Impact of Physical Activity on Autonomy and Quality of Life in Individuals with Down Syndrome: A Systematic Review

 ,
,  and
and
Abstract
1. Introduction
1.1. Epidemiology and General Characteristics of Down Syndrome
1.2. Physical Activity and People with Down Syndrome
1.3. Autonomy and Quality of Life
1.4. Impact of Physical Activity on Quality of Life in People with Down Syndrome
- Is physical activity or sports an effective strategy to increase autonomy and to improve physical, cognitive, emotional, and social quality of life in people with DS?
- What is the methodological quality of the investigations that have studied this topic?
- Is there any type of physical activity or sports intervention that should be encouraged and prescribed to this population to enhance autonomy and quality of life?
2. Materials and Methods
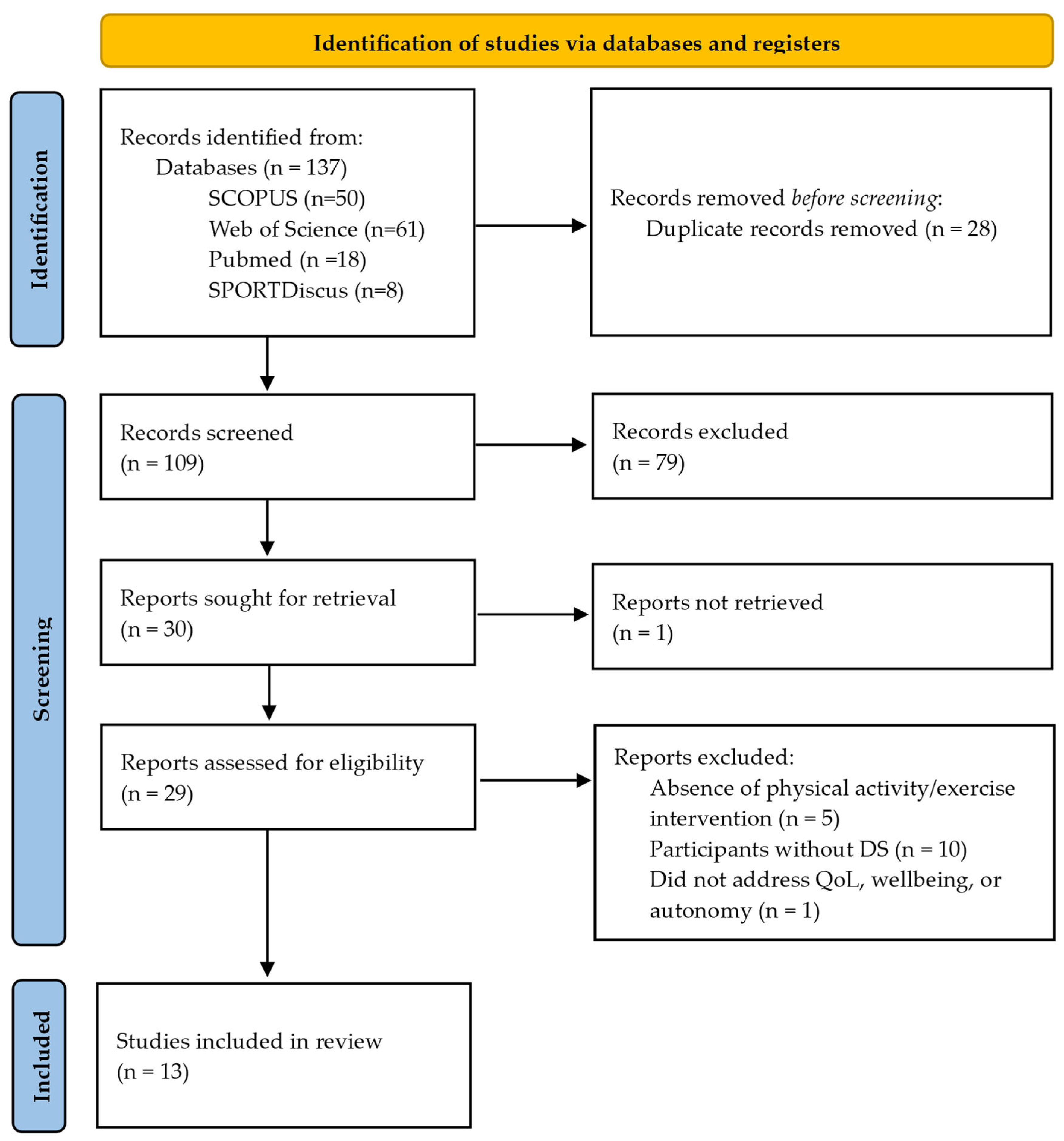
2.1. Data Source and Search Protocol
2.2. Study Selection Criteria
2.3. Methodological Quality Assessment
2.4. Use of Artificial Intelligence
3. Results
3.1. Methodological Quality Analysis
3.2. Characteristics of the Intervention
3.3. Characteristics of the Sample
3.4. Impact of the Intervention
3.4.1. Autonomy
- Cognitive Function
- Functional Mobility and Motor Proficiency
- Adherence and Independence
3.4.2. Quality of Life
- Physical Wellbeing
- Physical Fitness and Psychomotor Skills
- Anthropometric Measures
- Healthy Habits and Leisure Time Use
- Posture and Baropodometry
- Amount of Moderate to Vigorous Physical Activity
- General Health, Quality of Life and Wellbeing
- Psychological, Cognitive, and Emotional Wellbeing
- Self-Esteem and Self-Determination
- Emotional State and Mood
- Personal Satisfaction and Development
- Social Wellbeing
- Interpersonal Relationships
- Social Inclusion and Rights
4. Discussion
4.1. Effects of Interventions on Autonomy
- Cognitive Function
- Functional Mobility and Motor Proficiency
- Adherence
- Independence
4.2. Effects of Interventions on Physical Wellbeing
- Physical Fitness and Psychomotor Skills
- Anthropometric Measures
- Healthy Habits and Leisure Time Use
- Posture and Baropodometry
- Amount of Moderate to Vigorous Physical Activity
- General Health, Quality of Life and Wellbeing
4.3. Effects of Interventions on Psychological, Cognitive, and Emotional Wellbeing
- Self-Esteem and Self-Determination
- Emotional State and Mood
- Personal Satisfaction and Development
4.4. Effects of Interventions on Social Wellbeing
- Interpersonal Relationships
- Social Inclusion and Rights
4.5. General Considerations
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pérez-Chávez, D.A. Síndrome de Down. Rev. Actual Clín. Investig. 2014, 45, 2357–2361. [Google Scholar]
- Bittles, A.H.; Bower, C.; Hussain, R.; Glasson, E.J. The Four Ages of Down Syndrome. Eur. J. Public Health 2007, 17, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Cocchi, G.; Gualdi, S.; Bower, C.; Halliday, J.; Jonsson, B.; Myrelid, Å.; Mastroiacovo, P.; Amar, E.; Bakker, M.K.; Correa, A.; et al. International Trends of Down Syndrome 1993–2004: Births in Relation to Maternal Age and Terminations of Pregnancies. Birth Defects Res. A Clin. Mol. Teratol. 2010, 88, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Lai, F.M.; Woo, B.H.; Tan, K.H.; Huang, J.; Lee, S.T.; Yan, T.B.; Tan, B.H.; Chew, S.K.; Yeo, G.S.H. Birth Prevalence of Down Syndrome in Singapore from 1993 to 1998. Singap. Med. J. 2002, 43, 70–76. [Google Scholar]
- Royston, P.; Thompson, S.G. Model-based Screening by Risk with Application to down’s Syndrome. Stat. Med. 1992, 11, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Hernández-García, C.R.; Luján-Muñoz, I. Equinoterapia. Rehabilitación Holística. Plast. Restaur. Neurol. 2006, 5, 70–74. [Google Scholar]
- Gupta, S.; Rao, B.K.; Kumaran, S. Effect of Strength and Balance Training in Children with Down’s Syndrome: A Randomized Controlled Trial. Clin. Rehabil. 2011, 25, 425–432. [Google Scholar] [CrossRef]
- Lizama, M.; Retamales, N.; Mellado, C. Recomendaciones de Cuidados En Salud de Personas Con Síndrome de Down: 0 a 18 Años. Rev. Med. Chile 2013, 141, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Fox, B.; Moffett, G.E.; Kinnison, C.; Brooks, G.; Case, L.E. Physical Activity Levels of Children with Down Syndrome. Pediatr. Phys. Ther. 2019, 31, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Case, L.; Ross, S.; Yun, J. Physical Activity Guideline Compliance among a National Sample of Children with Various Developmental Disabilities. Disabil. Health J. 2020, 13, 100881. [Google Scholar] [CrossRef]
- Piggin, J. What Is Physical Activity? A Holistic Definition for Teachers, Researchers and Policy Makers. Front. Sports Act. Living 2020, 2, 72. [Google Scholar] [CrossRef]
- Amatori, S.; Sisti, D.; Perroni, F.; Brandi, G.; Rocchi, M.B.L.; Gobbi, E. Physical Activity, Sedentary Behaviour and Screen Time among Youths with Down Syndrome during the COVID-19 Pandemic. J. Intellect. Disabil. Res. 2022, 66, 903–912. [Google Scholar] [CrossRef] [PubMed]
- Menear, K. Parents’ Perceptions of Health and Physical Activity Needs of Children with Down Syndrome. Down’s Syndr. Res. Pract. 2007, 12, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, S.; Banakhar, M.; Badr, H.; Alsulami, S. Physical Activity among Children with down Syndrome: Maternal Perception. Int. J. Qual. Stud. Health Well-Being 2021, 16, 1932701. [Google Scholar] [CrossRef]
- Barr, M.; Shields, N. Identifying the Barriers and Facilitators to Participation in Physical Activity for Children with Down Syndrome. J. Intellect. Disabil. Res. 2011, 55, 1020–1033. [Google Scholar] [CrossRef]
- Mosso, C.; Santander, P.; Pettinelli, P.; Valdés, M.; Celis, M.; Espejo, F.; Navarro, L.; Sepúlveda, F. Evaluación de Una Intervención En Actividad Física En Niños Con Síndrome de Down. Rev. Chil. Pediatr. 2011, 82, 311–318. [Google Scholar] [CrossRef][Green Version]
- WHO. World Report on Disability; World Health Organization: Ginebra, Switzerland, 2011. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Intrinsic Motivation and Self-Determination in Human Behavior; Plenum Press: New York, NY, USA, 1985; ISBN 0-306-42022-8. [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Schalock, R.L.; Verdugo, M.Á. Handbook on Quality of Life for Human Service Practitioners; American Association on Mental Retardation: Silver Spring, MD, USA, 2002; ISBN 9780940898776. [Google Scholar]
- Rodríguez-Crespo, M.M. Evaluación de La Calidad de Vida En Niños y Jóvenes Con Síndrome de Down. Doctoral Dissertation, Universidad de Salamanca, Salamanca, Spain, 2018. [Google Scholar]
- Gómez, L.E.; Alcedo, M.Á.; Arias, B.; Fontanil, Y.; Arias, V.B.; Monsalve, A.; Verdugo, M.Á. A New Scale for the Measurement of Quality of Life in Children with Intellectual Disability. Res. Dev. Disabil. 2016, 53–54, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Van Hecke, N.; Claes, C.; Vanderplasschen, W.; De Maeyer, J.; De Witte, N.; Vandevelde, S. Conceptualisation and Measurement of Quality of Life Based on Schalock and Verdugo’s Model: A Cross-Disciplinary Review of the Literature. Soc. Indic. Res. 2018, 137, 335–351. [Google Scholar] [CrossRef]
- Schalock, R.L.; Keith, K.D.; Verdugo, M.A.; Gómez, L.E. Quality of Life Model Development in the Field of Intellectual Disability. In Quality of Life for People with Intellectual Disability; Kober, R., Ed.; Springer: New York, NY, USA, 2010; pp. 17–32. [Google Scholar]
- Schalock, R.L.; Verdugo, M.A. A Leadership Guide to Redefining Intellectual and Developmental Disabilities Organizations: Eight Successful Change Strategies; Brookes Publishing Company: Baltimore, MD, USA, 2012; ISBN 978-1-5985-7181-3. [Google Scholar]
- Norton, M.; Dyches, T.T.; Harper, J.M.; Roper, S.O.; Caldarella, P. Respite Care, Stress, Uplifts, and Marital Quality in Parents of Children with Down Syndrome. J. Autism Dev. Disord. 2016, 46, 3700–3711. [Google Scholar] [CrossRef]
- Bertapelli, F.; Martin, J.E.S.; Gonçalves, E.M.; de Oliveira Barbeta, V.J.; Guerra-Júnior, G. Growth Curves in Down Syndrome: Implications for Clinical Practice. Am. J. Med. Genet. A 2014, 164, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Tomporowski, P.D.; McCullick, B.; Pendleton, D.M.; Pesce, C. Exercise and Children’s Cognition: The Role of Exercise Characteristics and a Place for Metacognition. J. Sport Health Sci. 2015, 4, 47–55. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Farrell, A.; Fabiano, M.; Radler, T.; Naclerio, F.; Ratamess, N.A.; Kang, J.; Myer, G.D. Effects of Integrative Neuromuscular Training on Fitness Performance in Children. Pediatr. Exerc. Sci. 2011, 23, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Yeo, G.S.H.; Lai, F.-M.; Wei, X.; Lata, P.; Tan, D.T.H.; Yong, M.H.; Tan, E.T.H.; Kwek, K.Y.C. Validation of First Trimester Screening for Trisomy 21 in Singapore with Reference to Performance of Nasal Bone. Fetal Diagn. Ther. 2012, 32, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Temple, V.A.; Frey, G.C.; Stanish, H.I. Physical Activity of Adults with Mental Retardation: Review and Research Needs. Am. J. Health Promot. 2006, 21, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Landa-Ramírez, E.; Arredondo-Pantaleón, A.d.J. Herramienta PICO Para La Formulación y Búsqueda de Preguntas Clínicamente Relevantes En La Psicooncología Basada En La Evidencia. Psicooncología 2014, 11, 259–270. [Google Scholar] [CrossRef]
- Kennedy, C.E.; Fonner, V.A.; Armstrong, K.A.; Denison, J.A.; Yeh, P.T.; O’Reilly, K.R.; Sweat, M.D. The Evidence Project Risk of Bias Tool: Assessing Study Rigor for Both Randomized and Non-Randomized Intervention Studies. Syst. Rev. 2019, 8, 3. [Google Scholar] [CrossRef]
- González-Agüero, A.; Matute-Llorente, Á.; Gómez-Cabello, A.; Casajús, J.A.; Vicente-Rodríguez, G. Effects of Whole Body Vibration Training on Body Composition in Adolescents with Down Syndrome. Res. Dev. Disabil. 2013, 34, 1426–1433. [Google Scholar] [CrossRef]
- Moraru, C.; Hodorca, R.M.; Vasilescu, D. The Role of Gymnastics and Dance in Rehabilitating Motor Capacities in Children with Down Syndrome. Sport Soc. 2014, 14, 102–112. [Google Scholar]
- Adamo, E.K.; Wu, J.; Wolery, M.; Hemmeter, M.L.; Ledford, J.R.; Barton, E.E. Using Video Modeling, Prompting, and Behavior-Specific Praise to Increase Moderate-to-Vigorous Physical Activity for Young Children with Down Syndrome. J. Early Interv. 2015, 37, 270–285. [Google Scholar] [CrossRef]
- Kashi, A.; Sheikh, M.; Dadkhah, A.; Hemayattalab, R.; Arabameri, E. The Effect of “Kashi Practices” on the Improvement of Psycho-Motor Skills in People with down Syndrome. Iran. Rehabil. J. 2015, 13, 13–21. [Google Scholar]
- Silva, V.; Campos, C.; Sá, A.; Cavadas, M.; Pinto, J.; Simões, P.; Machado, S.; Murillo-Rodríguez, E.; Barbosa-Rocha, N. Wii-based Exercise Program to Improve Physical Fitness, Motor Proficiency and Functional Mobility in Adults with Down Syndrome. J. Intellect. Disabil. Res. 2017, 61, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Ayán Pérez, C.; Cancela Carral, J.M.; Álvarez Costas, A.; Varela Martínez, S.; Martínez-Lemos, R.I. Water-Based Exercise for Adults with Down Syndrome: Findings from a Preliminary Study. Int. J. Ther. Rehabil. 2018, 25, 20–28. [Google Scholar] [CrossRef]
- Mohamed, R.A.; Mohamed, E.S.H.; Habshy, S.M.; Aly, S.M. Impact of Two Different Pulmonary Rehabilitation Methods in Children with Down Syndrome. J. Bodyw. Mov. Ther. 2021, 27, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Ringenbach, S.; Arnold, N.; Myer, B.; Hayes, C.; Nam, K.; Chen, C.-C. Executive Function Improves Following Acute Exercise in Adults with Down Syndrome. Brain Sci. 2021, 11, 620. [Google Scholar] [CrossRef] [PubMed]
- Camacho, R.; Castejón-Riber, C.; Requena, F.; Camacho, J.; Escribano, B.; Gallego, A.; Espejo, R.; De Miguel-Rubio, A.; Agüera, E. Quality of Life: Changes in Self-Perception in People with Down Syndrome as a Result of Being Part of a Football/Soccer Team. Self-Reports and External Reports. Brain Sci. 2021, 11, 226. [Google Scholar] [CrossRef] [PubMed]
- Di Fabrizio, G.; Parisi, M.C.; Crescimanno, C.; Orofino, F.; Frattalemi, M.; Mingrino, O.G.M. Global Postural Evaluation and Motor Treatment in the Subject with Down Syndrome: Clinical Case Reports. In Proceedings of the Journal of Human Sport and Exercise; Universidad de Alicante: San Vicente del Raspeig, Spain, 2021; Volume 16, pp. S938–S962. [Google Scholar]
- Hojlo, M.A.; Milliken, A.L.; Baumer, N.T.; Davidson, E.J. DSFit: A Feasibility Pilot Study of a Group Exercise Programme for Adolescents with Down Syndrome. J. Intellect. Disabil. Res. 2022, 66, 952–966. [Google Scholar] [CrossRef]
- Perić, D.B.; Milićević-Marinković, B.; Djurović, D. The Effect of the Adapted Soccer Programme on Motor Learning and Psychosocial Behaviour in Adolescents with Down Syndrome. J. Intellect. Disabil. Res. 2022, 66, 533–544. [Google Scholar] [CrossRef]
- Benavides Pando, E.V.; Delgado Valles, C.; Ornelas Contreras, M.; Jiménez Lira, C. Actividad Física En Jóvenes Con Síndrome de Down. Retos 2023, 50, 415–420. [Google Scholar]
- Page, Z.E.; Barrington, S.; Edwards, J.; Barnett, L.M. Do Active Video Games Benefit the Motor Skill Development of Non-Typically Developing Children and Adolescents: A Systematic Review. J. Sci. Med. Sport 2017, 20, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Flynn, R. Therapeutic Uses of Active Videogames: A Systematic Review. Games Health J. 2014, 3, 351–365. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Burghardt, A.R.; Lloyd, M.; Tiernan, C.; Hornyak, J.E. Physical Activity Benefits of Learning to Ride a Two-Wheel Bicycle for Children with Down Syndrome: A Randomized Trial. Phys. Ther. 2011, 91, 1463–1477. [Google Scholar] [CrossRef]
- Rimmer, J.H.; Heller, T.; Wang, E.; Valerio, I. Improvements in Physical Fitness in Adults with Down Syndrome. Am. J. Ment. Retard. 2004, 109, 165. [Google Scholar] [CrossRef] [PubMed]
- Bartlo, P.; Klein, P.J. Physical Activity Benefits and Needs in Adults with Intellectual Disabilities: Systematic Review of the Literature. Am. J. Intellect. Dev. Disabil. 2011, 116, 220–232. [Google Scholar] [CrossRef]
- Frey, G.C.; Temple, V.A.; Stanish, H.I. Interventions to Promote Physical Activity for Youth with Intellectual Disabilities. Salud Publ. M. 2017, 59, 437. [Google Scholar] [CrossRef]
- Hardee, J.P.; Fetters, L. The Effect of Exercise Intervention on Daily Life Activities and Social Participation in Individuals with Down Syndrome: A Systematic Review. Res. Dev. Disabil. 2017, 62, 81–103. [Google Scholar] [CrossRef] [PubMed]
- Romero Ibarra, O.; López Obregón, M.; Ladinez Garces, J. Actividad Física, El Deporte y La Recreación En La Inclusión En Niños Con Discapacidad. Rev. Ecuat. Psicol. 2019, 1, 24–35. [Google Scholar] [CrossRef]
- Matute-Llorente, A.; González-Agüero, A.; Gómez-Cabello, A.; Vicente-Rodríguez, G.; Casajús, J.A. Physical Activity and Cardiorespiratory Fitness in Adolescents with Down Syndrome. Nutr. Hosp. 2013, 28, 1151–1155. [Google Scholar] [CrossRef]
- Cowley, P.M.; Ploutz-Snyder, L.L.; Baynard, T.; Heffernan, K.S.; Young Jae, S.; Hsu, S.; Lee, M.; Pitetti, K.H.; Reiman, M.P.; Fernhall, B. The Effect of Progressive Resistance Training on Leg Strength, Aerobic Capacity and Functional Tasks of Daily Living in Persons with Down Syndrome. Disabil. Rehabil. 2011, 33, 2229–2236. [Google Scholar] [CrossRef]
- Ptomey, L.T.; Szabo-Reed, A.N.; Martin, L.E.; Mayo, M.S.; Washburn, R.A.; Gorczyca, A.M.; Lepping, R.J.; Lee, P.; Forsha, D.E.; Sherman, J.R.; et al. The Promotion of Physical Activity for the Prevention of Alzheimer’s Disease in Adults with Down Syndrome: Rationale and Design for a 12 Month Randomized Trial. Contemp. Clin. Trials Commun. 2020, 19, 100607. [Google Scholar] [CrossRef]
- Salse-Batán, J.; Sanchez-Lastra, M.A.; Suárez-Iglesias, D.; Ayán-Pérez, C. Effects of Exercise Training on Obesity-related Parameters in People with Intellectual Disabilities: Systematic Review and Meta-analysis. J. Intellect. Disabil. Res. 2022, 66, 413–441. [Google Scholar] [CrossRef]
- Haigh, A.; Lee, D.; Shaw, C.; Hawthorne, M.; Chamberlain, S.; Newman, D.W.; Clarke, Z.; Beail, N. What Things Make People with a Learning Disability Happy and Satisfied with Their Lives: An Inclusive Research Project. J. Appl. Res. Intellect. Disabil. 2013, 26, 26–33. [Google Scholar] [CrossRef]
- Walseth, K. Bridging and Bonding Social Capital in Sport—Experiences of Young Women with an Immigrant Background. Sport Educ. Soc. 2008, 13, 1–17. [Google Scholar] [CrossRef]
- Lensen, S. When to Pool Data in a Meta-Analysis (and When Not To)? Fertil. Steril. 2023, 119, 902–903. [Google Scholar] [CrossRef] [PubMed]
- Escrig Sos, V.J.; Llueca Abella, J.A.; Granel Villach, L.; Bellver Oliver, M. Metaanálisis: Una Forma Básica de Entender e Interpretar Su Evidencia. Rev. Senol. Patol. Mamar. 2021, 34, 44–51. [Google Scholar] [CrossRef]


{kind=link}
| SCOPUS | ((TITLE-ABS-KEY (“síndrome de down”) OR TITLE-ABS-KEY (“Down Syndrome”))) AND ((TITLE-ABS-KEY (autonomía) OR TITLE-ABS-KEY (autonomy) OR TITLE-ABS-KEY (“calidad de vida”) OR TITLE-ABS-KEY (“quality of life”) OR TITLE-ABS-KEY (wellbeing) OR TITLE-ABS-KEY (bienestar))) AND ((TITLE-ABS-KEY (sport) OR TITLE-ABS-KEY (deporte) OR TITLE-ABS-KEY (“physical activity”) OR TITLE-ABS-KEY (“actividad física”))) AND PUBYEAR > 2007 AND PUBYEAR < 2024 AND (LIMIT-TO (DOCTYPE, “ar”)) AND (LIMIT-TO (LANGUAGE, “English”) OR LIMIT-TO (LANGUAGE, “Spanish”)) | |
| Web of Science | 1. TITLE-ABS-KEY (“syndrome down” OR “sindrome de down”) 2. TITLE-ABS-KEY (autonomía OR autonomy OR “calidad de vida” OR “quality of life” OR bienestar OR wellbeing) 3. TITLE-ABS-KEY (sport OR “physical activity” OR “actividad fisica”) 4. #1 AND #2 AND #3 | |
| MEDLINE (PubMed) | MeSH Terms and Text Word | ((((“Down Syndrome”[Text Word]) OR “Down Syndrome”[MeSH Terms])) AND ((((((autonomy[Text Word]) OR “quality of life”[MeSH Terms]) OR “quality of life”[Text Word]) OR “autonomy, personal”[MeSH Terms]) OR wellbeing[MeSH Terms]) OR wellbeing[Text Word])) AND ((((sport[MeSH Terms]) OR sport[Text Word]) OR “physical activity”[MeSH Terms]) OR “physical activity”[Text Word]) |
| Title/Abstract | (((((sport[Title/Abstract]) OR (deporte[Title/Abstract])) OR (“actividad física”[Title/Abstract])) OR (“physical activity”[Title/Abstract])) AND ((((((autonomía[Title/Abstract]) OR (autonomy[Title/Abstract])) OR (“calidad de vida”[Title/Abstract])) OR (“quality of life”[Title/Abstract])) OR (wellbeing[Title/Abstract])) OR (bienestar[Title/Abstract]))) AND ((“síndrome de down”[Title/Abstract]) OR (“Down Syndrome”[Title/Abstract])) | |
| SportDiscus | S1. SU “Down Syndrome” OR SU “síndrome de down” S2. SU autonomy OR SU autonomía OR SU “calidad de vida” OR SU “quality of life” OR SU wellbeing OR SU bienestar S3. SU deporte OR SU sports OR SU “actividad física” OR SU “physical activity” S4. (SU deporte OR SU sports OR SU “actividad física” OR SU “physical activity”) AND (S1 AND S2 AND S3) | |
| Study | 1. Cohort | 2. Control or Comparison Group | 3. Pre-post Intervention Data | 4. Random Assignment of Participants to the Intervention | 5. Random Selection of Participants for Assessment | 6. Follow-up Rate of 80% or More | 7. Comparison Groups Equivalent on Sociodemographics | 8. Comparison Groups Equivalent at Baseline |
|---|---|---|---|---|---|---|---|---|
| González-Agüero et al. [35] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Moraru et al. [36] | Yes | No | Yes | NA | No | Yes | NA | NA |
| Adamo et al. [37] | Yes | Yes | Yes | No | Yes | Yes | NR | Yes |
| Kashi et al. [38] | Yes | Yes | Yes | Yes | No | Yes | NR | Yes |
| Silva et al. [39] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Ayán Pérez et al. [40] | Yes | No | Yes | NA | No | Yes | NA | NA |
| Mohamed et al. [41] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Ringenbach et al. [42] | Yes | Yes | Yes | Yes * | No | Yes | Yes | Yes |
| Camacho et al. [43] | No | Yes | No | No | No | NA | Yes | NR |
| Di Fabrizio et al. [44] | Yes | No | Yes | NA | No | Yes | NA | NA |
| Hojlo et al. [45] | Yes | No | Yes | NA | No | Yes | NA | NA |
| Perić et al. [46] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Benavides Pando et al. [47] | Yes | No | Yes | NA | No | No | NA | NA |
| Study | Sample Characteristics | Intervention | Outcomes (Measurement Tool) | Results |
|---|---|---|---|---|
| González-Agüero et al. [35] | Sample size (n pre/post; sex) 30/24; 7 female Distribution: group; sex; age (years)
| IG: 20 weeks of WBV training
NR | Height (stadiometer) Weight (stadiometer) BMI (kg/m2) Pubertal development (specific observation scale) Fat mass (dual energy X-ray absorptiometry) Lean mass (dual energy X-ray absorptiometry) | IG adherence (%); mean attendance (%): 80%; 80% (final sample) Significant results: IG showed a higher percent declination in fat mass at the upper limbs than CG (p < 0.05) Positive (not statistically significant) results: IG showed a tendency toward a higher percent increase in whole body lean body mass (p = 0.08) Negative results/no changes: No significant group by time interactions were found for any variable after intervention (all p > 0.05) |
| Moraru et al. [36] | Sample size [n pre/post; sex; age (years)] 3/3; NR; 10–14 years | IG: 8 months of a gymnastics and dance training program
| Lower limb strength (timed sit to stand test) Spine mobility (seated forward functional reach test) Core strength (partial sit-up test) Unipodal balance (single leg stance—eyes closed test) | IG adherence (%); mean attendance (%): 100%; NR Positive (not statistically significant) results: Enhancement of the scores of IG in the four outcomes post-intervention |
| Adamo et al. [37] | Sample size [n pre/post; sex; age (years)] 3/3; 1 female; 4.11 ± 1.03 | IG: Packaged intervention including peer video modeling, prompting, and behavior-specific praise from an adult Experimental A-B-A-B withdrawal design: Baseline 1 (7 days), Intervention 1 (9 days), Baseline 2 (4 days), Intervention 2 (7 days)
| MVPA (specific observation scale) | IG adherence (%); mean attendance (%): 100%; 98.6% Positive (not statistically significant) results: MVPA increased during the intervention and decreased when the intervention was withdrawn for all participants. MVPA levels in the second baseline did not decrease to the level of the first baseline for any participant |
| Kashi et al. [38] | Sample size [n pre/post; sex; age (years)] 28/24; no females; 29.19 ± 3.93 Distribution:
| IG: 12 weeks of Kashi practices Combination of cardiovascular exercise and strength, balance, and flexibility training
Same conditions (i.e., eating, physical activity, sleeping and participation in the educational program) No exercise or physical activity training | Reaction time (specific subscale of BOTMP) Agility (specific subscale of BOTMP) Balance (specific subscale of BOTMP) Running speed (45 m running test) Power (vertical and long jump) Strength (wrist and trunk dynamometry) Muscular endurance (push-up test, long and sit test) | IG adherence (%); mean attendance (%): 85%; NR Significant results: Pre-test differences between IG and CG were not statistically significant [Wilks’ Lambda = 0.771, f(6,17) = 0.843, p = 0.554], but post-test differences were significant [Wilks’ Lambda = 0.428, f(6,17) = 3.8 = 787, p = 0.014]. After intervention, there were significant improvements in IG in all the outcomes (p < 0.01). CG did not show any significant improvements (p > 0.05) |
| Silva et al. [39] | Sample size [n pre/post; sex; age (years)] 27/25; NR; 18–60 years Distribution:
| IG: 2-month Wii-based exercise program included in regular occupational therapy program
Usual daily activities in the occupational therapy program | Height (stadiometer) Waist circumference (anthropometric tape) Weight (segmental body composition analyzer) BMI (segmental body composition analyzer) Body fat % (segmental body composition analyzer) Visceral fat (segmental body composition analyzer) Muscle mass (segmental body composition analyzer) Coordination (plate tapping test, beanbag overhead throw test) Strength (handgrip test) Running speed and agility (shuttle run test) Balance (flamingo test) Flexibility (sit and reach test) Power (standing broad jump test) Muscular endurance (30 s sit-ups test, bent arm hang test) Aerobic endurance (6-minute walk test) Functional mobility (timed up and go test) Reaction time (specific subscale of BOTMP) | IG adherence (%); mean attendance (%): 93%; NR Significant results: There were significant group by time interactions on flexibility (p = 0.027), lower limbs power (p = 0.003), and aerobic endurance (p = 0.005). There were also significant main effects for time on waist circumference (p = 0.009), handgrip strength (p = 0.004), lower limbs power (p < 0.001), reaction time (p = 0.034) and left-handed coordination (p = 0.040). There were also significant improvements in IG on waist circumference (p = 0.008), handgrip strength (p = 0.025), flexibility (p = 0.014), lower limbs power (p < 0.001), aerobic endurance (p = 0.003) and reaction time (p = 0.028). Participants from CG also improved handgrip strength (p = 0.039). Significant differences were also found between IG and CG (IG improved, CG did not) on coordination (p = 0.045), core resistance (p = 0.040), functional mobility (p = 0.049), visceral fat (p = 0.036) and running speed and agility (p = 0.014) Positive (not statistically significant) results: There was a trend towards significant differences between IG and CG on body weight (p = 0.059) Negative results/no changes: There were no significant interactions or main effects for body fat percentage, muscle mass and right-handed coordination |
| Ayán Pérez et al. [40] | Sample size [n pre/post; sex; age (years)] 14/14; 7 female; 37.07 ± 7.34 | IG: 12 weeks of water-based physical exercise training sessions
| Height (NR) Weight (NR) BMI (NR) Waist circumference (NR) Body composition (triceps and subscapular skinfolds) Cardiorespiratory fitness (20 m shuttle run test) Agility (4 × 10 m shuttle run test) Strength (handgrip test) Power (standing broad jump test) Swimming ability (specific observation scale) Quality of life (specific questionnaire) | IG adherence (%); mean attendance (%): 100%; >85% Positive (not statistically significant) results: IG increased 6 s in the cardiorespiratory fitness test (151.57 ± 66.70 vs. 157.50 ± 64.89) and reduced approximately 3 s in the agility test (30.16 ± 7.20 vs. 27.75 ± 5.20) Negative results/no changes: No significant changes were observed for any outcome |
| Mohamed et al. [41] | Sample size (n pre/post; sex) 45/45; 24 female Distribution: group; sex; age (years)
| IG1: 12 weeks of aerobic exercise in cycle ergometer + PNF of the respiratory muscles Aerobic exercise in cycle ergometer
12 weeks of aerobic exercise in cycle ergometer + IMT Aerobic exercise in cycle ergometer: described in IG1 IMT training
12 weeks of aerobic exercise in cycle ergometer (described in IG1) | Respiratory muscle strength—MIP and MEP (respiratory pressure meter) Ratio of the upper to lower chest wall (anteroposterior chest radiograph) Pulmonary function—vital capacity, forced expiratory volume in 1 s, peak expiratory flow rate, maximum voluntary ventilation (spirometry) Aerobic endurance (6-minute walk test) | IG adherence (%); mean attendance (%): 100%; NR Significant results: There was a significant interaction of treatment and time (Wilks’ Lambda = 0.06; F (16, 70) = 13.27, p = 0.001, h2 = 0.75). There also was a significant main effect of time (Wilks’ Lambda = 0.02; F (8, 35) = 157.28, p = 0.001, h2 = 0.97) and treatment (Wilks’ Lambda = 0.17; F (16, 70) = 6, p = 0.001, h2 = 0.57). IG1 and IG2 showed an increase in all outcomes post-test (p < 0.001), while CG only increased MIP, MEP, ratio of upper to lower chest wall, vital capacity, peak expiratory flow rate, and aerobic endurance (p < 0.05). Mean differences between pre and post treatment were greater than MCID in IG1 and IG2, and smaller in CG. There was a significant increase in all outcomes in IG1 compared with IG2 (p < 0.05) and CG (p < 0.001), and in IG2 compared with CG (p < 0.05) |
| Ringenbach et al. [42] | Sample size [n pre/post; sex; age (years)] 14/14; 6 female; 26.25 ± 5.17 | Block randomization into three different training sessions 4 total sessions (first session consisted on pre-test assessment) IG1: Resistance training session
Assisted cycling therapy
No training
| Heart rate (heart rate device) Inhibition control (Eriksen Flanker Task test) Cognitive planning (Tower of London test) | IG adherence (%); mean attendance (%): 100%; 100% Significant results: For cognitive planning, there was a significant interaction between intervention and time [F(2,20) = 3.08, p = 0.034]. There also was a main effect of time [t(10) = −1.99, p = 0.038] in CG Positive (not statistically significant) results: For inhibition control, there was a trend towards significance for the main effect of time [F(1,12) = 1.062, p = 0.16] on the percent correct responses in all interventions, and for the main effect of time [t(13) = −1.1, p = 0.15] on inhibition time in IG2. There was also a non-significant reduction in inhibition time on IG1 Negative results/no changes: Inhibition time increased in CG. No differences found on cognitive planning in IG1 and IG2. |
| Camacho et al. [43] | Sample size [n pre/post; sex; age (years)] 39/39 adults with DS; 15 female; 29 ± 3 39 informants (parents/teachers) Distribution (adults with DS):
| IG: Two physical education sessions/week + two 90 min soccer training sessions/week Physical education sessions
Two physical education sessions/week (described in IG) | Quality of life—self-determination, rights, emotional well-being, material well-being, physical well-being, social inclusion, interpersonal relationships, personal development, and Quality of Life Index (specific questionnaire) | IG adherence (%); mean attendance (%): 100%; NR Significant results: A statistically significant correlation (r = −0.353; p = 0.027) with moderate magnitude and negative meaning between age and IG results on physical well-being. IG perceptions showed significant sex differences (men > women) on emotional well-being (Z = −2.29; p = 0.022), material well-being (Z = −2.29; p = 0.022), and personal development (Z = −2.20; p = 0.028), and group differences (IG > CG) in all outcomes (p < 0.001). Informants perceptions also indicated significant differences between genders (men > women) on social inclusion (Z = −2.49; p = 0.013), emotional well-being (Z = −2.29; p = 0.022), physical well-being (Z = −2.45; p = 0.014), material well-being (Z = −3.88; p < 0.001), and Quality of Life Index (Z = −2.84; p = 0.004). Results of IG were significantly higher that informants results on social inclusion (Z =−2.89; p = 0.004), self-determination (Z = −4.25; p = 0.001), material well-being (Z = −2.88; p = 0.004), personal development (Z = −2.39; p = 0.017), and Quality of Life Index (Z = −3.27; p = 0.001) Negative results/no changes: No correlations between age and IG or informants results on any outcome (except for physical well-being). No sex differences were detected in IG perceptions on self-determination, rights, physical well-being, social inclusion, interpersonal relationships, and Quality of Life Index, and in informants perceptions on self-determination, rights, interpersonal relationships, and personal development. No group differences were found for any outcome in informants perceptions. There was no difference between IG and informants perceptions on rights, emotional well-being, physical well-being, and interpersonal relationships |
| Di Fabrizio et al. [44] | Sample size [n pre/post; sex; age (years)] 10/10; 3 female; 26.5 ± 7.59 | IG: 10 months of adapted physical activity protocols
| Posture (computerized videography) Baropodometry—plantar surface, pressure, force, and load distribution (baropodometric platform) | IG adherence (%); mean attendance (%): 100%; NR Positive (not statistically significant) results: Results showed a reduction in podalic overload points and a better distribution of the podalic load on both feet, both as regards the ratio of both feet and as regards the distribution between forefoot and rearfoot. Seven participants also improved in terms of joint degrees, position of the hip, knee, ankle, and foot joints, as well as a reduced pelvic anteversion and knee and rearfoot valgism, and an elevation of the plantar vault |
| Hojlo et al. [45] | Sample size (n pre/post; sex) 13/12; 8 female Distribution: group; sex; age (years)
| Two iterations of DSFit, a structured group exercise program for adolescents with DS with weekly meetings and independent home exercise sessions
| Height (stadiometer) Weight (scale) BMI (NR) Muscular strength and endurance (overhead/wall squat test, Sit to Stand test, modified Push-Up test, bird dog time, Trunk Lift test, plank time, Curl Up test, dynamometry) Flexibility (shoulder stretch, Sit and Reach test) Balance and gait (Timed Up and Go test) Aerobic endurance (6-min Walk Test) Goal setting (specific final survey) Feedback (specific final survey) Anxiety and depression (specific questionnaire) Hyperactivity and impulsivity (specific questionnaire) | IG adherence (%); mean attendance (%): 92%; NR Positive (not statistically significant) results: Repeating participants data reported better healthy habits related to exercising, lower BMI and, in one of them, higher motivation and self-confidence. The majority of participants in IG1 and IG2 improved in at least one physical outcome. Anxiety and depression decreased or remained the same for the majority of participants, and hyperactivity and impulsivity decreased for almost all of them. Participants and parents started to set physical activity and health goals in their daily lives, acknowledging the importance of a healthy lifestyle; they also identified fun, a positive and social climate, meeting other families, and practicing walking, ball or dance/musical exercises as key aspects for participant satisfaction. Parents also perceived an improvement in independence of participants; the latter also expressed enjoyment in learning new exercises and being relational with other children Negative results/no changes: Height, weight, and resting heart rate did not significantly change for any cohort. Waiting and standing exercises were perceived by participants as dissatisfying |
| Perić et al. [46] | Sample size (n pre/post; sex) 25/25; sex NR Distribution: group; age (years)
| IG: Usual daily regime (no physical activity) + 16 weeks of adapted soccer program
Usual daily regime (no physical activity) | Aggression (specific observation scale) Attention disorders (specific observation scale) Anxiety and depression (specific observation scale) Social problems (specific observation scale) Soccer skills (Special Olympics soccer skills test) | IG adherence (%); mean attendance (%): 100%; 100% Significant results: Results showed a significant interaction effect of factors (time and group) for all psychosocial outcomes (aggression, Wilks’ Lambda = 0.501, F = 17.930, p < 0.001, ηp2 = 0.499; attention disorders, Wilks’ Lambda = 0.507, F = 17.519, p = 0.001, ηp2 = 0.493; anxiety and depression, Wilks’ Lambda = 0.518, F = 16.761, p = 0.001, ηp2 = 0.482; social problems, Wilks’ Lambda = 0.584, F = 12.800, p = 0.002, ηp2 = 0.416) and straight dribbling (Wilks’ Lambda = 0.278, F = 59.800, p < 0.001, ηp2 = 0.722). Significant improvements (p < 0.05) were also found in IG for all psychosocial outcomes and only for one soccer skill (straight dribbling). No changes were detected in CG for any outcome |
| Benavides Pando et al. [47] | Sample size [n pre/post; sex; age (years)] 26/18; 10 female; 17.44 ± 4.26 | IG: 10 weeks of adapted physical activity program based on cheerleading
| Strength (Handgrip test) Power (Standing Broad Jump test) Coordination (Plate Tapping test) Flexibility (Sit and Reach test) Running speed and agility (10 × 5 m Shuttle Run test) Muscular endurance (30-s Sit Up test) Balance (Flamingo test) | IG adherence (%); mean attendance (%): 69%; NR Significant results: Improvements in core resistance (p = 0.002), power in lower limbs (p = 0.021), coordination in right upper limb (p = 0.01), flexibility (p < 0.001), and running speed and agility (p < 0.001) Negative results/no changes: No changes in coordination in left upper limb, balance, and handgrip strength (all p > 0.05) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Llerena, A.; Ladrón-de-Guevara, L.; Medina-Rebollo, D.; Alcaraz-Rodríguez, V. Impact of Physical Activity on Autonomy and Quality of Life in Individuals with Down Syndrome: A Systematic Review. Healthcare 2024, 12, 181. https://doi.org/10.3390/healthcare12020181
Muñoz-Llerena A, Ladrón-de-Guevara L, Medina-Rebollo D, Alcaraz-Rodríguez V. Impact of Physical Activity on Autonomy and Quality of Life in Individuals with Down Syndrome: A Systematic Review. Healthcare. 2024; 12(2):181. https://doi.org/10.3390/healthcare12020181
Chicago/Turabian StyleMuñoz-Llerena, Antonio, Laura Ladrón-de-Guevara, Daniel Medina-Rebollo, and Virginia Alcaraz-Rodríguez. 2024. "Impact of Physical Activity on Autonomy and Quality of Life in Individuals with Down Syndrome: A Systematic Review" Healthcare 12, no. 2: 181. https://doi.org/10.3390/healthcare12020181
APA StyleMuñoz-Llerena, A., Ladrón-de-Guevara, L., Medina-Rebollo, D., & Alcaraz-Rodríguez, V. (2024). Impact of Physical Activity on Autonomy and Quality of Life in Individuals with Down Syndrome: A Systematic Review. Healthcare, 12(2), 181. https://doi.org/10.3390/healthcare12020181