
Experience of Labour and Childbirth in a Sample of Portuguese Women: A Cross-Sectional Study


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Data Collection and Measures
2.3.1. Sociodemographic Questionnaire
2.3.2. Labour and Childbirth Experience Questionnaire (LCEQ)
2.3.3. Satisfaction with Life Scale
2.3.4. Women’s Perception of Care
2.3.5. Procedures
2.3.6. Statistical Analysis
3. Results and Discussion
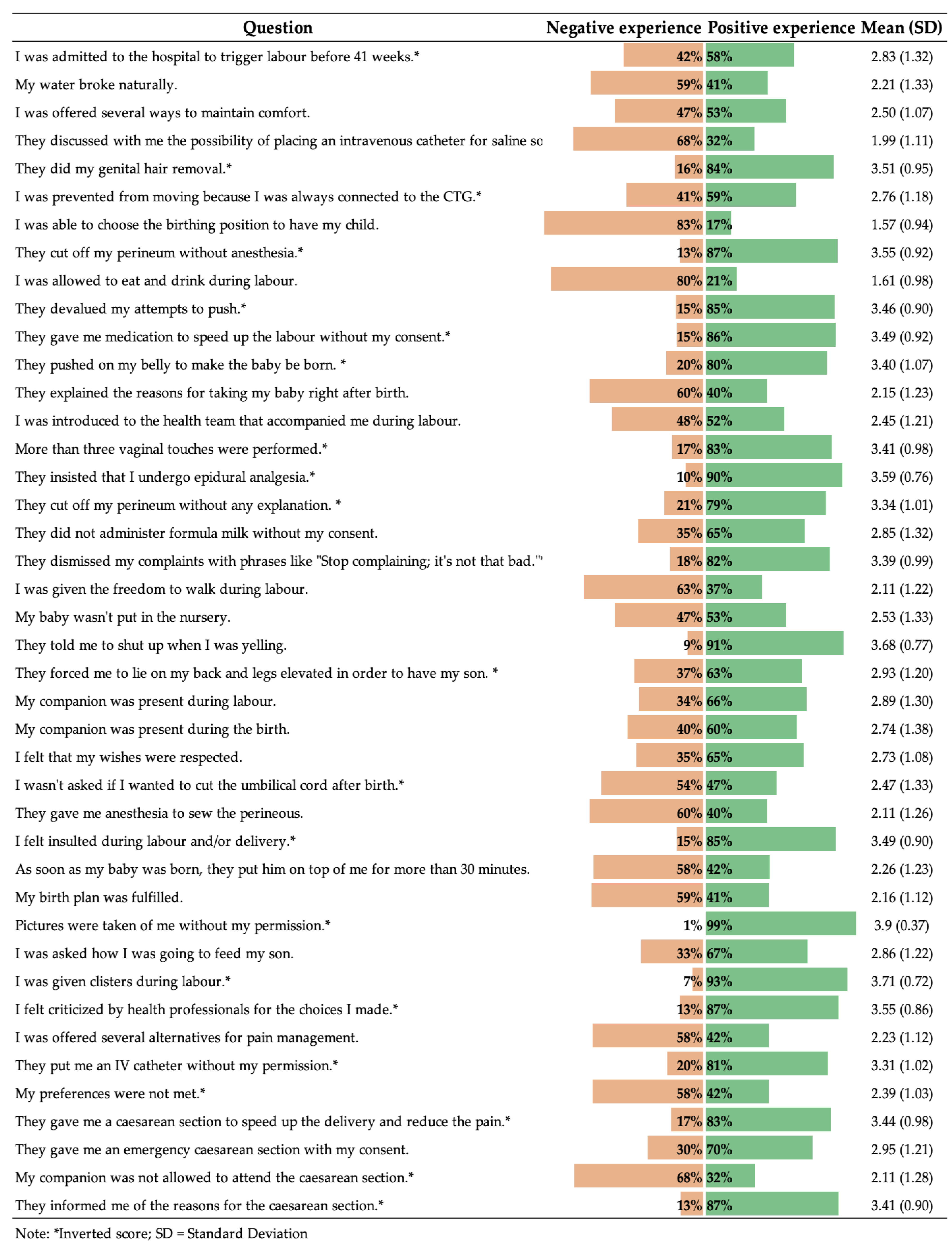
3.1. Analyzing the Variables
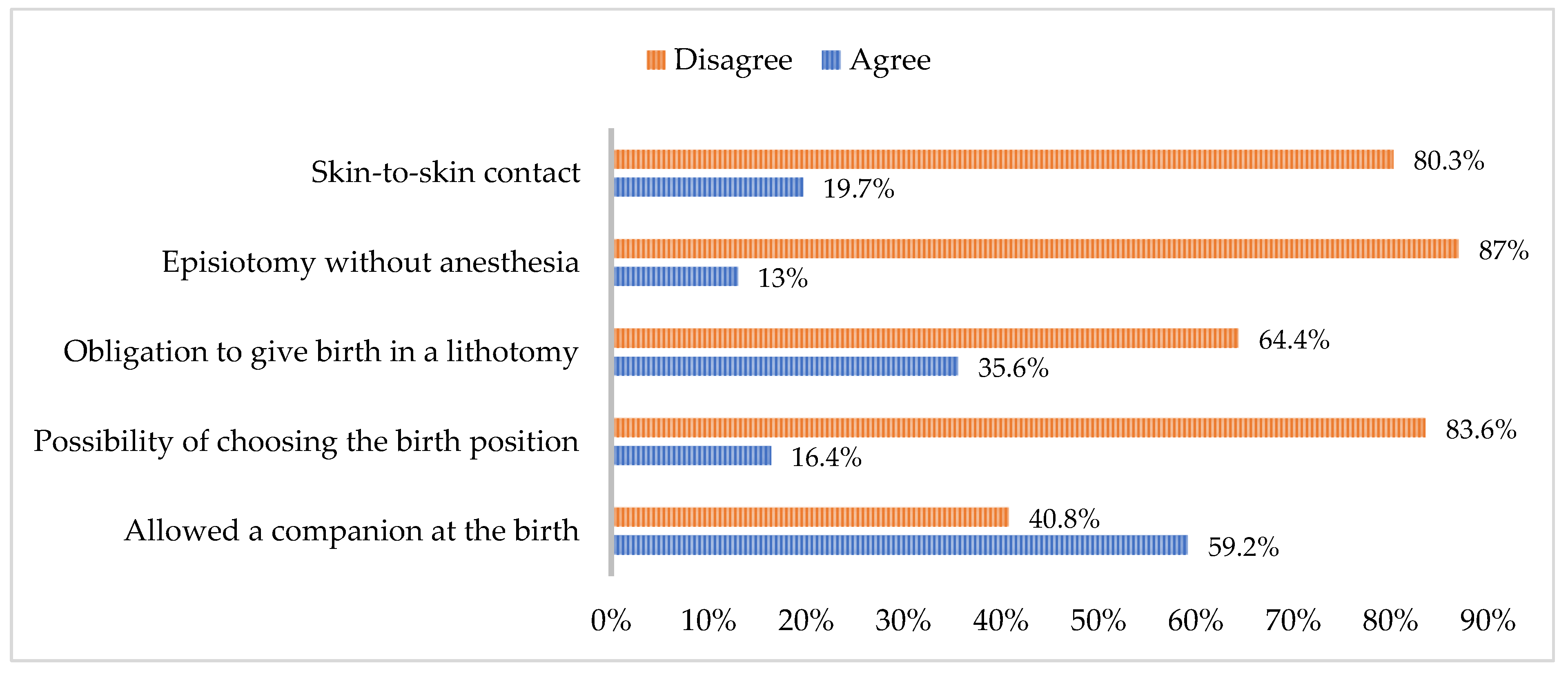
3.1.1. Practises That Influence the Experience of Labour
3.1.2. Practises That Influence the Experience of Vaginal Birth
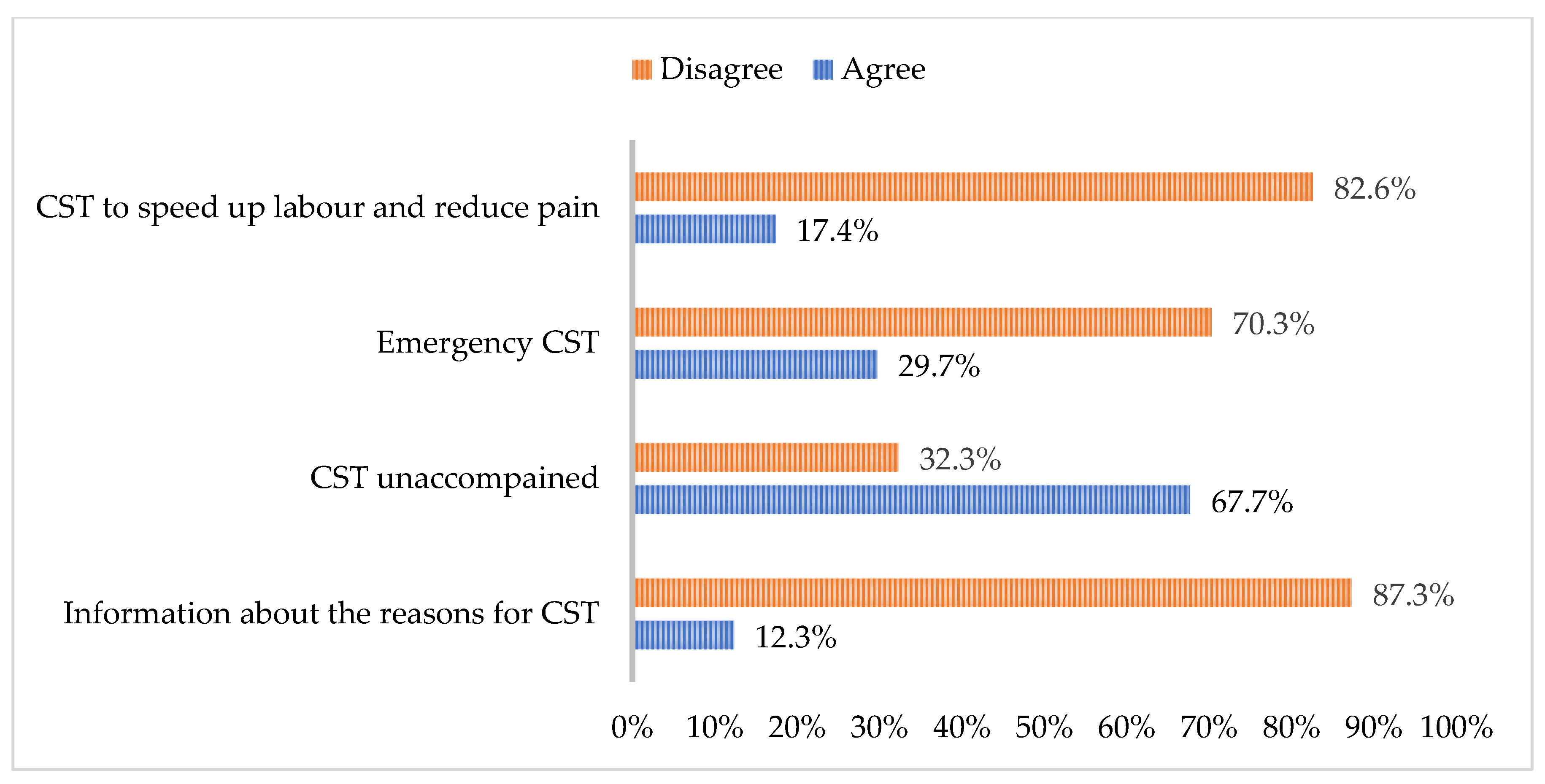
3.1.3. Practises That Influence the Experience of Caesarean Section
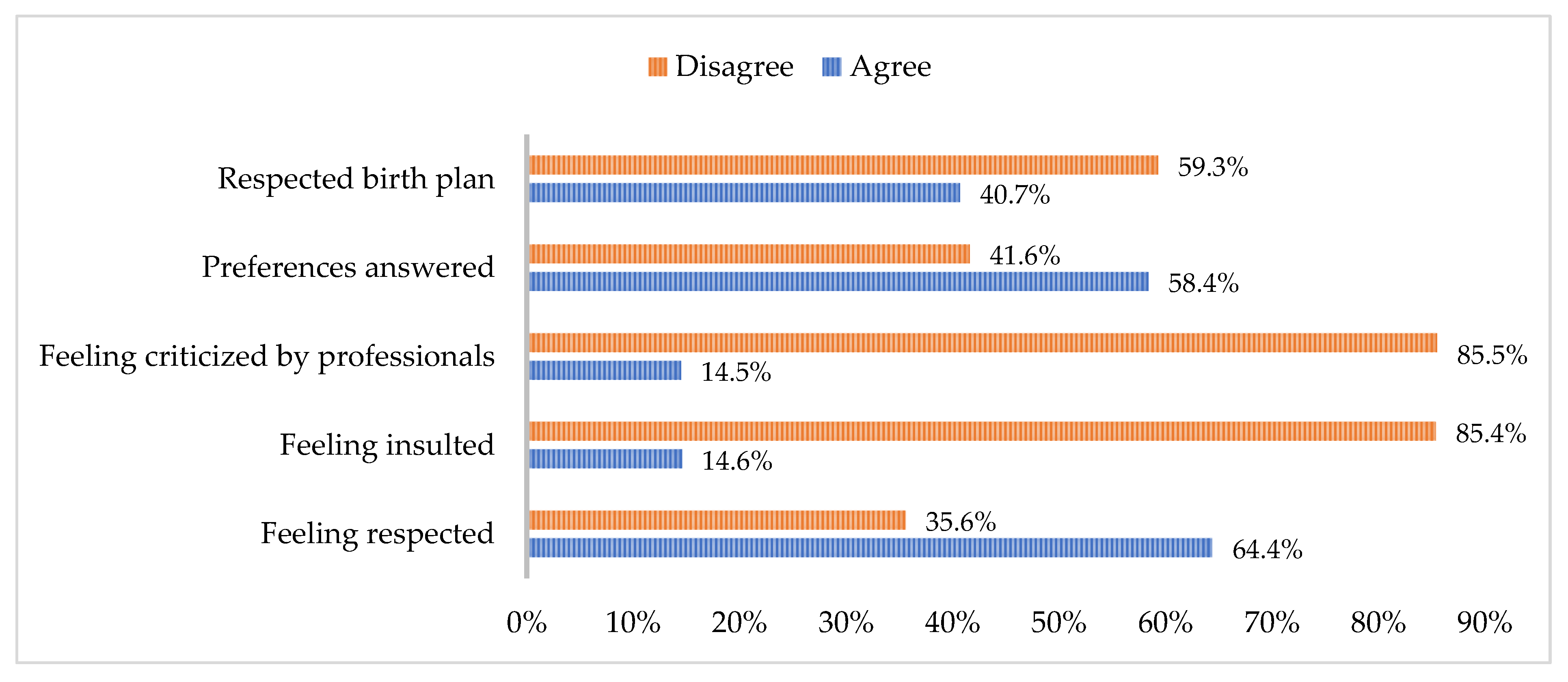
3.1.4. Emotional Experience During Labour and Birth
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beaton, J.; Gupton, A. Childbirth expectations: A qualitative analysis. Midwifery 1990, 6, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Webb, R.; Ayers, S.; Bogaerts, A.; Jeličić, L.; Pawlicka, P.; Van Haeken, S.; Uddin, N.; Xuereb, R.B.; Kolesnikova, N.; COST action CA18211:DEVoTION Team; et al. When birth is not as expected: A systematic review of the impact of a mismatch between expectations and experiences. BMC Pregnancy Childbirth 2021, 21, 475. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018; Available online: https://iris.who.int/handle/10665/260178 (accessed on 2 January 2024).
- Chervenak, F.A.; McLeod-Sordjan, R.; Pollet, S.L.; De Four Jones, M.; Gordon, M.R.; Combs, A.; Bornstein, E.; Lewis, D.; Katz, A.; Warman, A.; et al. Obstetric violence is a misnomer. Am. J. Obstet. Gynecol. 2024, 230, S1138–S1145. [Google Scholar] [CrossRef] [PubMed]
- Simonovic, D. A Human Rights-Based Approach to Mistreatment and Violence Against Women in Reproductive Health Services with a Focus on Childbirth and Obstetric Violence. 2019. Available online: https://digitallibrary.un.org/record/3823698 (accessed on 31 March 2024).
- Lundh, C.; Øvrum, A.-K.; Dahl, B. Women’s experiences with unexpected induction of labor: A qualitative study. Eur. J. Midwifery 2023, 7, 1–7. [Google Scholar] [CrossRef]
- Viirman, F.; Hess Engström, A.; Sjömark, J.; Hesselman, S.; Sundström Poromaa, I.; Ljungman, L.; Skoog Svanberg, A.; Wikman, A. Negative childbirth experience in relation to mode of birth and events during labour: A mixed methods study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2023, 282, 146–154. [Google Scholar] [CrossRef]
- Simões, A. Ulterior validação de uma escala de satisfação com a vida (SWLS). Rev. Port. Pedagog. 1992, 26, 503–515. [Google Scholar]
- Marôco, J.; Garcia-Marques, T. Qual a fiabilidade do alfa de Cronbach? Questões antigas e soluções modernas? Laboratório Psicol. 2006, 4, 65–90. [Google Scholar] [CrossRef]
- Bohren, M.A.; Mehrtash, H.; Fawole, B.; Maung, T.M.; Balde, M.D.; Maya, E.; Thwin, S.S.; Aderoba, A.K.; Vogel, J.P.; Irinyenikan, T.A.; et al. How women are treated during facility-based childbirth in four countries: A cross-sectional study with labour observations and community-based surveys. Lancet 2019, 394, 1750–1763. [Google Scholar] [CrossRef]
- Lukasse, M.; Schroll, A.; Karro, H.; Schei, B.; Steingrimsdottir, T.; Van Parys, A.; Ryding, E.L.; Tabor, A.; the Bidens Study Group. Prevalence of experienced abuse in healthcare and associated obstetric characteristics in six European countries. Acta Obs. Gynecol. Scand. 2015, 94, 508–517. [Google Scholar] [CrossRef]
- Kim, S. World Health Organization Quality of Life (WHOQOL) Assessment. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 7260–7261. [Google Scholar]
- Coates, D.; Homer, C.; Wilson, A.; Deady, L.; Mason, E.; Foureur, M.; Henry, A. Induction of labour indications and timing: A systematic analysis of clinical guidelines. Women Birth 2020, 33, 219–230. [Google Scholar] [CrossRef]
- Declercq, E.; Belanoff, C.; Iverson, R. Maternal perceptions of the experience of attempted labor induction and medically elective inductions: Analysis of survey results from listening to mothers in California. BMC Pregnancy Childbirth 2020, 20, 458. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, A.C.J.; Van Der Post, J.A.M.; De Groot, C.J.M.; Abu-Hanna, A.; Eskes, M. Does induction of labor at 41 weeks (early, mid or late) improve birth outcomes in low-risk pregnancy? A nationwide propensity score-matched study. Acta Obs. Gynecol. Scand. 2023, 102, 612–625. [Google Scholar] [CrossRef] [PubMed]
- Sgayer, I.; Wolf, M.F. Induction of labor at 39 weeks of gestation versus expectant management. Harefuah 2019, 12, 802–806. [Google Scholar]
- Silva, T.M.A.; Góis, G.A.S.; Filgueiras, T.F.; Candeia, R.M.S. Significados e práticas da equipe de enfermagem acerca do parto humanizado: Uma revisão de literatura. Braz. J. Surg. Clin. Res. 2019, 26, 90–94. [Google Scholar]
- Shea-Lewis, A.; Eckardt, P.; Stapleton, D. CE: Original Research: An Investigation into the Safety of Oral Intake During Labor. Am. J. Nurs. 2018, 118, 24–31. [Google Scholar] [CrossRef]
- Bocoum, F.; Kabore, C.P.; Barro, S.; Zerbo, R.; Tiendrebeogo, S.; Hanson, C.; Dumont, A.; Betran, A.P.; Bohren, M.A. Women’s and health providers’ perceptions of companionship during labor and childbirth: A formative study for the implementation of WHO companionship model in Burkina Faso. Reprod. Health 2023, 20, 46. [Google Scholar] [CrossRef]
- Bohren, M.A.; Berger, B.O.; Munthe-Kaas, H.; Tunçalp, Ö. Perceptions and experiences of labour companionship: A qualitative evidence synthesis. Cochrane Database Syst. Rev. 2019, 3, CD012449. [Google Scholar] [CrossRef]
- Tefera, Z.; Assefaw, M.; Gashaw, W.; Ayalew, S.; Birrie, E.; Selassie, M.W.; Wogie, G. Pregnant Women’s Knowledge and Desire Towards Labor Companionship and its Associated Factors at Public Hospitals in South Wollo Zone, Northeast Ethiopia. J. Midwifery Reprod. Health 1999, 10, 3393–3404. [Google Scholar] [CrossRef]
- Kaasen, A.; Aanstad, K.J.; Pay, A.S.D.; Økland, I.; Blix, E. National survey of routines for intrapartum fetal monitoring in Norway. Acta Obs. Gynecol. Scand. 2019, 98, 390–395. [Google Scholar] [CrossRef]
- Osorio-Ramírez, A.; Gómez-Gómez, M.M.; Alzate-Yepes, T.; Giraldo-Mejía, G.E.; Salazar-Blanco, O.F. Ser docente de ciencias de la salud en la Universidad de Antioquia, Colombia. Rev. Fac. Med. 2021, 70, e93520. [Google Scholar] [CrossRef]
- Camargo-Villalba, G.E.; Güezgüan-Pérez, J.A.; Sánchez-Capacho, N.; Barragán-Acevedo, J.T.; Huamanga-Gamarra, B.; Soto-Bringas, R.I. Clinical behavior of vertical delivery and in lithotomy position in two Health Centers of Cusco, Peru. Ginecol. Obs. Mex. 2022, 90, 222–233. [Google Scholar]
- Fagundes Baigorra, R.; Silva, Y.P.D.; Furlanetto, M.P. Análise dos desfechos do uso da banqueta durante o trabalho de parto: Revisão sistemática. Fisioter. Bras. 2023, 24, 215–230. [Google Scholar] [CrossRef]
- Fard, D.; Borchers, C.S.; Philippeit, J.-C.; Philippeit, A.V.; Kaukemüller, L.R.; Higgins-wood, L.R.; Papageorgiou, S.; Hillemanns, P.; Von Kaisenberg, C.S.; Klapdor, R. Comparing forces on the fetal neck in breech delivery in lithotomy versus all-fours position: A simulation model. Arch. Gynecol. Obs. 2022, 308, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Meijer, M.; Brandão, T.; Cañadas, S.; Falcon, K. Components of obstetric violence in health facilities in Quito, Ecuador: A descriptive study on information, accompaniment, and position during childbirth. Int. J. Gynecol. Obs. 2020, 148, 355–360. [Google Scholar] [CrossRef]
- Nikoukar, F.; Dadkhahtehrani, T.; Valiani, M.; Movahedi, M. Comparison of maternal and fetal outcomes between lithotomy with hands and knees positions for childbirth: A randomized clinical trial. J. Nurs. Midwifery Sci. 2023, 10, e135325. [Google Scholar]
- Martín-Vázquez, C.; Goás-Gómez, N.; Calvo-Ayuso, N.; Rosón-Matilla, L.; Quiroga-Sánchez, E.; García-Fernández, R. Analysis of maternal positions during the dilation and expulsive phase and their relationship with perineal injuries in eutocic deliveries attended by midwives. Healthcare 2024, 12, 441. [Google Scholar] [CrossRef]
- Ruiz, M.T.; Azevedo, N.F.; Raponi, M.B.G.; Fonseca, L.M.M.; Wernet, M.; Silva, M.P.C.; Contim, D. Skin-to-skin contact in the third stage of labor and postpartum hemorrhage prevention: A scoping review. Matern. Child. Health J. 2023, 27, 582–596. [Google Scholar] [CrossRef]
- Forde, D.; Fang, M.L.; Miaskowski, C. A Systematic Review of the Effects of Skin-to-Skin Contact on Biomarkers of Stress in Preterm Infants and Parents. Adv. Neonatal Care 2022, 22, 223–230. [Google Scholar] [CrossRef]
- NICE. Caesarean Birth. NG192. Available online: https://www.nice.org.uk/guidance/ng192/resources/caesarean-birth-pdf-66142078788805 (accessed on 18 October 2024).
- Bohren, M.A.; Hofmeyr, G.J.; Sakala, C.; Fukuzawa, R.K.; Cuthbert, A. Continuous support for women during childbirth. Cochrane Database Syst. Rev. 2017, 2017, CD003766. [Google Scholar] [CrossRef]
- Bohren, M.A.; Hunter, E.C.; Munthe-Kaas, H.M.; Souza, J.P.; Vogel, J.P.; Gülmezoglu, A.M. Facilitators and barriers to facility-based delivery in low- and middle-income countries: A qualitative evidence synthesis. Reprod. Health 2014, 11, 71. [Google Scholar] [CrossRef]
- Burcher, P.; Cheyney, M.J.; Li, K.N.; Hushmendy, S.; Kiley, K.C. Cesarean Birth Regret and Dissatisfaction: A Qualitative Approach. Birth 2016, 43, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Melo, B.L.P.L.; Moreira, F.T.D.S.; Moreira De Alencar, R.; Magalhães, B.D.C.; Cavalcante, E.R.; Maia, E.R.; Albuquerque, G.A. Violência obstétrica à luz da Teoria da Diversidade e Universalidade do Cuidado Cultural. Rev. Cuid. 2022, 13, e1536. [Google Scholar] [CrossRef]
- Rudman, A.; El-Khouri, B.; Waldenström, U. Women’s satisfaction with intrapartum care—A pattern approach. J. Adv. Nurs. 2007, 59, 474–487. [Google Scholar] [CrossRef]
- Coutinho, E.D.C.; Silva, A.L.D.; Pereira, C.M.F.P.; Almeida, A.I.; Nelas, P.A.B.; Parreira, V.B.C.; Amaral, M.O. Health care to immigrant and Portuguese pregnant women in Portugal. Rev. Esc. Enferm. USP 2014, 48, 9–16. [Google Scholar] [CrossRef]
- Fernandes, S.; Galacho, J.; Borrego, A.; Pereira, D.; Lança, F.; Ormonde, L. Impact of Labor Epidural Analgesia on Maternal Satisfaction and Childbirth Expectations in a Tertiary Care Center in Portugal: A Prospective Study. Acta Med. Port. 2021, 34, 272–277. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. QETPP | __ | 0.21 *** | −0.32 *** | 0.10 ** | 0.09 * | 0.06 | −0.14 *** | 0.05 | −0.12 ** | −0.01 | 0.62 *** |
| 2. SLWS | __ | −0.01 | 0.17 *** | 0.18 *** | −0.02 *** | 0.09 * | 0.11 * | 0.04 * | 0.04 | 0.34 *** | |
| 3. Type of labour | __ | −0.01 | 0.01 | 0.01 | −0.07 | −0.17 *** | 0.01 | 0.01 | −0.11 ** | ||
| 4. Age when becoming a mother | __ | 0.32 *** | 0.01 | 0.03 | 0.31 *** | −0.06 | −0.02 | 0.15 *** | |||
| 5. Educational qualifications | __ | 0.03 | −0.02 | −0.13 ** | −0.30 *** | −0.04 | 0.04 | ||||
| 6. Marital status | __ | −0.13 ** | −0.8 | −0.07 | 0.01 | 0.05 | |||||
| 7. Place of residence | __ | 0.13 ** | 0.18 *** | −0.02 | −0.06 | ||||||
| 8. Number of children | __ | 0.21 *** | −0.01 | 0.11 ** | |||||||
| 9. Labour preparation | __ | −0.01 | −0.02 | ||||||||
| 10. Pregnancy monitoring | __ | 0.03 | |||||||||
| 11. Overall satisfaction | __ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavares, M.; Alexandre-Sousa, P.; Victória, A.; Loureiro, S.; Santos, A.P.; Mendes, J. Experience of Labour and Childbirth in a Sample of Portuguese Women: A Cross-Sectional Study. Healthcare 2024, 12, 2125. https://doi.org/10.3390/healthcare12212125
Tavares M, Alexandre-Sousa P, Victória A, Loureiro S, Santos AP, Mendes J. Experience of Labour and Childbirth in a Sample of Portuguese Women: A Cross-Sectional Study. Healthcare. 2024; 12(21):2125. https://doi.org/10.3390/healthcare12212125
Chicago/Turabian StyleTavares, Márcio, Pedro Alexandre-Sousa, Andrea Victória, Susana Loureiro, Ana Paula Santos, and José Mendes. 2024. "Experience of Labour and Childbirth in a Sample of Portuguese Women: A Cross-Sectional Study" Healthcare 12, no. 21: 2125. https://doi.org/10.3390/healthcare12212125
APA StyleTavares, M., Alexandre-Sousa, P., Victória, A., Loureiro, S., Santos, A. P., & Mendes, J. (2024). Experience of Labour and Childbirth in a Sample of Portuguese Women: A Cross-Sectional Study. Healthcare, 12(21), 2125. https://doi.org/10.3390/healthcare12212125