

‘Misdiagnosed and Misunderstood’: Insights into Rarer Forms of Dementia through a Stepwise Approach to Co-Constructed Research Poetry

 ,
, 
 , , , ,
, , , ,
Abstract
1. Introduction
Research Aims
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
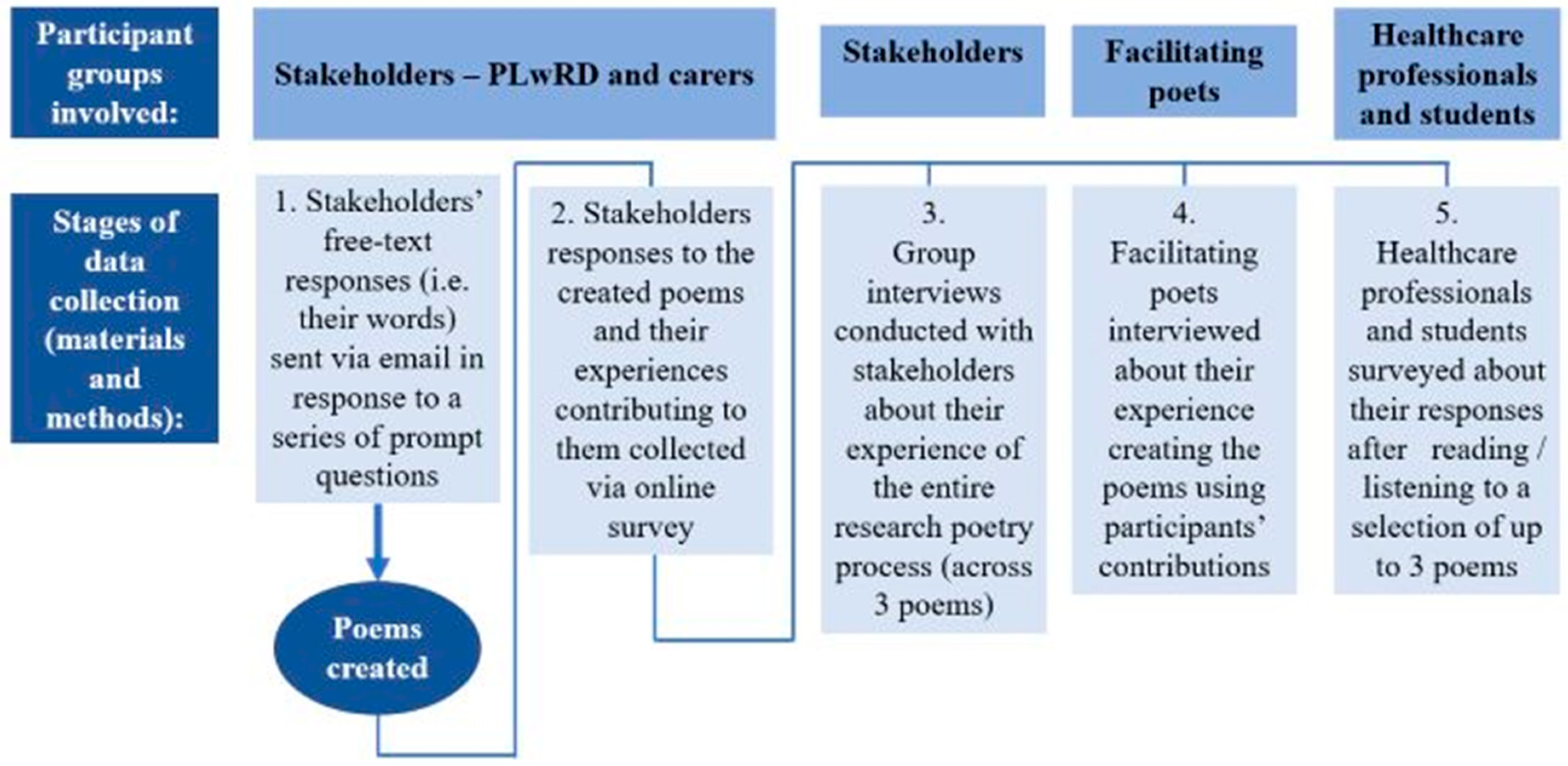
2.3. Data Collection
- What is your experience of having (type of dementia) or being a family member caring for someone with this type of dementia?
- How would you describe (type of dementia) to a friend or family member?
- What does support mean to you?
2.4. Data Analysis
3. Results
3.1. The Poems
3.1.1. Prompt 1 (for Poems 1–9, Supplemental Figure S2): What Is Your Experience of Having (Type of Dementia) or Being a Family Member Caring for Someone with This Type of Dementia?
3.1.2. Prompt 2 (for Poems 10–18, Supplemental Figure S2): How Would You Describe (Type of Dementia) to a Friend or Family Member?
3.1.3. Prompt 3 (for Poems 19–27, Supplemental Figure S2): What Does Support Mean to You?
3.1.4. Poems: Narrative Synthesis
3.2. Stakeholder Survey Findings
3.2.1. People Living with Rarer Forms of Dementia: Writing
“Initially, it was hard to get down on paper the points that I wanted to bring forward as there are so many aspects around living with my dementia. I did not want to overload my reply with too many aspects and responses. I was happy with my final response in the knowledge that others may express the aspects of living with the condition that I didn’t cover”(11.12.FTD.PLwRD-1).
“Initially, I needed to establish in my mind what I wanted to portray in a clear, concise way. Having hit on the idea that so often in my mind I feel jumbled and mixed up, I was then able to use the mental picture of a Tumble Drier/Washing machine as a simile for me to clearly portray how living with dementia often feels to me. I was pleased with the result”(11.12.FTD.PLwRD-2).
3.2.2. Care-Partners: Writing
3.2.3. Writing Poems: Narrative Synthesis
3.3. People Living with Rarer Forms of Dementia: Responding to Poems
3.3.1. Care-Partners: Responding to Poems
3.3.2. Responding to the Poems: Narrative Synthesis
3.4. Stakeholder Group Interviews
3.4.1. Lived Experience and Reflection
“Hearing these words spoken because just inside one’s head is almost not enough [...] It just expands the experience if you hear it. And if you hear it in someone else’s voice [...] because of his inflexions on certain things, and his understanding, and appreciation of those words, it just opened up another voice for me, and I found that—I’m getting goosebumps actually just thinking how that was revelatory to me.”(bvFTD.C-England).
“There was nobody that I could connect with there […] there was no local doctor, even our local Alzheimer’s group, there was no one at all that was even closely in my situation. And when I thought about the idea that other people were pondering this same question at the same time […] I thought, well, I’m not alone. I’m still in a little vacuum. I’m still in my little corner of the world, but somebody else is thinking the same painful thought or […] pondering the same issue that I’m pondering and so I think that was very important for me.”(YOAD. C-Canada).
“I think it’s fun. I think it’s amusing. It is a lot of fun for me to see how the words were put together. My thoughts and other people’s thoughts. And I see a lot of similarity of course of emotions, flowing throughout the poems.”(PPA.PLwRD-Singapore)
“And somehow, the rest of the words put meaning to what you said. [...] It expresses my feelings for me, if you like. I probably couldn’t put it into words. I mean, I can express lots of feelings, but those particular feelings, I couldn’t put- I don’t think, I don’t try, I haven’t tried.”(PCA.C-England)
3.4.2. Curiosity and Exploration
“Yes, I thought this was a really unusual opportunity and it was really refreshing [...] I thought poetry was a surprising choice [...] it’s the first time I’d been asked to do anything like this and I thought it’s innovative really, and unusual, so I was curious as well.”(PCA.C-England)
“It actually felt good to have participated in something and the process of doing it [...] for me was [...] very creative because it called on emotion, not on cognitive processing and I spend my life in a in different world, and so it was really a stretch to just respond from emotion.”(FTD.C-Canada)
3.4.3. Barriers and Inclusivity
“Just having the opportunity [...] to reflect on how you’re feeling because, my husband and I are both lawyers and we’re very analytical, and so feelings [...] for us or that’s not something that [...] we’re allowed.”(FTD.C-Canada)
“We have, generally, certainly, in this country, we have a really poor experience of poetry. Perhaps it’s not taught properly at school [...] I don’t know how it materialises, but people run away from it and miss, in my opinion, so much beauty.”(bvFTD.C-England).
“…perhaps highlighting individual poems at different times might be an option. Because it’s quite a lot all together, and that’s one of the reasons why I think it’s been more difficult to share with people, with friends and family, because it’s a whole volume.”(PCA.C-England).
3.4.4. Sharing the Poems
“I think of educating people [...] it seems like I would be more willing to [...] take the book, say to my husband’s physician office than I would be to give it to one of the people closest to me.”(FTD.C-Canada)
“Yes, I’ve actually not shared it very widely at all. I shared the book with a friend who is a nurse practitioner actually. I’ve been very careful about who I’ve shared it with, because it’s been an emotional journey really. And I think it’s a lot for people who don’t have experience of any sort of dementia.”(PCA.C-England)
3.4.5. Group Interviews: Narrative Synthesis
3.5. Healthcare Professionals and Student Survey
3.5.1. Other-Oriented Perspective Taking
“In this poem I felt a mixture of emotions. At the start, I felt so deeply sad about the impact dementia can have on every part of life. In response to the line, ‘a slow and painful death I encounter each day’, I thought about how cruel dementia is as a disease, in which people feel themselves slowly dying and how relentless this may be. Towards the end of the poem, I felt lighter in myself whilst reading the verse ‘My husband is my best friend and soulmate. I am a lucky woman to have him in my life. He treated me like a queen for over 30 years and he is still my knight in shining armour.’ It highlighted the person, instead of just the diagnosis and I smiled at the love that was so evident in this part of the poem. I was left really thinking about the instruction to ‘Live each day as that is the only guarantee you have’ and to take life as it comes, not worry about the trivial and enjoy as much as I can.”
3.5.2. Insight through Critical Reflection
“I think this poem reminded me to be patient when working with care recipients. There are numerous reasons why a person cannot articulate themselves well. It may or may not have to do with the dementia, but there is power in listening. Allowing the client the floor. Shows a person-centred approach to care and that your time is not more important than their experience.”
“Always being mindful of sensory overload, personalized care focusing on the patient’s strengths and abilities. They are trying so hard not to be angry with themselves we MUST try too. Unfortunately, I have seen too many ‘professional’ caregivers become angry or frustrated with their patient’s/client’s limitations, this is unsupportive, uncalled for and disheartening. An example of what never to do.”
“Overall, the poem reminds me of a concept called ‘medical waiting’ that I learned of in an article by Mary Hunter called ‘The Waiting Time of Prostitution: Gynaecology and Temporality in Henri de Toulouse-Lautrec’s Rue des Moulins, 1894. Medical waiting is about the anxiety one experiences while waiting for results of medical testing, and the fears surrounding the way the body will be policed or regulated by institutions after the diagnosis is delivered. To me, it seems that the impact of institutions—with their treatment protocols and the way they regulate, limit, and treat patients (both medically and interpersonally)—on the bodies, minds, and overall wellness of those being diagnosed…”
3.5.3. Value of Support
“As with the other poems, when caring and support dementia patients, compassion and patience is key. They are not themselves, their behaviours if they have any are not who they are but a product of their disease progression and deserve compassion, love and patience.”
3.5.4. Acceptability of Poetry as a Learning Tool
“Articles from academic journals can be so stale—clinically reporting the experiences of others and it has us looking down at them and their struggles. However, qualitative/artistic/narrative can actually have us be with the person, their experience and their struggles—have us empathise to the point of us being in their own shoes, and better understand how we can interact with them as professionals in a way that’s more humane.”(healthcare professional)
“…if it is integrated into the curriculum/supervision in ways that highlight specific issues and experiences (e.g., isolation, fear of the future, not knowing what’s next, dementia activism, different symptoms and problems). I wouldn’t just bring in poems and read them without a context though. It would be important to use them (as visual art is now used in some medical school training) to help support whatever teaching or supervision is occurring---otherwise eyes will roll and only a few interested trainees will take it on. Have the class create poems together, that’s where I might begin.”(healthcare professional)
3.5.5. Using Poetry as a Learning Tool
4. Discussion
4.1. Cross Synthesis and Interpretation
4.2. Limitations and Strengths
4.3. Future Research and Practice Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hendriks, S.; Peetoom, K.; Bakker, C.; van der Flier, W.M.; Papma, J.M.; Koopmans, R.; Verhey, F.R.J.; de Vugt, M.; Köhler, S.; Withall, A.; et al. Global Prevalence of Young-Onset Dementia: A Systematic Review and Meta-Analysis. JAMA Neurol. 2021, 78, 1080–1090. [Google Scholar] [CrossRef]
- Hendriks, S.; Peetoom, K.; Bakker, C.; Koopmans, R.; van der Flier, W.; Papma, J.; Verhey, F.; de Vugt, M.; Köhler, S.; Young-Onset Dementia Epidemiology Study Group. Global incidence of young-onset dementia: A systematic review and meta-analysis. Alzheimer’s Dement. 2023, 19, 831–843. [Google Scholar] [CrossRef]
- Jitlal, M.; Amirthalingam, G.N.K.; Karania, T.; Parry, E.; Neligan, A.; Dobson, R.; Noyce, A.J.; Marshall, C.R. The Influence of Socioeconomic Deprivation on Dementia Mortality, Age at Death, and Quality of Diagnosis: A Nationwide Death Records Study in England and Wales 2001–2017. J. Alzheimer’s Dis. 2021, 81, 321–328. [Google Scholar] [CrossRef]
- Millenaar, J.K.; Bakker, C.; Koopmans, R.T.C.M.; Verhey, F.R.J.; Kurz, A.; de Vugt, M.E. The Care Needs and Experiences with the Use of Services of People with Young-Onset Dementia and their Caregivers: A Systematic Review. Int. J. Geriatr. Psychiatry 2016, 31, 1261–1276. [Google Scholar] [CrossRef]
- Rossor, M.N.; Fox, N.C.; Mummery, C.J.; Schott, J.M.; Warren, J.D. The Diagnosis of Young-Onset Dementia. Lancet Neurol. 2010, 9, 793–806. [Google Scholar] [CrossRef]
- Hanauer, D. The Genre-Specific Hypothesis of Reading: Reading Poetry and Encyclopedic Items. Poetics 1998, 26, 63–80. [Google Scholar] [CrossRef]
- Camic, P.M.; Harding, E.; Sullivan, M.P.; Grillo, A.; McKee-Jackson, R.; Wilson, L.; Zimmermann, N.; Brotherhood, E.V.; Crutch, S.J. Developing Poetry as a Research Methodology with Rarer Forms of Dementia: Four Research Protocols. Int. J. Qual. Methods 2022, 21, 16094069221081377. [Google Scholar] [CrossRef]
- Faulkner, S.L. Poetry as Method: Reporting Research through Verse, 2nd ed.; Routledge: London, UK, 2016; ISBN 978-1-59874-401-9. [Google Scholar]
- Zeilig, H. Dementia as a Cultural Metaphor. Gerontologist 2014, 54, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, S.L. Research/poetry: Exploring Poets’ Conceptualizations of Craft, Practice, and Good and Effective Poetry. Educ. Insights 2009, 13, 3. [Google Scholar]
- McCulliss, D. Poetic Inquiry and Multidisciplinary Qualitative Research. J. Poet. Ther. 2013, 26, 83–114. [Google Scholar] [CrossRef]
- Killick, J. Poetry and Dementia; Jessica Kingsley: Philadelphia, PA, USA, 2018; ISBN 9781785921766. [Google Scholar]
- Aadlandsvik, R. The Second Sight: Learning about and with Dementia by Means of Poetry. Dementia 2008, 7, 321–339. [Google Scholar] [CrossRef]
- Swinnen, A.; de Medeiros, K. “Play” and People Living with Dementia: A Humanities-based Inquiry of TimeSlips and the Alzheimer’s Poetry Project. Gerontologist 2018, 58, 261–269. [Google Scholar] [CrossRef]
- Camic, P.M.; Crutch, S.J.; Murphy, C.; Firth, N.C.; Harding, E.; Harrison, C.R.; Howard, S.; Strohmaier, S.; Van Leewen, J.; West, J.; et al. Conceptualising and Understanding Artistic Creativity in the Dementias: Interdisciplinary Approaches to Research and Practise. Front. Psychol. 2018, 9, 1842. [Google Scholar] [CrossRef]
- Gregory, H. Using Poetry to Improve the Quality of Life and Care for People with Dementia: A Qualitative Analysis of the Try to Remember Programme. Arts Health 2011, 3, 160–172. [Google Scholar] [CrossRef]
- Kidd, L.L.; Zauszniewski, J.A.; Morris, D.L. Benefits of a Poetry Writing Intervention for Family Caregivers of Elders with Dementia. Issues Ment. Health Nurs. 2011, 32, 598–604. [Google Scholar] [CrossRef]
- Clark-McGhee, K.; Castro, M. A Narrative Analysis of Poetry Written from the Words of People Given a Diagnosis of Dementia. Dementia 2015, 14, 9–26. [Google Scholar] [CrossRef] [PubMed]
- Hurren, W. The Convenient Portability of Words. In Poetic Inquiry: Vibrant Voices in the Social Sciences; Prendergast, M., Leggo, C., Sameshima, P., Eds.; Sense Publishers: Rotterdam, The Netherlands, 2009; pp. 229–238. ISBN 978-90-8790-949-9. [Google Scholar]
- Graham, N.L. Dysgraphia in Dementia. Neurocase 2000, 6, 365–376. [Google Scholar] [CrossRef]
- Gerber, K.; Brijnath, B.; Lock, K.; Bryant, C.; Hills, D.; Hjorth, L. ‘Unprepared for the Depth of My Feelings’—Capturing Grief in Older People through Research Poetry. Age Ageing 2022, 51, afac030. [Google Scholar] [CrossRef]
- Ratan, S.K.; Anand, T.; Ratan, J. Formulation of Research Question—Stepwise Approach. J. Indian Assoc. Pediatr. Surg. 2019, 24, 15–20. [Google Scholar] [CrossRef]
- Ryman, D.C.; Acosta-Baena, N.; Aisen, P.S.; Bird, T.; Danek, A.; Fox, N.C.; Goate, A.; Frommelt, P.; Ghetti, B.; Langbaum, J.B.; et al. Symptom Onset in Autosomal Dominant Alzheimer Disease: A Systematic Review and Meta-Analysis. Neurology 2014, 83, 253–260. [Google Scholar] [CrossRef]
- Sivasathiaseelan, H.; Marshall, C.R.; Agustus, J.L.; Benhamou, E.; Bond, R.L.; van Leeuwen, J.E.P.; Hardy, C.J.D.; Rohrer, J.D.; Warren, J.D. Frontotemporal Dementia: A Clinical Review. Semin. Neurol. 2019, 39, 251–263. [Google Scholar] [CrossRef]
- Marshall, C.R.; Hardy, C.J.D.; Volkmer, A.; Russell, L.L.; Bond, R.L.; Fletcher, P.D.; Clark, C.N.; Mummery, C.J.; Schott, J.M.; Rossor, M.N.; et al. Primary Progressive Aphasia: A Clinical Approach. J. Neurol. 2018, 265, 1474–1490. [Google Scholar] [CrossRef]
- Crutch, S.J.; Schott, J.M.; Rabinovici, G.D.; Murray, M.; Snowden, J.S.; van der Flier, W.M.; Dickerson, B.C.; Vandenberghe, R.; Ahmed, S.; Bak, T.H.; et al. Consensus Classification of Posterior Cortical Atrophy. Alzheimer’s Dement. 2017, 13, 870–884. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I. Dementia with Lewy Bodies. Dialogues Clin. Neurosci. 2004, 6, 333–341. [Google Scholar] [CrossRef]
- Collins, J.D.; Henley, S.M.D.; Suárez-González, A. A Systematic Review of the Prevalence of Depression, Anxiety, and Apathy in Frontotemporal Dementia, Atypical and Young-Onset Alzheimer’s Disease, and Inherited Dementia. Int. Psychogeriatr. 2020, 35, 457–476. [Google Scholar] [CrossRef] [PubMed]
- Brotherhood, E.V.; Stott, J.; Windle, G.; Barker, S.; Culley, S.; Harding, E.; Camic, P.M.; Caufield, M.; Ezeofor, V.; Hoare, Z.; et al. Protocol for the Rare Dementia Support (RDS) Impact Study. Int. J. Geriart. Psychiatry 2018, 35, 833–841. [Google Scholar] [CrossRef]
- Eriksen, S.; Helvik, A.-S.; Juvet, L.K.; Skovdahl, K.; Førsund, L.H.; Grov, E.K. The Experience of Relations in Persons with Dementia: A Systematic Meta-Synthesis. Dement. Geriatr. Cogn. Disord. 2016, 42, 342–368. [Google Scholar] [CrossRef]
- Nolan, M.R.; Davies, S.; Brown, J.; Keady, J.; Nolan, J. Beyond ‘Person-Centred’ Care: A New Vision for Gerontological Nursing. J. Clin. Nurs. 2004, 13, 45–53. [Google Scholar] [CrossRef]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description—The Poor Cousin of Health Research? BMC Med. Res. Methodol. 2009, 9, 52. [Google Scholar] [CrossRef] [PubMed]
- Wadham, O.; Simpson, J.; Rust, J.; Murray, C. Couples’ Shared Experiences of Dementia: A Meta-Synthesis of the Impact upon Relationships and Couplehood. Aging Ment. Health 2016, 20, 463–473. [Google Scholar] [CrossRef]
- Bannon, S.M.; Grunberg, V.A.; Reichman, M.; Popok, P.J.; Traeger, L.; Dickerson, B.C.; Vranceanu, A.-M. Thematic Analysis of Dyadic Coping in Couples with Young-Onset Dementia. JAMA Netw. Open 2021, 4, e216111. [Google Scholar] [CrossRef]
- Qualtrics Software. Available online: https://www.qualtrics.com/uk/ (accessed on 1 September 2023).
- Sandelowski, M. Whatever Happened to Qualitative Description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Sandelowski, M. What’s in a Name? Qualitative Description Revisited. Res. Nurs. Health 2010, 33, 77–84. [Google Scholar] [CrossRef]
- Kahlke, R.M. Generic Qualitative Approaches: Pitfalls and Benefits of Methodological Mixology. Int. J. Qual. Methods 2014, 13, 37–52. [Google Scholar] [CrossRef]
- Kennedy, D.M. Is It Any Clearer? Generic Qualitative Inquiry and the VSAIEEDC Model of Data Analysis. Qual. Rep. 2016, 21, 1369–1379. [Google Scholar] [CrossRef]
- Chafe, R. The Value of Qualitative Description in Health Services and Policy Research. Valeur de la Description Qualitative dans la Recherche sur les Politiques et Services de Santé. Healthc. Policy 2017, 12, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, A. Description versus interpretation: Competing Alternative Strategies for Qualitative Research. J. Phenomenol. Psychol. 1992, 23, 119–135. [Google Scholar] [CrossRef]
- Macdonald, M.E.; Siedlikowski, S.; Liu, K.; Carnevale, F.A. Introducing SAMMSA: A Five-Step Method for Producing ‘Quality’ Qualitative Analysis. Qual. Health Res. 2023, 33, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Cascio, M.A.; Lee, E.; Vaudrin, N.; Freedman, D.A. A Team-Based Approach to Open Coding: Considerations for Creating Intercoder Consensus. Field Methods 2019, 31, 116–130. [Google Scholar] [CrossRef]
- Sandelowski, M. Words that Should be Seen but Not Written. Res. Nurs. Health 2007, 30, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Mezzalira, S.; Santoro, G.; Bochicchio, V.; Schimmenti, A. Trauma and the Disruption of Temporal Experience: A Psychoanalytical and Phenomenological Perspective. Am. J. Psychoanal. 2023, 83, 36–55. [Google Scholar] [CrossRef]
- Tranvåg, O.; Petersen, K.A.; Nåden, D. Relational Interactions Preserving Dignity Experience: Perceptions of Persons Living with Dementia. Nurs. Ethics. 2015, 22, 577–593. [Google Scholar] [CrossRef] [PubMed]
- Petty, S.; Harvey, K.; Griffiths, A.; Coleston, D.M.; Dening, T. Emotional Distress with Dementia: A Systematic Review using Corpus-based Analysis and Meta-ethnography. Int. J. Geriatr. Psychiatry 2018, 33, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Kitwood, T.; Bredin, K. Towards a Theory of Dementia Care: Personhood and Well-Being. Ageing Soc. 1992, 12, 269–287. [Google Scholar] [CrossRef]
- Poz, R. Facing Degeneration with Compassion on Your Side: Using Compassion Focused Therapy with People with a Diagnosis of Dementia. In Eastern Influences on Neuropsychotherapy; Yeates, G., Farrell, G., Eds.; Routledge: London, UK, 2014; pp. 82–101. ISBN 9780429466618. [Google Scholar]
- Merriam-Webster. Webster’s Seventh New Collegiate Dictionary; Merriam-Webster: Springfield, MA, USA, 1971; ISBN 87779-113-9. [Google Scholar]
- Keyes, S.E.; Clarke, C.L.; Wilkinson, H.; Alexjuk, E.J.; Wilcockson, J.; Robinson, L.; Reynolds, J.; McClelland, S.; Corner, L.; Cattan, M. “We’re All Thrown in the Same Boat…”: A qualitative Analysis of Peer Support in Dementia Care. Dementia 2016, 15, 560–577. [Google Scholar] [CrossRef]
- Rushforth, A.; Ladds, E.; Wieringa, S.; Taylor, S.; Husain, L.; Greenhalgh, T. Long Covid—The Illness Narratives. Soc. Sci. Med. 2021, 286, 114326. [Google Scholar] [CrossRef]
- Bakhtin, M. Problems of Dostoevsky’s Poetics; University of Minnesota Press: Minneapolis, MN, USA, 1984; ISBN 0-8166-1227-7. [Google Scholar]
- Keady, J.D.; Campbell, S.; Clark, A.; Dowlen, R.; Elvish, R.; Jones, L.; Kindell, J.; Swarbrick, C.; Williams, S. Re-thinking and Re-positioning ‘Being in the Moment’ within a Continuum of Moments: Introducing A New Conceptual Framework for Dementia Studies. Ageing Soc. 2022, 42, 681–702. [Google Scholar] [CrossRef]
- Pistrang, N.; Barker, C. Varieties of Qualitative Research. In APA Handbook of Research Methods in Psychology; Cooper, H., Camic, P.M., Long, D.L., Panter, A.T., Rindskopf, D., Sher, K.J., Eds.; American Psychological Association: Washington, DC, USA, 2012; Volume 2, pp. 5–18. ISBN 978-14338-10003-9. [Google Scholar]
- Barker, C.; Pistrang, N. Choosing a Qualitative Method: A Pragmatic, Pluralistic Perspective. In Qualitative Research in Psychology, Expanding Perspectives in Methodology and Design, 2nd ed.; Camic, P.M., Ed.; American Psychological Association: Washington, DC, USA, 2021; ISBN 9781433834455. [Google Scholar]
- Galbraith, D. Writing as Discovery. Br. J. Educ. Psychol. Monogr. Ser. 2009, 11, 5–26. [Google Scholar] [CrossRef]
- Hanauer, D.I. The Writing Processes Underpinning Wellbeing: Insight and Emotional Clarity in Poetic Autoethnography and Freewriting. Front. Commun. 2022, 7, 923824. [Google Scholar] [CrossRef]
- Pennebaker, J.W. Writing about Emotional Experiences as a Therapeutic Process. Psychol. Sci. 1997, 8, 162–166. [Google Scholar] [CrossRef]
- Stevanovic, M.; Peräkylä, A. Experience Sharing, Emotional Reciprocity, and Turn-taking. Front. Psychol. 2015, 6, 450. [Google Scholar] [CrossRef] [PubMed]
- Illingworth, S. Science Communication through Poetry; SpringerLink: New York, NY, USA, 2022; ISBN 978-3-030-96828-1. [Google Scholar]
- Gao, Z. Methodologism/Methodological Imperative. In Encyclopedia of Critical Psychology; Teo, T., Ed.; Springer Nature: London, UK, 2014; pp. 1176–1179. [Google Scholar]
- Cutts, Q.M.; Waters, M.B.S. Poetic Approaches to Qualitative Data Analysis; Oxford Research Encyclopedias: Oxford, UK, 2019. [Google Scholar] [CrossRef]
- Hanauer, I.D. Poetry as Research; John Benjamins Publishing: Amsterdam, The Netherlands, 2010; ISBN 978 90 2723342 4. [Google Scholar]
- Morbey, H.; Harding, A.J.E.; Swarbrick, C.; Ahmed, F.; Elvish, R.; Keady, J.; Williamson, P.R.; Reilly, S.T. Involving People Living with Dementia in Research: An Accessible Modified Delphi Survey for Core Outcome Set Development. Trials 2019, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, P.; Lee, J.; Taylor, R. Evidence-based Poetry: Using Poetic Representation of Phenomenological Research to Create an Educational Tool for Enhancing Empathy in Medical Trainees in the Management of Depression. J. Poet. Ther. 2018, 31, 75–86. [Google Scholar] [CrossRef]
- Moya-Méndez, N.C.; Zwart, H. Science and Poetry: Poems as an Educational Tool for Biology Teaching. Cult. Stud. Sci. Educ. 2022, 17, 727–743. [Google Scholar] [CrossRef]
- Bloom, B.S. (Ed.) Taxonomy of Educational Objectives: The Classification of Educational Goals. Handbook 1: Cognitive Domain; David McKay: New York, NY, USA, 1956. [Google Scholar]
- Krathwohl, D.R. A Revision of Bloom’s Taxonomy: An Overview. Theory Prac. 2002, 41, 212–218. [Google Scholar] [CrossRef]
- Stanny, C.J. Reevaluating Bloom’s Taxonomy: What Measurable Verbs Can and Cannot Say about Student Learning. Educ. Sci. 2016, 6, 37. [Google Scholar] [CrossRef]
- Menix, K.D. Domains of Learning: Interdependent Components of Achievable Learning Outcomes. J. Contin. Educ. Nurs. 1996, 27, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.J. What does emotion have to do with learning? Everything! J. Food Sci. Educ. 2017, 16, 64–66. [Google Scholar] [CrossRef]
- Speare, J.; Henshall, A. ‘Did Anyone Think the Trees were Students?’: Using Poetry as a Tool for Critical Reflection. Reflective Prac. 2014, 15, 807–820. [Google Scholar] [CrossRef]
- Neuman, K.A.; Friedman, B.D. Affective Learning: A Taxonomy for Teaching Social Work Values. J. Soc. Work Values Ethics 2010, 7, 2–13. [Google Scholar] [CrossRef]
- Muszkat, M.; Ben Yehuda, A.; Moses, S.; Naparstek, Y. Teaching empathy through poetry: A clinically based model. Med. Educ. 2010, 44, 503. [Google Scholar] [CrossRef]
- Ball, S.; Leach, B.; Bousfield, J.; Smith, P.; Marjanovic, S. Arts-Based Approaches to Public Engagement with Research; Rand Corporation: Cambridge, UK, 2021. [Google Scholar]
- Carr, J.M. Poetic Expressions of Vigilance. Qual. Health Res. 2003, 13, 1324–1331. [Google Scholar] [CrossRef]
- Williams, E.N.; Morrow, S.L. Achieving Trustworthiness in Qualitative Research: A Pan-Paradigmatic Perspective. Psychother. Res. 2009, 19, 576–582. [Google Scholar] [CrossRef]
- Riedijk, S.R.; De Vugt, M.E.; Duivenvoorden, H.J.; Niermeijer, M.F.; Van Swieten, J.C.; Verhey, F.R.J.; Tibben, A. Caregiver Burden, Health-Related Quality of Life and Coping in Dementia Caregivers: A Comparison of Frontotemporal Dementia and Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2006, 22, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Stamou, V.; La Fontaine, J.; Gage, H.; Jones, B.; Williams, P.; O’Malley, M.; Parkes, J.; Carter, J.; Oyebode, J. Services for People with Young Onset Dementia: The ‘Angela’ Project National UK Survey of Service Use and Satisfaction. Int. J. Geriatr. Psychiatry 2021, 36, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Woolley, J.D.; Khan, B.K.; Murthy, N.K.; Miller, B.L.; Rankin, K.P. The Diagnostic Challenge of Psychiatric Symptoms in Neurodegenerative Disease: Rates of and Risk Factors for Prior Psychiatric Diagnosis in Patients with Early Neurodegenerative Disease. J. Clin. Psychiatry 2011, 72, 126–133. [Google Scholar] [CrossRef]
- Merrick, K.; Camic, P.M.; O’Shaughnessy, M. Couples Constructing their Experiences of Dementia: A Relational Perspective. Dementia 2016, 15, 34–50. [Google Scholar] [CrossRef]
- Carter, G.; Monaghan, C.; Santin, O. What is Known from the Existing Literature about Peer Support Interventions for Carers of Individuals Living with Dementia: A Scoping Review. Health Soc. Care Community 2020, 28, 1134–1151. [Google Scholar] [CrossRef]
- Smith, R.; Drennan, V.; Mackenzie, A.; Greenwood, N. The Impact of Befriending and Peer Support on Family Carers of People Living with Dementia: A Mixed Methods study. Arch. Gerontol. Geriatr. 2018, 76, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.P.; Williams, V.; Grillo, A.; McKee-Jackson, R.; Camic, P.M.; Windle, G.; Stott, J.; Brotherhood, E.; Crutch, S.J. Peer Support for People Living with Rare and Young Onset Dementia: An Integrative Review. Dementia 2022, 21, 2700–2726. [Google Scholar] [CrossRef]
- Clarke, C.L.; Wilcockson, J.; Watson, J.; Wilkinson, H.; Keyes, S.; Kinnaird, L.; Williamson, T. Relational Care and Co-operative Endeavour: Reshaping Dementia Care through Participatory Secondary Data Analysis. Dementia 2020, 19, 1151–1172. [Google Scholar] [CrossRef]
- Hennessy, J.; Mannix Mcnamara, P. Packaging poetry? Pupils’ Perspectives of their Learning Experience within the Post-primary Poetry Classroom. Engl. Educ. 2011, 45, 206–223. [Google Scholar] [CrossRef]
- Xerri, D. Colluding in the ‘Torture’ of Poetry: Shared Beliefs and Assessment. Engl. Educ. 2013, 47, 134–146. [Google Scholar] [CrossRef]
- Weaven, M.; Clark, T. ‘I guess it scares us’—Teachers Discuss the Teaching of Poetry in Senior Secondary English. Engl. Educ. 2013, 47, 197–212. [Google Scholar] [CrossRef]
- Fletcher, J.R. Renegotiating Relationships: Theorising Shared Experiences of Dementia within the Dyadic Career. Dementia 2020, 19, 708–720. [Google Scholar] [CrossRef] [PubMed]
- Windle, G.; Algar-Skaife, K.; Caulfield, M.; Pickering-Jones, L.; Killick, J.; Zeilig, H.; Tischler, V. Enhancing Communication between Dementia Care Staff and their Residents: An Arts-Inspired Intervention. Aging Ment. Health 2020, 24, 1306–1315. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.J.; Warren, J.D. Shouting from far away: Three poems about living with speechlessness. Pract. Neurol. 2023, 23, 176–177. [Google Scholar] [CrossRef] [PubMed]
- Zeilig, H.; Tischler, V.; van der Byl Williams, M.; West, J.; Strohmaier, S. Co-Creativity, Well-Being and Agency: A Case Study Analysis of a Co-Creative Arts Group for People with Dementia. J. Aging Stud. 2019, 49, 16–24. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Age a (Mean = 63.0, SD = 9.8) | |
| Gender b | |
| Female | 47 (70.1) |
| Male | 20 (29.9) |
| Diagnostic subtype * | |
| PCA 1 | 26 (36.6) |
| FTD 2 | 22 (31.0) |
| PPA 3 | 9 (12.7) |
| YOAD 4 | 7 (9.9) |
| Mixed dementia | 4 (5.6) |
| Other dementia 5 | 3 (4.2) |
| Status | |
| PLwRD 6 | 27 (38.0) |
| Care-partner | 39 (54.9) |
| Bereaved carer | 5 (7.0) |
| Relationship to PLwRD | |
| Spouse | 33 (75.0) |
| Child | 8 (18.2) |
| Other relative | 3 (6.8) |
| Ethnicity c | |
| Caucasian | 63 (92.6) |
| Asian | 4 (5.9) |
| Métis d | 1 (1.5) |
| Professionals | Students | |
|---|---|---|
| Sex | ||
| Male | 13 | 7 |
| Female | 41 | 28 |
| Non-Binary | 0 | 2 |
| Prefer not to say | 1 | 1 |
| Age | ||
| 18–29 | 4 | 31 |
| 30–39 | 15 | 6 |
| 40–49 | 15 | 0 |
| 50–59 | 11 | 0 |
| 60+ | 10 | 0 |
| Location | ||
| Canada | 1 | 38 |
| United Kingdom | 50 | 0 |
| United States | 3 | 0 |
| Other | 1 | 0 |
| Occupation | ||
| Researcher | 5 | 0 |
| Psychologist (Clinical) | 18 | 0 |
| Nurse | 7 | 0 |
| Psychotherapist/Counsellor | 2 | 0 |
| Occupational Therapist | 4 | 0 |
| Social Worker | 2 | 0 |
| Neuropsychologist | 3 | 0 |
| Paid Caregiver | 1 | 0 |
| Other | 8 | 0 |
| Honours Bachelor of Social Work Student | 0 | 18 |
| Bachelor of Science Nursing Student | 0 | 20 |
| Dementia Care Experience | ||
| Yes | 44 | 18 |
| No | 11 | 20 |
| Types of Dementia Experience | ||
| Frontotemporal dementia | 22 | 13 |
| Young onset Alzheimer’s dementia | 33 | 12 |
| Lewy body dementia | 31 | 15 |
| Posterior cortical atrophy | 15 | 0 |
| Familiar Alzheimer’s disease | 24 | 13 |
| Familiar frontotemporal dementia | 14 | 6 |
| Other | 12 | 4 |
| Read or Wrote Poetry in last 5 years | ||
| Yes | 14 | 13 |
| No | 41 | 25 |
| Prompts | Themes/Subthemes | Associated Poems 1 |
|---|---|---|
| Prompt 1: What is your experience of having (type of dementia) or being a family member caring for someone with this type of dementia? | Temporality Disrupted Uncharted Territory Being in the Moment Rediscovering Identities and Relationships | (1) A Steep Learning Curve (2) Still Me (3) No One Would Believe Me (4) Changing (5) Eleven (6) Accept This Honour (7) When Will I No Longer Be Me? (8) Out Here in The Rain (9) How May I Help You? |
| Prompt 2: How would you describe (type of dementia) to a friend or family member? | A Rollercoaster Heart-Breaking Losses Shifting Selves and Changing WorldsMisdiagnosed and Misunderstood | (10) Bewilderingly So (11) Where to Begin (12) Unwavering Braveness (13) There is So Much I Could Say (14) Description (15) I Know You Have Noticed (16) Tumbling, Jumbling (17) Why I Repeat the Same Question at Random (18) Who Our Loved Ones Used To Be |
| Prompt 3: What does support mean to you? | Multidimensional Support Not in This alone Compassion and UnderstandingSupport as an Action | (19) Truth: A Fib (20) SUPPORT (21) What Else Could I Try To Do (22) A Journey (23) Relief (24) Help Me (25) To Continue (26) The Resiliency (27) Please Stick Around |
| Themes/ Prompts | Sub-Themes | Illustrative Quotes |
|---|---|---|
| Temporality Disrupted/What is your experience of having (type of dementia) or being a family member caring for someone with this type of dementia? | Unchartered Territory | “A journey into the unknown, caring in love, the constant challenge of adapting” (6.5.PCA.C-1); “Doors closing, fading slowly. Becoming invisible and written off” (9.12.FTD.PLwRD-1); “uncharted territory, cascading loss, fear and uncertainty about what’s coming next” (13.5.PCA.C-1); “The sister I loved so dearly was being taken from me, piece by piece” (10.2.YOAD.BC-1); “Our dreams are shattered and we will never be the same again, I never thought a disease could be so horrible and have such a dramatic impact on a family” (13.11.FTD.C-1); “Losses of myself, my essence, my work, my driver’s licence, my job, my body, friends, love of husband” (13.12.FTD.PLwRD-1); “I’m stuck here with a rare disea eeeze and the physicians don’t have a clue” (12.5.LBD.C-1); “professionals [who] seem at a loss and are slow to respond” (13.9.PCA.PLwRD-1) |
| Being in the Moment | “Time slows down and remembering to truly be in the moment” (5.1.PCA.BC-1) “Trying to be positive and know these moments with him won’t come again” (10.4.MD.C-1) “Take every opportunity to have a laugh” (6.17.PCA.PLwRD-1)“At first it was a hectic pace, as time passed I felt more at peace that I am doing the best I can do” (8.3.FTD.C-1). | |
| Re-discovering Identities and Relationships | “Then curiosity and call to action took over. I have been learning about myself and a brighter side of this world ever since. I am energised and happy” (11.10.PPA.PLwRD-1); “I needed to accept what was what and become a better person. I needed to fight, be more patient and find answers. (8.3.FTD.C) | |
| A Rollercoaster/How would you describe (type of dementia) to a friend or family member? | Heartbreaking Losses | “heart breaking” (10.3.YOAD.C-2; 12.7.FTD.BC-2; 9.10.FTD.C-2); “frightening” (9.16. FTD.C-2; 6.23.PCA.PLwRD-2); “The Destroyer of Lives” (9.11.FTD.C-2); “the cruellest dementia you have never heard of” (9.3.FTD.C-2); a “rollercoaster” (12.7.FTD.BC-2; 5.8.PCA.BC-2); “constant emotional and physical ups-and-downs” (8.3.PPA.C-1) “She is still the same person, but is not able to do the things she used to do because of the disease” (13.10.PCA.C-2); “Not able to make any decisions big or small on most basic tasks. Choking often, falling, loss of balance. Loss of not being able to accomplish what used to be second nature” (13.12.FTD. PLwRD-2); “Brain blindness. Extreme turmoil. Unwavering braveness. An excruciatingly slow drip of profound loss” (7.7.PCA-C-2). |
| Shifting Selves and Changing Worlds | “A disease that…erodes everything you thought about that person and your relationship with them. A disease that eats away the soul of the person and everything they are or who they had wanted to be.” (9.10.FTD.C-2). Profound changes in how the self relates to the world created a sense invisibility, “Increasing opacity between me and the world” (11.5.PPA.PLwRD-2), “You just don’t see me anymore” (12.4.YOAD, PLwRD-2); “retreating into own world” (9.4.FTD.C-2). | |
| Misdiagnosed and Misunderstood | “Things aren’t where they appear to be. Which way round does this go? Where is the top or the bottom?” (6.5.PCA.C-2)“A neurological disease that does not follow the perceived norms of dementia of memory loss and only for the older person but far more aggressive and devastating as it affects behaviours and personalities of younger people in ways that make them disinhibited, lacking empathy and insight” (9.10.FTD.C-2); “a misdiagnosed and misunderstood condition” (6.22. PCA.C-2); “they never say drop him off to my house and get your hair done … they just say LOOK AFTER YOURSELF” (9.20.FTD.C-1) | |
| Multidimensional Support/What does support mean to you? | Not in This Alone | “Support means not feeling utterly alone. It means having someone to help bear the unbearable” (P7.7.PCA.C-3); “Meeting others who are in the same place as you and who understand” (P9.10. FTD.C-3); “a togetherness beyond family” (P5.1.PCA.BC-3); “Support helps me when I get confused and frustrated…it helps me live my life independently” (P6.1.PCA.PLwRD-3); “Being part of a PPA network, not feeling alone…giving me a degree of comfort” (P11.1.PPA.PLwRD-3); “Subject matter experts who listen objectively and share their expertise” (P8.3.FTD.C-3); “Professional help to educate doctors and the general public” (P13.12.FTD.PLwRD-3); “Provide support strategies that are specific to my condition” (P13.9.PCA.PLwRD-3) “Others understand or have travelled this road as well” (P13.2.YOAD.C-3). |
| Compassion and Understanding | “Support means you are aboard my train and will help in any way you can” (P8.4.FTD.C-3); “Taking time to listen and giving time for talking (P13.PCA.PLwRD-3); “In between there is support that helps me see things differently and support that just takes time to listen and see things the way I do” (P10.3YOAD.C-3); “Old fashioned underwear” (P6.8.PCA.C-3); “From someone to hug me to someone who can take over when it’s too much. Someone who listens….and believes me” (P10.1.FTD.C-3); “Learn to accept me as I am, with all my faults and errors” (P12.4.YOAD.PLwRD-3); “Not judged by expression of my thoughts or feelings” (P10.2.YOAD.C-3); “Support me by showing acceptance” (P12.6.VD.PLwRD-3); Help to affirm decisions” (P5.2.PCA.C-3). | |
| Support As An Action | “Always include stimulation. Always include companionship” (P12.3.FTD.PLwRD-3); “Support means enablement/kicking ass/being there when down” (P6.14.PCA.PLwRD-3); “It lifts me up in times of doubt. It allows me to move forward in a positive way with my life.” (P11.12.FTD.PLwRD-3); “Unconditional actions to ease the burden of care” (P12.7.FTD.BC-3); “If I am able to connect/talk with others that have PPA and I am able to help/support them—that is very helpful for me” (P7.4.PPA.PLwRD-3); “Support is helping me to feel better about myself as I contribute to help others.” (P7.4.PCA.C-3) |
| Stakeholder Group | Themes | Sub-Themes | Illustrative Quotes |
|---|---|---|---|
| PLwRD | I Wanted to Do It | Challenging but Enjoyable | “I am much more comfortable with the written word than I am with verbal conversation and that carries over to writing poetry”; (12.4.YOAD.PLwRD-1), “I found it very easy to just sit quietly and let my thoughts form my words” (12.6.YOVaD/.PLwRD-2), “I found finding the words was relatively easy as it was around the basic support that I feel I need on an ongoing basis (11.12.FTD.PLwRD-3)”; “Challenging but nonetheless enjoyable” (11.1.PPA.PLwRD-2); “I found the first word was difficult and challenging, but found after the first word was down, the rest just seemed to come easily, and it was then enjoyable” (6.1.PCA.PLwRD-2); “Having never written poetry before I found it challenging but a positive thing to do” (6.7.PCA.PLwRD-3). |
| Hurts So Much | “I had a very hard time understanding the question and accessing the words. I felt very detached” (13.3.YOAD.PLwRD-2); “Sensed that I was having problems, Frustrated, when can’t remember” (8.1.PPA.PLwRD-2); “Challenging and to start and scary to go in your feelings cause I try to suppress how I really feel cause I’m afraid to go negative and think of all that hurts so very much but it ends up feeling so good to get it off your chest and ends up being cathartic. So much that I would like to go deeper and write more and get out my sad feelings instead of pushing them so deep and these 2 exercises have made me realize how good it is to see it on paper and hear it read by someone. It’s such a good idea.” (13.12.FTD.PLwRD-2). | ||
| Purposeful | See Section 3.2.1 in the text | ||
| Care-Partners | Consolidating | Challenging/Difficult | “Challenging to distil my thoughts in just a few words” (6.5.PCA.C-1) “I struggled a bit to decide on what words really captured my experience” (10.3.YOAD.C-3, “First was the battle of just getting to the task but to actually sit down and consolidate the thoughts into sentences was met with great reluctance” (13.10.PCA.C-2). |
| Enjoyable | “It was easy and enjoyable for me. The words popped into my head quite readily. It was interesting to me to realize how much can be said with just a few words (13.8.FTD.C-1); “The experience was enjoyable because I think of many words that mean ‘support’. It was cathartic to put those words on paper, and I felt less isolated and more supported knowing that other people were doing the same thing” (13.8.FTD.C-3). | ||
| Purposeful | “It was not a challenging task because I immediately knew what I wanted to say and I found it exciting to add to the gut-level offering I knew it would become…My staccato words express the small bites at life which is our daily experience; one thing at a time is the only way to survive this.....for us.” (9.11.FTD.C-1); “…forced me to truly think about what I would most want a friend or family member to know about the diagnosis from my perspective as care partner to my wife. I believe I captured that well” (8.4.FTD.C-2). | ||
| Reflective | “In the end I decided to share some of the common themes I would tell others during the experience. It was touching to remember those days and to reflect on how I feel now versus how much harder it was when she was alive” (10.3.YOAD.BC-1); “It was helpful in causing me to actually sit down and reflect on what we wanted (needed?) people to know and how to interact” (13.10.PCA.C-2). |
| Stakeholder Group | Themes | Sub-Themes | Illustrative Quotes |
|---|---|---|---|
| PLwRD | A Collection of Understandings | Has Meaning for Me | “I love the completed poem, it has a meaning to me as I can relate to the words written down, and it’s interesting to see how a poem can be thought of by a list off words or sentences by different people” (6.1.PCA.PLwRD-1); I liked the way our various views and feelings were interwoven with other people’s responses to give an active description of the challenges of life living alongside dementia” (11.12.FTD.PLwRD-1); “I appreciated being able to describe some of my feelings about being ill and the sadness about no treatment/cure” (7.4.PPA.PLwRD-1); “It touches a chord for me. I absolutely like it and feel less alone in this…now I rarely write but when I read something good I’m amazed at the craft and how people put the beautiful words together and convey images or feelings succinctly. I can’t get it out right and it hurts that I’ve lost it but this makes me want to try again. Thank you! Great idea” (13.12.FTD.PLwRD-2). |
| Staying Connected | “The poem helps to capture the different ways people are thinking about what support should be for them. The words or the ways of saying may be different, but the emotions and concerns behind those words are very similar. Clearly articulates the emotional and personal aspects of what are perceived as needs—caring, communicating, staying connected, kindness—seem to override the many physical supports required although they are just as important for the overall well-being of the person and their care giver)s)” (13.9.PCA.PLwRD-3); “I liked the idea that the words were formed into a virtual buttress to allow us to fight back and defend us from the trials and tribulations that our condition now causes us in our lives.” (11.12.FTD.PLwRD-3). | ||
| Not Speaking to Me | “Sorry, did not sound like a poem—but maybe I am not up to date on how poems are now/can be. My words were taken fine. Very short comments—thought they could be elaborated more” (7.4.PPA.PLwRD-1); “It was more like a statement than a poem. It read a little bit like a poem, but much more like a book” (11.1.PPA.PLwRD-1); “To me with my understanding of what a poem is I did not find it to be a poem just a collection of words” (12.2.YOVaD.PLwRD-1); “I did not appreciate the poem. It seemed a little cumbersome and though I understand that these words were contributed by group members, I do not feel that the author expressed our deeper feelings” (11.10.PPA.PLwRD-2). | ||
| Care- partners | Crystallise Lived Experience | Bringing Into a Whole | “I really liked how it started out in the first line. FTD is indeed a journey. Then....beginning each stanza with the words “There is so much I could say...” Then, you HEAR this spoken from the perspective of each care partner. Each stanza stands on its own and is unique, which, to me, speaks to the disease itself. I very much treasure the final product and the creativity to bring individual parts into a whole” (8.4.FTD.C-2); “Beforehand was cynical about how a poem could be constructed from a collection of words submitted by various contributors. The final poem crystallises the various feelings, emotions and experiences of rare dementia carers” (5.8.PCA.BC-1);“Both my husband and myself really loved the finished poem and felt it expressed so clearly what it feels like to suffer from PCA. The title is excellent and the repetition of the first and last lines in each verse is particularly effective” (6.5.PCA.C-2); “Spoke volumes to me! It is amazing how different people’s thoughts could come together to create such a symbolic poem of dementia” (10.2.YOAD.BC-1). |
| Not feel alone | “Reading the pain and hope of others makes me feel connected, and this disease typically causes such rifts of disconnection” (10.5.PPA.C-1). Initially I felt overwhelming sadness and grief, while at the same time it’s helpful to know you’re not alone in experiencing the impact the condition can cause” (5.7.PCA.BC-2). | ||
| Shared experience | “Our poem appears to be a first opportunity for some of Eleven (as I now think of us) to experience their feelings in this way. I do not want it to stop. I KNOW those feelings, I have them EVERY day.....somehow there is comfort in sharing the awfulness of it all” (9.11.FTD.C-1). I enjoyed reading the poem because it was a thoughtful compilation of our shared experience with PCA. Hearing the thoughts and feelings of others living this challenge was comforting, encouraging, and empowering” (13.5.PCA.C-1); “I found reading it made me feel extremely emotional, it created a very strong response, seeing my words on the page amongst those of other people who are sharing different stages of this condition” (5.7.PCA.BC-2); “The completed poem makes me feel oddly secure. Caregiving is often a very isolating experience. Tying our reflections all together tethers our boats together” (10.5.PPA.C-3). | ||
| Non-Resonating | “The poem does not meet the brief for me. As a means to inform those ignorant of FTD and its awfulness, it fails to elicit enough disgust, nor raise compassion towards those who daily battle it. I do thank the poet, of course” (9.11.FTD.C-2). “It was good to hear the words of others and to compare them (similarities and differences) to your own thoughts. We had thought that the ideas and feelings would be synthesized into a more holistic ‘statement’ that provided insight into the emotional and personal challenges experienced by this ‘group of people’ as a whole…(the poem) seems to be incomplete and lacks the emotional and insightful impact you would hope for in a poem of this nature” (13.10.PCA.C-2). |
| Lived Experience and Reflection | Hearing Own Experience in a different Way Validating Invisible Distress Multi-Voiced or Group Lived Experience Poetry Conveys Emotion and Meaning |
| Curiosity and Exploration | Creative aspect piquing interest Novel methodology and experience No wrong answers (gut response) |
| Barriers and Inclusivity | Am I a poetry person? Poetry as scary Reading all the poems was overwhelming |
| Sharing the Poems | Value as activity vs. value as product Where and how to disseminate Risks and benefits of sharing the poems |
| Participant Group | N | Poems |
|---|---|---|
| Group 1: | Hear My Pain | |
| Professionals | 14 | Tumble Jumble |
| Students | 16 | Support |
| Group 2: | Eleven | |
| Professionals | 20 | There’s So Much I Could Say |
| Students | 13 | Still Me |
| Group 3: | Steep Learning | |
| Professionals | 21 | When Will I Know Longer Be Me |
| Students | 9 | Accept This Honour |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camic, P.M.; Sullivan, M.P.; Harding, E.; Gould, M.; Wilson, L.; Rossi-Harries, S.; Grillo, A.; McKee-Jackson, R.; Cox, S.M.; Stott, J.; et al. ‘Misdiagnosed and Misunderstood’: Insights into Rarer Forms of Dementia through a Stepwise Approach to Co-Constructed Research Poetry. Healthcare 2024, 12, 485. https://doi.org/10.3390/healthcare12040485
Camic PM, Sullivan MP, Harding E, Gould M, Wilson L, Rossi-Harries S, Grillo A, McKee-Jackson R, Cox SM, Stott J, et al. ‘Misdiagnosed and Misunderstood’: Insights into Rarer Forms of Dementia through a Stepwise Approach to Co-Constructed Research Poetry. Healthcare. 2024; 12(4):485. https://doi.org/10.3390/healthcare12040485
Chicago/Turabian StyleCamic, Paul M., Mary Pat Sullivan, Emma Harding, Martha Gould, Lawrence Wilson, Sam Rossi-Harries, Adetola Grillo, Roberta McKee-Jackson, Susan M. Cox, Joshua Stott, and et al. 2024. "‘Misdiagnosed and Misunderstood’: Insights into Rarer Forms of Dementia through a Stepwise Approach to Co-Constructed Research Poetry" Healthcare 12, no. 4: 485. https://doi.org/10.3390/healthcare12040485
APA StyleCamic, P. M., Sullivan, M. P., Harding, E., Gould, M., Wilson, L., Rossi-Harries, S., Grillo, A., McKee-Jackson, R., Cox, S. M., Stott, J., Brotherhood, E. V., Windle, G., & Crutch, S. J. (2024). ‘Misdiagnosed and Misunderstood’: Insights into Rarer Forms of Dementia through a Stepwise Approach to Co-Constructed Research Poetry. Healthcare, 12(4), 485. https://doi.org/10.3390/healthcare12040485