
Patient-Reported Outcome and Experience Measures (PROM/PREM) in Patients Undergoing Liver Surgery with Enhanced Recovery after Surgery (ERAS®): An Exploratory Study


Abstract
1. Introduction
- (1)
- Which PROM and PREM can be derived from the post-discharge follow-up telephone calls conducted by the ERAS nurse after liver surgery within the ERAS® pathway?
- (2)
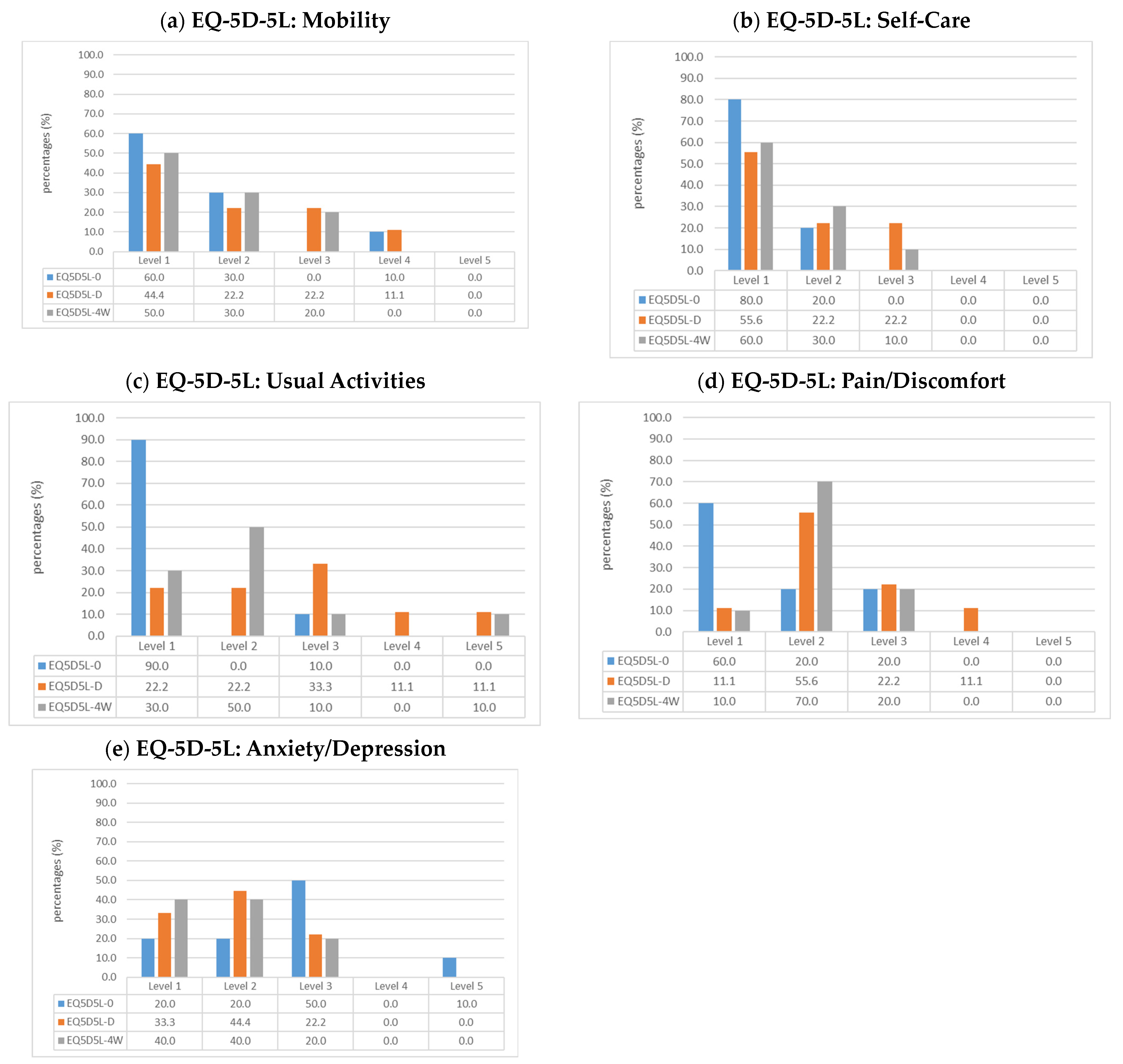
- How does the health status, as evaluated by EQ-5D-5L, change from preoperatively to discharge and then four weeks postoperatively?
- (3)
- How do patients experience the care provided while undergoing liver surgery in the hospital, specifically in relation to interprofessional collaboration and service integration within the ERAS® pathway?
2. Materials and Methods
2.1. Qualitative Content Analysis
2.1.1. Deductive Analysis
2.1.2. Inductive Analysis
2.2. Prospective Questionnaire Survey
2.2.1. EQ-5D-5L
2.2.2. PREM Survey
2.2.3. Measurement Timepoints
- Preoperatively (EQ5D5L-0)
- Postoperatively at discharge (EQ5D5L-D)
- Four weeks postoperatively (EQ5D5L-4W)
2.2.4. Analysis
2.2.5. Study Population
3. Results
3.1. Population Characteristics and Classical Outcomes
3.2. Qualitative Content Analysis
3.2.1. Deductive Qualitative Content Analysis
3.2.2. Inductive Qualitative Content Analysis
3.3. Prospective Quantitative Analysis
3.3.1. EQ-5D-5L Changes over the Three Survey Timepoints
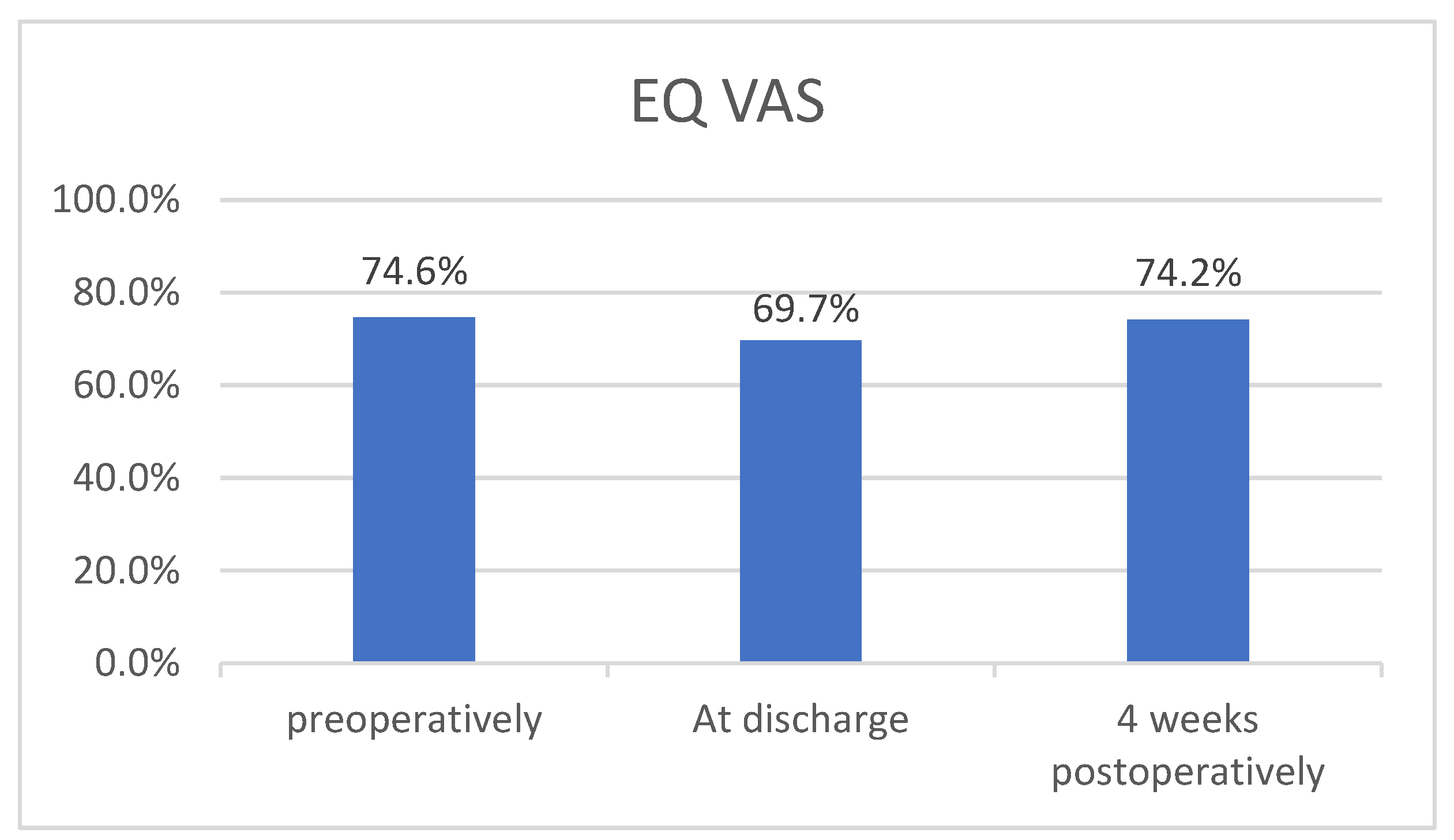
3.3.2. EQ VAS
3.3.3. PREM
4. Discussion
4.1. Qualitative Data
4.2. EQ-5D-5L
4.3. Limitations
4.4. Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Inclusion and Exclusion Criteria
| Inclusion criteria Adult men and women (≥18 years), who undergo liver surgery and are cared for by the interprofessional treatment team in accordance with the ERAS® treatment pathway in one Austrian hospital. |
Benign tumors
|
Elective liver surgery
|
Surgical approach
|
| Exclusion criteria |
| Combined surgery of multiple organs (e.g., surgery for primary rectal cancer and removal of colorectal liver metastases at the same time) |
Additionally for part 1 (retrospective qualitative content analysis)
|
Additionally for part 2 (prospective questionnaire survey)
|
References
- Ljungqvist, O. Enhanced Recovery After Surgery: A Paradigm Shift in Perioperative Care. In Enhanced Recovery after Surgery (ERAS). A Complete Guide to Optimizing Outcomes; Ljungqvist, O., Francis, N.K., Urman, R.D., Eds.; Springer Nature AG: Cham, Switzerland, 2020; pp. 3–9. [Google Scholar]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017, 152, 292. [Google Scholar] [CrossRef]
- Neville, A.; Lee, L.; Antonescu, I.; Mayo, N.E.; Vassiliou, M.C.; Fried, G.M.; Feldman, L.S. Systematic Review of Outcomes Used to Evaluate Enhanced Recovery after Surgery. Br. J. Surg. 2014, 101, 159–170. [Google Scholar] [CrossRef]
- Burch, J.; Balfour, A. Preoperative Patient Education. In Enhanced Recovery after Surgery; Ljungqvist, O., Francis, N.K., Urman, R.D., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 37–49. ISBN 978-3-030-33442-0. [Google Scholar]
- Burch, J.; Fecher-Jones, I.; Balfour, A.; Fitt, I.; Carter, F. What Is an Enhanced Recovery Nurse: A Literature Review and Audit. Gastrointest. Nurs. 2017, 15, 43–50. [Google Scholar] [CrossRef]
- Burch, J. Enhanced Recovery and Nurse-Led Telephone Follow-up Post Surgery. Br. J. Nurs. 2012, 21 (Suppl. S16), S24–S29. [Google Scholar] [CrossRef] [PubMed]
- Feldman, L.S.; Lee, L.; Fiore, J. What Outcomes Are Important in the Assessment of Enhanced Recovery After Surgery (ERAS) Pathways? Can. J. Anesth/J. Can. Anesth. 2015, 62, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Domenghino, A.; Walbert, C.; Birrer, D.L.; Puhan, M.A.; Clavien, P.-A.; The Outcome4Medicine Consensus Group; Jury; Heuskel, D.; Man, N.K.; Monteiro, J.; et al. Consensus Recommendations on How to Assess the Quality of Surgical Interventions. Nat. Med. 2023, 29, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Calvert, M.; King, M.; Mercieca-Bebber, R.; Aiyegbusi, O.; Kyte, D.; Slade, A.; Chan, A.-W.; Basch, E.; Bell, J.; Bennett, A.; et al. SPIRIT-PRO Extension Explanation and Elaboration: Guidelines for Inclusion of Patient-Reported Outcomes in Protocols of Clinical Trials. BMJ Open 2021, 11, e045105. [Google Scholar] [CrossRef]
- Weldring, T.; Smith, S.M.S. Article Commentary: Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). HealthServicesInsights 2013, 6, HSI.S11093. [Google Scholar] [CrossRef]
- Currie, A.; Soop, M.; Demartines, N.; Fearon, K.; Kennedy, R.; Ljungqvist, O. Enhanced Recovery After Surgery Interactive Audit System: 10 Years’ Experience with an International Web-Based Clinical and Research Perioperative Care Database. Clin. Colon. Rectal Surg. 2019, 32, 075–081. [Google Scholar] [CrossRef]
- Fiore, J.F.; Figueiredo, S.; Balvardi, S.; Lee, L.; Nauche, B.; Landry, T.; Mayo, N.E.; Feldman, L.S. How Do We Value Postoperative Recovery?: A Systematic Review of the Measurement Properties of Patient-Reported Outcomes After Abdominal Surgery. Ann. Surg. 2018, 267, 656–669. [Google Scholar] [CrossRef]
- Bowyer, A.; Royse, C.F. Measurement of Recovery Within ERAS. In Enhanced Recovery after Surgery; Ljungqvist, O., Francis, N.K., Urman, R.D., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 323–335. ISBN 978-3-030-33442-0. [Google Scholar]
- Burch, J.; Taylor, C. Patients’ Need for Nursing Telephone Follow-up after Enhanced Recovery. Gastrointest. Nurs. 2012, 10, 51–58. [Google Scholar] [CrossRef]
- Melloul, E.; Hübner, M.; Scott, M.; Snowden, C.; Prentis, J.; Dejong, C.H.C.; Garden, O.J.; Farges, O.; Kokudo, N.; Vauthey, J.-N.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2425–2440. [Google Scholar] [CrossRef]
- Joliat, G.-R.; Kobayashi, K.; Hasegawa, K.; Thomson, J.-E.; Padbury, R.; Scott, M.; Brustia, R.; Scatton, O.; Tran Cao, H.S.; Vauthey, J.-N.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations 2022. World J. Surg. 2023, 47, 11–34. [Google Scholar] [CrossRef]
- Ovaere, S.; Boscart, I.; Parmentier, I.; Steelant, P.J.; Gabriel, T.; Allewaert, J.; Pottel, H.; Vansteenkiste, F.; D’Hondt, M. The Effectiveness of a Clinical Pathway in Liver Surgery: A Case-Control Study. J. Gastrointest. Surg. 2018, 22, 684–694. [Google Scholar] [CrossRef]
- Ni, T.-G.; Yang, H.-T.; Zhang, H.; Meng, H.-P.; Li, B. Enhanced Recovery after Surgery Programs in Patients Undergoing Hepatectomy: A Meta-Analysis. World J. Gastroenterol. 2015, 21, 9209–9216. [Google Scholar] [CrossRef] [PubMed]
- Burchard, P.R.; Dave, Y.A.; Loria, A.P.; Parikh, N.B.; Pineda-Solis, K.; Ruffolo, L.I.; Strawderman, M.; Schoeniger, L.O.; Galka, E.; Tomiyama, K.; et al. Early Postoperative ERAS Compliance Predicts Decreased Length of Stay and Complications Following Liver Resection. HPB 2022, 24, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- ENCARE A.B. ERAS® Qualified Centers. Available online: https://encare.net/map/ (accessed on 12 January 2024).
- Mayring, P. Qualitative Inhaltsanalyse. Grundlagen und Techniken, 13th revised ed.; Julius Beltz GmbH & Co. KG: Weinheim, Germany, 2022; ISBN 978-3-407-25898-4. [Google Scholar]
- Mokkink, L.B.; De Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN Risk of Bias Checklist for Systematic Reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; De Vet, H.C.W. The COSMIN Checklist for Assessing the Methodological Quality of Studies on Measurement Properties of Health Status Measurement Instruments: An International Delphi Study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef]
- Donsel, P.O.; Missel, M. What’s Going on after Hospital?—Exploring the Transition from Hospital to Home and Patient Experiences of Nurse-led Follow-up Phone Calls. J. Clin. Nurs. 2021, 30, 1694–1705. [Google Scholar] [CrossRef]
- Black, N.; Varaganum, M.; Hutchings, A. Relationship between Patient Reported Experience (PREMs) and Patient Reported Outcomes (PROMs) in Elective Surgery. BMJ Qual. Saf. 2014, 23, 534–542. [Google Scholar] [CrossRef]
- National Health Service NHS Patient Experience Framework. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/215159/dh_132788.pdf (accessed on 29 December 2023).
- EuroQol Research Foundation EQ-5D-5L User Guide. Available online: https://euroqol.org/publications/user-guides/ (accessed on 28 May 2023).
- Benson, T.; Benson, A. Routine Measurement of Patient Experience. BMJ Open Qual. 2023, 12, e002073. [Google Scholar] [CrossRef]
- Benson, T.; Potts, H.W. A Short Generic Patient Experience Questionnaire: HowRwe Development and Validation. BMC Health Serv. Res. 2014, 14, 499. [Google Scholar] [CrossRef]
- Devlin, N.; Parkin, D.; Janssen, B. An Introduction to EQ-5D Instruments and Their Applications. In Methods for Analysing and Reporting EQ-5D Data; Springer International Publishing: Cham, Switzerland, 2020; pp. 1–22. ISBN 978-3-030-47621-2. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Dokmak, S.; Ftériche, F.S.; Borscheid, R.; Cauchy, F.; Farges, O.; Belghiti, J. 2012 Liver Resections in the 21st Century: We Are Far from Zero Mortality. HPB 2013, 15, 908–915. [Google Scholar] [CrossRef]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.-A. The Comprehensive Complication Index: A Novel Continuous Scale to Measure Surgical Morbidity. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vandrevala, T.; Senior, V.; Spring, L.; Kelliher, L.; Jones, C. ‘Am I Really Ready to Go Home?’: A Qualitative Study of Patients’ Experience of Early Discharge Following an Enhanced Recovery Programme for Liver Resection Surgery. Support. Care Cancer 2016, 24, 3447–3454. [Google Scholar] [CrossRef]
- Wang, D.; Hu, Y.; Liu, K.; Liu, Z.; Chen, X.; Cao, L.; Zhang, W.; Li, K.; Hu, J. Issues in Patients’ Experiences of Enhanced Recovery after Surgery (ERAS) : A Systematic Review of Qualitative Evidence. BMJ Open 2023, 13, e068910. [Google Scholar] [CrossRef]
- Cusack, M.; Taylor, C. A Literature Review of the Potential of Telephone Follow-up in Colorectal Cancer. J. Clin. Nurs. 2010, 19, 2394–2405. [Google Scholar] [CrossRef]
- Spencer, C.L.; Court, E.L.; Francis, N.K. Cognitive Behavior Counseling: Preoperative Preparation in ERAS. In Enhanced Recovery after Surgery; Ljungqvist, O., Francis, N.K., Urman, R.D., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 101–103. ISBN 978-3-030-33442-0. [Google Scholar]
- Sliwinski, S.; Werneburg, E.; Faqar-Uz-Zaman, S.F.; Detemble, C.; Dreilich, J.; Mohr, L.; Zmuc, D.; Beyer, K.; Bechstein, W.O.; Herrle, F.; et al. A Toolbox for a Structured Risk-Based Prehabilitation Program in Major Surgical Oncology. Front. Surg. 2023, 10, 1186971. [Google Scholar] [CrossRef] [PubMed]
- EORTC Quality of Life Group Website EORTC—Quality of Life of Cancer Patients. Available online: https://qol.eortc.org/questionnaire/eortc-qlq-c30/ (accessed on 8 September 2023).
- Black, N. Patient Reported Outcome Measures Could Help Transform Healthcare. BMJ 2013, 346, f167. [Google Scholar] [CrossRef]
- Devlin, N.; Pickard, S.; Busschbach, J. The Development of the EQ-5D-5L and Its Value Sets. In Value Sets for EQ-5D-5L; Devlin, N., Roudijk, B., Ludwig, K., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 1–12. ISBN 978-3-030-89288-3. [Google Scholar]
- Jenkins, D.G.; Quintana-Ascencio, P.F. A Solution to Minimum Sample Size for Regressions. PLoS ONE 2020, 15, e0229345. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Sample Size Justification. Collabra Psychol. 2022, 8, 33267. [Google Scholar] [CrossRef]
- Vanbrabant, L.; Van De Schoot, R.; Rosseel, Y. Constrained Statistical Inference: Sample-Size Tables for ANOVA and Regression. Front. Psychol. 2015, 5, 1565. [Google Scholar] [CrossRef] [PubMed]
- Devlin, N.J.; Parkin, D.; Browne, J. Patient-Reported Outcome Measures in the NHS: New Methods for Analysing and Reporting EQ-5D Data. Health Econ. 2010, 19, 886–905. [Google Scholar] [CrossRef]
- Lee, L.; Tran, T.; Mayo, N.E.; Carli, F.; Feldman, L.S. What Does It Really Mean to “Recover” from an Operation? Surgery 2014, 155, 211–216. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Qualitative Content Analysis N = 13 | Prospective Questionnaire Survey N = 10 | |
|---|---|---|
| Age [years] | ||
| Mean ± SD | 55.5 ± 10.0 | 62.8 ± 11.5 |
| Median | 56 | 65 |
| Sex | ||
| Male | 46.2% | 70.0% |
| Female | 53.8% | 30.0% |
| Surgical approach | ||
| Robotic | 61.5% | 70.0% |
| Standard Laparoscopic | 23.2% | 20.0% |
| Open | 15.3% | 10.0% |
| Main procedure name | ||
| Segmentectomies/Atypical resections | 61.5% | 80.0% |
| Wegde resections | 10.0% | |
| Extended left hemihepatectomy | 15.4% | |
| Right hemihepatectomy | 23.1% | |
| Extended right hemihepatectomy | 10.0% | |
| Histological diagnosis | ||
| Colorectal liver metastasis | 53.8% | 30.0% |
| Non-colorectal/non-neuroendocrine liver metastases | 7.7% | 10.0% |
| Perihilar cholangiocarcinoma | 7.7% | |
| Intrahepatic cholangiocellular carcinoma | 7.7% | |
| Hepatocellular carcinoma | 30.0% | |
| Hepatocellular adenomas | 15.4% | |
| Hemangioma | 10.0% | |
| Other benign disease | 7.7% | 20.0% |
| Oncological diagnosis | ||
| Yes | 76.9% | 70.0% |
| No | 23.1% | 30.0% |
| Qualitative Content Analysis N = 13 | Prospective Questionnaire Survey N = 10 | |
|---|---|---|
| LOS 1 [days] | ||
| Mean ± SD | 7.1 ± 6.0 | 8.8 ± 11.8 |
| Median | 6.0 | 5.0 |
| Complications [CD 2] | ||
| No complications | 61.5% | 60.0% |
| CD I | 7.7% | 0% |
| CD II | 15.4% | 30.0% |
| CD IIIa | 15.4% | 10.0% |
| Readmission 3 | 7.7% | 10.0% |
| Mean (N = 10) | |
|---|---|
| Interprofessional care services 1 | |
| Friendliness | 1.00 |
| Listening and explaining | 1.20 |
| Waiting times | 1.40 |
| Appointment coordination | 1.30 |
| Feeling informed | 1.30 |
| Interprofessional collaboration 2 | |
| Professionals talk to each other | 1.20 |
| Staff know what others are doing | 1.20 |
| I don´t have to repeat my story | 1.30 |
| Different professionals work well together | 1.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rappold, D.; Stättner, S.; Nöhammer, E. Patient-Reported Outcome and Experience Measures (PROM/PREM) in Patients Undergoing Liver Surgery with Enhanced Recovery after Surgery (ERAS®): An Exploratory Study. Healthcare 2024, 12, 629. https://doi.org/10.3390/healthcare12060629
Rappold D, Stättner S, Nöhammer E. Patient-Reported Outcome and Experience Measures (PROM/PREM) in Patients Undergoing Liver Surgery with Enhanced Recovery after Surgery (ERAS®): An Exploratory Study. Healthcare. 2024; 12(6):629. https://doi.org/10.3390/healthcare12060629
Chicago/Turabian StyleRappold, Daniela, Stefan Stättner, and Elisabeth Nöhammer. 2024. "Patient-Reported Outcome and Experience Measures (PROM/PREM) in Patients Undergoing Liver Surgery with Enhanced Recovery after Surgery (ERAS®): An Exploratory Study" Healthcare 12, no. 6: 629. https://doi.org/10.3390/healthcare12060629
APA StyleRappold, D., Stättner, S., & Nöhammer, E. (2024). Patient-Reported Outcome and Experience Measures (PROM/PREM) in Patients Undergoing Liver Surgery with Enhanced Recovery after Surgery (ERAS®): An Exploratory Study. Healthcare, 12(6), 629. https://doi.org/10.3390/healthcare12060629