
Assessment, Treatment, and Follow-Up of Phlebitis Related to Peripheral Venous Catheterisation: A Delphi Study in Spain

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
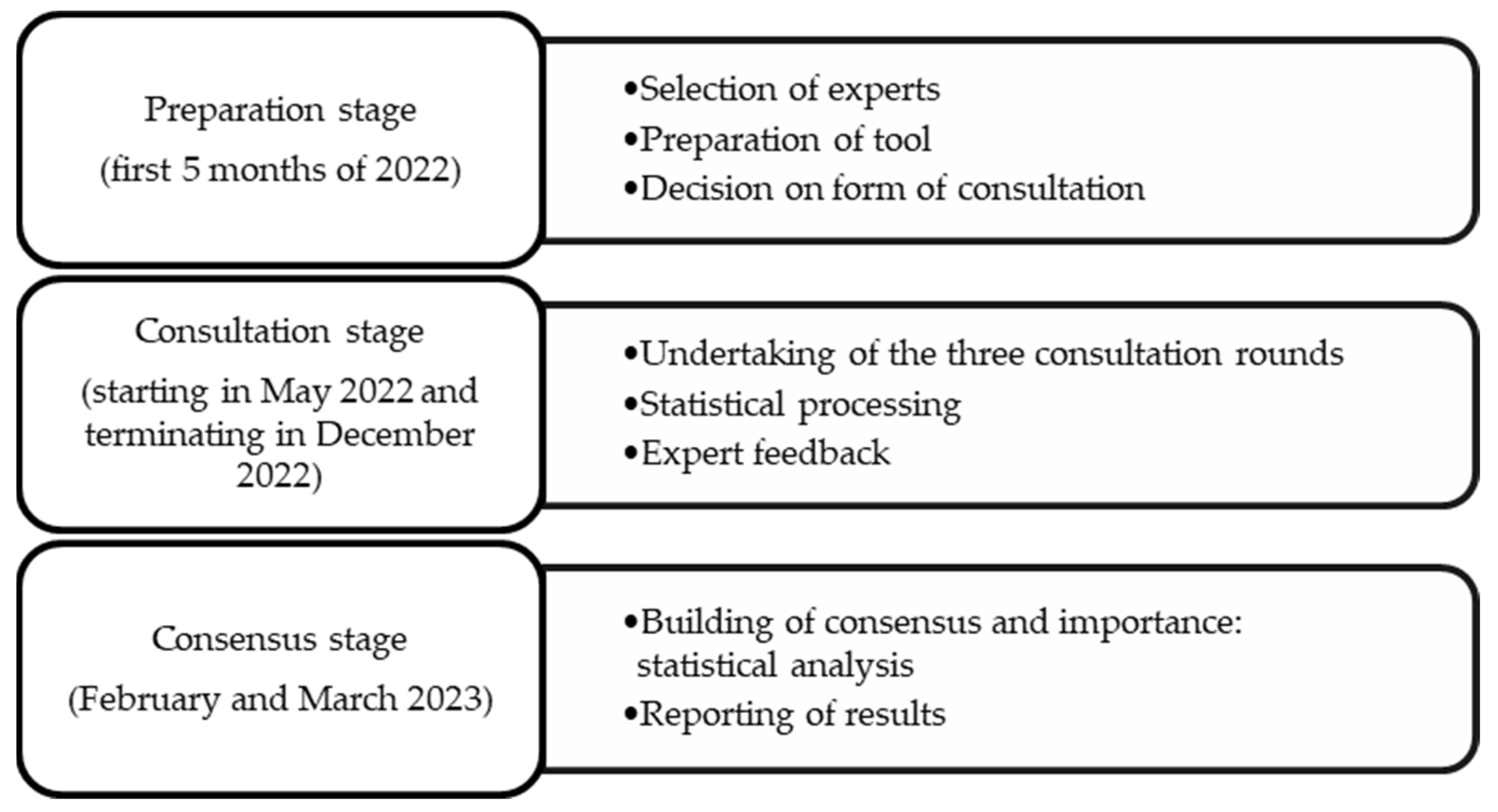
2.2. Stages and Tools
2.3. Preparation Stage: Selection of Experts
- Clinical nursing with practical experience in the field of intravenous therapy. Expertise was established on the basis of at least 10 years of nursing experience and professional practice in a second- or third-level hospital (without differentiating between hospital units). Second-level hospitals offer general care services and some specialist services of generally lower complexity. Third-level hospitals offer a full range of specialist care. The hospitals could be public, fully private, or private state-contracted hospitals.
- Participation in national projects such as Phlebitis Zero. This Spanish national project promotes the use of standardised interventions to stop phlebitis (http://flebitiszero.com/app/ (accessed on 15 March 2022)).
- Currently working in a second- or third-level hospital in Spain.
2.4. Preparation Stage: Preparation of Tool
- ASSESSMENT: How do you assess the degree of phlebitis associated with an upper extremity venous catheter in a patient?
- TREATMENT: What treatment do you apply in the event of PVC-related phlebitis?
- FOLLOW-UP: What follow-up activities are established?
2.5. Consultation Stage and Data Collection
- In round 1, participants were asked to answer the three open-ended questions on the three dimensions (assessment, treatment, and follow-up) with regard to PVC-related phlebitis.
- In round 2, the results of the first consultation (i.e., the responses and their frequency) were incorporated, and the same participants were asked to express their agreement or otherwise with each response item (with a YES or NO) and rate its importance using a 5-point Likert scale: None (0), Little (1), Neutral (2), Quite (3), and Very (4). All responses were included for evaluation.
- In round 3, the results of the second round were presented to the same group: the percentages (%) of ‘agreement’, and the mean (M) and standard deviation (SD) values of ‘importance’. The experts were then asked to prioritise the importance by ranking the response items of each dimension numerically from 1 (least important) to the maximum number possible (which varied according to the number of response items in each dimension). In other words, the highest score was given to the most important item. To analyse these data, the mean and SD of the inverted ranking values were calculated, and finally, the coefficient of variation (CV) was calculated.
2.6. Consensus Stage: Statistical Analysis
2.7. Methodological Quality of the Study
2.8. Ethical Considerations
3. Results
3.1. Participant Characteristics by Round
3.2. Results by Round
4. Discussion
4.1. Assessment Dimension
4.2. Treatment Dimension
4.3. Follow-Up Dimension
4.4. Limitations of the Study
4.5. Implications for Clinical Practice and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Almirante, B. Diagnóstico y Tratamiento de Las Bacteriemias Asociadas Con El Uso de Los Catéteres Vasculares: Que Aporta Una Nueva Guía de Práctica Clínica. Med. Intensiv. 2018, 42, 1–4. [Google Scholar] [CrossRef]
- Sociedad Española Medicina Preventiva Salud Pública y Gestión sanitaria. Prevalencia de infecciones (relacionadas con la asistencia sanitaria y comunitaria) y uso de antimicrobianos en hospitales de agudo. Estudio EPINE-EPPS 2022, 32, 6–92. [Google Scholar]
- Yadav, C.; Samuel, G.; Bano, H.; Mol, S.; Jaiswal, P.; Sootrakar, R.; Singh, S.; Shukla, P. Effectiveness of Alovera, Glycerin, and Cold Application on Superficial Thrombophlebitis among Patients. Int. J. Bioassays 2016, 5, 4858. [Google Scholar] [CrossRef]
- Guanche-Sicilia, A.; Sánchez-Gómez, M.B.; Castro-Peraza, M.E.; Rodríguez-Gómez, J.Á.; Gómez-Salgado, J.; Duarte-Clíments, G. Prevention and Treatment of Phlebitis Secondary to the Insertion of a Peripheral Venous Catheter: A Scoping Review from a Nursing Perspective. Healthcare 2021, 9, 611. [Google Scholar] [CrossRef]
- Pittiruti, M.; Van Boxtel, T.; Scoppettuolo, G.; Carr, P.; Konstantinou, E.; Ortiz Miluy, G.; Lamperti, M.; Goossens, G.A.; Simcock, L.; Dupont, C.; et al. European Recommendations on the Proper Indication and Use of Peripheral Venous Access Devices (the ERPIUP Consensus): A WoCoVA Project. J. Vasc. Access 2023, 24, 165–182. [Google Scholar] [CrossRef]
- Garcia-Expósito, J.; Masot, O.; Gros, S.; Botigué, T.; Roca, J. Practical View of the Topical Treatment of Peripheral Venous Catheter-related Phlebitis: A Scoping Review. J. Clin. Nurs. 2022, 31, 783–797. [Google Scholar] [CrossRef] [PubMed]
- Atay, S.; Sen, S.; Cukurlu, D. Phlebitis-Related Peripheral Venous Catheterization and the Associated Risk Factors. Niger. J. Clin. Pract. 2018, 21, 827–831. [Google Scholar] [CrossRef] [PubMed]
- Di Nisio, M.; Peinemann, F.; Porreca, E.; Rutjes, A.W. Treatment for Superficial Infusion Thrombophlebitis of the Upper Extremity. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Murayama, R.; Abe-Doi, M.; Miyahara-Kaneko, M.; Kanno, C.; Nakamura, M.; Mizuno, M.; Komiyama, C.; Sanada, H. Preventing Peripheral Intravenous Catheter Failure by Reducing Mechanical Irritation. Sci. Rep. 2020, 10, 1550. [Google Scholar] [CrossRef]
- Milutinović, D.; Simin, D.; Zec, D. Risk Factor for Phlebitis: A Questionnaire Study of Nurses’ Perception. Rev. Lat. Am. Enfermagem 2015, 23, 677–684. [Google Scholar] [CrossRef]
- Ray-Barruel, G.; Polit, D.F.; Murfield, J.E.; Rickard, C.M. Infusion Phlebitis Assessment Measures: A Systematic Review. J. Eval. Clin. Pract. 2014, 20, 191–202. [Google Scholar] [CrossRef]
- Gorski, L.A.; Hadaway, L.; Hagle, M.E.; Broadhurst, D.; Clare, S.; Kleidon, T.; Meyer, B.M.; Nickel, B.; Rowley, S.; Sharpe, E.; et al. Infusion Therapy Standards of Practice, 8th Edition. J. Infus. Nurs. 2021, 44, S1–S224. [Google Scholar] [CrossRef]
- Shamloo, M.B.B.; Nasiri, M.; Maneiy, M.; Dorchin, M.; Mojab, F.; Bahrami, H.; Naseri, M.S.; Kiarsi, M. Effects of Topical Sesame (Sesamum Indicum) Oil on the Pain Severity of Chemotherapy-Induced Phlebitis in Patients with Colorectal Cancer: A Randomized Controlled Trial. Complement. Ther. Clin. Pract. 2019, 35, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Goulart, C.B.; Custódio, C.S.; Vasques, C.I.; Ferreira, E.B.; Diniz Dos Reis, P.E. Effectiveness of Topical Interventions to Prevent or Treat Intravenous Therapy-related Phlebitis: A Systematic Review. J. Clin. Nurs. 2020, 29, 2138–2149. [Google Scholar] [CrossRef]
- Braga, L.M.; Salgueiro-Oliveira, A.d.S.; Henriques, M.A.P.; Arreguy-Sena, C.; Albergaria, V.M.P.; Parreira, P.M.d.S.D. Perpipheral Venipuncture: Comprehension and Evaluation of Nursing Practices. Enfermagem 2019. [Google Scholar] [CrossRef]
- García-Expósito, J.; Reguant, M.; Canet-Vélez, O.; Ruiz Mata, F.; Botigué, T.; Roca, J. Evidence of Learning on the Insertion and Care of Peripheral Venous Catheters in Nursing Students: A Mixed Study. Nurse Educ. Today 2021, 107, 105157. [Google Scholar] [CrossRef]
- Reguant Alvarez, M.; Torrado Fonseca, M. El Método Delphi. REIRE Rev. Innov. Recer. En Educ. 2016, 9, 87–102. [Google Scholar] [CrossRef]
- González-García, A.; Díez-Fernández, A.; Martín-Espinosa, N.; Pozuelo-Carrascosa, D.P.; Mirón-González, R.; Solera-Martínez, M. Barriers and Facilitators Perceived by Spanish Experts Concerning Nursing Research: A Delphi Study. Int. J. Environ. Res. Public. Health 2020, 17, 3224. [Google Scholar] [CrossRef] [PubMed]
- Landeta, J.; Lertxundi, A. Quality Indicators for Delphi Studies. Futures Foresight Sci. 2023. [Google Scholar] [CrossRef]
- Spranger, J.; Homberg, A.; Sonnberger, M.; Niederberger, M. Reporting Guidelines for Delphi Techniques in Health Sciences: A Methodological Review. Z. Für Evidenz Fortbild. Qual. Im Gesundheitswesen 2022, 172, 1–11. [Google Scholar] [CrossRef]
- Valdés, M.G.; Marín, M.S. El Método Delphi Para La Consulta a Expertos En La Investigación Científica. Rev. Cuba. Salud Pública 2012, 39, 253–267. [Google Scholar]
- Martínez-Jaimez, P.; Fuster Linares, P.; Piller, N.; Masia, J.; Yamamoto, T.; López-Montoya, L.; Monforte-Royo, C. Multidisciplinary Preventive Intervention for Breast Cancer-related Lymphedema: An International Consensus. Eur. J. Cancer Care 2022, 31, e13704. [Google Scholar] [CrossRef]
- Niederberger, M.; Köberich, S. Coming to Consensus: The Delphi Technique. Eur. J. Cardiovasc. Nurs. 2021, 20, 692–695. [Google Scholar] [CrossRef]
- Tomás Sábado, J. Fundamentos de Bioestadística y Análisis de Datos para Enfermería; Universidad Autònoma de Barcelona: Bellaterra, Spain, 2009; ISBN 978-84-490-2616-4. [Google Scholar]
- Ruiz Díaz, M.Á.; Pardo Merino, A.; San Martín Castellanos, R. Análisis de Datos en Ciencias Sociales y de la Salud I, 2nd ed.; Sintesis: Madrid, Spain, 2021; ISBN 978-84-9756-647-6. [Google Scholar]
- Morrow, S.L. Quality and Trustworthiness in Qualitative Research in Counseling Psychology. J. Couns. Psychol. 2005, 52, 250–260. [Google Scholar] [CrossRef]
- Steel, M.; Seaton, P.; Christie, D.; Dallas, J.; Absalom, I. Nurse Perspectives of Nurse-Sensitive Indicators for Positive Patient Outcomes: A Delphi Study. Collegian 2021, 28, 145–156. [Google Scholar] [CrossRef]
- Marsh, N.; Mihala, G.; Ray-Barruel, G.; Webster, J.; Wallis, M.C.; Rickard, C.M. Inter-Rater Agreement on PIVC-Associated Phlebitis Signs, Symptoms and Scales: Inter-Rater Agreement on Phlebitis. J. Eval. Clin. Pract. 2015, 21, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.C.; Su, L.T.; Liu, Y.C.; Chang, H.Y.; Ou-Yang, M.C.; Chung, M.Y.; Chen, F.S.; Chen, C.C.; Chen, I.L. The Role of Ultrasonography for Detecting Tip Location of Percutaneous Central Venous Catheters in Neonates—A Single-Center, Prospective Cohort Study. Pediatr. Neonatol. 2021, 62, 265–270. [Google Scholar] [CrossRef]
- Hidayah, N.; Rahman, T.A.; Salmarini, D.D. Effect of Warm Water Compress Therapy on the Incidence of Hyperemia in Phlebitis Patients at the Inpatient Eard of Brigjend H. Hasan Basri General Hospital Kandangan. Berk. Kedokt. 2017, 13, 131. [Google Scholar] [CrossRef]
- Wan, Y. Observation for Clinical Effect of Phellodendron Wet Compress in Treating the Phlebitis Caused by Infusion. Pak. J. Pharm. Sci. 2018, 31, 1099–1102. [Google Scholar] [PubMed]
- Zheng, G.H.; Yang, L.; Chen, H.Y.; Chu, J.F.; Mei, L. Aloe Vera for Prevention and Treatment of Infusion Phlebitis. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed]
- Mihala, G.; Ray-Barruel, G.; Chopra, V.; Webster, J.; Wallis, M.; Marsh, N.; McGrail, M.; Rickard, C.M. Phlebitis Signs and Symptoms with Peripheral Intravenous Catheters: Incidence and Correlation Study. J. Infus. Nurs. 2018, 41, 260–263. [Google Scholar] [CrossRef]
- Marsh, N.; Webster, J.; Ullman, A.J.; Mihala, G.; Cooke, M.; Chopra, V.; Rickard, C.M. Peripheral Intravenous Catheter Non-infectious Complications in Adults: A Systematic Review and Meta-analysis. J. Adv. Nurs. 2020, 76, 3346–3362. [Google Scholar] [CrossRef]
- Ogston-Tuck, S. Patient Safety and Pain in IV Therapy. Br. J. Nurs. 2014, 23, S10–S11. [Google Scholar] [CrossRef]
- Whitney, R.; Langhan, M. Vascular Access in Pediatric Patients in the Emergency Department: Types of Access, Indications, and Complications. Pediatr. Emerg. Med. Pract. 2017, 14, 1–20. [Google Scholar]
- Simin, D.; Milutinović, D.; Turkulov, V.; Brkić, S. Incidence, Severity and Risk Factors of Peripheral Intravenous Cannula-induced Complications: An Observational Prospective Study. J. Clin. Nurs. 2019, 28, 1585–1599. [Google Scholar] [CrossRef]
- Simões, A.M.N.; Vendramim, P.; Pedreira, M.L.G. Risk Factors for Peripheral Intravenous Catheter-Related Phlebitis in Adult Patients. Rev. Esc. Enferm. USP 2022, 56, e20210398. [Google Scholar] [CrossRef]
- Webster, J.; Osborne, S.; Rickard, C.M.; Marsh, N. Clinically-Indicated Replacement versus Routine Replacement of Peripheral Venous Catheters. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Pérez Melgarejo, E. Flebitis Postinfusión En Catéteres Venosos: Una Actualización Del Arte. Horiz. Enferm. 2011, 22, 37–48. [Google Scholar] [CrossRef]
- Annisa, F.; Nurhaeni, N.; Wanda, D. Warm Water Compress as an Alternative for Decreasing the Degree of Phlebitis. Compr. Child Adolesc. Nurs. 2017, 40, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Gauttam, V.K.; Vati, D.J. A Study to Assess and Compare the Effectiveness of Moist Heat Versus Ice Packs Application in Reducing the Signs and Symptoms of Intravenous Cannulation Induced Thrombophlebitis among Patients Admitted in Civil Hospital of Dausa District, Rajasthan. Int. J. Appl. Sci. 2016, 3, 410–423. [Google Scholar] [CrossRef]
- Rukhsana, J.R.; Tamang, E.L.; Kochhar, A. A Quasi-Experimental Study to Assess the Effectiveness of Cold Application versus Glycerin Magnesium Sulphate Application in Relieving Phlebitis among Patients Receiving Intravenous Therapy in a Selected Hospital of Delhi. Res. Rev. J. Surg. 2016, 5, 7–11. [Google Scholar]
- Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Thrombocid Forte FORTE 5 Mg/g Pomada; Agencia Española de Medicamentos y Productos Sanitarios (AEMPS): Madrid, Spain, 2001.
- García-Quintanilla, L.; Otero-Barreiro, M.C.; González-Barcia, M.; Virgós-Lamela, A.; Rodríguez-Prada, M. Estudio de La Utilización, Eficacia y Seguridad de La Solución de Burow En El Tratamiento de La Flebitis. Rev. OFIL·LIAPHAR 2018, 28, 199–202. [Google Scholar]
- Lorenzo Ramírez, M.D.; Navarro Torres, M.; Cases Jordán, C.; Morte Cabistany, C.M.; Peñalva Boronat, E.; Milagro Jiménez, M.E. Propiedades Del Agua de Burow. Rev. Sanit. Investig. 2021, 2, 91. [Google Scholar]
- Babaieasl, F.; Yarandi, H.N.; Saeidzadeh, S.; Kheradmand, M. Comparison of EMLA and Diclofenac on Reduction of Pain and Phlebitis Caused by Peripheral IV Catheter. Home Healthc. Now 2019, 37, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Basu, B.; Kaur, S.; Singh, R.S.; Medhi, B. Comparison of Efficacy, Safety and Pharmaco-economic Evaluation of “Ichthammol Glycerine”, “Heparinoid Preparation” and “Magnesium Sulphate Glycerine” Application on the Reduction of Post Cannulation Phlebitis: A Randomized Observer Blind Clinical Study. Glob. Sci. J. 2017, 5, 142–162. [Google Scholar]
- Parthipan, R. Effectiveness of Ichthammol Glycerin Dressing and Hirudoid Ointment on Infiltration and Phlebitis among Patients with Intravenous Infusion in the Selected Wards of Government Rajaji Hospital, Madurai. Master’s Thesis, College Nursing and Medical College, Madurai, India, 2012. [Google Scholar]
- Thomas, M. Prevalence of Phlebitis and Comparison of the Effectiveness of Topical Ichthammol Glycerin and Heparinoid Application on Phlebitis among Patients on Peripheral Intravenous Therapy. J. Med. Sci. Clin. Res. 2016, 4, 12265–12271. [Google Scholar] [CrossRef]
- Yambem, M.; Madhale, M.; Bagi, D. A Comparative Study to Assess the Effectiveness of Glycerin with Magnesium Sulphate versus Heparin—Benzyl Nicotinate (Thrombophob) Ointment on Management of Thrombophlebitis among Patients Admitted in Intensive Care Units (ICU) of Selected Hospital. Int. J. Sci. Res. 2015, 4, 1458–1461. [Google Scholar]
- Saini, V.; Samra, T.; Ahuja, N.; Sethi, S. A Prospective Randomized Study to Evaluate Safety and Efficacy of Heparin Topical Solution (1000 IU/Ml) Compared to Heparin Topical Gel (200 IU/g) in Prevention of Infusion-Associated Phlebitis. Indian J. Pharmacol. 2018, 50, 344. [Google Scholar] [CrossRef] [PubMed]
- Bernatchez, S.F. Care of Peripheral Venous Catheter Sites: Advantages of Transparent Film Dressings Over Tape and Gauze. J. Assoc. Vasc. Access 2014, 19, 256–261. [Google Scholar] [CrossRef]
- Atay, S.; Kurt, F.Y. Effectiveness of Transparent Film Dressing for Peripheral Intravenous Catheter. J. Vasc. Access 2021, 22, 135–140. [Google Scholar] [CrossRef]
- Marsh, N.; Webster, J.; Mihala, G.; Rickard, C.M. Devices and Dressings to Secure Peripheral Venous Catheters: A Cochrane Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2017, 67, 12–19. [Google Scholar] [CrossRef]
- Simonetti, V.; Comparcini, D.; Miniscalco, D.; Tirabassi, R.; Di Giovanni, P.; Cicolini, G. Assessing Nursing Students’ Knowledge of Evidence-Based Guidelines on the Management of Peripheral Venous Catheters: A Multicentre Cross-Sectional Study. Nurse Educ. Today 2019, 73, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Høvik, L.H.; Gjeilo, K.H.; Lydersen, S.; Solligård, E.; Damås, J.K.; Gustad, L.T. Use of Peripheral Venous Catheters in Two Norwegian Hospitals. Tidsskr. Den Nor. Legeforening 2020. [Google Scholar] [CrossRef]
- Lulie, M.; Tadesse, A.; Tsegaye, T.; Yesuf, T.; Silamsaw, M. Incidence of Peripheral Intravenous Catheter Phlebitis and Its Associated Factors among Patients Admitted to University of Gondar Hospital, Northwest Ethiopia: A Prospective, Observational Study. Thromb. J. 2021, 19, 48. [Google Scholar] [CrossRef] [PubMed]
- Mandal, A.; Raghu, K. Study on Incidence of Phlebitis Following the Use of Pheripheral Intravenous Catheter. J. Fam. Med. Prim. Care 2019, 8, 2827. [Google Scholar] [CrossRef]
- Galen, B.; Baron, S.; Young, S.; Hall, A.; Berger-Spivack, L.; Southern, W. Reducing Peripherally Inserted Central Catheters and Midline Catheters by Training Nurses in Ultrasound-Guided Peripheral Intravenous Catheter Placement. BMJ Qual. Saf. 2020, 29, 245–249. [Google Scholar] [CrossRef]
- Yabunaka, K.; Murayama, R.; Tanabe, H.; Takahashi, T.; Oe, M.; Oya, M.; Fujioka, M.; Sanada, H. Ultrasonographic Classification of Subcutaneous Edema Caused by Infusion via Peripheral Intravenous Catheter. J. Med. Ultrasound 2016, 24, 60–65. [Google Scholar] [CrossRef]

{kind=link}
| Variables | n | % | |
|---|---|---|---|
| Age * | 45.0 | 11.3 | |
| Sex | Male | 3 | 11.1 |
| Female | 24 | 88.9 | |
| Years of experience * | 23.0 | 11.6 | |
| Advanced training (professionals) | Speciality | 8 | 29.6 |
| Master’s | 13 | 48.1 | |
| Postgraduate diploma | 5 | 18.5 | |
| None | 1 | 3.7 | |
| Hospital level (place of work) | Second | 10 | 37 |
| Third | 17 | 63 | |
| Work experience (professionals) | Urology | 1 | 3.7 |
| Infection Unit | 4 | 14.8 | |
| Paediatrics and mother and child healthcare | 3 | 11.1 | |
| Emergency Unit | 4 | 14.8 | |
| Internal Medicine | 3 | 11.1 | |
| Surgical Area | 3 | 11.1 | |
| Rotating shifts | 2 | 7.4 | |
| Intensive Care Unit | 1 | 3.7 | |
| Geriatrics | 3 | 11.1 | |
| Management | 2 | 7.4 | |
| Midwife | 1 | 3.7 | |
| Autonomous Community | Catalonia | 8 | 29.6 |
| Navarre | 2 | 7.4 | |
| Valencian Community | 2 | 7.4 | |
| Principality of Asturias | 3 | 11.3 | |
| Balearic Islands | 1 | 3.7 | |
| Cantabria | 1 | 3.7 | |
| Castilla and León | 2 | 7.4 | |
| Community of Madrid | 2 | 7.4 | |
| Region of Murcia | 1 | 3.7 | |
| Extremadura | 1 | 3.7 | |
| Galicia | 2 | 7.4 | |
| Aragón | 1 | 3.7 | |
| Canary Islands | 1 | 3.7 | |
| Assessment Items | f * | Treatment Items | f | Follow-Up Items | f |
|---|---|---|---|---|---|
| Symptomology (observation) | 25 | Burow’s solution | 27 | General monitoring | 24 |
| Maddox Scale | 23 | Catheter removal | 10 | Monitoring + observation of symptoms | 4 |
| Pain | 13 | Pentosan polysulphate sodium ointment | 6 | None | 4 |
| Erythema | 6 | Burow’s solution + pentosan polysulphate sodium ointment | 3 | Monitoring + temperature control | 2 |
| Reddening | 5 | Pentosan polysulphate sodium ointment + application of cold | 3 | Monitoring of insertion point | 2 |
| Swelling | 5 | Cold compresses | 2 | Monitoring + PVC * change every 72 h | 2 |
| Oedema | 3 | Warm compresses | 1 | Monitoring + pain control | 2 |
| Venous cord | 3 | Non-steroid anti-inflammatories (ointment) | 1 | Monitoring + Doppler ultrasonography | 1 |
| Induration | 3 | Non-steroid anti-inflammatories (oral) | 1 | Monitoring + other measures | 1 |
| Warmth | 2 | Simple cure | 1 | Change PVC and dressing | 1 |
| Irritation | 2 | Elevating the limb | 1 | ||
| Size | 1 | Request PICC * insertion | 1 | ||
| Temperature | 1 | ||||
| Other | 1 | ||||
| Scale + symptomology | 1 |
| Importance | Agree | Importance | Agree | Importance | Agree | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Assessment Items | M * | SD * | Mdn * | (%) | Treatment Items | M | SD | Mdn | (%) | Follow-Up Items | M | SD | Mdn | (%) |
| Maddox scale | 3.4 | 1.2 | 4 | 80 | Catheter removal | 3.8 | 0.64 | 4 | 70 | General monitoring | 3.7 | 0.81 | 4 | 80 |
| Symptomology (observation) | 3.9 | 0.43 | 4 | 56.7 | Burow’s solution | 2.6 | 1.52 | 3 | 63.3 | Monitoring + observation of symptoms | 3.6 | 0.67 | 4 | 50 |
| Pain | 3.3 | 0.92 | 4 | 43.3 | Pentosan polysulphate sodium ointment + application of cold | 2.7 | 1.39 | 3 | 30 | Monitoring of insertion point | 3.8 | 0.54 | 4 | 46.7 |
| Erythema | 3.4 | 0.88 | 4 | 33.3 | Cold compresses | 2.5 | 1.15 | 3 | 20 | Change PVC * and dressing | 2.4 | 1.43 | 2 | 16.7 |
| Venous cord | 3.3 | 1.37 | 4 | 30 | Pentosan polysulphate sodium ointment | 1.8 | 1.49 | 1.5 | 13.3 | Monitoring + PVC change every 72 h | 1.8 | 1.62 | 1 | 13.3 |
| Reddening | 2.9 | 1.25 | 3 | 30 | Burow’s solution + Pentosan polysulphate sodium ointment | 2.2 | 1.49 | 2.5 | 10 | Monitoring + pain control | 3.2 | 0.96 | 3.5 | 10 |
| Induration | 3.2 | 1.35 | 4 | 26.7 | Non-steroid anti-inflammatories (ointment) | 2.1 | 1.35 | 2 | 6.7 | Monitoring + temperature control | 3 | 1.14 | 3 | 10 |
| Temperature | 2.9 | 1.21 | 3 | 23.3 | Non-steroid anti-inflammatories (oral) | 0.6 | 0.88 | 1 | 3.3 | Elevating the limb | 1.7 | 1.55 | 1.5 | 10 |
| Swelling | 2.8 | 1.32 | 3 | 16.7 | Request PICC * insertion | 1.2 | 1.26 | 1 | 10 | |||||
| Oedema | 2.7 | 1.37 | 3 | 16.7 | Monitoring + Doppler ultrasonography | 1.1 | 0.96 | 1 | 6.7 | |||||
| Colour | 2.3 | 1.31 | 2.5 | 16.7 | Monitoring + other measures | 0.9 | 1.24 | 0 | 6.7 | |||||
| Scale + symptomology | 2.2 | 1.87 | 3 | 13.3 | ||||||||||
| Irritation | 1.7 | 1.12 | 1.5 | 3.3 | ||||||||||
| Assessment Item | M * | SD * | CV * (%) | Mdn * | Treatment Item | M | SD | CV (%) | Mdn | Follow-Up Item | M | SD | CV (%) | Mdn |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptomology (observation) | 11.1 | 2.1 | 18 | 12 | Catheter removal | 8.0 | 0.0 | 0 | 8 | Monitoring + temperature control | 5.9 | 1.7 | 28 | 6 |
| Reddening | 7.3 | 2.0 | 27 | 8 | Pentosan polysulphate sodium ointment + application of cold | 5.2 | 1.4 | 26 | 4.5 | Monitoring of insertion point | 7.9 | 2.5 | 31 | 9 |
| Maddox scale | 11.2 | 3.2 | 28 | 12 | Cold compresses | 5.0 | 1.6 | 32 | 6 | Monitoring + observation of symptoms | 8.3 | 2.8 | 33 | 9.5 |
| Induration | 7.7 | 2.2 | 28 | 7 | Pentosan polysulphate sodium ointment | 3.65 | 1.3 | 35 | 4 | Monitoring + pain control | 6.2 | 2.2 | 35 | 6.5 |
| Temperature | 6.0 | 1.8 | 30 | 6 | Burow’s solution | 5.6 | 2.1 | 37 | 7 | Change PVC * and dressing | 6.6 | 2.4 | 36 | 3 |
| Pain | 9.3 | 2.8 | 30 | 10 | Burow’s solution + Pentosan polysulphate sodium ointment | 4.0 | 1.5 | 37 | 3.5 | General monitoring | 7.8 | 3.5 | 44 | 9 |
| Venous cord | 8.7 | 2.7 | 31 | 9 | Non-steroid anti-inflammatories (ointment) | 2.65 | 1.3 | 49 | 2 | Elevating the limb | 4.5 | 2.2 | 48 | 4 |
| Erythema | 7 | 2.5 | 35 | 7 | Non-steroid anti-inflammatories (oral) | 1.8 | 1.4 | 77 | 2 | Request PICC * insertion | 3.7 | 2.3 | 62 | 3 |
| Oedema | 4.8 | 2.2 | 45 | 6 | Monitoring + other measures | 2.6 | 1.7 | 65 | 2 | |||||
| Colour | 4.2 | 2.2 | 52 | 4 | Monitoring + PVC change every 72 h | 4.9 | 3.3 | 67 | 5 | |||||
| Scale + symptomology | 8.1 | 4.6 | 56 | 10 | Monitoring + Doppler ultrasonography | 3.2 | 2.45 | 76 | 2 | |||||
| Swelling | 4.3 | 2.5 | 58 | 5 | ||||||||||
| Irritation | 1.6 | 1.6 | 100 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torné-Ruiz, A.; Reguant, M.; Sanromà-Ortiz, M.; Piriz, M.; Roca, J.; García-Expósito, J. Assessment, Treatment, and Follow-Up of Phlebitis Related to Peripheral Venous Catheterisation: A Delphi Study in Spain. Healthcare 2024, 12, 378. https://doi.org/10.3390/healthcare12030378
Torné-Ruiz A, Reguant M, Sanromà-Ortiz M, Piriz M, Roca J, García-Expósito J. Assessment, Treatment, and Follow-Up of Phlebitis Related to Peripheral Venous Catheterisation: A Delphi Study in Spain. Healthcare. 2024; 12(3):378. https://doi.org/10.3390/healthcare12030378
Chicago/Turabian StyleTorné-Ruiz, Alba, Mercedes Reguant, Montserrat Sanromà-Ortiz, Marta Piriz, Judith Roca, and Judith García-Expósito. 2024. "Assessment, Treatment, and Follow-Up of Phlebitis Related to Peripheral Venous Catheterisation: A Delphi Study in Spain" Healthcare 12, no. 3: 378. https://doi.org/10.3390/healthcare12030378
APA StyleTorné-Ruiz, A., Reguant, M., Sanromà-Ortiz, M., Piriz, M., Roca, J., & García-Expósito, J. (2024). Assessment, Treatment, and Follow-Up of Phlebitis Related to Peripheral Venous Catheterisation: A Delphi Study in Spain. Healthcare, 12(3), 378. https://doi.org/10.3390/healthcare12030378