mackesy-Amiti ME, Page K, Ozik J, Boodram B, Dahari H, Gutfraind A. Reducing Sample Size While Improving Equity in Vaccine Clinical Trials: A Machine Learning-Based Recruitment Methodology with Application to Improving Trials of Hepatitis C Virus Vaccines in People Who Inject Drugs. Healthcare. 2024; 12(6):644. https://doi.org/10.3390/healthcare12060644
Chicago/Turabian StyleChiu, Richard, Eric Tatara, Mary Ellen Mackesy-Amiti, Kimberly Page, Jonathan Ozik, Basmattee Boodram, Harel Dahari, and Alexander Gutfraind. 2024. "Reducing Sample Size While Improving Equity in Vaccine Clinical Trials: A Machine Learning-Based Recruitment Methodology with Application to Improving Trials of Hepatitis C Virus Vaccines in People Who Inject Drugs" Healthcare 12, no. 6: 644. https://doi.org/10.3390/healthcare12060644
APA StyleChiu, R., Tatara, E., Mackesy-Amiti, M. E., Page, K., Ozik, J., Boodram, B., Dahari, H., & Gutfraind, A. (2024). Reducing Sample Size While Improving Equity in Vaccine Clinical Trials: A Machine Learning-Based Recruitment Methodology with Application to Improving Trials of Hepatitis C Virus Vaccines in People Who Inject Drugs. Healthcare, 12(6), 644. https://doi.org/10.3390/healthcare12060644