Abstract
The present study seeks to evaluate the factors determining the continuance intention to use hearing aids in older adults. This cross-sectional study was carried out in 2021. The technology post-acceptance model (PAM) framework was used to develop a model for the continuance intention to use hearing aids. In total, 300 hearing aid users aged ≥60 years, who were selected via a randomized stratified sampling method, completed the self-evaluation tools used in this study. With a mean age of 71.38 years (SD = 8), the participants comprised 50.7% and 49.3% females and males, respectively. The path analysis results showed that the continuance intention to use hearing aids was positively and significantly influenced by the actual use of hearing aids, the perceived benefits, satisfaction, confirmation, self-efficacy in using hearing aids, an extraverted personality trait, self-perceived hearing handicap, and perceived social support. The main results of the present study can help hearing care providers develop a better understanding of older users to design effective rehabilitation strategies and ensure their continuance intention to use hearing aids.
1. Introduction
Presbycusis or age-related hearing loss is the most common hearing loss in humans, and is observed in around 10.9–17.6% of people aged 60–69 years, 41.9–51.2% of those aged 80–89 years, and 52.9–64.9% people aged ≥90 years [1,2]. Experts suggest that no compensation for or correction of hearing loss can impact various mental and emotional health aspects of older adults. For instance, prolonged deprivation of the sense of hearing brings about changes in the central nervous system that eventually lead to dementia [3,4].
Using hearing aids is the most convenient solution to compensate for hearing loss in older adults. Hearing aids can largely make up for the communicational problems and defects stemming from hearing loss and increase the health-related quality of life in the elderly [5]. Yet, many older adults are not willing to receive hearing aids and use hearing rehabilitation services [6]. Furthermore, the results of several studies suggest that around 30–50% of the elderly do not use them regularly or set them aside permanently [7,8,9]. Thus, identifying and understanding the role of the real determinants of the actual and continuous use of hearing aids can significantly help us develop effective interventions and promote the use of hearing aids in the elderly suffering from hearing loss [10].
Three review studies have summarized the results of other relevant studies and reported that factors such as socioeconomic status, educational level, the severity of hearing loss, insertion gains, perceived hearing handicap, the personality traits of the elderly, and positive social support could play vital roles in the acceptance and use of hearing aids [11,12,13]. These studies highlighted the role of psychosocial factors, attitudes, and beliefs, and suggested that the reasons behind not using hearing aids were beyond the features and performance of hearing aids, given the advancements in the technology and appearance of modern hearing aids [14]. Hence, audiologists have partnered with health psychologists in recent years to explain the predictors of a person using hearing aids and other hearing rehabilitation interventions through the application of social psychology and health models and theories [15].
A review of the studies that have so far used these models—e.g., the health belief model [15,16], theory of planned behavior [17], and the theory of reasoned action [18]—indicates that they mostly focus on the factors and behaviors that determine the acceptance intention or the early stages of receiving hearing aids. Some researchers argue that the psychosocial and behavioral aspects influencing the use of technology or the adopting of a new health behavior change over time and across various stages of acceptance [19]. Thus, a model investigating the behaviors affecting the post-acceptance stage of receiving hearing aids—that is, the continuous and actual use of hearing aids—in older adults is among the research gaps that have yet to be addressed, to the best of our knowledge. Therefore, the present study proposes a model to examine the behaviors of hearing aid users in the stages following the prescription of hearing aids.
2. Theoretical Background and Research Framework
The determinants of technology acceptance are often investigated in four stages, including (1) familiarization with the technology, (2) the intention to use the technology, (3) the acceptance of the technology, and (4) the post-acceptance stage of the technology [20]. The theories of reasoned action, planned behavior, technology acceptance, and expectation-confirmation are among the most renowned theories examining user behaviors at various stages of technology acceptance [21]. For instance, Cobelli et al. [18] used Ajzen’s theory of reasoned action to identify the factors affecting the intention to use hearing aids. Meister et al. [17] used the planned behavior theory to evaluate the determinants of hearing aid acceptance intention. Laplante et al. [22] used the theory of change stages to present a model for the stage of change in hearing rehabilitation in older adults suffering from hearing loss. Saunders et al. [16] investigated hearing health behaviors based on the framework of the health belief model.
Few studies have relied on these theories to examine the actual use of hearing aids at the post-fitting stage [23,24]. According to researchers, the impact of the perceptions and attitudes of individuals on their use of hearing aids might vary before and after their initial acceptance of hearing aids, due to their experience of using hearing aids and their practical application in daily life [16,25]. In other words, identifying practical and effective methods to improve the use of hearing aids or any other assistive devices would be extremely difficult without an adequate understanding of users’ attitudes and behaviors throughout the whole rehabilitation process.
2.1. Expectation-Confirmation Theory (ECT)
Several studies beyond the scope of health have sought to employ technology post-acceptance models to explain users’ behaviors in the post-acceptance stage [26,27,28]. In this group of studies, the ECT (Oliver 1980) is widely used and explains user satisfaction and their intentions toward the continued use of goods and services [29]. This theory suggests that satisfaction with a product is a function of their expectation, performance, and confirmation. This model consists of four interconnected sections; the first stage is the individual’s expectation. At this stage, users form their initial expectations based on their previous experiences, the knowledge available to them, and their interaction with various people regarding specific goods or services, without purchasing or receiving them [30]. The second stage is the perceived benefits of the product’s performance, in which people receive a product if they deem it to be useful [26]. The third stage is the confirmation or rejection of their beliefs. After a period of using the product, users form their perception of the product’s performance based on their initial expectations and decide the extent to which their expectations are met. Confirmation occurs if the product is better than expected, while rejection occurs when the users’ assessments are lower than expected [31]. The fourth stage is satisfaction with the product, in which users’ confirmation of the product informs their sense of satisfaction. Satisfied users generally continue their use of the product, and unsatisfied users might cease their use of the product [32].
Overall, confirmation and satisfaction are the two fundamental principles of the expectation-confirmation theory that influence the intention to repurchase or continue the use of a product [33]. Wong et al. (2004) [34] and Meyer et al. (2014) [35] examined the relationship between the expectation of and satisfaction with hearing aids using the expectation-confirmation model. Wong et al. [34] investigated 42 hearing aid users with an average age of 64.2 years (SD = 14.8) in Hong Kong and reported a positive and significant relationship between confirmation and satisfaction with hearing aids, but they observed no direct relationship between expectations and a satisfaction with hearing aids. Meyer et al. [35] studied 123 hearing aid users with a mean age of 72 years (SD = 7) and found that satisfaction with the hearing aids was associated with confirmation, hearing ability in various environments, appearance features, and ease of use, based on their logistic regression results.
2.2. Post-Acceptance Model (PAM)
Given that some constructs of the expectation-confirmation model have been associated with the pre-acceptance stage of the technology, Bhattacherjee (2001) made modifications to this theory and integrated it with Davis’s technology acceptance model (TAM) to propose a PAM to explain the behaviors and beliefs of users at the stage of using the technology [26,36]. This model focuses on the key role of the two concepts of satisfaction and confirmation and their influence on improving the continuance intention to use the technology. In this model, technology confirmation obtained through comparing users’ expectations before using the technology to its real performance increases their satisfaction with technology and leads to their continuance intention of its use. The PAM’s reasoning indicates that the two constructs of satisfaction and confirmation cover the factors influencing the pre-acceptance stage; additionally, the expectation of individuals may vary throughout their use of the technology. Therefore, the PAM interprets and evaluates the expectations at the stage of using the technology as the perceived benefits [26,37]. As a result, the model assumes that the confirmation of technology impacts its perceived benefits and satisfaction. The users then decide whether or not to continue using the technology based on its benefits and their satisfaction with it. Several studies have developed a PAM to investigate factors affecting the continuance intention to use various types of technology [38,39,40].
For instance, Cho et al. [41] employed a PAM to investigate factors influencing the continued use of health applications in 343 participants in South Korea. Their results suggested that 58.6% of the variation in continuance intention to use health applications was explained by the constructs of the model proposed in the study.
2.3. Extended Post-Acceptance Model (PAM)
The determinants of technology use may vary depending on the type of the technology, its application, and the user community. Many researchers have recommended the development of technology acceptance models by adding other influential constructs [42]. The results of previous studies show that factors such as self-efficacy in using hearing aids, perceived hearing handicap, personality traits, and perceived social support play determining roles in hearing aid outcomes (use, benefits, and satisfaction) [11,12,13]. Therefore, the present study added these mentioned constructs to the original PAM and developed a model of the continuance intention to use hearing aids based on the PAM’s framework. The following subsections explain the causal relationships between the constructs of the proposed model.
2.4. Confirmation
The post-acceptance theory suggests that satisfaction with the technology will increase if its performance is confirmed through its usage [43]. Moreover, confirmation of the technology positively affects its perceived benefits, which means that the user will find the technology useful if its performance is compliant with their expectations [26]. Although the influence of confirmation on the satisfaction with and benefits of hearing aids has yet to be investigated using the PAM, several studies have confirmed this relationship using the expectation-confirmation model [44,45,46].
2.5. Perceived Benefits
According to Davis and Venkatesh, perceived benefits refer to the extent to which the individual believes that the use of a system will increase their performance [36,47]. The original technology acceptance model (TAM) emphasizes the direct influence of perceived benefits on a person’s attitude toward a type of technology, which will eventually determine their intention to continue using the technology [48,49]. Since satisfaction is a positive stage of feelings and attitude, the perceived benefits can have a positive relationship with the satisfaction with technology [38]. A significant impact of perceived benefits on satisfaction with hearing aids (0.5–0.83; p ≤ 0.05), examined using self-evaluation tools, has been reported in previous studies [50,51]. Moreover, several studies have reported that perceived benefits had a significant relationship with the actual use of hearing aids [7,23,52].
2.6. Satisfaction
Satisfaction can be defined as a pleasant feeling and experience when evaluating the product’s performance compared to expectations about it [43]. Satisfaction is an extremely essential factor in the process of hearing aid prescription [53]. Patients who are satisfied with their hearing aids generally use them regularly, whereas a low level of satisfaction is among the main reasons to abandon the use of hearing aids in most patients who do not use their hearing aids [34,54].
2.7. Hearing Aid Self-Efficacy
Self-sufficient people generally tend to resist their encountered obstacles and adopt new behaviors to manage their health conditions. Hearing aid self-efficacy can be defined as the level of self-confidence and capability of an individual in using hearing aids [55]. Several studies have demonstrated that the elderly people suffering from hearing impairment who were adequately self-sufficient used hearing aids more successfully. Thus, self-efficacy can be considered among the predictors affecting the benefits, satisfaction, and use of hearing aids [23,46].
2.8. Extraverted Personality Trait
Several studies suggest that extroverts benefit more from their hearing aids and have a higher level of satisfaction and hours of hearing aid usage than introverts [56,57,58].
2.9. Perceived Social Support
Recent studies have reported considerable correlations between positive social support and longer use of hearing aids. These studies suggest that the accessibility of social support, encouragement, and the presence of associates in rehabilitation programs are factors that eventually increase the successful use of hearing aids in those suffering from hearing loss [53,59].
2.10. Self-Perceived Hearing Handicap
According to the World Health Organization, self-perceived hearing handicap refers to the non-hearing consequences, such as emotional distress and restricted social participation, directly caused by a disorder in the hearing structure [60]. The results of several studies indicate that people who more often reported their hearing problems used their hearing aids for longer hours [5,61,62].
2.11. Actual Use and Continuance Intention to Use
There is no agreed-upon definition for the actual use of hearing aids in the literature on hearing. However, the definition of actual and successful hearing aid use suggested by Hickson et al. (2014)—reporting at least one hour of daily hearing aid use and receiving the least moderate benefits in situations where the individuals need to hear better—appears to be more rational than the definitions relying merely on the number of hours hearing aids are used for [23]. The continuance intention to use a type of technology refers to the intentions of users to continue their use of a specific technology [26]. This means that the continuance intention to use could predict the future use of technology. At the stage following the acceptance of hearing aids, users use their hearing aids and may either continue or discontinue using them. Thus, the actual use of hearing aids can influence the continuance intention to use them.
3. Materials and Methods
3.1. Participants
In the present cross-sectional study, the participants were 300 hearing aid users (60 years or older) residing in Tehran. In the sampling process, Tehran was divided into four zones, namely low, lower–moderate, upper–moderate, and high in terms of socioeconomic development levels [63]. Several audiology clinics were then randomly contacted in each zone to collect the address and contact information of the older adults who had received hearing aids from these clinics. Next, the elderly were classified into four categories based on their place of residence. Eventually, 75 people from each category were randomly selected (through a draw) as the research sample group. The inclusion criteria were its having been at least 6 months after their hearing aid prescription (unilateral and bilateral hearing aid fitting), their ability to communicate and good command of the Persian language to respond to the questions, and consent to participate in the study voluntarily. The exclusion criteria were reluctance to keep participating in the study, incomplete completion of questionnaires, and physical or mental discomfort in completing the questionnaires.
3.2. Measurement Scales
In the present study, the data were collected using several self-evaluation tools, demographic information forms, and the last recorded audiograms of the individuals. Table 1 explains the details and reliability of the tools used in the present study. Translation and psychometrics of the three questionnaires were carried out before executing the study, as detailed below.
3.2.1. Continuance Intention and Confirmation Scales
Given the lack of a special tool to assess the confirmation and continuance intention to use hearing aids, the present study uses the constructs of the general PAM questionnaire (Bhattacherjee 2001), which is a 12-item tool scored on a five-point Likert scale. This tool has been used in several studies to evaluate the factors affecting the use of technologies such as health applications, information technologies, cellphones, etc. [26,27,37]. Thus, the constructs of continuance intention to use (three items) and confirmation (three items) in this questionnaire were translated into Persian, and their face and content validity were evaluated and confirmed by a group of experts consisting of 10 audiology and geriatric specialists. The Content Validity Ratio (CVR) and Content Validity Index (CVI) of the two scales of confirmation and continuance intention to use were higher than 0.85 and 0.90, respectively, indicating the favorable content validity of the scales. The internal consistency of the questionnaire items was calculated at α = 0.74 and α = 0.83 for continuance intention to use and confirmation, respectively, using Cronbach’s alpha, suggesting the appropriate internal reliability of the two tools.
3.2.2. Hearing Aid Self-Efficacy Questionnaire
Self-efficacy was evaluated using the Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids (MARS-HA) [64], consisting of 24 questions and four subscales. To score the questions, the respondents must assign to each question a score on a 10-unit interval scale (0, 10, …, 100%), specifying their level of confidence in their ability. A score of zero means that the respondents feel they have no skill or ability, and a score of 100 means that the respondents are completely confident when performing this skill. Higher scores in this questionnaire indicate higher self-efficacy. This questionnaire was also translated into Persian, and its face and content validity were evaluated and confirmed by a group of experts. The calculated CVR and CVI indices were, respectively, >0.80 and 0.91 for this questionnaire. The internal consistency of the questionnaire items was calculated as α = 0.94 using Cronbach’s alpha.

Table 1.
The characteristics of the questionnaires.
Table 1.
The characteristics of the questionnaires.
| Construct | Instruments | Description/Scale | Cronbach’s α |
|---|---|---|---|
| Satisfaction | Persian version of Satisfaction with Amplification in Daily Life (SADL) [65]. | A 15-item questionnaire that evaluates the satisfaction that people feel with their current hearing aids. It quantifies satisfaction using a global score and four subscales: Positive Effect, Service and Cost, Negative Features, and Personal Image. The SADL response scale: 7-point Likert (not at all; a little; somewhat; medium; considerably; greatly; tremendously) | 0.91 |
| Perceived benefit | Persian version of Abbreviated Profile of Hearing Aid Performance (APHAP) [66]. | A 24-item self-assessment inventory that is divided into four subscales that assess communication, including situations in favorable environments (EC scale) and experiences in the presence of noise (BN scale), reverberating rooms (RV scale), and loud sounds (AV scale). The APHAP response scale: A. Always (99%), B. Almost Always (87%), C. Generally, (75%), D. Half the time (50%), E. Occasionally (25%), F. Seldom (12%), G. Never (1%) | 0.92 |
| Actual use | Persian version of the International Outcome Inventory for Hearing Aids (IOI-HA) [67]. | In this study, we defined the actual use of hearing aids based on each participant’s self-report responses to question 1 (average hours of hearing aid use per day) and question 2 (the benefit from hearing aids in the situations where the individual most wanted to hear better) on the IOI-HA. Response scale: 5-point Likert; question 1 (none = 1 … to more than 8 h a day = 5), question 2 (helped not at all = 1 … helped very much = 5) | 0.85 |
| Self-perceived hearing handicap | Persian version of the Hearing Handicap Inventory Screening Version for the Elderly (HHIE-S) [68]. | A 10-item questionnaire that evaluates how an individual perceives the social and emotional effects of hearing impairment. Response scale: 3-point Likert (No = 0; Sometimes = 2; Yes = 4) | 0.85 |
| Perceived social support | The Iranian version of the Multidimensional Scale of Perceived Social Support (MSPSS) [69]. | A 12-item measure of the perceived adequacy of social support from three sources: family, friends, and significant other Response scale: 5-point Likert (strongly disagree = 0, strongly agree = 5) | 0.93 |
| Extraverted personality trait | Persian version of the Ten-Item Personality Inventory (TIPI) [70]. | In this study, we used questions 1 and 6 of the Ten-Item Personality Inventory that evaluates the personality trait of extraversion. Response scale: a 7-point scale ranging from 1 = strongly disagree to 7 = strongly agree | 0.64 |
3.3. Data Analysis
Data were analyzed using descriptive statistics and analytical tests, including Pearson’s correlation coefficient, an independent t-test, a one-way analysis of variance (ANOVA), and multiple linear regression, using the SPSS V.24 software. The relationships between the main research variables were simultaneously analyzed using SEM (structural equation modeling) (path analysis through maximum likelihood estimation) in AMOS V.24 software. The model fit and the consistency between experimental data and the conceptual model were examined using the goodness of fit (GOF) indices and criteria. In the present study, the GOF indices included X2/Df, RMSEA, GFI, and TLI, which were used to measure the final GOF of the model.
4. Results
The mean age of the participants was 71.38 years (SD = 8), ranging between 60 and 95 years. In terms of gender, 49.30% and 50.70% of the respondents were male and female, respectively. Table 2 details the demographic information of the participants. The results of the bivariate analyses indicated that factors such as age (r = −0.16, p ˂ 0.001), level of education (F (4, 295) = 12.29, p ≤ 0.001), employment status (F (3, 296) = 4.3, p ˂ 0.001), and the type of hearing aids (F (2, 297) = 7.09, p ≤ 0.001) had significant relationships with the actual use of hearing aids. However, no significant relationship was observed between actual hearing aid use and other audiological factors (p > 0.05) (Table 3). Among all the audiological factors and demographic variables (Table 3), the results suggested that only the type of hearing aids had a significant relationship with the continued use of hearing aids (F (2, 297) = 6.87, p ≤ 0.001). Descriptive results from the main research variables indicated that 63.3% of hearing aid users had actual use of, while 36.7% failed in the actual use of, their hearing aids. The overall average values of actual hearing aid use and continuance intention to use hearing aids were, respectively, 6.12 (SD = 2.19) and 10.14 (SD = 2.91), which indicate a moderate level of actual use and continuance intention to use hearing aids among the participants, considering the mean values of the questionnaires. The analysis of Pearson’s correlation revealed a significant and positive relationship between the actual use and the continuance intention to use hearing aids (r = 0.67, p < 0.01). Table 4 lists the descriptive data and correlation coefficients between the research variables.
Table 2.
Participants’ demographic information (N = 300).
Table 3.
Correlation analysis of demographic variables (n = 300).
Table 4.
Descriptive statistics of the Pearson correlation coefficients between variables.
4.1. Findings from Multiple Linear Regression
The prediction power of all the significant variables in Table 3 and Table 4 (p-value < 0.2) in predicting the actual use and continuance intention to use hearing aids was examined using a multivariate analysis. In this study, the assumptions of the linear regression included data normality (all the variables had kurtosis and skewness ranges of −2, 2 according to the tests) and a residual normality test, and the mean standardized residual error was calculated as close to zero for all models, and their standard deviation was calculated as close to one. Durbin–Watson test values confirmed the independence of the errors, meaning the obtained values were between 1.5 and 2.5. The multiple collinearity test revealed that the VIF values for the independent research variables were <3 and the tolerance values were >0.25, indicating no collinearity between the independent research variables. Dummy variables were used to include the qualitative variables in the regression analysis.
Table 5 shows the characteristics and statistics related to the fitting of the regression models. The F value and the significance level of the regression models indicated a statistically significant relationship between the dependent variables—namely actual use and continue intention to use hearing aids—and the independent research variables (p < 0.001). In the actual hearing aid use model, the variables included in the equation explained 69% (R2 = 69) of the real variations in the actual use of hearing aids by the participants.
Table 5.
Model summary of actual use and continuance intention to use hearing aids.
The Beta values indicated that, among the demographic variables, high school education level and higher had a positive impact on the actual use of hearing aids (β = 0.08, p ≤ 0.05), while the use of analog hearing aids (β = −0.08, p ≤ 0.05) and unemployment (β = −0.12, p ≤ 0.005) had negative impacts on the actual use of hearing aids. Of the main variables, factors such as perceived benefits (β = 0.22, p ˂ 0.001), confirmation (β = 0.26, p ˂ 0.001), self-perceived hearing handicap (β = 0.19, p ˂ 0.001), and hearing aid satisfaction (β = 0.18, p ˂ 0.01) were the best predictors of the use of hearing aids. In the model of continuance intention to use hearing aids, the independent variables explained 60% (R2 = 60) of the variation in the continuance intention to use hearing aids. β values in the model indicated that the influence of a low education level (β = −0.10, p ˂ 0.04) and the use of analog hearing aids (β = −0.08, p ˂ 0.03) had negative impacts on the continuance intention to use hearing aids. Confirmation (β = 0.22, p ˂ 0.001) and the actual use of hearing aids (β = 0.43, p ˂ 0.01) had the greatest influence on the continuance intention to use hearing aids.
4.2. Results from SEM
The values of the GOF indices, after making the necessary modifications based on the modified indices in the final model, resulting from the SEM were CMIN = 2.52, RMSEA = 0.07, GFI = 0.87, and CFI = 0.92, which are suitable GOF indices and reveal the confirmation of the proposed research model. Moreover, Table 6 summarizes the final model’s GOF indices and their recommended values. Standard regression weights, standard error, significance levels, and the critical ratio (CR) were investigated to confirm or reject the causal relationships between the research variables (Table 7). Figure 1 demonstrates the final research model in its standard state.
Table 6.
Results of the goodness of fit test.
Table 7.
Standardized path coefficients from the structural equation modeling analysis.
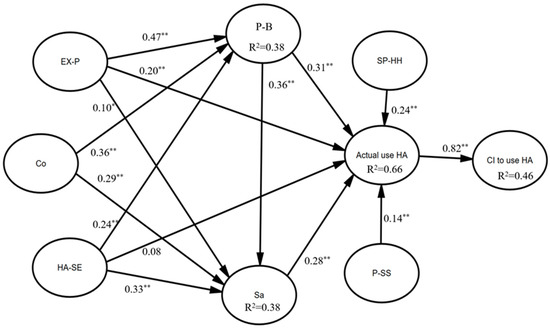
Figure 1.
Results of path analysis. Note: p ˂ 0.05 = *, p ˂ 0.001 = **; CI = continuance intention to use hearing aid; Co = confirmation; Sa = satisfaction; P-B = perceived benefit; SP-HH = self-perceived hearing handicap; HA-SE = hearing-aid self-efficacy; EX-P = extraverted personality trait; P-SS = perceived social support; HA = hearing aid.
5. Discussion
The present research mainly sought to evaluate the determinants of the continuance intention to use hearing aids in older adults. The mean continuance intention to use hearing aids was at a moderate level, and 36.7% of the participants did not actually use their hearing aids. Using similar criteria, the Hickson et al. (2014) study found that 46% of their participants were unsuccessful in using their hearing aids [23]. Overall, this result from the present study is consistent with some other studies, suggesting no regular use of hearing aids in 30–50% of the elderly [71,72].
5.1. Demographic and Audiological Characteristics
The relationships between the actual use and continuance intention to use hearing aids and several demographic variables such as age, gender, and marital status were not significant according to the results of our multivariate analysis. Similarly, some other studies suggest that factors such as age, gender, and marital status cannot determine the amount of use of hearing aids when several other predictors are incorporated into the multivariate model [52,62,73]. However, some studies (e.g., Klyn et al., 2019) reported that women used hearing aids significantly less than men [74], while Ji-Su (2015) found that older adults in the age group of 60–64 used hearing aids for longer times than older groups [75].
Among the demographic variables, a higher education level and job status (pensioner compared to unemployed) significantly predicted the actual and continued use of hearing aids. It is not surprising that those with higher educational levels and socioeconomic status used hearing aids more often due to their greater feeling of their need for hearing aids, as they are able to afford hearing aids, and have a more prominent presence in the community. Likewise, higher education levels and socioeconomic status positively impacted the use of hearing aids in other studies [76,77,78].
In the present study, the actual use of and continuance intention to use hearing aids had no significant relationships with audiological factors such as the severity of hearing loss, a history of using hearing aids, the types of fittings, and the appearance of hearing aids. In terms of the type of hearing aids, however, analog hearing aids negatively influenced their actual use. Confirming this result, three studies reported that the risk of irregular hearing aid use was higher in analog hearing aids than in more advanced signal-processing hearing aids [79,80,81]. Contrary to the results of the present study, several studies argued that higher degrees of hearing loss were associated with a more frequent use of hearing aids [61,76,82]. The present results corroborate those of Ferguson et al. (2016) and Maeda et al. (2016), who reported that the degree of hearing loss did not determine the regular use of hearing aids [46,62]. Given the factors investigated in the present study, it can generally be understood that demographic features and audiological factors cannot be strong predictors for the actual and continuous use of hearing aids in older adults. Although there is a need to examine other audiological factors, the important role of the beliefs, hearing-associated quality of life, and personality traits of the elderly in their actual and continuous use of hearing aids cannot be overlooked in such studies.
5.2. Extended PAM-Related Constructs
The present study explained the influence of the main research variables on the continuance intention to use hearing aids through the development of a PAM. The results of the path analysis confirmed the positive impact of the perceived benefits of and satisfaction with hearing aids. This means that hearing aid users perceive higher benefits and satisfaction with their hearing aids if they confirm that their experience of using the hearing aids is compliant with or beyond their initial expectations, which will eventually result in the continuous use of hearing aids [45]. Similarly, a direct relationship between the benefits of and satisfaction with hearing aids has been reported in previous studies [32,46,83]. However, one study found that confirmation was not a strong predictor of hearing aid outcomes [84].
The results of several studies have suggested that most successful hearing aid users had a high self-efficacy in using them, and self-efficacy was a significant factor in the adherence to hearing aids [85,86,87]. The present study found that self-efficacy had the greatest impact on the level of satisfaction, followed by the perceived benefits of hearing aids; however, self-efficacy’s direct relationship with the actual use of hearing aids was not significant. This result is consistent with that of Ferguson et al. (2016), who suggested that self-efficacy was associated with satisfaction with hearing aids but that it had no significant relationship with the frequency of the use of hearing aids [46]. Thus, it can be justified that self-efficacy in using hearing aids increases the level of satisfaction and the perceived benefits of hearing aids in users, which will eventually lead to higher actual and continuous hearing aid use. The present study calculated a mean self-efficacy score of 64.58%, which indicates the moderate self-efficacy of the older adults participating in the study. It is thus recommended that audiology experts enhance the self-efficacy beliefs of the elderly in their hearing rehabilitation sessions through an awareness of the potential factors, such as cognitive disorders, physical abilities, or educational levels, influencing self-efficacy in the older population. The results of several studies suggest that reporting a self-perceived hearing handicap—or in other words, reporting the emotional and social effects of a hearing impairment—in daily life can play a determining role in all aspects of hearing aid use [61,62,88]. In the present study, the path coefficient also indicated that higher scores in the hearing handicap variable were among the determinants of actual hearing aid use, meaning that the individual needs to achieve a significant understanding of the emotional and social impacts of hearing loss to make actual use of their hearing aids. However, several studies suggest that a perceived hearing handicap may be influenced by non-audiological factors such as ethnicity, gender, language, educational level, and the individual’s health conditions. For instance, those of a slightly older age may consider their hearing loss a natural consequence of age and report it less frequently [10,89,90].
There is ample evidence suggesting that specific aspects of the moods and personalities of individuals influence their ability to tackle stress and adapt to new environments [91,92]. The present study found significant and positive relationships between an extraverted personality trait and the perceived benefits, satisfaction, and actual use of hearing aids, as reported in previous studies [58,83,93]. Extroverts gain more benefits from and satisfaction with their hearing aids over time and become more willing to use them continuously due to their active presence in social environments and their use of hearing aids in various environments [94].
Studies that focused on the role of social support in managing hearing loss revealed that older adults with hearing loss who have access to social support networks adapt to their hearing loss faster than others, and use their hearing aids more regularly [13,53,95]. The present study also found social support to be among the determinants of the actual use of hearing aids, suggesting that more support received by individuals from their families, friends, and other significant people in their lives will make them more open to the actual use and continuance intention to use their hearing aids. Several recommendations can be given concerning the role of social support in the actual use of hearing aids. Firstly, encouragement and motivation from others can be a reinforcing factor for the continued use of hearing aids. Secondly, participation in the handling and maintaining of hearing aids (repairing, changing batteries, and helping in taking, wearing, and cleaning hearing aids) by others can be another influential factor encouraging the continued use of hearing aids. Thirdly, social support in the form of emotional support can help hearing aid users adapt to their hearing aids [96].
The results of the path analysis indicated that the perceived benefits of hearing aids could predict a person’s satisfaction with their actual use of hearing aids. To interpret the predictive power of the benefits, if hearing aids act in such a way as to improve the hearing difficulties of users in various hearing conditions, their satisfaction with hearing aids will increase accordingly. High levels of satisfaction with hearing aids will eventually lead to the actual use of hearing aids. However, older adults may remain dissatisfied with their hearing aids for a number of reasons, but their perception of the beneficial performance of hearing aids can steer them toward an actual use and continuance intention to use hearing aids. This finding is confirmed by other studies, in which the perceived benefits and satisfaction in the post-fitting stage of hearing aids were two significant and determining factors in hearing aid use [46,97,98]. Contrary to the benefits that are merely associated with the performance of hearing aids, satisfaction encompasses the appearance, social, psychological, and financial aspects of receiving and using hearing aids [34,99]. The present study also revealed that satisfaction was among the factors determining the rate of the actual use of hearing aids, such that an increased level of satisfaction will increase actual hearing aid usage, which corresponds to reports indicating that satisfaction with hearing aids had a positive relationship with the number of hours of hearing aid use [54,100,101]. However, Aurelio et al. (2012) found no significant relationship between satisfaction and the number of hours of hearing aid use, but they noted that significant results would be obtained in the case of larger sample size [102].
Finally, the results of the present study suggest that the actual use of hearing aids is a strong predictor of the continuance intention to use hearing aids. This means that the successful use of hearing aids by the elderly will increase their intention to use them continuously in the future. Confirming this result, Lee et al. (2020) investigated the key factors influencing the continuance intention to use wearable healthcare devices. Their results revealed that internal factors (knowledge, attitudes, and beliefs) and external factors (technological and social factors) positively impacted actual user behavior, and the continuance intention to use wearable healthcare devices could be improved through actual use behavior [103].
6. Limitations and Further Research
Similar to other studies, the present study faced several limitations. First and foremost, the cross-sectional nature of this study makes it difficult to make conclusions about the causalities. Thus, it would be better to collect data longitudinally for a closer investigation of the perceptual factors affecting the actual and continuous use of hearing aids. Secondly, the present study used questionnaire tools for data collection, hence some participants might have refrained from giving completely truthful answers. Thirdly, our research was conducted on older adults with hearing loss in Tehran, thus the results may not be generalizable to other cities, age groups, countries, or cultures. Thus, it is recommended that similar studies are carried out in various cultural and social contexts and other age groups. Fourth, the present study did not investigate some potentially influential audiological factors mentioned in some other studies, such as the results of speech tests in the presence of noise (SIN) [104], real ear measurements [23], and people’s overall health condition. Future studies are thus recommended to examine these factors as well.
7. Conclusions
This study developed a PAM to examine the determinants of the continuous use of hearing aids among older adults in Tehran. The results of this study contribute to the existing literature by highlighting the importance of psychosocial factors in determining the continuance intention to use hearing aids among older adults. Understanding these factors can aid healthcare professionals and policymakers in developing interventions and strategies to promote the continued use of hearing aids in this population. By addressing factors such as satisfaction, self-efficacy, and social support, it may be possible to enhance the overall experience with and acceptance of hearing aids among older adults. Further research is warranted to explore additional variables that may influence continuance intentions and to validate these findings in different populations. Overall, this study provides valuable insights into improving the adoption and long-term usage of hearing aids among older adults.
Author Contributions
A.J. and Y.A.M. designed and conducted the study, analyzed the data, drafted and revised the final manuscript; A.J. and Y.A.M. reviewed the literature, collected data, and reviewed and edited the manuscript; M.F. and Y.A.M. consulted on the research and designed and reviewed the manuscript; and A.J. and S.M. performed the statistical analyses of the data and reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Ethics Committee of the Social Welfare and Rehabilitation Sciences University in Tehran, which deals with research authorizations and ethical considerations in the field of education, has approved this study (IR.USWR.REC.1399.027, on 25 February 2020). This committee follows the stipulated clauses of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Since this paper is extracted from a thesis, open access to the raw data is not permitted by the Medical University. If necessary, the authors can provide access to the data with the permission of the university.
Acknowledgments
The source of the data used in this paper was the Ph.D. thesis of Abdolhakim Jorbonyan, a student at the Department of Gerontology in the Social Welfare and Rehabilitation Sciences University. We deeply appreciate the elderly and the audiology clinics that fully cooperated on this research project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chadha, S.; Kamenov, K.; Cieza, A. The world report on hearing. Bull. World Health Organ. 2021, 99, 242. [Google Scholar] [CrossRef] [PubMed]
- Cui, Q.; Chen, N.; Wen, C.; Xi, J.; Huang, L. Research trends and hotspot analysis of age-related hearing loss from a bibliographic perspective. Front. Psychol. 2022, 13, 921117. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Yaffe, K.; Xia, J.; Xue, Q.-L.; Harris, T.B.; Purchase-Helzner, E.; Satterfield, S.; Ayonayon, H.N.; Ferrucci, L.; Simonsick, E.M. Hearing loss and cognitive decline in older adults. JAMA Intern. Med. 2013, 173, 293–299. [Google Scholar] [CrossRef]
- Patel, R.; McKinnon, B.J. Hearing loss in the elderly. Clin. Geriatr. Med. 2018, 34, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.L.; Hyer, K.; Small, B.J.; Chisolm, T.; Saunders, G.H.; McEvoy, C.L.; Lee, D.J.; Dhar, S.; Bainbridge, K.E. Hearing aid prevalence and factors related to use among older adults from the Hispanic community health study/study of Latinos. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Kochkin, S. MarkeTrak VIII: 25-year trends in the hearing health market. Hear. Rev. 2009, 16, 12–31. [Google Scholar]
- McCormack, A.; Fortnum, H. Why do people fitted with hearing aids not wear them? Int. J. Audiol. 2013, 52, 360–368. [Google Scholar] [CrossRef]
- Moon, I.J.; Baek, S.Y.; Cho, Y.-S. Hearing aid use and associated factors in South Korea. Medicine 2015, 94, e1580. [Google Scholar] [CrossRef]
- Hougaard, S.; Ruf, S.; Egger, C. EuroTrak+ JapanTrak 2012: Societal and personal benefits of hearing rehabilitation with hearing aids. Hear. Rev. 2013, 20, 16–26. [Google Scholar]
- Sawyer, C.S.; Armitage, C.J.; Munro, K.J.; Singh, G.; Dawes, P.D. Biopsychosocial Classification of Hearing Health Seeking in Adults Aged Over 50 Years in England. Ear Hear. 2020, 41, 1215–1225. [Google Scholar] [CrossRef]
- Jorbonyan, A.; Momtaz, Y.A.; Foroghan, M.; Mehrkian, S. Factors Affecting the Adoption and Use of Hearing Aids among Older Adults: A Systematic Review. Curr. Psychiatry Res. Rev. Former. 2021, 17, 172–187. [Google Scholar] [CrossRef]
- Vestergaard Knudsen, L.; Öberg, M.; Nielsen, C.; Naylor, G.; Kramer, S.E. Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: A review of the literature. Trends Amplif. 2010, 14, 127–154. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.H.-Y.; Loke, A.Y. Determinants of hearing-aid adoption and use among the elderly: A systematic review. Int. J. Audiol. 2015, 54, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Saunders, G.H.; Chisolm, T.H.; Wallhagen, M.I. Older adults and hearing help-seeking behaviors. Am. J. Audiol. 2012, 21, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Saunders, G.H.; Frederick, M.T.; Silverman, S.C.; Nielsen, C.; Laplante-Lévesque, A. Health behavior theories as predictors of hearing-aid uptake and outcomes. Int. J. Audiol. 2016, 55, S59–S68. [Google Scholar] [CrossRef] [PubMed]
- Saunders, G.H.; Frederick, M.T.; Silverman, S.; Papesh, M. Application of the health belief model: Development of the hearing beliefs questionnaire (HBQ) and its associations with hearing health behaviors. Int. J. Audiol. 2013, 52, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Meister, H.; Grugel, L.; Meis, M. Intention to use hearing aids: A survey based on the theory of planned behavior. Patient Prefer. Adherence 2014, 8, 1265–1275. [Google Scholar] [CrossRef][Green Version]
- Cobelli, N.; Gill, L.; Cassia, F.; Ugolini, M. Factors that influence intent to adopt a hearing aid among older people in Italy. Health Soc. Care Community 2014, 22, 612–622. [Google Scholar] [CrossRef]
- DeSanctis, G.; Poole, M.S. Capturing the complexity in advanced technology use: Adaptive structuration theory. Organ. Sci. 1994, 5, 121–147. [Google Scholar] [CrossRef]
- Khaksar, S.M.S.; Khosla, R.; Singaraju, S.; Slade, B. Carer’s perception on social assistive technology acceptance and adoption: Moderating effects of perceived risks. Behav. Inf. Technol. 2021, 40, 337–360. [Google Scholar] [CrossRef]
- Taherdoost, H. A review of technology acceptance and adoption models and theories. Procedia Manuf. 2018, 22, 960–967. [Google Scholar] [CrossRef]
- Laplante-Lévesque, A.; Hickson, L.; Worrall, L. Stages of change in adults with acquired hearing impairment seeking help for the first time: Application of the transtheoretical model in audiologic rehabilitation. Ear Hear. 2013, 34, 447–457. [Google Scholar] [CrossRef] [PubMed]
- Hickson, L.; Meyer, C.; Lovelock, K.; Lampert, M.; Khan, A. Factors associated with success with hearing aids in older adults. Int. J. Audiol. 2014, 53, S18–S27. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Hickson, L.; Lovelock, K.; Lampert, M.; Khan, A. An investigation of factors that influence help-seeking for hearing impairment in older adults. Int. J. Audiol. 2014, 53, S3–S17. [Google Scholar] [CrossRef] [PubMed]
- Duijvestijn, J.; Anteunis, L.J.; Hoek, C.; Van Den Brink, R.H.; Chenault, M.N.; Manni, J.J. Help-seeking behaviour of hearing-impaired persons aged ≥55 years; effect of complaints, significant others and hearing aid image. Acta Oto-Laryngol. 2003, 123, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Bhattacherjee, A. Understanding information systems continuance: An expectation-confirmation model. MIS Q. 2001, 25, 351–370. [Google Scholar] [CrossRef]
- Bøe, T.; Gulbrandsen, B.; Sørebø, Ø. How to stimulate the continued use of ICT in higher education: Integrating information systems continuance theory and agency theory. Comput. Hum. Behav. 2015, 50, 375–384. [Google Scholar] [CrossRef]
- Lin, C.S.; Wu, S.; Tsai, R.J. Integrating perceived playfulness into expectation-confirmation model for web portal context. Inf. Manag. 2005, 42, 683–693. [Google Scholar] [CrossRef]
- Oliver, R.L. A cognitive model of the antecedents and consequences of satisfaction decisions. J. Mark. Res. 1980, 17, 460–469. [Google Scholar] [CrossRef]
- Lankton, N.; McKnight, D.H. Using Expectation Disconfirmation Theory to Predict Technology Trust and Usage Continuance Intentions; Eli Broad College of Business: East Lansing, MI, USA, 2006. [Google Scholar]
- Schwarz, C. Understanding the Role of Expectation Disconfirmation Theory on IT Outsourcing Success. Ph.D. Thesis, Louisiana State University, Baton Rouge, LA, USA, 2011. [Google Scholar]
- Venkatesh, V.; Goyal, S. Expectation disconfirmation and technology adoption: Polynomial modeling and response surface analysis. MIS Q. 2010, 34, 281–303. [Google Scholar] [CrossRef]
- Liao, C.; Palvia, P.; Chen, J.-L. Information technology adoption behavior life cycle: Toward a Technology Continuance Theory (TCT). Int. J. Inf. Manag. 2009, 29, 309–320. [Google Scholar] [CrossRef]
- Wong, L.L.; Hickson, L.; McPherson, B. Satisfaction with hearing aids: A consumer research perspective. Int. J. Audiol. 2009, 48, 405–427. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Hickson, L.; Khan, A.; Walker, D. What is important for hearing aid satisfaction? Application of the expectancy-disconfirmation model. J. Am. Acad. Audiol. 2014, 25, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- You, J.-J.; Jong, D.; Wiangin, U. Consumers’ Purchase Intention of Organic Food via Social Media: The Perspectives of Task-Technology Fit and Post-acceptance Model. Front. Psychol. 2020, 11, 579274. [Google Scholar] [CrossRef] [PubMed]
- Thong, J.Y.; Hong, S.-J.; Tam, K.Y. The effects of post-adoption beliefs on the expectation-confirmation model for information technology continuance. Int. J. Hum. Comput. Stud. 2006, 64, 799–810. [Google Scholar] [CrossRef]
- Hsiao, C.-H. The effects of post-adoption beliefs on the expectation–confirmation model in an electronics retail setting. Total Qual. Manag. Bus. Excell. 2018, 29, 866–880. [Google Scholar] [CrossRef]
- Cho, J.; Lee, H.E. Post-adoption beliefs and continuance intention of smart device use among people with physical disabilities. Disabil. Health J. 2020, 13, 100878. [Google Scholar] [CrossRef]
- Cho, J. The impact of post-adoption beliefs on the continued use of health apps. Int. J. Med. Inform. 2016, 87, 75–83. [Google Scholar] [CrossRef]
- Gao, S.; Zhang, X.; Peng, S. Understanding the adoption of smart wearable devices to assist healthcare in China. In Proceedings of the Conference on e-Business, e-Services and e-Society, Swansea, UK, 13–15 September 2016; pp. 280–291. [Google Scholar]
- Oliver, R.L. Satisfaction: A Behavioral Perspective on the Consumer; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Cox, R.M.; Alexander, G.C. Expectations about hearing aids and their relationship to fitting outcome. J. Am. Acad. Audiol. 2000, 11, 368–382. [Google Scholar] [CrossRef]
- Saunders, G.H.; Lewis, M.S.; Forsline, A. Expectations, prefitting counseling, and hearing aid outcome. J. Am. Acad. Audiol. 2009, 20, 320–334. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, M.A.; Woolley, A.; Munro, K.J. The impact of self-efficacy, expectations, and readiness on hearing aid outcomes. Int. J. Audiol. 2016, 55, S34–S41. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef]
- Kim, J.; Park, H.-A. Development of a health information technology acceptance model using consumers’ health behavior intention. J. Med. Internet Res. 2012, 14, e133. [Google Scholar] [CrossRef] [PubMed]
- Kochkin, S. On the Issue of Value: Hearing Aid Benefit. Price Satisf. Brand Repurchase Rates Hear. Rev. 2003, 7, 6–34. [Google Scholar]
- Purdy, S.C.; Jerram, C.K. Investigation of the profile of hearing aid performance in experienced hearing aid users. Ear Hear. 1998, 19, 473–480. [Google Scholar] [CrossRef]
- Aazh, H.; Prasher, D.; Nanchahal, K.; Moore, B.C. Hearing-aid use and its determinants in the UK National Health Service: A cross-sectional study at the Royal Surrey County Hospital. Int. J. Audiol. 2015, 54, 152–161. [Google Scholar] [CrossRef]
- Singh, G.; Lau, S.-T.; Pichora-Fuller, M.K. Social support predicts hearing aid satisfaction. Ear Hear. 2015, 36, 664–676. [Google Scholar] [CrossRef]
- Korkmaz, M.H.; Bayır, Ö.; Er, S.; Işık, E.; Saylam, G.; Tatar, E.Ç.; Özdek, A. Satisfaction and compliance of adult patients using hearing aid and evaluation of factors affecting them. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3723–3732. [Google Scholar] [CrossRef]
- Meyer, C.; Hickson, L.; Fletcher, A. Identifying the barriers and facilitators to optimal hearing aid self-efficacy. Int. J. Audiol. 2014, 53, S28–S37. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.K.; McCarthy, P. The relationship between personality type and perceived hearing aid benefit. Hear. J. 2001, 54, 41–44. [Google Scholar] [CrossRef]
- Cox, R.M.; Alexander, G.C.; Gray, G.A. Who wants a hearing aid? Personality profiles of hearing aid seekers. Ear Hear. 2005, 26, 12–26. [Google Scholar] [CrossRef]
- Dwarakanath, V.M.; Manjula, P. Influence of Personality and Attitude towards Loss of Hearing on Hearing Aid Outcome in Older Adults with Hearing Loss. Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Launer, S. Social context and hearing aid adoption. Trends Hear. 2016, 20, 2331216516673833. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Impairments, Disabilities, and Handicaps: A Manual of Classification Relating to the Consequences of Disease, Published in Accordance with Resolution WHA29. 35 of the Twenty-Ninth World Health Assembly, May 1976; World Health Organization: Geneva, Switzerland, 1980. [Google Scholar]
- Angara, P.; Tsang, D.C.; Hoffer, M.E.; Snapp, H.A. Self-Perceived Hearing Status Creates an Unrealized Barrier to Hearing Healthcare Utilization. Laryngoscope 2021, 131, E289–E295. [Google Scholar] [CrossRef] [PubMed]
- Maeda, Y.; Sugaya, A.; Nagayasu, R.; Nakagawa, A.; Nishizaki, K. Subjective hearing-related quality-of-life is a major factor in the decision to continue using hearing aids among older persons. Acta Oto-Laryngol. 2016, 136, 919–922. [Google Scholar] [CrossRef]
- Sadeghi, R.; Zanjari, N. The inequality of development in the 22 districts of Tehran metropolis. Soc. Welf. Q. 2017, 17, 149–184. [Google Scholar]
- West, R.L.; Smith, S.L. Development of a hearing aid self-efficacy questionnaire. Int. J. Audiol. 2007, 46, 759–771. [Google Scholar] [CrossRef]
- FarajiKhiavi, F.; Bayat, A.; Dashti, R.; Sameni, S.J. Hearing aid-related satisfaction based on type and degree of hearing loss in elderly. Bimon. Audiol. Tehran Univ. Med. Sci. 2015, 23, 114–122. [Google Scholar]
- Madani, R. Standard Translation APHAB Questionnaire and Evaluation of Benefit in People with Mild to Severe Hearing Loss; Iran University of Medical Sceinces: Tehran, Iran, 2008. (In Persian) [Google Scholar]
- Moossavi, A.; Jalilzade, A.P.; Lotfian, E.; Bakhshi, E. Translating and Assessing the Validity and Reliability of Persian Version of the International Outcome Inventory for Hearing Aids (IOI-HA). J. Rehabil. Sci. Res. 2018, 5, 36–40. [Google Scholar]
- Heidari, F.; Ghahraman, M.A.; Tavanai, E.; Jalaie, S.; Abdollahi, F.Z. Self-assessed hearing handicap in the elderly: A pilot study on Iranian population. Audit. Vestib. Res. 2021, 30, 33–41. [Google Scholar] [CrossRef]
- Bagherian-Sararoudi, R.; Hajian, A.; Ehsan, H.B.; Sarafraz, M.R.; Zimet, G.D. Psychometric properties of the Persian version of the multidimensional scale of perceived social support in Iran. Int. J. Prev. Med. 2013, 4, 1277–1281. [Google Scholar] [PubMed]
- Azkhosh, M.; Sahaf, R.; Rostami, M.; Ahmadi, A. Reliability and Validity of the 10-Item Personality Inventory among Older Iranians. Psychol. Russ. 2019, 12, 28. [Google Scholar] [CrossRef]
- Hartley, D.; Rochtchina, E.; Newall, P.; Golding, M.; Mitchell, P. Use of hearing aids and assistive listening devices in an older Australian population. J. Am. Acad. Audiol. 2010, 21, 642–653. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, L.; Novak, M. Factors influencing hearing aid adoption. Semin. Hear. 2020, 41, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Bulğurcu, S.; Uçak, I.; Yönem, A.; Erkul, E.; Çekin, E. Hearing Aid Problems in Elderly Populations. Ear Nose Throat J. 2020, 99, 323–326. [Google Scholar] [CrossRef]
- Klyn, N.A.M.; Shaikh, Z.M.; Dhar, S. Health literacy and self-reported hearing aid use in the Health and Retirement Study. Ear Hear. 2020, 41, 386–394. [Google Scholar] [CrossRef]
- Ji-Su, K. Prevalence and factors associated with hearing loss and hearing aid use in korean elders. Iran. J. Public Health 2015, 44, 308–317. [Google Scholar]
- Helvik, A.-S.; Krokstad, S.; Tambs, K. How sociodemographic and hearing related factors were associated with use of hearing aid in a population-based study: The HUNT Study. BMC Ear Nose Throat Disord. 2016, 16, 8. [Google Scholar] [CrossRef]
- Perez, E.; Edmonds, B.A. A systematic review of studies measuring and reporting hearing aid usage in older adults since 1999: A descriptive summary of measurement tools. PLoS ONE 2012, 7, e31831. [Google Scholar] [CrossRef] [PubMed]
- Tahden, M.A.; Gieseler, A.; Meis, M.; Wagener, K.C.; Colonius, H. What Keeps Older Adults With Hearing Impairment From Adopting Hearing Aids? Trends Hear. 2018, 22, 2331216518809737. [Google Scholar] [CrossRef] [PubMed]
- Bertoli, S.; Staehelin, K.; Zemp, E.; Schindler, C.; Bodmer, D.; Probst, R. Survey on hearing aid use and satisfaction in Switzerland and their determinants. Int. J. Audiol. 2009, 48, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Bertoli, S.; Bodmer, D.; Probst, R. Survey on hearing aid outcome in Switzerland: Associations with type of fitting (bilateral/unilateral), level of hearing aid signal processing, and hearing loss. Int. J. Audiol. 2010, 49, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Yueh, B.; Souza, P.E.; McDowell, J.A.; Collins, M.P.; Loovis, C.F.; Hedrick, S.C.; Ramsey, S.D.; Deyo, R.A. Randomized trial of amplification strategies. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Solheim, J.; Gay, C.; Hickson, L. Older adults’ experiences and issues with hearing aids in the first six months after hearing aid fitting. Int. J. Audiol. 2018, 57, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.M.; Alexander, G.C.; Gray, G.A. Personality, hearing problems, and amplification characteristics: Contributions to self-report hearing aid outcomes. Ear Hear. 2007, 28, 141–162. [Google Scholar] [CrossRef]
- Gatehouse, S. Components and determinants of hearing aid benefit. Ear Hear. 1994, 15, 30–49. [Google Scholar] [CrossRef]
- Fuentes-López, E.; Fuente, A.; Valdivia, G.; Luna-Monsalve, M. Does educational level predict hearing aid self-efficacy in experienced older adult hearing aid users from Latin America? Validation process of the Spanish version of the MARS-HA questionnaire. PLoS ONE 2019, 14, e0226085. [Google Scholar] [CrossRef]
- Kelly-Campbell, R.J.; McMillan, A. The relationship between hearing aid self-efficacy and hearing aid satisfaction. Am. J. Audiol. 2015, 24, 529–535. [Google Scholar] [CrossRef]
- Johnson, C.E.; Jilla, A.M.; Danhauer, J.L.; Sullivan, J.C.; Sanchez, K.R. Benefits from, satisfaction with, and self-efficacy for advanced digital hearing aids in users with mild sensorineural hearing loss. Semin. Hear. 2018, 39, 158–171. [Google Scholar]
- Mizutari, K.; Michikawa, T.; Saito, H.; Okamoto, Y.; Enomoto, C.; Takebayashi, T.; Ogawa, K.; Nishiwaki, Y. Age-related hearing loss and the factors determining continued usage of hearing aids among elderly community-dwelling residents. PLoS ONE 2013, 8, e73622. [Google Scholar] [CrossRef]
- Hallberg, L.R.-M.; Hallberg, U.; Kramer, S.E. Self-reported hearing difficulties, communication strategies and psychological general well-being (quality of life) in patients with acquired hearing impairment. Disabil. Rehabil. 2008, 30, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Kamil, R.J.; Genther, D.J.; Lin, F.R. Factors associated with the accuracy of subjective assessments of hearing impairment. Ear Hear. 2015, 36, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Amirkhan, J.H.; Risinger, R.T.; Swickert, R.J. Extraversion: A “hidden” personality factor in coping? J. Personal. 1995, 63, 189–212. [Google Scholar] [CrossRef] [PubMed]
- Vollrath, M.; Torgersen, S. Personality types and coping. Personal. Individ. Differ. 2000, 29, 367–378. [Google Scholar] [CrossRef]
- Alexander, G.C.; Gray, G. Personality and the subjective assessment of hearing aids. J. Am. Acad. Audiol. 1999, 10, 1–13. [Google Scholar]
- Berens, E.-M.; Ganahl, K.; Vogt, D.; Schaeffer, D. Health literacy among elderly immigrants in Germany. Findings from a cross-sectional survey. Eur. J. Public Health 2018, 28, 191–192. [Google Scholar] [CrossRef]
- Moser, S.; Luxenberger, W.; Freidl, W. The influence of social support and coping on quality of life among elderly with age-related hearing loss. Am. J. Audiol. 2017, 26, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Pichora-Fuller, M.K. The benefits of social support for listeners with impaired hearing. Hear. J. 2016, 69, 34–36. [Google Scholar] [CrossRef]
- Saunders, G.H.; Jutai, J.W. Hearing specific and generic measures of the psychosocial impact of hearing aids. J. Am. Acad. Audiol. 2004, 15, 238–248. [Google Scholar] [CrossRef]
- Hamidi Pouyandeh, M.; Hoseinabadi, R. Factors Influencing the Hearing Aids Use and Satisfaction: A Review Study. J. Mod. Rehabil. 2019, 13, 137–146. [Google Scholar] [CrossRef]
- Laperuta, E.B.; Fiorini, A.C. Satisfaction of elderly individuals with hearing aids in the first six months of use. J. Soc. Bras. Fonoaudiol. 2012, 24, 316–321. [Google Scholar] [CrossRef]
- Kaplan-Neeman, R.; Muchnik, C.; Hildesheimer, M.; Henkin, Y. Hearing aid satisfaction and use in the advanced digital era. Laryngoscope 2012, 122, 2029–2036. [Google Scholar] [CrossRef]
- Laplante-Lévesque, A.; Knudsen, L.V.; Preminger, J.E.; Jones, L.; Nielsen, C.; Öberg, M.; Lunner, T.; Hickson, L.; Naylor, G.; Kramer, S.E. Hearing help-seeking and rehabilitation: Perspectives of adults with hearing impairment. Int. J. Audiol. 2012, 51, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Aurélio, F.S.; Silva, S.P.d.; Rodrigues, L.B.; Kuniyoshi, I.C.; Botelho, M.S. Satisfaction of patients fit with a hearing aid in a high complexity clinic. Braz. J. Otorhinolaryngol. 2012, 78, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Lee, D. Healthcare wearable devices: An analysis of key factors for continuous use intention. Serv. Bus. 2020, 14, 503–531. [Google Scholar] [CrossRef]
- Davidson, A.; Marrone, N.; Wong, B.; Musiek, F. Predicting Hearing Aid Satisfaction in Adults: A Systematic Review of Speech-in-noise Tests and Other Behavioral Measures. Ear Hear. 2021, 42, 1485–1498. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).