

Hospital Incidence, Sex Disparities, and Perioperative Mortality in Open Surgically Treated Patients with Aneurysms of the Ascending Aorta and Aortic Arch in Switzerland

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
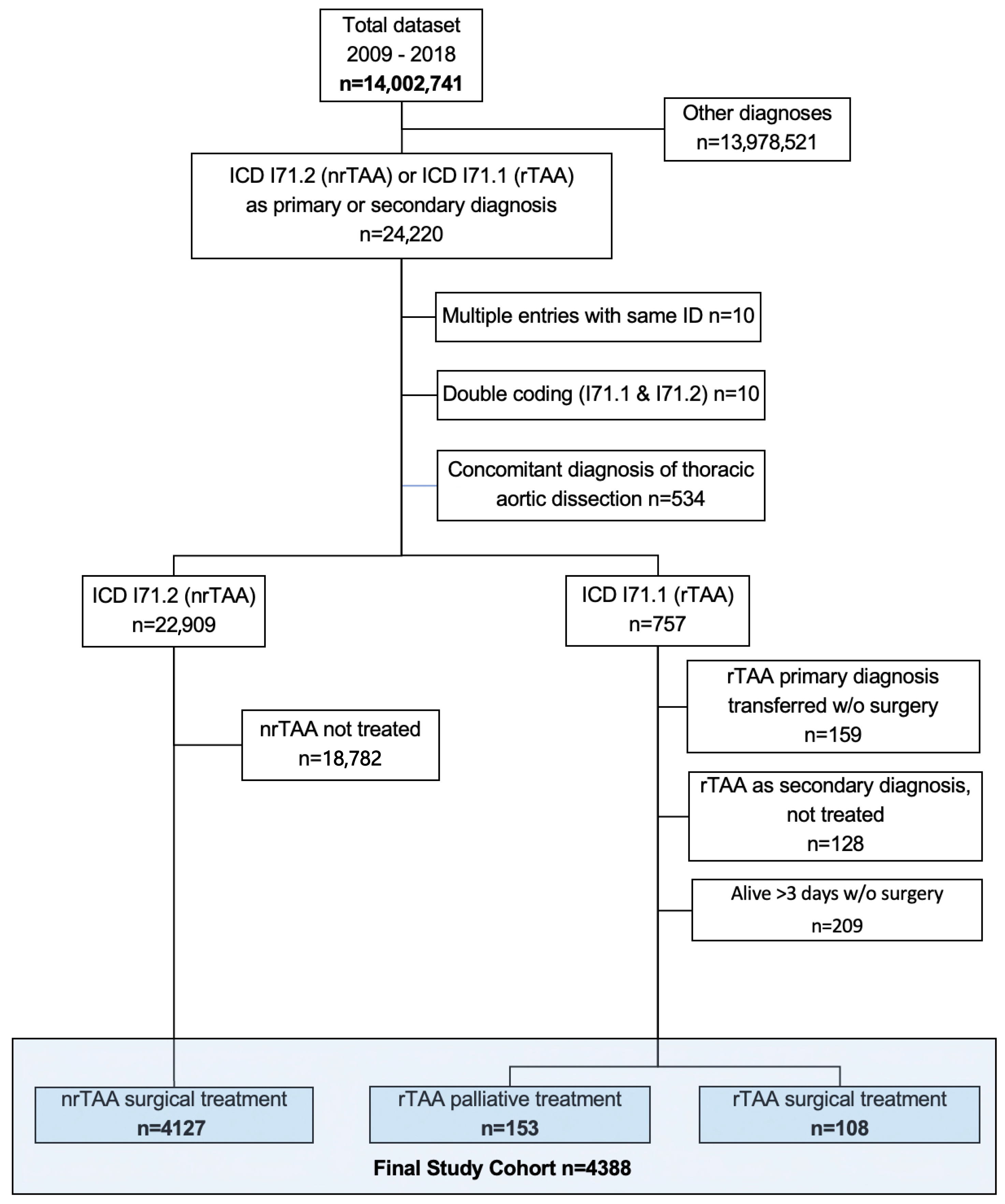
2.1. Inclusion and Exclusion Criteria
2.2. Statistical Analysis
3. Results
3.1. Epidemiology
3.2. Treatment Specifications and Outcomes in nrAA
3.3. Treatment Specifications and Outcomes in rAA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdulameer, H.; Al Taii, H.; Al-Kindi, S.G.; Milner, R. Epidemiology of Fatal Ruptured Aortic Aneurysms in the United States (1999–2016). J. Vasc. Surg. 2019, 69, 378–384.e2. [Google Scholar] [CrossRef] [PubMed]
- Clouse, W.D.; Hallett, J.W.J.; Schaff, H.V.; Gayari, M.M.; Ilstrup, D.M.; Melton, L.J., 3rd. Improved Prognosis of Thoracic Aortic Aneurysms: A Population-Based Study. JAMA 1998, 280, 1926–1929. [Google Scholar] [CrossRef] [PubMed]
- Olsson, C.; Thelin, S.; Ståhle, E.; Ekbom, A.; Granath, F. Thoracic Aortic Aneurysm and Dissection: Increasing Prevalence and Improved Outcomes Reported in a Nationwide Population-Based Study of More than 14,000 Cases from 1987 to 2002. Circulation 2006, 114, 2611–2618. [Google Scholar] [CrossRef] [PubMed]
- Meuli, L.; Menges, A.-L.; Steigmiller, K.; Kuehnl, A.; Reutersberg, B.; Held, U.; Zimmermann, A. Hospital Incidence and Mortality of Patients Treated for Abdominal Aortic Aneurysms in Switzerland—A Secondary Analysis of Swiss DRG Statistics Data. Swiss Med. Wkly. 2022, 152, w30191. [Google Scholar] [CrossRef] [PubMed]
- Tala, P.; Kyllönen, K.E.; Harjola, P.; Appelqvist, P. Aneurysms of the Thoracic and Abdominal Aorta. I. Incidence of Aortic Aneurysm in 10,392 Autopsies. Ann. Chir. Gynaecol. Fenn. 1967, 56, 270–277. [Google Scholar] [PubMed]
- Huang, Y.; Schaff, H.V.; Dearani, J.A.; Oderich, G.S.; Bower, T.C.; Kalra, M.; Greason, K.L.; Pochettino, A.; Viehman, J.K.; Harmsen, W.S.; et al. A Population-Based Study of the Incidence and Natural History of Degenerative Thoracic Aortic Aneurysms. Mayo Clin. Proc. 2021, 96, 2628–2638. [Google Scholar] [CrossRef] [PubMed]
- Geisbüsch, S.; Kuehnl, A.; Salvermoser, M.; Reutersberg, B.; Trenner, M.; Eckstein, H.-H. Increasing Incidence of Thoracic Aortic Aneurysm Repair in Germany in the Endovascular Era: Secondary Data Analysis of the Nationwide German DRG Microdata. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 499–509. [Google Scholar] [CrossRef]
- ICD10 Data. Available online: https://www.icd10data.com/ICD10CM/Codes (accessed on 10 November 2023).
- Bentall, H.; De Bono, A. A Technique for Complete Replacement of the Ascending Aorta. Thorax 1968, 23, 338–339. [Google Scholar] [CrossRef]
- David, T.E.; Feindel, C.M. An Aortic Valve-Sparing Operation for Patients with Aortic Incompetence and Aneurysm of the Ascending Aorta. J. Thorac. Cardiovasc. Surg. 1992, 103, 617–621; discussion 622. [Google Scholar] [CrossRef]
- David, T.E.; Feindel, C.M.; Webb, G.D.; Colman, J.M.; Armstrong, S.; Maganti, M. Aortic Valve Preservation in Patients with Aortic Root Aneurysm: Results of the Reimplantation Technique. Ann. Thorac. Surg. 2007, 83, S732–S735; discussion S785–S790. [Google Scholar] [CrossRef]
- Dake, M.D.; Miller, D.C.; Semba, C.P.; Mitchell, R.S.; Walker, P.J.; Liddell, R.P. Transluminal Placement of Endovascular Stent-Grafts for the Treatment of Descending Thoracic Aortic Aneurysms. N. Engl. J. Med. 1994, 331, 1729–1734. [Google Scholar] [CrossRef] [PubMed]
- Abisi, S.; Elnemr, M.; Clough, R.; Alotaibi, M.; Gkoutzios, P.; Modarai, B.; Haulon, S. The Development of Totally Percutaneous Aortic Arch Repair with Inner-Branch Endografts: Experience from 2 Centers. J. Endovasc. Ther. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Garg, K.; Pergamo, M.; Jiang, J.; Smith, D. Endovascular Stenting of the Ascending Aorta for Visceral Malperfusion in a Patient with Type A Aortic Dissection. J. Vasc. Surg. Cases Innov. Tech. 2023, 9, 101341. [Google Scholar] [CrossRef] [PubMed]
- Ghoreishi, M.; Chahal, D.; Shah, A.; Kang, J.; Hirsch, J.; Tran, D.; McCloskey, D.; Shkullaku, M.; Gupta, A.; Strauss, E.R.; et al. First-in-Human Endovascular Aortic Root Repair (Endo-Bentall) for Acute Type A Dissection. Circ. Cardiovasc. Interv. 2023, 16, e013348. [Google Scholar] [CrossRef] [PubMed]
- Schweizerische Operationsklassifikation (CHOP). Systematisches Verzeichnis–Version 2022. Available online: https://bit.ly/3zYViv6 (accessed on 10 November 2023).
- STROBE. Strengthening the Reporting of Observational Studies in Epidemiology. Available online: https://www.strobe-statement.org/ (accessed on 10 November 2023).
- Federal Statistical Office. Permanent and Nonpermanent Resident Population by Institutional Units, Citizenship (Category), Sex and Age. 2020. Available online: https://www.pxweb.bfs.admin.ch/pxweb/de/px-x-0102010000_101/-/px-x-0102010000_101.px (accessed on 10 November 2023).
- Gesundheitsberichterstattung des Bundes. 2020. Available online: https://www.gbe-bund.de/gbe/pkg_isgbe5.prc_menu_olap?p_uid=gast&p_aid=3767823&p_sprache=D&p_help=0&p_indnr=1000&p_indsp=&p_ityp=H&p_fid= (accessed on 10 November 2023).
- Federal Statistical Office. Population Data. 2020. Available online: https://www.bfs.admin.ch/bfs/en/home/statistics/population.assetdetail.14367975.html (accessed on 10 November 2023).
- Altman, D.G.; Machin, D.; Bryant, T.; Gardner, M. Statistics with Confidence: Confidence Intervals and Statistical Guidelines, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- van Walraven, C.; Austin, P.C.; Jennings, A.; Quan, H.; Forster, A.J. A Modification of the Elixhauser Comorbidity Measures into a Point System for Hospital Death Using Administrative Data. Med. Care 2009, 47, 626–633. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. Vienna Austria R Foundation for Statistical Computing. 2013. Available online: https://www.r-project.org/, (accessed on 16 May 2023).
- Lodewyks, C.L.; Prior, H.J.; Hiebert, B.M.; Nickel, N.C.; Yamashita, M.H.; Ouzounian, M.; Kumar, K.K.; Arora, R.C.; Tangri, N. A Province-Wide Analysis of the Epidemiology of Thoracic Aortic Disease: Incidence Is Increasing in a Sex-Specific Way. Can. J. Cardiol. 2020, 36, 1729–1738. [Google Scholar] [CrossRef] [PubMed]
- McClure, R.S.; Brogly, S.B.; Lajkosz, K.; Payne, D.; Hall, S.F.; Johnson, A.P. Epidemiology and Management of Thoracic Aortic Dissections and Thoracic Aortic Aneurysms in Ontario, Canada: A Population-Based Study. J. Thorac. Cardiovasc. Surg. 2018, 155, 2254–2264.e4. [Google Scholar] [CrossRef]
- Gouveia, E.; Melo, R.; Mourão, M.; Caldeira, D.; Alves, M.; Lopes, A.; Duarte, A.; Fernandes, E.; Fernandes, R.; Mendes Pedro, L. A Systematic Review and Meta-Analysis of the Incidence of Acute Aortic Dissections in Population-Based Studies. J. Vasc. Surg. 2022, 75, 709–720. [Google Scholar] [CrossRef]
- Ailawadi, G.; Eliason, J.L.; Roelofs, K.J.; Sinha, I.; Hannawa, K.K.; Kaldjian, E.P.; Lu, G.; Henke, P.K.; Stanley, J.C.; Weiss, S.J.; et al. Gender Differences in Experimental Aortic Aneurysm Formation. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 2116–2122. [Google Scholar] [CrossRef]
- Beyer, S.E.; Secemsky, E.A.; Khabbaz, K.; Carroll, B.J. Elective Ascending Aortic Aneurysm Repair Outcomes in a Nationwide US Cohort. Heart 2023, 109, 1080–1087. [Google Scholar] [CrossRef]
- Gökalp, A.L.; Thijssen, C.G.E.; Bekkers, J.A.; Roos-Hesselink, J.W.; Bogers, A.J.J.C.; Geuzebroek, G.S.C.; Houterman, S.; Takkenberg, J.J.M.; Mokhles, M.M. Male-Female Differences in Contemporary Elective Ascending Aortic Surgery: Insights from the Netherlands Heart Registration. Ann. Cardiothorac. Surg. 2023, 12, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Flink, B.J.; Long, C.A.; Duwayri, Y.; Brewster, L.P.; Veeraswamy, R.; Gallagher, K.; Arya, S. Women Undergoing Aortic Surgery Are at Higher Risk for Unplanned Readmissions Compared with Men Especially When Discharged Home. J. Vasc. Surg. 2016, 63, 1496–1504.e1. [Google Scholar] [CrossRef] [PubMed]
- Pouncey, A.L.; David, M.; Morris, R.I.; Ulug, P.; Martin, G.; Bicknell, C.; Powell, J.T. Editor’s Choice–Systematic Review and Meta-Analysis of Sex Specific Differences in Adverse Events after Open and Endovascular Intact Abdominal Aortic Aneurysm Repair: Consistently Worse Outcomes for Women. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 367–378. [Google Scholar] [CrossRef]
- De Freitas, S.; Falls, G.; Weis, T.; Bakhshi, K.; Korepta, L.M.; Bechara, C.F.; Erben, Y.; Arya, S.; Fatima, J. Comprehensive Framework of Factors Accounting for Worse Aortic Aneurysm Outcomes in Females: A Scoping Review. Semin. Vasc. Surg. 2023, 36, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, C.; Freundt, M.; Salem, M.A.; Panholzer, B.; Huenges, K.; Puehler, T.; Cremer, J.; Haneya, A. Sex-Specific Outcome after Ascending Aortic Surgery in Moderate Hypothermic Circulatory Arrest. Thorac. Cardiovasc. Surg. 2021, 69, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Trenner, M.; Kuehnl, A.; Salvermoser, M.; Reutersberg, B.; Geisbuesch, S.; Schmid, V.; Eckstein, H.-H. Editor’s Choice-High Annual Hospital Volume Is Associated with Decreased in Hospital Mortality and Complication Rates Following Treatment of Abdominal Aortic Aneurysms: Secondary Data Analysis of the Nationwide German DRG Statistics from 2005 to 2013. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.; Harky, A.; Fok, M.; Shaw, M.; Hickey, G.L.; Grant, S.W.; Uppal, R.; Oo, A. Acute Type A Aortic Dissection in the United Kingdom: Surgeon Volume-Outcome Relation. J. Thorac. Cardiovasc. Surg. 2017, 154, 398–406.e1. [Google Scholar] [CrossRef]
- Lenos, A.; Bougioukakis, P.; Irimie, V.; Zacher, M.; Diegeler, A.; Urbanski, P.P. Impact of Surgical Experience on Outcome in Surgery of Acute Type A Aortic Dissection. Eur. J. Cardio-Thorac. Surg. 2015, 48, 491–496. [Google Scholar] [CrossRef]
- Stulberg, J.J.; Huang, R.; Kreutzer, L.; Ban, K.; Champagne, B.J.; Steele, S.R.; Johnson, J.K.; Holl, J.L.; Greenberg, C.C.; Bilimoria, K.Y. Association Between Surgeon Technical Skills and Patient Outcomes. JAMA Surg. 2020, 155, 960–968. [Google Scholar] [CrossRef]
- Goodney, P.P.; Travis, L.; Lucas, F.L.; Fillinger, M.F.; Goodman, D.C.; Cronenwett, J.L.; Stone, D.H. Survival after Open versus Endovascular Thoracic Aortic Aneurysm Repair in an Observational Study of the Medicare Population. Circulation 2011, 124, 2661–2669. [Google Scholar] [CrossRef]
- Johansson, G.; Markström, U.; Swedenborg, J. Ruptured Thoracic Aortic Aneurysms: A Study of Incidence and Mortality Rates. J. Vasc. Surg. 1995, 21, 985–988. [Google Scholar] [CrossRef]
- Yiu, R.S.; Cheng, S.W.K. Natural History and Risk Factors for Rupture of Thoracic Aortic Arch Aneurysms. J. Vasc. Surg. 2016, 63, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Dorros, G.; Dorros, A.M.; Planton, S.; O’Hair, D.; Zayed, M. Transseptal Guidewire Stabilization Facilitates Stent-Graft Deployment for Persistent Proximal Ascending Aortic Dissection. J. Endovasc. Ther. 2000, 7, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Regar, E.; Lachat, M.; von Segesser, L.K.; Maisano, F.; Ferrari, E. Endovascular Treatment of Non-Dissected Ascending Aorta Disease: A Systematic Review. Eur. J. Cardio-Thorac. Surg. 2018, 53, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Dakour-Aridi, H.; Yin, K.; Hussain, F.; Locham, S.; Azizzadeh, A.; Malas, M.B. Outcomes of Intact Thoracic Endovascular Aortic Repair in Octogenarians. J. Vasc. Surg. 2021, 74, 882–892.e1. [Google Scholar] [CrossRef]
- Trenner, M.; Eckstein, H.-H.; Kallmayer, M.; Reutersberg, B.; Kühnl, A. Secondary Analysis of Statutorily Collected Routine Data. Gefässchirurgie 2019, 24, 220–227. [Google Scholar] [CrossRef]
- Juraszek, A.; Czerny, M.; Rylski, B. Thoracic Endovascular Aortic Repair: Current Evidence and Challenges. Kardiol. Pol. 2022, 80, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.; Wanhainen, A.; Mani, K.; Kuzniar, M.; Grima, M.; Zuccon, G.; Lindström, D. In Situ Laser Fenestrations of Aortic Endografts for Emergent Aortic Disease. Ann. Vasc. Surg. 2023, 93, 329–337. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male (N = 3036) | Female (N = 1091) | Total (N = 4127) | p-Value | |
|---|---|---|---|---|
| Age, years | 64 (55, 71) | 69 (60, 75) | 65 (56, 72) | <0.001 |
| van Walraven score | 7 (3, 14) | 8 (2, 14) | 7 (3, 14) | 0.411 |
| Coronary artery disease | 1126 (37.1%) | 306 (28.0%) | 1432 (34.7%) | <0.001 |
| Chronic heart failure | 519 (17.1%) | 186 (17.0%) | 705 (17.1%) | 0.972 |
| Cerebrovascular disease | 246 (8.1%) | 80 (7.3%) | 326 (7.9%) | 0.419 |
| Arterial hypertension | 1455 (47.9%) | 543 (49.8%) | 1998 (48.4%) | 0.295 |
| COPD | 333 (11.0%) | 149 (13.7%) | 482 (11.7%) | 0.018 |
| Diabetes mellitus | 240 (7.9%) | 67 (6.1%) | 307 (7.4%) | 0.057 |
| Chronic kidney disease | 304 (10.0%) | 109 (10.0%) | 413 (10.0%) | 0.983 |
| Cancer | 18 (0.6%) | 3 (0.3%) | 21 (0.5%) | 0.206 |
| Obesity | 143 (4.7%) | 67 (6.1%) | 210 (5.1%) | 0.065 |
| Marfan syndrome | 49 (1.6%) | 15 (1.4%) | 64 (1.6%) | 0.584 |
| Level of care | 0.372 | |||
| University Hospital | 1690 (55.7%) | 587 (53.8%) | 2277 (55.2%) | |
| Major Hospital | 922 (30.4%) | 334 (30.6%) | 1256 (30.4%) | |
| Other | 424 (14.0%) | 170 (15.6%) | 594 (14.4%) | |
| Location before admission | 0.344 | |||
| Home | 2832 (93.3%) | 1016 (93.1%) | 3848 (93.2%) | |
| Nursing home | 3 (0.1%) | 1 (0.1%) | 4 (0.1%) | |
| Other | 30 (1.0%) | 5 (0.5%) | 35 (0.8%) | |
| Acute care hospital | 171 (5.6%) | 69 (6.3%) | 240 (5.8%) | |
| Treatment period | 0.921 | |||
| 2009–2013 | 1464 (48.2%) | 528 (48.4%) | 1992 (48.3%) | |
| 2014–2018 | 1572 (51.8%) | 563 (51.6%) | 2135 (51.7%) |
| Male (N = 74) | Female (N = 34) | Total (N = 108) | p-Value | |
|---|---|---|---|---|
| Age, years | 65 (52, 75) | 73 (68, 78) | 69 (54, 75) | 0.012 |
| van Walraven score | 13 (3, 20) | 12 (3, 16) | 13 (3, 19) | 0.540 |
| Coronary artery disease | 17 (23.0%) | 7 (20.6%) | 24 (22.2%) | 0.782 |
| Chronic heart failure | 8 (10.8%) | 6 (17.6%) | 14 (13.0%) | 0.326 |
| Cerebrovascular disease | 14 (18.9%) | 6 (17.6%) | 20 (18.5%) | 0.874 |
| Arterial hypertension | 30 (40.5%) | 17 (50.0%) | 47 (43.5%) | 0.357 |
| COPD | 7 (9.5%) | 4 (11.8%) | 11 (10.2%) | 0.713 |
| Diabetes mellitus | 2 (2.7%) | 4 (11.8%) | 6 (5.6%) | 0.056 |
| Chronic kidney disease | 9 (12.2%) | 0 (0.0%) | 9 (8.3%) | 0.034 |
| Cancer | 1 (1.4%) | 0 (0.0%) | 1 (0.9%) | 0.496 |
| Obesity | 1 (1.4%) | 0 (0.0%) | 1 (0.9%) | 0.496 |
| Marfan syndrome | 1 (1.4%) | 1 (2.9%) | 2 (1.9%) | 0.569 |
| Level of care | 0.680 | |||
| University hospital | 50 (67.6%) | 22 (64.7%) | 72 (66.7%) | |
| Major hospital | 19 (25.7%) | 8 (23.5%) | 27 (25.0%) | |
| Other | 5 (6.8%) | 4 (11.8%) | 9 (8.3%) | |
| Location before admission | 0.821 | |||
| Home | 42 (56.8%) | 19 (55.9%) | 61 (56.5%) | |
| Nursing home | 0 (0.0%) | 1 (2.9%) | 1 (0.9%) | |
| Acute care hospital | 32 (43.2%) | 14 (41.2%) | 46 (42.6%) | |
| Treatment period | 0.420 | |||
| 2009–2013 | 33 (44.6%) | 18 (52.9%) | 51 (47.2%) | |
| 2014–2018 | 41 (55.4%) | 16 (47.1%) | 57 (52.8%) |
| Male (N = 3036) | Female (N = 1091) | Total (N = 4127) | p-Value | |
|---|---|---|---|---|
| Aortic valve management | 0.003 | |||
| No replacement | 2540 (83.7%) | 956 (87.6%) | 3496 (84.7%) | |
| Valve replaced, allograft | 2 (0.1%) | 0 (0.0%) | 2 (0.0%) | |
| Valve replaced, mechanical | 58 (1.9%) | 15 (1.4%) | 73 (1.8%) | |
| Valve replaced, biological | 284 (9.4%) | 94 (8.6%) | 378 (9.2%) | |
| Composite graft, biological | 116 (3.8%) | 23 (2.1%) | 139 (3.4%) | |
| Composite graft, mechanical | 36 (1.2%) | 3 (0.3%) | 39 (0.9%) | |
| Hybrid procedure | 19 (0.6%) | 11 (1.0%) | 30 (0.7%) | 0.202 |
| Length of Ssay ICU, hours | 26 (21, 58) | 29 (22, 68) | 27 (21, 62) | 0.004 |
| Length of stay (swissdrg), days | 10 (9, 14) | 11 (9, 15) | 11 (9, 14) | < 0.001 |
| Packed red blood cells | < 0.001 | |||
| 0 | 2208 (72.7%) | 620 (56.8%) | 2828 (68.5%) | |
| 1–5 | 639 (21.0%) | 383 (35.1%) | 1022 (24.8%) | |
| >5 | 189 (6.2%) | 88 (8.1%) | 277 (6.7%) | |
| Fresh frozen plasma | 0.052 | |||
| 0 | 2877 (94.8%) | 1034 (94.8%) | 3911 (94.8%) | |
| 1–5 | 107 (3.5%) | 48 (4.4%) | 155 (3.8%) | |
| >5 | 52 (1.7%) | 9 (0.8%) | 61 (1.5%) | |
| Platelet concentrate | 0.050 | |||
| 0 | 2940 (96.8%) | 1072 (98.3%) | 4012 (97.2%) | |
| 1–5 | 91 (3.0%) | 18 (1.6%) | 109 (2.6%) | |
| >5 | 5 (0.2%) | 1 (0.1%) | 6 (0.1%) | |
| Complications | ||||
| Myocardial infarction | 46 (1.5%) | 15 (1.4%) | 61 (1.5%) | 0.742 |
| Acute stroke | 58 (1.9%) | 11 (1.0%) | 69 (1.7%) | 0.046 |
| Acute paraplegia | 3 (0.1%) | 2 (0.2%) | 5 (0.1%) | 0.491 |
| Acute renal failure | 2 (0.1%) | 2 (0.2%) | 4 (0.1%) | 0.285 |
| CVVHD | 71 (2.3%) | 25 (2.3%) | 96 (2.3%) | 0.929 |
| Acute mesenteric ischemia | 6 (0.2%) | 4 (0.4%) | 10 (0.2%) | 0.330 |
| Large bowl resection | 4 (0.1%) | 1 (0.1%) | 5 (0.1%) | 0.744 |
| Small bowl resection | 3 (0.1%) | 2 (0.2%) | 5 (0.1%) | 0.491 |
| Acute limb ischemia | 15 (0.5%) | 20 (1.8%) | 35 (0.8%) | < 0.001 |
| Crural fasciotomy | 3 (0.1%) | 2 (0.2%) | 5 (0.1%) | 0.491 |
| Amputation | 1 (0.0%) | 0 (0.0%) | 1 (0.0%) | 0.549 |
| Destination after discharge | < 0.001 | |||
| Home | 1098 (36.2%) | 313 (28.7%) | 1411 (34.2%) | |
| Nursing home | 10 (0.3%) | 3 (0.3%) | 13 (0.3%) | |
| Other | 18 (0.6%) | 5 (0.5%) | 23 (0.6%) | |
| Rehabilitation | 1712 (56.4%) | 663 (60.8%) | 2375 (57.5%) | |
| Acute care hospital | 148 (4.9%) | 76 (7.0%) | 224 (5.4%) | |
| Deseased | 50 (1.6%) | 31 (2.8%) | 81 (2.0%) | |
| Hospital Mortality | 50 (1.6%) | 31 (2.8%) | 81 (2.0%) | 0.015 |
| Male (N = 74) | Female (N = 34) | Total (N = 108) | p-Value | |
|---|---|---|---|---|
| Aortic valve management | 0.485 | |||
| No replacement | 66 (89.2%) | 32 (94.1%) | 98 (90.7%) | |
| Valve replaced, mechanical | 1 (1.4%) | 0 (0.0%) | 1 (0.9%) | |
| Valve replaced, biological | 4 (5.4%) | 0 (0.0%) | 4 (3.7%) | |
| Composite graft, biological | 2 (2.7%) | 2 (5.9%) | 4 (3.7%) | |
| Composite graft, mechanical | 1 (1.4%) | 0 (0.0%) | 1 (0.9%) | |
| Hybrid procedure | 1 (1.4%) | 0 (0.0%) | 1 (0.9%) | 0.496 |
| Length of stay ICU, hours | 55 (20, 132) | 58 (20, 142) | 58 (20, 137) | 0.924 |
| Length of stay (swissdrg), days | 11 (8, 17) | 15 (8, 20) | 12 (8, 19) | 0.240 |
| Transfusion Ec | 0.444 | |||
| 0 | 33 (44.6%) | 11 (32.4%) | 44 (40.7%) | |
| 1–5 | 21 (28.4%) | 13 (38.2%) | 34 (31.5%) | |
| >5 | 20 (27.0%) | 10 (29.4%) | 30 (27.8%) | |
| Transfusion FFP | 0.223 | |||
| 0 | 64 (86.5%) | 33 (97.1%) | 97 (89.8%) | |
| 1–5 | 7 (9.5%) | 1 (2.9%) | 8 (7.4%) | |
| >5 | 3 (4.1%) | 0 (0.0%) | 3 (2.8%) | |
| Transfusion Tc | 0.667 | |||
| 0 | 67 (90.5%) | 30 (88.2%) | 97 (89.8%) | |
| 1–5 | 6 (8.1%) | 4 (11.8%) | 10 (9.3%) | |
| >5 | 1 (1.4%) | 0 (0.0%) | 1 (0.9%) | |
| Complications | ||||
| Myocardial infarction | 1 (1.4%) | 1 (2.9%) | 2 (1.9%) | 0.569 |
| Acute stroke | 1 (1.4%) | 1 (2.9%) | 2 (1.9%) | 0.569 |
| Acute paraplegia | 0 | 0 | 0 | n.a. |
| Acute renal failure | 1 (1.4%) | 0 (0.0%) | 1 (0.9%) | 0.496 |
| CVVHD | 2 (2.7%) | 2 (5.9%) | 4 (3.7%) | 0.416 |
| Acute mesenteric ischemia | 4 (5.4%) | 2 (5.9%) | 6 (5.6%) | 0.920 |
| Large bowl resection | 2 (2.7%) | 0 (0.0%) | 2 (1.9%) | 0.333 |
| Small bowl resection | 2 (2.7%) | 0 (0.0%) | 2 (1.9%) | 0.333 |
| Acute limb ischemia | 5 (6.8%) | 0 (0.0%) | 5 (4.6%) | 0.121 |
| Crural fasciotomy | 0 | 0 | 0 | n.a. |
| Amputation | 0 | 0 | 0 | n.a. |
| Destination after discharge | 0.205 | |||
| Home | 14 (18.9%) | 3 (8.8%) | 17 (15.7%) | |
| Rehabilitation | 27 (36.5%) | 19 (55.9%) | 46 (42.6%) | |
| Acute care hospital | 18 (24.3%) | 5 (14.7%) | 23 (21.3%) | |
| Deseased | 15 (20.3%) | 7 (20.6%) | 22 (20.4%) | |
| Hospital Mortality | 15 (20.3%) | 7 (20.6%) | 22 (20.4%) | 0.970 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menges, A.-L.; Zimmermann, A.; Stoklasa, K.; Reitnauer, D.; Meuli, L.; Reutersberg, B. Hospital Incidence, Sex Disparities, and Perioperative Mortality in Open Surgically Treated Patients with Aneurysms of the Ascending Aorta and Aortic Arch in Switzerland. Healthcare 2024, 12, 388. https://doi.org/10.3390/healthcare12030388
Menges A-L, Zimmermann A, Stoklasa K, Reitnauer D, Meuli L, Reutersberg B. Hospital Incidence, Sex Disparities, and Perioperative Mortality in Open Surgically Treated Patients with Aneurysms of the Ascending Aorta and Aortic Arch in Switzerland. Healthcare. 2024; 12(3):388. https://doi.org/10.3390/healthcare12030388
Chicago/Turabian StyleMenges, Anna-Leonie, Alexander Zimmermann, Kerstin Stoklasa, Daniela Reitnauer, Lorenz Meuli, and Benedikt Reutersberg. 2024. "Hospital Incidence, Sex Disparities, and Perioperative Mortality in Open Surgically Treated Patients with Aneurysms of the Ascending Aorta and Aortic Arch in Switzerland" Healthcare 12, no. 3: 388. https://doi.org/10.3390/healthcare12030388
APA StyleMenges, A.-L., Zimmermann, A., Stoklasa, K., Reitnauer, D., Meuli, L., & Reutersberg, B. (2024). Hospital Incidence, Sex Disparities, and Perioperative Mortality in Open Surgically Treated Patients with Aneurysms of the Ascending Aorta and Aortic Arch in Switzerland. Healthcare, 12(3), 388. https://doi.org/10.3390/healthcare12030388