Listening and Processing Skills in Young School Children with a History of Developmental Phonological Disorder


Abstract
1. Introduction
Aims of the Study
2. Materials and Methods
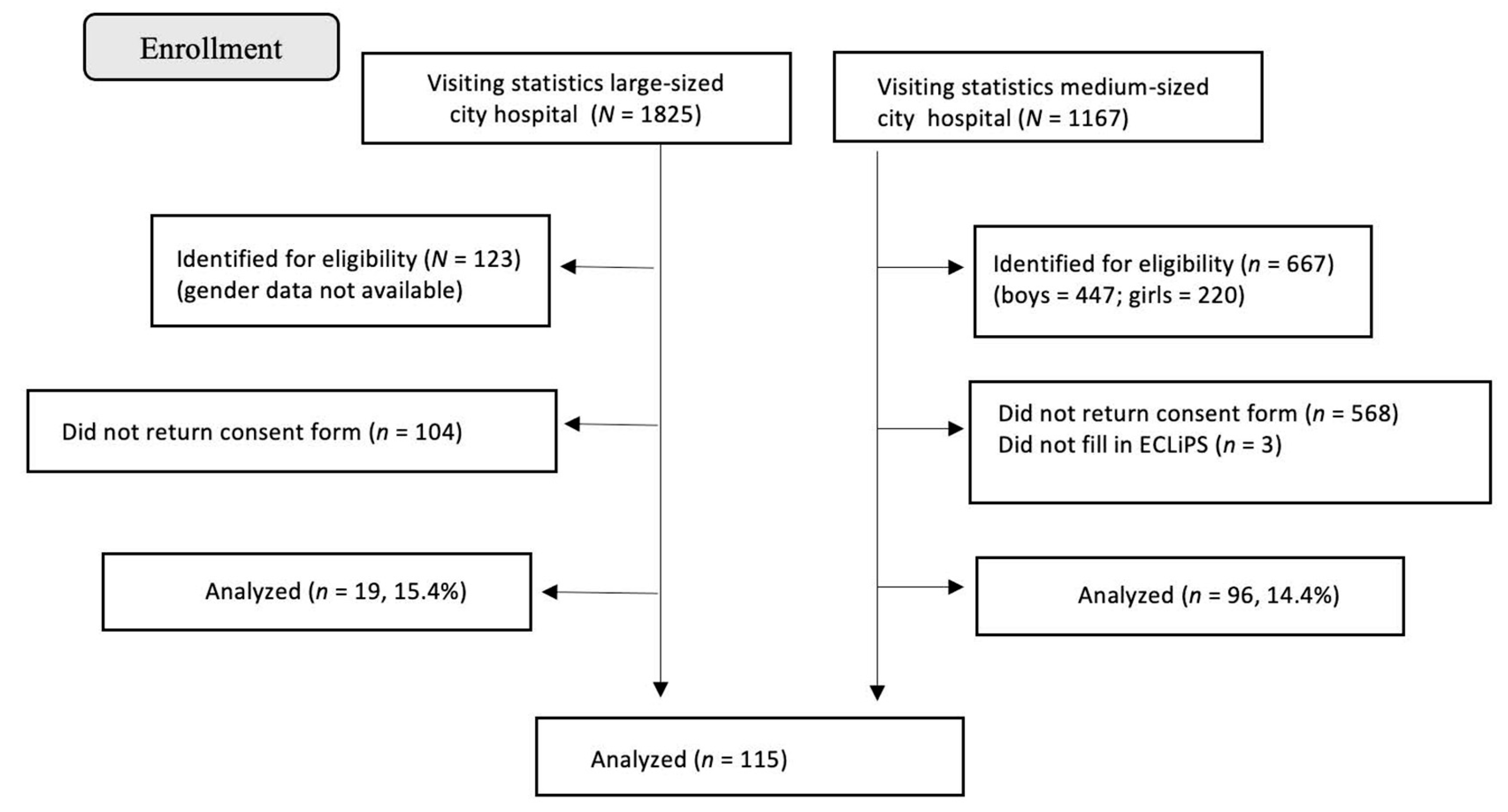
2.1. Participants
2.2. Procedure
2.3. Data Analysis
3. Results
3.1. Total ECLiPS Scores and Subscale Scores
3.2. Proportions of Participants with Clinically Significant Difficulties (≤10th Percentile)
3.3. Co-Occurrence of Subscales with Clinically Significant Difficulties
4. Discussion
4.1. Core Results: Differences with Respect to Overall Mean Scores
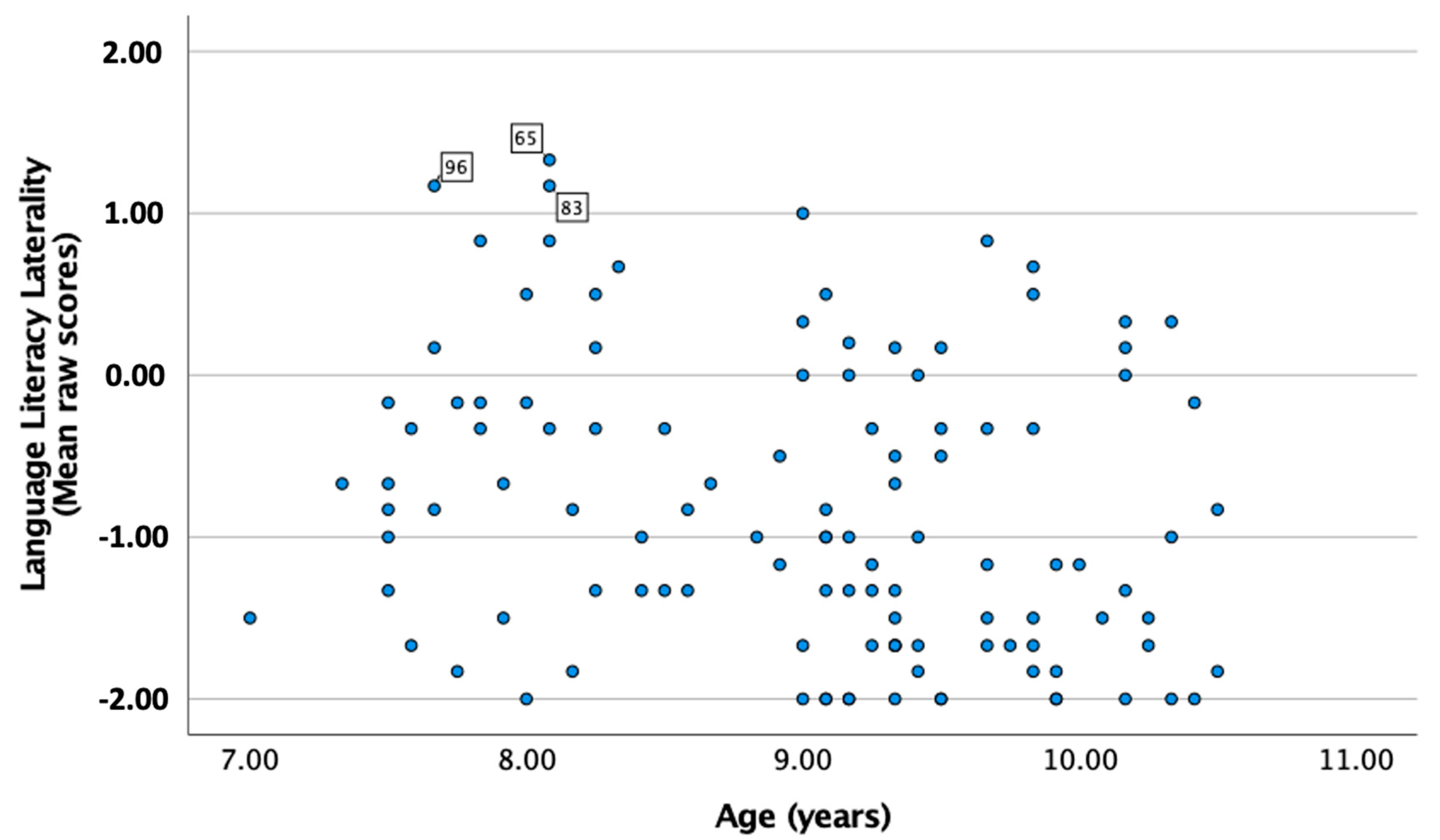
4.2. Associations with Age and Gender Comparisons
4.3. Differences with Respect to Clinically Significant Difficulties
4.4. The Results Regarding Type of Subscales Involved When Below the Cut-Off ≤ 10th Percentile
4.5. Limitations
4.6. Future Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krueger, B.I.; Storkel, H.L. Speech Perception and Spoken Word Recognition; Gaskell, M.G., Mirkovic, J., Eds.; Psychology Press: New York, NY, USA, 2017. [Google Scholar]
- Eadie, P.; Morgan, A.; Ukoumunne, O.C.; Ttofari Eecen, K.; Wake, M.; Reilly, S. Speech sound disorder at 4 years: Prevalence, comorbidities, and predictors in a community cohort of children. Dev. Med. Child Neurol. 2015, 57, 578–584. [Google Scholar] [CrossRef]
- Nakeva von Mentzer, C. Audiometric profiles in children with speech sound disorder: Subclinical hearing loss as a potential factor. Clin. Linguist. Phon. 2020, 35, 847–873. [Google Scholar] [CrossRef]
- Peterson, R.L.; Pennington, B.F.; Shriberg, L.D.; Boada, R. What influences literacy outcome in children with speech sound disorder? J. Speech Lang. Hear. Res. 2009, 52, 1175–1188. [Google Scholar] [CrossRef]
- American Speech-Language-Hearing Association. Speech Sound Disorders: Articulation and Phonology. (Practice Portal). 2023. Available online: www.asha.org/Practice-Portal/Clinical-Topics/Articulation-and-Phonology/ (accessed on 30 January 2024).
- Shriberg, L.D.; Kwiatkowski, J.; Mabie, H.L. Estimates of the prevalence of motor speech disorders in children with idiopathic speech delay. Clin. Linguist. Phon. 2019, 33, 679–706. [Google Scholar] [CrossRef]
- Lohmander, A.; Persson, C. A longitudinal study of speech production in Swedish children with unilateral cleft lip and palate and two-stage palatal repair. Cleft Palate-Craniofacial J. 2008, 45, 32–41. [Google Scholar] [CrossRef]
- Madell, J.R.; Flexer, C. Pediatric Audiology: Diagnosis, Technology, and Management; Thieme Medical Publishers, Inc.: New York, NY, USA, 2019. [Google Scholar]
- Shriberg, L.D.; Tomblin, J.B.; McSweeny, J.L. Prevalence of speech delay in 6-year-old children and comorbidity with language impairment. J. Speech Lang. Hear. Res. 1999, 42, 1461–1481. [Google Scholar] [CrossRef] [PubMed]
- Wren, Y.; McLeod, S.; White, P.; Miller, L.L.; Roulstone, S. Speech characteristics of 8-year-old children: Findings from a prospective population study. J. Commun. Disord. 2013, 46, 53–69. [Google Scholar] [CrossRef]
- McLeod, S.; Harrison, L.J. Epidemiology of speech and language impairment in a nationally representative sample of 4- to 5-year-old children. J. Speech Lang. Hear. Res. 2009, 52, 1213–1229. [Google Scholar] [CrossRef] [PubMed]
- McCormack, J.; McLeod, S.; McAllister, L.; Harrison, L.J. My speech problem, your listening problem, and my frustration: The experience of living with childhood speech impairment. Lang. Speech Hear. Serv. Sch. 2010, 41, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Lohmander, A.; Lundeborg, I.; Persson, C. SVANTE–The Swedish Articulation and Nasality Test–Normative data and a minimum standard set for cross-linguistic comparison. Clin. Linguist. Phon. 2017, 31, 137–154. [Google Scholar] [CrossRef]
- Bleses, D.; Vach, W.; Slott, M.; Wehberg, S.; Thomsen PI, A.; Madsen, T.O.; Basbøll, H. Early vocabulary development in Danish and other languages: A CDI-based comparison. J. Child Lang. 2008, 35, 619–650. [Google Scholar] [CrossRef]
- To CK, S.; McLeod, S.; Sam, K.L.; Law, T. Predicting which children will normalize without intervention for speech sound disorders. J. Speech Lang. Hear. Res. 2022, 65, 1724–1741. [Google Scholar]
- Kalnak, N.; Peyrard-Janvid, M.; Forssberg, H.; Sahlén, B. Nonword repetition--a clinical marker for specific language impairment in Swedish associated with parents’ language-related problems. PLoS ONE 2014, 9, e89544. [Google Scholar] [CrossRef]
- Claessen, M.; Leitão, S. Phonological representations in children with SLI. Child Lang. Teach. Ther. 2012, 28, 211–223. [Google Scholar] [CrossRef]
- Sutherland, D.; Gillon, G.T. Assessment of phonological representations in children with speech impairment. Lang. Speech Hear. Serv. Sch. 2005, 36, 294–307. [Google Scholar] [CrossRef]
- Sutherland, D.; Gillon, G.T. Development of phonological representations and phonological awareness in children with speech impairment. Int. J. Lang. Commun. Disord. 2007, 42, 229–250. [Google Scholar] [CrossRef]
- Elbro, C.; Nielsen, I.; Petersen, D.K. Dyslexia in adults: Evidence for deficits in non-word reading and in the phonological representation of lexical items. Ann. Dyslexia 1994, 44, 203–226. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.; Moore, D. Evaluation of Children’s Listening and Processing Skills, Technical Manual, 2nd ed.; Medical Research Council, Institute of Hearing Research: Nottingham, UK, 2015. [Google Scholar]
- Dillon, H.; Cameron, S. Separating the causes of listening difficulties in children. Ear Hear. 2021, 42, 1097. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Purdy, S.C.; Kelly, A.S. Comorbidity of auditory processing, language, and reading disorders. J. Speech Lang. Hear. Res. 2009, 52, 706–722. [Google Scholar] [CrossRef] [PubMed]
- Petley, L.; Hunter, L.L.; Zadeh, L.M.; Stewart, H.J.; Sloat, N.T.; Perdew, A.; Moore, D.R. Listening difficulties in children with normal audiograms: Relation to hearing and cognition. Ear Hear. 2021, 42, 1640. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.; Tomlin, D.; Moore, D.R.; Dillon, H. Use of Questionnaire-Based Measures in the Assessment of Listening Difficulties in School-Aged Children. Ear Hear. 2015, 36, e300–e313. [Google Scholar] [CrossRef]
- Purdy, J.; Wright, M.; Woodman, J.; Levy, E. Comparison of the Auditory Processing Domains (APDQ) and Evaluation of Children’s Listening and Processing Skills (ECLiPS) Questionnaires. Conference paper. J. Hear. Sci. 2022, 12, 131. [Google Scholar]
- Bishop, D.V.M. The Children’s Communication Checklist-2, 2nd ed.; The Psychological Corporation: London, UK, 2006. [Google Scholar]
- Purdy, S.C.; Smart, J.L.; Baily, M.; Sharma, M. Do children with reading delay benefit from the use of personal FM systems in the classroom? Int. J. Audiol. 2009, 48, 843–852. [Google Scholar] [CrossRef]
- Purdy, S.C.; Kelly, A.S.; Davies, M.G. Auditory brainstem response, middle latency response, and late cortical evoked potentials in children with learning disabilities. J. Am. Acad. Audiol. 2002, 13, 367–382. [Google Scholar] [CrossRef]
- Sharma, M.; Purdy, S. Management of auditory processing disorder for school aged children applying the ICF (International Classification of Functioning, Disability and Health) framework. In Auditory Processing Disorders: Assessment, Management and Treatment; Geffner, D.S., Ross-Swain, D., Eds.; Plural Publishing Inc.: San Diego, CA, USA, 2012; pp. 495–528. [Google Scholar]
- Fisher, L. Fisher’s Auditory Problems Checklist; Life Products: Bemidji, MN, USA, 1976. [Google Scholar]
- Hunter, L.L.; Monson, B.B.; Moore, D.R.; Dhar, S.; Wright, B.A.; Munro, K.J.; Siegel, J.H. Extended high frequency hearing and speech perception implications in adults and children. Hear. Res. 2020, 397, 107922. [Google Scholar] [CrossRef]
- Moore, D.R. Listening difficulties in children: Bottom-up and top-down contributions. J. Commun. Disord. 2012, 45, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, E.; Ohtamaa, L. Listening Difficulties in Children with Developmental Phonological Disorder. A Survey of Parent’s Perception of Their Children’s Listening Difficulties. Master’s Thesis, Uppsala University, Uppsala, Sweden, 2019. [Google Scholar]
- Lewis, B.A.; Freebairn, L. Residual effects of preschool phonology disorders in grade school, adolescence, and adulthood. J. Speech Lang. Hear. Res. 1992, 35, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Lewis, B.A.; Freebairn, L.A.; Taylor, H.G. Academic outcomes in children with histories of speech sound disorders. J. Commun. Disord. 2000, 33, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Kalnak, N.; Peyrard-Janvid, M.; Sahlén, B.; Forssberg, H. Family history interview of a broad phenotype in specific language impairment and matched controls. Genes Brain Behav. 2012, 11, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Nudel, R.; Christensen, R.V.; Kalnak, N.; Schwinn, M.; Banasik, K.; Dinh, K.M.; DBDS Genomic Consortium. Developmental language disorder—A comprehensive study of more than 46,000 individuals. Psychiatry Res. 2023, 323, 115171. [Google Scholar] [CrossRef]
- Whitehouse, A.J. Is there a sex ratio difference in the familial aggregation of specific language impairment? A meta-analysis. J. Speech Lang. Hear. Res. 2010, 53, 1015–1025. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| DPD (n = 115) | TD (n = 46) | p-Value | |
|---|---|---|---|
| Age mean, years, months (range) | 9.0 (7.0–10.5) | 8.5 (7.0–10.6) | 0.003 |
| Female-to-male ratio (%) | 36:79 (31.3:68.7) | 18:28 (39.1:60.9) | 0.342 |
| DPD | TD | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | SD | Min–Max | Mean | Median | SD | Min–Max | p-Value | |
| Total raw score | −1.01 | −1.16 | 0.77 | −2.00–1.46 | −1.22 | −1.26 | 0.50 | −1.97–0.30 | 0.24 |
| SAP | −1.17 | −1.33 | 0.84 | −2.00–1.56 | −1.44 | −1.62 | 0.53 | −2.00–0.22 | 0.19 |
| EAS | −1.17 | −1.63 | 0.98 | −2.00–1.75 | −1.33 | −1.63 | 0.80 | −2.00–1.13 | 0.68 |
| LLL | −0.84 | −1.00 | 0.9 | −2.00–1.33 | −0.99 | −1.17 | 0.83 | −2.00–0.67 | 0.33 |
| PSS | −0.98 | −1.00 | 0.85 | −2.00–2.00 | −1.25 | −1.33 | 0.63 | −2.00–0.17 | 0.09 |
| MA | −0.85 | −0.88 | 0.88 | −2.00–1.13 | −0.97 | −1.00 | 0.67 | −2.00–0.50 | 0.60 |
| DPD % (n) | TD % (n) | χ2 | p-Value | Odds Ratio | |
|---|---|---|---|---|---|
| Total score | 31.3 (36) | 10.9 (5) | 6.5 | 0.01 | 3.0 |
| SAP | 30.0 (31) | 10.9 (5) | 4.2 | 0.04 | 2.8 |
| EAS | 21.7 (25) | 8.7 (4) | * | 0.03 | 2.6 |
| LLL | 36.5 (42) | 30.4 (14) | 0.4 | 0.53 | 1.2 |
| PSS | 16.5 (19) | 4.3 (2) | * | 0.03 | 3.9 |
| MA | 22.6 (26) | 13.0 (6) | 1.5 | 0.22 | 1.8 |
| No of Subscales | DPD % (n) | TD % (n) | χ2 | p-Value | Odds Ratio |
|---|---|---|---|---|---|
| 0 subscales | 51.3 (59) | 56.5 (26) | 0.36 | 0.55 | 0.9 |
| 1 subscale | 14.8 (17) | 34.8 (16) | 8.07 | <0.01 | 0.4 |
| 2 subscales | 13.0 (15) | 4.3 (2) | * | 0.15 | 3.0 |
| 3 subscales | 8.7 (10) | 4.3 (2) | * | 0.51 | 2.0 |
| 4 subscales | 3.5 (4) | 0.0 (0) | * | 0.32 | 3.5 |
| 5 subscales | 8.7 (10) | 2.2 (1) | * | ns | 4.0 |
| Sum of 2 or more | 33.9 (39) | 10.9 (5) | 8.8 | <0.01 | 3.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalnak, N.; Nakeva von Mentzer, C. Listening and Processing Skills in Young School Children with a History of Developmental Phonological Disorder. Healthcare 2024, 12, 359. https://doi.org/10.3390/healthcare12030359
Kalnak N, Nakeva von Mentzer C. Listening and Processing Skills in Young School Children with a History of Developmental Phonological Disorder. Healthcare. 2024; 12(3):359. https://doi.org/10.3390/healthcare12030359
Chicago/Turabian StyleKalnak, Nelli, and Cecilia Nakeva von Mentzer. 2024. "Listening and Processing Skills in Young School Children with a History of Developmental Phonological Disorder" Healthcare 12, no. 3: 359. https://doi.org/10.3390/healthcare12030359
APA StyleKalnak, N., & Nakeva von Mentzer, C. (2024). Listening and Processing Skills in Young School Children with a History of Developmental Phonological Disorder. Healthcare, 12(3), 359. https://doi.org/10.3390/healthcare12030359