Abstract
Promoting subjective well-being is a crucial challenge in aging societies. In 2022, we launched a community-based intervention trial (the Chofu-Digital-Choju Movement). This initiative centered on fostering in-person and online social connections to enhance the subjective well-being of older adults. This paper describes the study design and baseline survey. This quasi-experimental study involved community-dwelling older adults aged 65–84 years in Chofu City, Tokyo, Japan. A self-administered questionnaire was distributed to 3742 residents (1681 men and 2061 women), and a baseline survey was conducted in January 2022. We assessed subjective well-being (primary outcome); psychosocial, physical, and dietary factors; and the use of information and communication technology variables (secondary outcomes) among the participants. After the intervention involving online classes, community hubs, and community events, a 2-year follow-up survey will be conducted to evaluate the effects of the intervention, comparing the intervention group (participants) with the control group (non-participants). We received 2503 questionnaires (66.9% response rate); of these, the analysis included 2343 questionnaires (62.6% valid response rate; mean age, 74.4 (standard deviation, 5.4) years; 43.7% male). The mean subjective well-being score was 7.2 (standard deviation, 1.9). This study will contribute to the development of a prototype subjective well-being strategy for older adults.
1. Introduction
Japan’s demographic landscape has shown notable progression toward an aging society, with the proportion of the population aged ≥65 years estimated to reach 30% by 2025 [1]. Aging is associated with worsening self-rated health status [2], cognitive impairment [3], and various life events such as bereavement [4,5]. Within this context, subjective well-being is a crucial factor in aging. Well-being is defined as the state where individuals realize their abilities, cope with the normal stresses of life, function productively, contribute to their community, and find contentment [6]. Notably, older adults with high levels of subjective well-being tend to exhibit lower risks of frailty and mortality [7,8,9]. Therefore, it has become imperative to maintain and improve the subjective well-being of older adults in aging societies, aiming to extend their healthy lifespans and overall life expectancy.
Social networks are the determinants of higher subjective well-being. Frequent contact with friends, emotionally positive exchanges, enjoyment, and shared good experiences can contribute to an individual’s subjective well-being [10]. Moreover, psychological intervention programs involving social interactions positively affect subjective well-being [11]. There are four key strategies identified by Suragarn et al. for enhancing social connections among older adults: (1) multi-generational programs, (2) aging-friendly communities, (3) group-based physical activity approaches, and (4) the use of information and communication technology (ICT) [12]. Of these, ICT use warrants particular attention because of its indirect influence on well-being by enhancing social capital [13], which is a feature of social organizations such as networks, norms, and social trust that facilitate coordination and cooperation for mutual benefit [14].
While prior community-based interventions aimed at improving the subjective well-being of older adults have been implemented [15,16,17], none have been community-based with ICT use, to the best of our knowledge. In this context, this study aims to assess the effect of a community-based intervention on improving subjective well-being among the older Japanese population. Accordingly, we launched a study project in 2022 and implemented a multi-component intervention based on strategies to create both in-person and online social connections.
In this study, we describe the study design and baseline characteristics of the participants of the intervention launched in 2022.
2. Materials and Method
2.1. Study Design, Study Setting, and Participants
The Chofu-Digital-Choju (CDC; Choju means longevity in Japanese) movement is a quasi-experimental study [18] spanning from January 2022 to March 2024, conducted in collaboration with industry, academia, and the government. The CDC movement aims to foster in-person and online social connections to enhance the subjective well-being of older adults. In January 2022, a survey was conducted by mailing a self-administered questionnaire to collect baseline data for the intervention study. A subsequent follow-up survey, following up on the baseline measurements, is scheduled for a 2-year period.
The study population comprises community-dwelling individuals aged 65–84 years as of 1 October 2022, living independently in two districts of Chofu City, Tokyo, Japan. Individuals older than 85 years were excluded since the response rate that can be employed was extremely low, according to a previous study [19]. These districts were selected through consultation with city and social welfare council employees based on previous surveys and demographic trends. Chofu City, located in the middle of Tokyo (Figure 1), had a population of 238,311 (115,964 men and 122,347 women) as of 1 October 2021, with 51,536 individuals (22,018 men and 29,518 women) aged ≥65 years, constituting 21.6% of older adults [20]. These districts are located in the south and north of the city, where more than half the households reside in apartment buildings and detached houses, respectively [21].
Figure 1.
Geographical locations of the study areas (Chofu City, Tokyo, Japan).
The sample size was determined through several steps, as follows: first, a previous review by Bolier et al. indicated that positive psychology interventions showed an effect size of 0.34 for subjective well-being [22]. To detect this effect using a t-test, 137 individuals were required in both the intervention and control groups (with a statistical power of 0.8 and a risk level of 0.05). Second, based on a previous survey [23], we estimated a dropout rate of approximately 20% over 2 years. Third, the expected valid response rate at baseline and follow-up was approximately 80%, based on previous baseline surveys [19,24]. The percentage of participants required in the intervention group was approximately 10% of the total participants. From these estimates, we calculated a baseline survey sample size of 2675 participants.
Figure 2 illustrates the study flow diagram. The intervention group consists of participants who received the CDC movement’s intervention, while the control group consists of those who did not. During the 2-year follow-up survey, we will ask the participants whether they engaged in any or all of the interventions, including attending online classes, visiting local community interaction hubs, and joining the community events organized by us. Subsequently, the participants who received at least one of these interventions will be categorized into the intervention group in accordance with the responses in the 2-year follow-up survey.
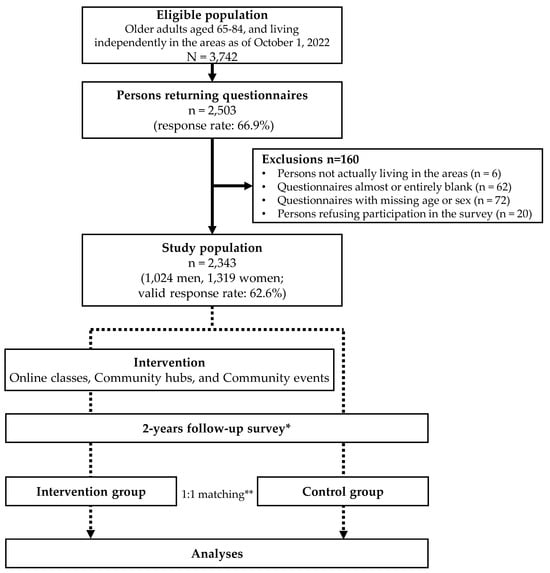
Figure 2.
Study flow diagram. * Participants will be categorized into either the intervention or control group based on their response in the follow-up survey regarding prior participation in any of the interventions. ** Propensity score matching with a ratio of 1:1 between the intervention and control groups will be applied using logistic regression based on the baseline survey.
2.2. Baseline and Follow-Up Surveys
As shown in Table 1, the key measurements included subjective well-being as the primary outcome and psychosocial function, physical activity and function, use of ICT, and dietary habits as the secondary outcomes. As additional measures, demographics, socio-economic status, and medical and lifestyle profiles were collected. The self-administered questionnaire, mirroring the items from the baseline survey, will be distributed to the participants, except those who died or relocated from the study area, during the 2-year follow-up survey.

Table 1.
Summary of the items surveyed at baseline, 2022.
2.3. Primary Outcome Measures
Subjective well-being was assessed using the Cantril Ladder, which evaluates people’s attitudes toward their lives and components in various respects [25]. The scale comprised an 11-level Likert scale ranging from 0 (lowest) to 10 (highest).
2.4. Secondary Outcome Measures
2.4.1. Psychosocial Function
Social isolation was assessed according to the frequency of outings or contact with family members, relatives, and friends. Social isolation was defined as contact with others less than once a week [26]. Neighborhood relationships were assessed using a four-point scale encompassing “visiting each other”, “standing and chatting”, “exchanging of greetings”, or “none [27,28]”. Additionally, social participation was evaluated based on the frequency of participation in the following activities or groups more than once a month: volunteering, civic action, and nonprofit organizations; sports groups; hobbies and learning groups; senior citizen clubs; neighborhood associations; and others [23].
Psychological aspects include health literacy [29], psychological health [30,31], and depressive mood [32,33].
2.4.2. Physical Activity and Physical Function
Exercise habits were defined as engaging in any exercise one or more times a week and recreational walking or walking for transport for 150 min or more a week [34,35]. Physical function was evaluated according to frailty status [36,37], activities of daily living [38], and the Motor Fitness Scale [39].
2.4.3. Dietary Habits
Dietary variety and food frequency scores were used to evaluate dietary variety [40,41]. The participants were also asked about their status of eating alone [42].
2.4.4. Use of ICT
The questionnaire assessed the type of ICT device used weekly or more frequently and the frequency of Internet usage, such as browsing web pages and exchanging e-mails [43,44].
2.5. Intervention Overview
The CDC movement aims to improve the subjective well-being of older adults by creating in-person and online connections. After completing the baseline survey, we will implement the community-based intervention designed by the CDC movement. This intervention consists of online classes, community hubs, and community events.
The online classes integrate an intervention approach combining exercises, nutrition, and cognitive aspects effective in preventing frailty [45]. Additionally, this class employs the Coimagination Method to foster formal conversation techniques aimed at building relationships [46,47]. The exercise component involves workouts designed by professional instructors based on the 10-item muscle training validated in the Japanese Oniishi Model [48,49]. The Oniishi Model’s muscle training is derived from the 19-item regimen by Fiatarone et al. [50] and focuses on fundamental movements such as walking and standing. For safety in an online environment, no specific intensity is designated for the training. The nutrition component, supervised by nutrition experts, includes lectures on diet and food intake for frailty prevention [40]. The lectures center around a mnemonic phrase in Japanese, “sa-a-ni-gi-ya-ka-ni-i-ta-daku” (‘Let’s eat with diversity’), highlighting the importance and techniques of consuming a variety of food groups for frailty prevention [23]. The cognitive aspect involves cognitive enhancement activities led by trainers, such as finger exercises and short-term memory stimulation. The Coimagination Method, designed for equitable participation in communication, comprises two phases, as follows: participants explain their pre-prepared photos and answer questions from others. This process is repeated until all participants have completed both phases. Each session of the online classes focuses on themes such as landscapes, favorite foods, passions, health, and memorable experiences, with facilitation to encourage conversation. Each group, consisting of about ten members, meets once a week for six weeks. The weekly online classes include exercises, nutrition, cognitive aspects, and the Coimagination Method, with participants joining from their homes. Throughout the intervention period, a total of 25 sets of these online classes will be conducted with different participants.
The community hub, serving as a local third place, is operated with the intent of promoting well-being through emotional support provided by volunteers [51,52]. This social interaction center aims to foster trust by listening to and empathizing with the elderly residents of the area. Additionally, it seeks to facilitate social support for older individuals through collaboration with external agencies when necessary [53]. To motivate visits to the hub, health measuring devices are installed, and consultations on smartphone usage are offered. The health measuring devices are capable of assessing or estimating blood pressure, vegetable intake, hemoglobin levels, autonomic nerve function, balance, and cognitive abilities. The hub is open three times a week during the intervention period, with volunteers present during operating hours.
As community events, activities ranging in size from a few to about 30 participants are conducted, being open to all age groups, from youth to the elderly. The themes of these events include general health, exercise, diet, hobbies and entertainment, and the use of ICT such as smartphones. These events are held about four times a month in community centers or university facilities.
2.6. Ethical Considerations
The study protocol was approved by the Ethics Committee of the University of Electro-Communications (approval on 16 December 2021; 21068). All the participants provided informed consent. A statement attached to the questionnaire explained the study’s purpose and the voluntary nature of participation and confirmed that the analysis was anonymous. In addition to consent to participate, returning the questionnaire was viewed as consent to participate. All research data are stored on a dedicated computer disconnected from the Internet, and access is exclusively restricted to the members of the research team.
The trial is registered in the UMIN Clinical Trials Registry (UMIN000051393).
2.7. Statistical Analyses
All data in the baseline survey are presented as means (standard deviations) or proportions, considering sex differences. The main measures were compared between sexes using the chi-square test for nominal variables and Welch’s t-test for continuous variables. A significance level of α = 0.05 indicated statistical significance, and all statistical analyses were performed using IBM SPSS Statistics for Windows, version 29.0 (IBM Corp., Armonk, NY, USA).
As a primary analysis, repeated measures analysis of variance (ANOVA) will be used to verify the interaction between time (pre- and post-intervention) and group (intervention and control groups) to clarify the effect of the interventions on the subjective well-being of older adults after the follow-up survey. In cases where the interaction is significant, a multiple comparison test will be performed using the Bonferroni method. Before ANOVA is performed, propensity score matching with a ratio of 1:1 will be applied using logistic regression based on the baseline survey to reduce bias in background factors between the intervention (participants) and control (non-participants) groups.
A secondary subgroup analysis will be performed to detect differences in the effects of the types of interventions or the intervention frequency on subjective well-being.
3. Results
The self-administered questionnaires were distributed to 3742 eligible participants, from whom data were analyzed from 2503 participants (response rate: 66.9%). After excluding 160 questionnaires, including six from respondents living outside the designated areas, 62 questionnaires that were almost entirely blank, 72 that were missing essential identification labels (age or sex), and 20 from respondents who refused to participate in the survey, the analysis included data from 2343 individuals (1024 men and 1319 women; valid response rate: 62.6%).
Table 2 shows the baseline characteristics of the study population. The mean age was 74.4 (standard deviation, 5.4) years. The mean subjective well-being score was 7.2 (standard deviation, 1.9). Compared with women, men were significantly less likely to live alone; have less musculoskeletal pain; have lower subjective well-being, psychological health, activities of daily living, Dietary Variety Score, and Food Frequency Score; and have lower levels of social activities. Additionally, men were significantly more likely to be employed, socially isolated, and frail; have more current drinking and smoking habits; have higher health literacy and Motor Fitness Scale scores; and use the Internet more frequently.
Table 2.
Baseline characteristics of the participants.
Although physical function deteriorates with aging [54], subjective well-being can be maintained or promoted [22,55,56]. Higher levels of subjective well-being were observed in the participants in this study compared with those in the nationwide survey (the score was 6.2 in 2022) [57]. A previous study revealed that a higher density of older people in certain areas was associated with a higher level of subjective well-being [58]. Although the percentage of the population aged ≥65 years was lower in Chofu City than in Japan as a whole (21.6% vs. 28.9% as of 1 October 2021) [20,59], the participants had higher subjective well-being.
4. Discussion
To the best of our knowledge, the present study describes a unique intervention because it facilitates the formation of online and in-person communities; provides group-based online programs consisting of physical exercise, cognitive training, and nutrition lectures; establishes community hubs with psychological support from volunteers; and organizes multi-generational community events. These attempts to create connections for older adults may extend their healthy life expectancy, mediated by maintaining or promoting subjective well-being.
Previous reviews have indicated that ICT use can reduce loneliness and social isolation [60]; however, older individuals who use the Internet have a higher socioeconomic status than non-users [61]. In this baseline survey, the proportion of older adults using the Internet was lower than that in a national survey in Japan (60.1%) [62]. The promotion of Internet and ICT use through this intervention can allow community-dwelling older adults to obtain its benefits, leading to reduced social isolation.
This study has some limitations. First, the participation rate was not high compared to that in some cohort studies in the baseline survey [19,24,63]. Second, the low proportion of participants using the Internet, compared with a national survey in Japan, can potentially influence the results. Third, the study’s internal validity may have been affected by participants’ recall bias, as a self-administered questionnaire was used. Fourth, although the random selection of participants and the calculation of sample size for interventions would typically be performed, the present study was conducted as a quasi-experimental study. Finally, in this community-based intervention, there is a potential risk of contamination that could affect the accurate assessment of intervention effects, as both the intervention and control groups reside in the same area. Therefore, the fact that all participants belong to the same residential area may affect the results of the study.
The CDC movement was launched in 2022 to create connections to enhance subjective well-being among community-dwelling older adults. A multi-component intervention and the planned 2-year follow-up survey will be implemented. This study is expected to contribute to the development of a prototype strategy to promote the subjective well-being of older adults.
5. Conclusions
The community-based intervention trial (the Chofu-Digital-Choju movement) was launched in 2022 to improve the subjective well-being of community-dwelling older adults by fostering in-person and online connections. The insights of this study could contribute to the development of a prototype subjective well-being strategy for older adults.
Author Contributions
Conceptualization, T.N., T.K., S.S., S.M., M.E., J.S., Y.S., Y.I., M.S., K.T., K.Y., O.M., K.K. and K.O.; methodology, T.N., T.K., S.S., S.M., M.E., J.S., Y.S., S.T., F.K., O.M., K.K. and K.O.; software, K.S. and H.W.; formal analysis, T.N., T.K., S.S., K.K. and K.O.; investigation, T.N., T.K., S.S., O.M., C.K., H.S., K.K. and K.O.; data curation, T.N., T.K., S.S., O.M., C.K., K.K. and K.O.; writing—original draft preparation, T.N., K.K. and K.O.; writing—review and editing, T.N., T.K., S.S., S.M., M.E., J.S., Y.S., S.T., F.K., K.S., H.W., Y.I., M.S., K.T., K.Y., O.M., C.K., H.S., K.K. and K.O.; visualization, T.N., T.K., S.S., K.K. and K.O.; supervision, K.O.; project administration, K.O.; funding acquisition, S.S., O.M., C.K., H.S. and K.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Chofu City who used a Tokyo Metropolitan Government grant; JST SPRING, Grant Number: JPMJSP2131.
Institutional Review Board Statement
The study protocol was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Electro-Communications (approval on 16 December 2021; 21068). The trial is registered in the UMIN Clinical Trials Registry (UMIN000051393).
Informed Consent Statement
All of the participants provided informed consent. A statement attached to the questionnaire explained the study’s purpose and the voluntary nature of participation and confirmed that the analysis was anonymous. In addition to consent to participate, returning the questionnaire was viewed as consent to participate.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We are grateful to the residents and staff members of the Chofu-Digital-Choju movement.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cabinet Office. Japan Annual Report on the Ageing Society FY2022 (Entire Edition). Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2022/html/zenbun/index.html (accessed on 12 June 2023). (In Japanese)
- Andersen, F.K.; Christensen, K.; Frederiksen, H. Self-rated health and age: A cross-sectional and longitudinal study of 11,000 Danes aged 45–102. Scand. J. Public. Health 2007, 35, 164–171. [Google Scholar] [CrossRef]
- Matsui, Y.; Tanizaki, Y.; Arima, H.; Yonemoto, K.; Doi, Y.; Ninomiya, T.; Sasaki, K.; Iida, M.; Iwaki, T.; Kanba, S.; et al. Incidence and survival of dementia in a general population of Japanese elderly: The Hisayama study. J. Neurol. Neurosurg. Psychiatry 2009, 80, 366–370. [Google Scholar] [CrossRef]
- Hughes, M.E.; Waite, L.J. Marital biography and health at mid-life. J. Health Soc. Behav. 2009, 50, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Laditka, J.N.; Laditka, S.B. Increased hospitalization risk for recently widowed older women and protective effects of social contacts. J. Women Aging 2003, 15, 7–28; discussion 185. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Mental Health Action Plan 2013–2020. Available online: https://www.who.int/publications-detail-redirect/9789241506021 (accessed on 12 June 2023).
- Gale, C.R.; Cooper, C.; Deary, I.J.; Aihie Sayer, A. Psychological well-being and incident frailty in men and women: The English longitudinal study of ageing. Psychol. Med. 2014, 44, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Chida, Y.; Steptoe, A. Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, Y.; Saito, Y. Subjective well-being and active life expectancy in Japan: Evidence from a longitudinal Study. Innov. Aging 2023, 7, igac075. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Sörensen, S. Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychol. Aging 2000, 15, 187–224. Available online: https://psycnet.apa.org/doi/10.1037/0882-7974.15.2.187 (accessed on 1 June 2023). [CrossRef] [PubMed]
- Iwano, S.; Kambara, K.; Aoki, S. Psychological interventions for well-being in healthy older adults: Systematic review and meta-analysis. J. Happiness Stud. 2022, 23, 2389–2403. [Google Scholar] [CrossRef]
- Suragarn, U.; Hain, D.; Pfaff, G. Approaches to enhance social connection in older adults: An integrative review of literature. Aging Health Res. 2021, 1, 100029. [Google Scholar] [CrossRef]
- Kokubun, K.; Ogawa, T.; Browne, R.; Shinada, T.; Granrath, L.; Moeller, J.; Tram, N.; Wieching, R.; Taki, Y. Social capital mediates the association between the ICT usage and well-being of older People in Japan: Implication for a new design paradigm. Sustainability 2022, 14, 4148. [Google Scholar] [CrossRef]
- Putnam, R.D.; Alone, B. America’s declining social capital. In Culture and Politics; Reader, A., Crothers, L., Lockhart, C., Eds.; Palgrave MacMillan: New York, NY, USA, 2000; pp. 223–234. ISBN 978-1-349-62397-6. [Google Scholar]
- Gasteiger, C.; Collens, P.; du Preez, E. Community-based support to improve mental health and wellbeing in older sexually and gender diverse people: A scoping review. Aging Ment. Health 2023, 1–9. [Google Scholar] [CrossRef]
- Foettinger, L.; Albrecht, B.M.; Altgeld, T.; Gansefort, D.; Recke, C.; Stalling, I.; Bammann, K. The Role of community-based men’s sheds in health promotion for older men: A mixed-methods systematic review. Am. J. Mens. Health 2022, 16, 15579883221084490. [Google Scholar] [CrossRef]
- Giebel, C.; Shrestha, N.; Reilly, S.; White, R.G.; Zuluaga, M.I.; Saldarriaga, G.; Liu, G.; Allen, D.; Gabbay, M. Community-based mental health and well-being interventions for older adults in low- and middle-income countries: A systematic review and meta-analysis. BMC Geriatr. 2022, 22, 773. [Google Scholar] [CrossRef]
- Handley, M.A.; Lyles, C.R.; McCulloch, C.; Cattamanchi, A. Selecting and improving quasi-experimental designs in effectiveness and implementation research. Annu. Rev. Public. Health 2018, 39, 5–25. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Seino, S.; Nofuji, Y.; Sugawara, Y.; Osuka, Y.; Kitamura, A.; Shinkai, S. The Kesennuma Study in Miyagi, Japan: Study design and baseline profiles of participants. J. Epidemiol. 2022, 32, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Chofu City Households and Population in Chofu City. 2021. Available online: https://www.city.chofu.tokyo.jp/www/contents/1610018912361/index.html (accessed on 1 June 2023). (In Japanese).
- Statistics of Japan Population Census 2020. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200521&tstat=000001136464&cycle=0&tclass1=000001136472&tclass2=000001159886&cycle_facet=tclass1%3Acycle&tclass3val=0 (accessed on 1 June 2023). (In Japanese)
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public. Health 2013, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- Seino, S.; Tomine, Y.; Nishi, M.; Hata, T.; Fujiwara, Y.; Shinkai, S.; Kitamura, A. Effectiveness of a community-wide intervention for population-level frailty and functional health in older adults: A 2-year cluster nonrandomized controlled trial. Prev. Med. 2021, 149, 106620. [Google Scholar] [CrossRef] [PubMed]
- Seino, S.; Kitamura, A.; Tomine, Y.; Tanaka, I.; Nishi, M.; Nonaka, K.; Nofuji, Y.; Narita, M.; Taniguchi, Y.; Yokoyama, Y.; et al. A community-wide intervention trial for preventing and reducing frailty among older adults living in metropolitan areas: Design and baseline survey for a study integrating participatory action research with a cluster trial. J. Epidemiol. 2019, 29, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Glatzer, W.; Gulyas, J. Cantril self-anchoring striving scale. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 509–511. ISBN 978-94-007-0753-5. [Google Scholar]
- Saito, M.; Kondo, K.; Ojima, T.; Hirai, H.; JAGES group. Criteria for social isolation based on associations with health indicators among older people a 10-year follow-up of the Aichi gerontological evaluation study. Nihon Koshu Eisei Zasshi 2015, 62, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Seino, S.; Kitamura, A.; Nishi, M.; Tomine, Y.; Tanaka, I.; Taniguchi, Y.; Yokoyama, Y.; Amano, H.; Narita, M.; Ikeuchi, T.; et al. Individual- and community-level neighbor relationships and physical activity among Older Japanese adults living in a metropolitan area: A cross-sectional multilevel analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 46. [Google Scholar] [CrossRef]
- Nakamura, H.; Nakamura, M.; Okada, E.; Ojima, T.; Kondo, K. Association of food access and neighbor relationships with diet and underweight among community-dwelling Older Japanese. J. Epidemiol. 2017, 27, 546–551. [Google Scholar] [CrossRef]
- Ishikawa, H.; Nomura, K.; Sato, M.; Yano, E. Developing a measure of communicative and critical health literacy: A pilot study of Japanese office workers. Health Promot. Int. 2008, 23, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Awata, S.; Bech, P.; Yoshida, S.; Hirai, M.; Suzuki, S.; Yamashita, M.; Ohara, A.; Hinokio, Y.; Matsuoka, H.; Oka, Y. Reliability and validity of the Japanese version of the World Health Organization-five well-being index in the context of detecting depression in diabetic patients. Psychiatry Clin. Neurosci. 2007, 61, 112–119. [Google Scholar] [CrossRef]
- Awata, S.; Bech, P.; Koizumi, Y.; Seki, T.; Kuriyama, S.; Hozawa, A.; Ohmori, K.; Nakaya, N.; Matsuoka, H.; Tsuji, I. Validity and utility of the Japanese version of the WHO-five well-being index in the context of detecting suicidal ideation in elderly community residents. Int. Psychogeriatr. 2007, 19, 77–88. [Google Scholar] [CrossRef]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef]
- Rinaldi, P.; Mecocci, P.; Benedetti, C.; Ercolani, S.; Bregnocchi, M.; Menculini, G.; Catani, M.; Senin, U.; Cherubini, A. Validation of the five-item Geriatric Depression Scale in elderly subjects in three different settings. J. Am. Geriatr. Soc. 2003, 51, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Kamada, M.; Kitayuguchi, J.; Inoue, S.; Ishikawa, Y.; Nishiuchi, H.; Okada, S.; Harada, K.; Kamioka, H.; Shiwaku, K. A community-wide campaign to promote physical activity in middle-aged and elderly People: A cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 44. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Shinkai, S.; Watanabe, N.; Yoshida, H.; Fujiwara, Y.; Amano, H.; Lee, S.; Nishi, M.; Tsuchiya, Y. Research on Screening for Frailty: Development of “the Kaigo-Yobo Checklist”. Nihon Koshu Eisei Zasshi 2010, 57, 345–354. [Google Scholar] [CrossRef]
- Shinkai, S.; Watanabe, N.; Yoshida, H.; Fujiwara, Y.; Nishi, M.; Fukaya, T.; Lee, S.; Kim, M.J.; Ogawa, K.; Murayama, H.; et al. Validity of the “Kaigo-Yobo Check-List” as a frailty index. Nihon Koshu Eisei Zasshi 2013, 60, 262–274. [Google Scholar] [PubMed]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG index of competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Kinugasa, T.; Nagasaki, H. Reliability and validity of the motor fitness scale for older adults in the community. Aging 1998, 10, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Yasumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. Nihon Koshu Eisei Zasshi 2003, 50, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Moriyasu, A.; Kumagai, S.; Furuna, T.; Akita, S.; Kimura, S.; Suzuki, T. Community-based intervention to improve dietary habits and promote physical activity among older adults: A cluster randomized trial. BMC Geriatr. 2013, 13, 8. [Google Scholar] [CrossRef]
- Tani, Y.; Sasaki, Y.; Haseda, M.; Kondo, K.; Kondo, N. Eating Alone and depression in older men and women by cohabitation status: The JAGES longitudinal survey. Age Ageing 2015, 44, 1019–1026. [Google Scholar] [CrossRef]
- LaMonica, H.M.; Davenport, T.A.; Roberts, A.E.; Hickie, I.B. Understanding technology preferences and requirements for health information technologies designed to improve and maintain the mental health and well-being of older adults: Participatory design Study. JMIR Aging 2021, 4, e21461. [Google Scholar] [CrossRef] [PubMed]
- Duplaga, M. The association between Internet use and health-related outcomes in older adults and the elderly: A cross-sectional study. BMC Med. Inform. Decis. Mak. 2021, 21, 150. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: A randomized controlled trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Otake, M.; Kato, M.; Takagi, T.; Asama, H. The Coimagination method and its evaluation via the conversation interactivity measuring method. In Early Detection and Rehabilitation Technologies for Dementia: Neuroscience and Biomedical Applications; IGI Global: Hershey, PA, USA, 2011; pp. 356–364. [Google Scholar]
- Mihoko, O.-M. Conversation assistive technology for maintaining cognitive health. J. Korean Gerontol. Nurs. 2018, 20 (Suppl. 1), 154–159. [Google Scholar] [CrossRef]
- Asakawa, Y.; Endo, F.; Yamaguchi, H.; Takahashi, R. The characteristics of participants and the effects of self-paced resistance training for community-dwelling elders in early period of a residents-led preventive care program, the Onishi Model. Rigaku Ryōhōgaku 2008, 35, 229–236. [Google Scholar] [CrossRef]
- Matsubayashi, Y.; Asakawa, Y.; Yamaguchi, H. Low-frequency group exercise improved the motor functions of community-dwelling elderly People in a rural area when combined with home exercise with self-monitoring. J. Phys. Ther. Sci. 2016, 28, 366–371. [Google Scholar] [CrossRef][Green Version]
- Fiatarone, M.A.; Marks, E.C.; Ryan, N.D.; Meredith, C.N.; Lipsitz, L.A.; Evans, W.J. High-intensity strength training in nonagenarians. Effects on skeletal muscle. JAMA 1990, 263, 3029–3034. [Google Scholar] [CrossRef]
- Marzuki, A.A.; Nor, N.N.F.M.; Rashid, S.M.R.A.; Ghazali, S. Social support by communities for older adults in Malaysia. Nurture 2023, 17, 272–280. [Google Scholar] [CrossRef]
- Choi, E.; Han, K.M.; Chang, J.; Lee, Y.J.; Choi, K.W.; Han, C.; Ham, B.J. Social participation and depressive symptoms in community-dwelling older adults: Emotional social support as a mediator. J. Psychiatr. Res. 2021, 137, 589–596. [Google Scholar] [CrossRef]
- Colistra, C.; Bixler, R.; Schmalz, D. Exploring factors that contribute to relationship building in a community center. J. Leis. Res. 2019, 50, 1–17. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Tiefenbach, T.; Kohlbacher, F. Subjective well-being across gender and age in Japan: An econometric analysis. In Gender, Lifespan and Quality of Life: An International Perspective; Eckermann, E., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 183–201. ISBN 978-94-007-7829-0. [Google Scholar] [CrossRef]
- Blanchflower, D.G.; Oswald, A.J. Is well-being U-shaped over the life cycle? Soc. Sci. Med. 2008, 66, 1733–1749. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, J.F.; Layard, R.; Sachs, J.D.; Neve, J.E.D.; Aknin, L.B.; Wang, S. World Happiness Report; Gallup: Washington, DC, USA, 2023; Volume 2023. [Google Scholar]
- Saito, T.; Sugisawa, H.; Harada, K.; Kai, I. Population aging in local areas and subjective well-being of older adults: Findings from two studies in Japan. BioSci Trends 2016, 10, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Statistics Bureau of Japan Current Population Estimates as of 2021. Available online: https://www.stat.go.jp/english/data/jinsui/2021np/index.html (accessed on 13 June 2023).
- Döring, N.; Conde, M.; Brandenburg, K.; Broll, W.; Gross, H.M.; Werner, S.; Raake, A. Can communication technologies reduce loneliness and social isolation in older People? A scoping review of reviews. Int. J. Environ. Res. Public. Health 2022, 19, 11310. [Google Scholar] [CrossRef] [PubMed]
- Hunsaker, A.; Hargittai, E. A review of Internet use among older adults. New Media Soc. 2018, 20, 3937–3954. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications the Communications Usage Trend Survey. 2022. Available online: https://www.soumu.go.jp/johotsusintokei/statistics/statistics05.html (accessed on 5 July 2023).
- Murayama, H.; Nofuji, Y.; Matsuo, E.; Nishi, M.; Taniguchi, Y.; Fujiwara, Y.; Shinkai, S. The Yabu cohort Study: Design and profile of participants at baseline. J. Epidemiol. 2014, 24, 519–525. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).