
Effect of Periodontal Treatment in Patients with Periodontitis and Diabetes: Review of Systematic Reviews with Meta-Analyses in the Last Five Years



Abstract
1. Introduction
2. Materials and Methods
2.1. Registration and Description of Tools
2.2. Quality of Evidence
2.3. Data Sources and Bibliographic Search
2.4. Inclusion and Exclusion Criteria
2.5. Data Extraction
3. Results
3.1. Characteristics of Included Meta-Analyses
3.2. Quality of Evidence (GRADE System)
3.3. AMSTAR-2 Analysis
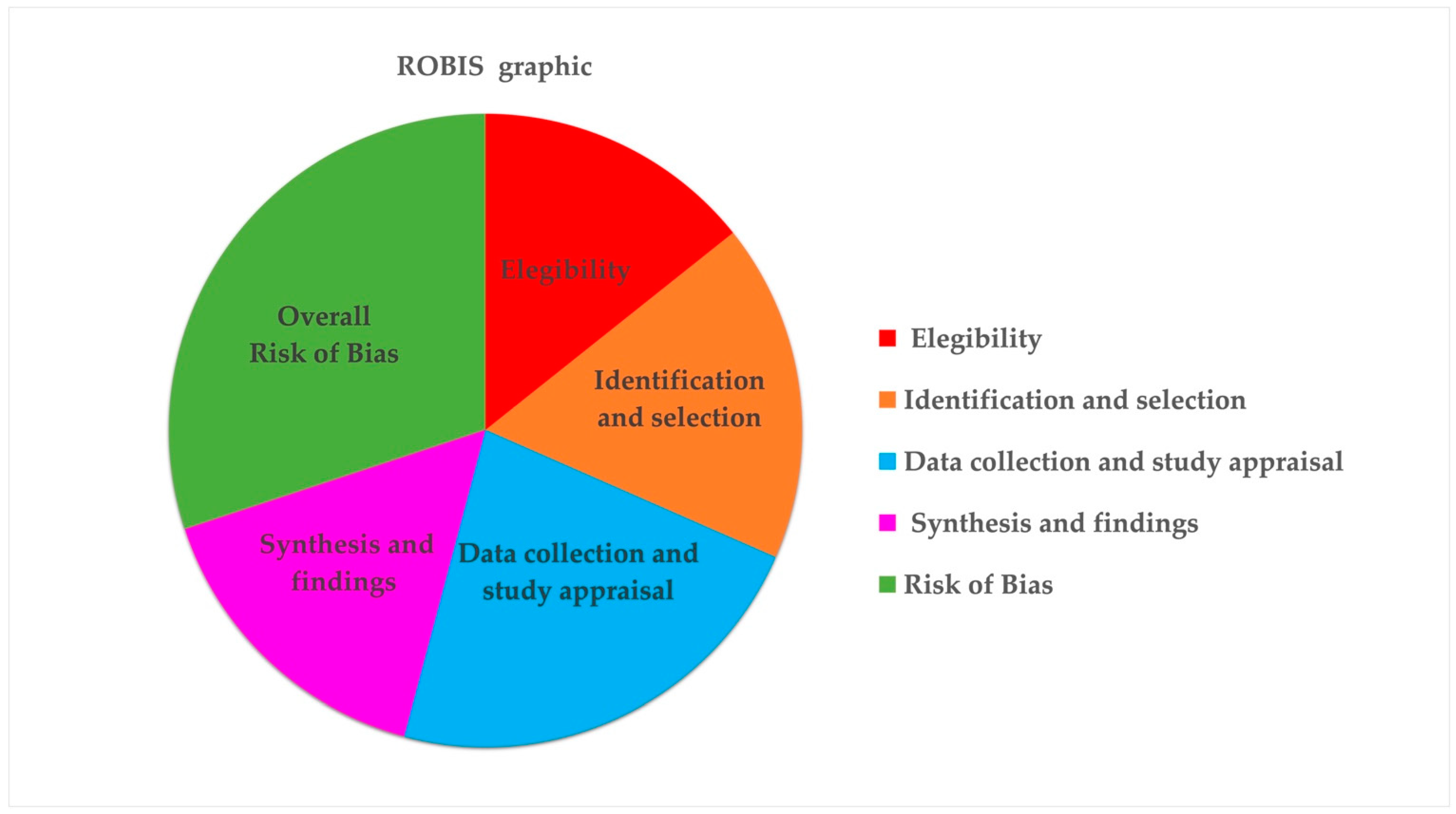
3.4. Analysis Using ROBIS Tool
4. Discussion
4.1. Antidiabetic Drugs
4.2. Antimicrobial Drugs
4.3. Lipid Metabolism
4.4. Biomodulation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed]
- Meyle, J.; Chapple, I. Molecular aspects of the pathogenesis of periodontitis. Periodontology 2000 2015, 69, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Diabetes as a potential risk for periodontitis: Association studies. Periodontology 2000 2020, 83, 40–45. [Google Scholar] [CrossRef]
- Parra-Torres, V.; Melgar-Rodríguez, S.; Muñoz-Manríquez, C.; Sanhueza, B.; Cafferata, E.A.; Paula-Lima, A.C.; Díaz-Zúñiga, J. Periodontal bacteria in the brain-Implication for Alzheimer’s disease: A systematic review. Oral Dis. 2023, 29, 21–28. [Google Scholar] [CrossRef]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Chavakis, T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat. Rev. Immunol. 2021, 21, 426–440. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.T.; Ngo, Q.T.; Tran, D.H.; Nguyen, T.T. Effect of Two Nonsurgical Periodontal Treatment Modalities in Type 2 Diabetes Mellitus Patients with Chronic Periodontitis: A Randomized Clinical Trial. J. Contemp. Dent. Pract. 2021, 22, 1275–1280. [Google Scholar] [CrossRef]
- Sundaram, S.G.; Ramakrishnan, T.; Krishnan, S.G.; Narayan, K.V.; Shankar, S.; Kanimozhi, G. Effect of Non-Surgical Periodontal Therapy on Systemic Inflammatory Markers, Glycemic Status and Levels of Proteinuria in Type 2 Diabetic and Non-Diabetic Patients with Chronic Periodontitis. Cureus 2023, 15, e44757. [Google Scholar] [CrossRef]
- Syed, N.K. Effects of Nonsurgical Periodontal Therapy on Glycemic Control in Diabetic Patients under Systemic Administration of Antidiabetic Ayurvedic Drug. J. Contemp. Dent. Pract. 2023, 24, 481–484. [Google Scholar] [CrossRef] [PubMed]
- Simpson, T.C.; Clarkson, J.E.; Worthington, H.V.; MacDonald, L.; Weldon, J.C.; Needleman, I.; Iheozor-Ejiofor, Z.; Wild, S.H.; Qureshi, A.; Walker, A.; et al. Treatment of periodontitis for glycaemic control in people with diabetes mellitus. Cochrane Database Syst. Rev. 2022, 4, CD004714. [Google Scholar]
- Moher, D.; Tetzlaff, J.; Tricco, A.C.; Sampson, M.; Altman, D.G. Epidemiology and reporting characteristics of systematic reviews. PLoS Med. 2007, 4, e78. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Cook, D.J.; Eastwood, S.; Olkin, I.; Rennie, D.; Stroup, D.F. Improving the quality of reports of meta-analyses of randomised controlled trials: The QUOROM statement. Quality of Reporting of Meta-analyses. Lancet 1999, 354, 1896–1900. [Google Scholar] [CrossRef]
- Moher, D.; Cook, D.J.; Eastwood, S.; Olkin, I.; Rennie, D.; Stroup, D.F. Improving the quality of reports of meta-analyses of randomised controlled trials: The QUOROM statement. QUOROM Group. Br. J. Surg. 2000, 87, 1448–1454. [Google Scholar] [CrossRef] [PubMed]
- Delaney, A.; Bagshaw, S.M.; Ferland, A.; Manns, B.; Laupland, K.B.; Doig, C.J. A systematic evaluation of the quality of meta-analyses in the critical care literature. Crit. Care 2005, 9, R575–R582. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS Group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef]
- Riley, R.D.; Hayden, J.A.; Steyerberg, E.W.; Moons, K.G.; Abrams, K.; Kyzas, P.A.; Malats, N.; Briggs, A.; Schroter, S.; Altman, D.G.; et al. Prognosis Research Strategy (PROGRESS) 2: Prognostic factor research. PLoS Med. 2013, 10, e1001380. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Malmivaara, A. Methodological considerations of the GRADE method. Ann. Med. 2015, 47, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, A.C.; Grisa, T.A.; Muniz, F.W.M.G.; Rösing, C.K.; Cavagni, J. Effect of adjuvant use of metformin on periodontal treatment: A systematic review and meta-analysis. Clin. Oral Investig. 2019, 23, 2659–2666. [Google Scholar] [CrossRef]
- Yap, K.C.H.; Pulikkotil, S.J. Systemic doxycycline as an adjunct to scaling and root planing in diabetic patients with periodontitis: A systematic review and meta-analysis. BMC Oral Health 2019, 19, 209. [Google Scholar] [CrossRef]
- Garde, S.; Akhter, R.; Nguyen, M.A.; Chow, C.K.; Eberhard, J. Periodontal Therapy for Improving Lipid Profiles in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 3826. [Google Scholar] [CrossRef]
- Cao, R.; Li, Q.; Wu, Q.; Yao, M.; Chen, Y.; Zhou, H. Effect of non-surgical periodontal therapy on glycemic control of type 2 diabetes mellitus: A systematic review and Bayesian network meta-analysis. BMC Oral Health 2019, 19, 176. [Google Scholar] [CrossRef]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, e20190248. [Google Scholar] [CrossRef] [PubMed]
- Corbella, S.; Calciolari, E.; Alberti, A.; Donos, N.; Francetti, L. Systematic review and meta-analysis on the adjunctive use of host immune modulators in non-surgical periodontal treatment in healthy and systemically compromised patients. Sci. Rep. 2021, 11, 12125. [Google Scholar] [CrossRef] [PubMed]
- Esteves Lima, R.P.; Atanazio, A.R.S.; Costa, F.O.; Cunha, F.A.; Abreu, L.G. Impact of non-surgical periodontal treatment on serum TNF-α levels in individuals with type 2 diabetes: A systematic review and meta-analysis. J. Evid. Based Dent. Pract. 2021, 21, 101546. [Google Scholar] [CrossRef]
- Zhao, P.; Song, X.; Wang, Q.; Zhang, P.; Nie, L.; Ding, Y.; Wang, Q. Effect of adjunctive diode laser in the non-surgical periodontal treatment in patients with diabetes mellitus: A systematic review and meta-analysis. Lasers Med. Sci. 2021, 36, 939–950. [Google Scholar] [CrossRef]
- Zhong, O.; Hu, J.; Wang, J.; Tan, Y.; Hu, L.; Lei, X. Antioxidant for treatment of diabetic complications: A meta-analysis and systematic review. J. Biochem. Mol. Toxicol. 2022, 36, e23038. [Google Scholar] [CrossRef]
- Corbella, S.; Calciolari, E.; Donos, N.; Alberti, A.; Ercal, P.; Francetti, L. Laser treatments as an adjunct to non-surgical periodontal therapy in subjects with periodontitis and type 2 diabetes mellitus: A systematic review and meta-analysis. Clin. Oral Investig. 2023, 27, 1311–1327. [Google Scholar] [CrossRef] [PubMed]
- Da Silva-Junior, P.G.B.; Abreu, L.G.; Costa, F.O.; Cota, L.O.M.; Esteves-Lima, R.P. The effect of antimicrobial photodynamic therapy adjunct to non-surgical periodontal therapy on the treatment of periodontitis in individuals with type 2 diabetes mellitus: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2023, 42, 103573. [Google Scholar] [CrossRef]
- Elnour, M.A.A.; Mirghani, H.O. Periodontitis treatment (surgical and nonsurgical) effects on glycemic control: A review and meta-analysis. Ann. Afr. Med. 2023, 22, 131–135. [Google Scholar] [CrossRef]
- Greggianin, B.F.; Marques, A.E.M.; Amato, A.A.; de Lima, C.L. Effect of periodontal therapy on insulin resistance in adults with dysglycemia and periodontitis: A systematic review and meta-analysis. Clin. Oral Investig. 2023, 27, 1329–1342. [Google Scholar] [CrossRef] [PubMed]
- Freire, B.L.; Abreu, L.G.; Costa, F.O.; Cota, L.O.M.; Esteves-Lima, R.P. Effect of photobiomodulation adjunct to periodontal therapy on individuals with type 2 diabetes mellitus regarding periodontal clinical parameters: A systematic review and meta-analysis. Lasers Med. Sci. 2023, 38, 116. [Google Scholar] [CrossRef]
- Carra, M.C.; Blanc-Sylvestre, N.; Courtet, A.; Bouchard, P. Primordial and primary prevention of peri-implant diseases: A systematic review and meta-analysis. J. Clin. Periodontol. 2023, 50, 77–112. [Google Scholar] [CrossRef]
- Oliveira, V.B.; Costa, F.W.G.; Haas, A.N.; Júnior, R.M.M.; Rêgo, R.O. Effect of subgingival periodontal therapy on glycaemic control in type 2 diabetes patients: Meta-analysis and meta-regression of 6-month follow-up randomized clinical trials. J. Clin. Periodontol. 2023, 50, 1123–1137. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, F.B.; Antoniazzi, R.P.; Oliveira, L.M.; Lietzan, A.D.; Miguez, P.A.; Susin, C. The efficacy of combining adjuvants with non-surgical periodontal therapy in individuals with type 2 diabetes: A Bayesian network meta-analysis. J. Clin. Periodontol. 2024, 51, 610–630. [Google Scholar] [CrossRef]
- Kang, S.; Liu, Z.Y.; Yuan, H.H.; Wang, S.M.; Pan, G.G.; Wei, W.; Jiang, Y.; Hou, Y. The impact of different states of type 2 diabetes when stratified by baseline HbA1c on the periodontal outcomes of non-surgical periodontal treatment: A systematic review and network meta-analysis. Int. J. Dent. Hyg. 2024, 22, 401–413. [Google Scholar] [CrossRef]
- Page, M.J.; Shamseer, L.; Altman, D.G.; Tetzlaff, J.; Sampson, M.; Tricco, A.C.; Catalá-López, F.; Li, L.; Reid, E.K.; Sarkis-Onofre, R.; et al. Epidemiology and Reporting Characteristics of Systematic Reviews of Biomedical Research: A Cross-Sectional Study. PLoS Med. 2016, 13, e1002028. [Google Scholar] [CrossRef]
- Hartling, L.; Vandermeer, B.; Fernandes, R.M. Systematic reviews, overviews of reviews and comparative effectiveness reviews: A discussion of approaches to knowledge synthesis. Evid.-Based Child Health 2014, 9, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Becker, L.A.; Oxman, A.D. Overviews of reviews. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: Oxford, UK, 2011; Volume 22, pp. 607–631. [Google Scholar]
- Hunt, H.; Pollock, A.; Campbell, P.; Estcourt, L.; Brunton, G. An introduction to overviews of reviews: Planning a relevant research question and objective for an overview. Syst. Rev. 2018, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.Y.; Łagosz-Ćwik, K.B.; Hogervorst, J.M.A.; Schoenmaker, T.; Grabiec, A.M.; Forouzanfar, T.; van der Weijden, F.A.; de Vries, T.J. Diabetes Medication Metformin Inhibits Osteoclast Formation and Activity in In Vitro Models for Periodontitis. Front. Cell Dev. Biol. 2022, 9, 777450. [Google Scholar] [CrossRef] [PubMed]
- Gu, M.; Wang, P.; Xiang, S.; Xu, D.; Jin, C.; Jiang, Z.; Hu, N. Effects of type 2 diabetes and metformin on salivary microbiota in patients with chronic periodontitis. Microb. Pathog. 2021, 161, 105277. [Google Scholar] [CrossRef]
- Sun, X.; Li, M.; Xia, L.; Fang, Z.; Yu, S.; Gao, J.; Feng, Q.; Yang, P. Alteration of salivary microbiome in periodontitis with or without type-2 diabetes mellitus and metformin treatment. Sci. Rep. 2020, 10, 15363. [Google Scholar] [CrossRef]
- Das, A.C.; Das, S.J.; Panda, S.; Sharma, D.; Taschieri, S.; Fabbro, M.D. Adjunctive Effect of Doxycycline with Conventional Periodontal Therapy on Glycemic Level for Chronic Periodontitis with Type 2 Diabetes Mellitus Subjects. J. Contemp. Dent. Pract. 2019, 20, 1417–1423. [Google Scholar]
- Alblowi, J.A.; Farid, Z.S.; Attia, M.S. Comparative Study of Azithromycin Versus Doxycycline Effect on the Resistin Level in Periodontitis Patients with Type 2 Diabetes: A Randomized Controlled Clinical Trial. Cureus 2024, 16, e54849. [Google Scholar] [CrossRef]
- Gaikwad, S.P.; Gurav, A.N.; Shete, A.R.; Desarda, H.M. Effect of scaling and root planing combined with systemic doxycycline therapy on glycemic control in diabetes mellitus subjects with chronic generalized periodontitis: A clinical study. J. Periodontal Implant Sci. 2013, 43, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Mugri, M.H. Efficacy of Systemic Amoxicillin-Metronidazole in Periodontitis Patients with Diabetes Mellitus: A Systematic Review of Randomized Clinical Trials. Medicina 2022, 58, 1605. [Google Scholar] [CrossRef]
- Zhou, L.J.; Lin, W.Z.; Meng, X.Q.; Zhu, H.; Liu, T.; Du, L.J.; Bai, X.B.; Chen, B.Y.; Liu, Y.; Xu, Y.; et al. Periodontitis exacerbates atherosclerosis through Fusobacterium nucleatum-promoted hepatic glycolysis and lipogenesis. Cardiovasc. Res. 2023, 119, 1706–1717. [Google Scholar] [CrossRef]
- Chen, Z.; Song, J.; Tang, L. Investigation on the association between serum lipid levels and periodontitis: A bidirectional Mendelian randomization analysis. BMC Oral Health 2023, 23, 827. [Google Scholar] [CrossRef] [PubMed]
- Kudiyirickal, M.G.; Pappachan, J.M. Periodontitis: An often-neglected complication of diabetes. World J. Diabetes 2024, 15, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Deandra, F.A.; Ketherin, K.; Rachmasari, R.; Sulijaya, B.; Takahashi, N. Probiotics and metabolites regulate the oral and gut microbiome composition as host modulation agents in periodontitis: A narrative review. Heliyon 2023, 9, e13475. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, K.; Farhadi, M.; Fekrazad, R.; Chaibakhsh, S.; Mahmoudian, S. Photobiomodulation therapy in mood disorders: A systematic review. Lasers Med. Sci. 2022, 37, 3343–3351. [Google Scholar] [CrossRef]
- Theodoro, L.H.; Marcantonio, R.A.C.; Wainwright, M.; Garcia, V.G. LASER in periodontal treatment: Is it an effective treatment or science fiction? Braz. Oral Res. 2021, 35, e099. [Google Scholar] [CrossRef]
- Jia, L.; Jia, J.; Xie, M.; Zhang, X.; Li, T.; Shi, L.; Shi, H.; Zhang, X. Clinical attachment level gain of lasers in scaling and root planing of chronic periodontitis: A network meta-analysis of randomized controlled clinical trials. Lasers Med. Sci. 2020, 35, 473–485. [Google Scholar] [CrossRef]
- Wu, C.Z.; Yuan, Y.H.; Liu, H.H.; Li, S.S.; Zhang, B.W.; Chen, W.; An, Z.J.; Chen, S.Y.; Wu, Y.Z.; Han, B.; et al. Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral Health 2020, 20, 204. [Google Scholar] [CrossRef] [PubMed]
- Borgnakke, W.S. Modifiable risk factors for periodontitis and diabetes. Curr. Oral Health Rep. 2016, 3, 254–269. [Google Scholar] [CrossRef]
- Timonen, P.; Suominen-Taipale, L.; Jula, A.; Niskanen, M.; Knuuttila, M.; Ylöstalo, P. Insulin sensitivity and periodontal infection in a non-diabetic, non-smoking adult population. J. Clin. Periodontol. 2011, 38, 17–24. [Google Scholar] [CrossRef]
- Blasco-Baque, V.; Garidou, L.; Pomié, C.; Escoula, Q.; Loubieres, P.; Le Gall-David, S.; Lemaitre, M.; Nicolas, S.; Klopp, P.; Waget, A.; et al. Periodontitis induced by Porphyromonas gingivalis drives periodontal microbiota dysbiosis and insulin resistance via an impaired adaptive immune response. Gut 2017, 66, 872–885. [Google Scholar] [CrossRef]
- Saeb, A.T.M.; Al-Rubeaan, K.A.; Aldosary, K.; Udaya Raja, G.K.; Mani, B.; Abouelhoda, M.; Tayeb, H.T. Relative reduction of biological and phylogenetic diversity of the oral microbiota of diabetes and pre-diabetes patients. Microb. Pathog. 2019, 128, 215–229. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Databases | Search Terms |
|---|---|
| PubMed/Medline | Periodontitis [Mesh] OR Periodontal AND Chronic Periodontitis [Mesh] OR Adult Periodontitis [Title/Abstract] OR Periodontal Disease* [Title/Abstract] OR Periodontal Pocket [Title/Abstract] OR Attachment Loss [Title/Abstract] OR Alveolar Bone Loss [Title/Abstract]; Periodontitis OR Etiology [Mesh]; Periodontitis AND Treatment [Mesh] OR Therapy OR Intervention [Mesh]; Periodontitis AND Diabetes Mellitus Type 2 OR T2DM [Text Word] OR Hyperglycemia [Text Word] OR Glycemic Control [Text Word] OR Glycosylated Hemoglobin [Text Word] OR Glycated Hemoglobin [Text Word]. |
| Embase | Periodontitis OR Periodontal Disease* AND Therapy OR Treatment [Mesh] AND Diabetes OR Diabetes Mellitus/prevention & control* OR Metabolic Control OR Glycemic Control [Mesh] OR Glycated Hemoglobin OR HbA1c OR Systemic Inflammation AND Humans [Mesh]. |
| Cochrane Central | Periodontitis OR Periodontal Disease* OR Periodontal Pocket OR Chronic Periodontitis OR Aggressive Periodontitis AND Periodontal Treatment [Mesh] OR Periodontal Therapy OR Periodontitis Therapy AND Diabetes mellitus Type 2 OR Hyperglycemia. |
| Dentistry & Oral Sciences | Periodontitis OR Periodontal Disease* AND Complications AND Treatment. Diabetes Mellitus Type 2 AND Periodontitis OR Periodontal Disease. |
| Web of Science | Periodontal Disease OR Periodontitis/Etiology AND Therapy AND Humans; Diabetes Complications* OR Hyperglycemia Complications; Diabetes Mellitus Type 2 Therapy OR Hyperglycemia Therapy. |
| Inclusion Criteria |
|---|
| 1. SRs with meta-analyses performed in adult subjects (≥18 years) with a diagnosis of periodontitis and type 2 diabetes. |
| 2. Outcome indicators: periodontal indices and/or glycemic level. |
| 3. RCTs. |
| Exclusion criteria |
| 1. SRs that did not include meta-analyses. |
| 2. SR that used only one database in its bibliographic search strategy |
| 3. Studies of predictive models or prognostic scales. |
| Study, Year | RCTs Evaluated | Subjects Included | Type of Participants | Pathologies Involved | Diagnostic Criteria | Conclusions |
|---|---|---|---|---|---|---|
| Nicolini et al. 2019 [22] | 3 | 206 | Adult patients (aged 30+ years) diagnosed with chronic periodontitis | Periodontitis | NR | The adjuvant use of metformin provides additional benefit to the results of NSPT. |
| Yap and Pulikkotil 2019 [23] | 6 | 276 | Patients diagnosed with periodontitis and diabetes mellitus | Periodontitis and DM | NR | Systemic doxycycline as an adjunct to NSPT does not significantly improve clinical attachment levels or the reduction in HbA1C levels in the treatment of diabetic patients with periodontitis. |
| Garde et al. 2019 [24] | 7 | 707 | Individuals with T2DM | Periodontitis; T2DM; lipid profiles | NR | Reduction in triglyceride levels by approximately 8% achieved by periodontitis treatment in patients with T2DM. |
| Cao et al. 2019 [25] | 14 | 629 | Adult patients (aged ≥ 30 years) with periodontitis and T2DM | Periodontitis and T2DM | NR | Periodontal treatment with laser aPDT + doxycline is effective in reducing HbA1c% in periodontitis in non-smokers without severe T2DM complications. |
| Baeza et al. 2020 [26] | 9 | 623 | Patients ≥ 18 years with a diagnosis of T2DM and periodontitis | Periodontitis and T2DM | T2DM according to the WHO criteria; periodontitis as defined by the authors. | Evidence of periodontal treatment in improving metabolic control and reducing systemic inflammation in patients with T2DM. |
| Corbella et al. (**) 2021 [27] | 27 | 2279 | Patients ≥ 18 years affected by periodontitis, both systemically healthy and systemically compromised | Periodontitis and systemic diseases | Criteria extracted from included articles by 3 independent reviewers | There is no strong scientific evidence to advise the application in clinical practice of modulatory therapies such as laser or photomodulatory therapy as an adjunct to nonsurgical periodontal therapy. |
| Esteves de Lima et al. 2021 [28] | 18 | 715 | Individuals with T2DM | Periodontitis and T2DM | WHO criteria | NSPT modifies serum TNF-α levels at 6 months in patients with T2DM. |
| Zhao et al. 2021 [29] | 9 | 376 | Patients diagnosed with DM and Chronic Periodontitis | Periodontitis and DM | NR | DL + NSPT provided additional benefits on periodontal parameters (PD and CAL) and HbA1c levels compared to NSPT alone. |
| Zhong et al. 2022 [30] | 36 | 3091 | Patients with DM | DM; nephropathy; nonalcoholic fatty liver disease; periodontitis | NR | The results of this study indicate that antioxidant therapy is effective in the treatment of the above three complications of diabetes (periodontitis, nephropathy and nonalcoholic fatty liver disease). |
| Corbella et al. (*) 2023 [31] | 11 | 504 | Patients ≥ 18 years of age with previously untreated periodontitis affected by controlled or uncontrolled T2DM. | Periodontitis and T2DM | T2DM according to the World Health Organization criteria; periodontitis as defined by Papapanou et al. (2018) and Armitage (2004) | Decrease in short-term HbA1C (results should be interpreted with caution due to small effect sizes and statistical heterogeneity). |
| Da Silva-Junior et al. 2023 [32] | 11 | 418 | Individuals with T2DM and periodontitis | Periodontitis and T2DM | NR | aPDT as an adjunct to NSPT contributes significantly to the reduction in Periodontitis in individuals with type T2DM. |
| Elnour and Mirghani 2023 [33] | 11 | 1469 | NR | Periodontitis and T2DM | NR | There is a slight association between periodontal treatment and glycemic control among patients with uncontrolled diabetes. Early detection and treatment of periodontitis is recommended to improve glycemic control. |
| Greggianin et al. 2023 [34] | 7 | 706 | Adults with prediabetes or T2DM and periodontitis | Periodontitis and T2DM | NR | Absence of effect between NSPT and insulin resistance. |
| Freire et al. 2023 [35] | 6 | 299 | Individuals with T2DM and periodontitis | Periodontitis and T2DM | NR | Photobiomodulation complementary to contributes to the improvement in periodontal clinical parameters in individuals with T2DM, with further reduction in PPD and improvements in CAL. |
| Carra et al. 2023 [36] | 48 | 909 | Adult patients awaiting dental implant placement or having dental implants with peri-implant health | Peri-implant diseases | NR | Primary prevention of peri-implantitis is based on regular glycemic control. In diabetic patients receiving dental implants, glycemic control is essential for primary prevention of peri-implantitis. |
| Oliveira et al. 2023 [37] | 11 | 1374 | Patients with T2DM and periodontitis | T2DM; periodontitis | NR | Subgingival periodontal treatment produces a clinically relevant improvement in glycemic control in patients with T2DM and periodontitis. |
| Zanatta et al. 2024 [38] | 72 | 1110 | Adult subjects ≥ 18 years diagnosed with T2DM and Periodontitis | Periodontitis and T2DM | Definitions of T2DM and periodontitis described in the publication. | The adjuvant use of systemic metronidazole or ALA appears to bring significant additional benefits to both periodontitis and HbA1c reduction after NSPT in patients with T2DM. |
| Kang et al. 2024 [39] | 10 | 566 | Patients with periodontitis; patients with poorly controlled periodontitis and T2DM; and patients with controlled periodontitis and T2DM. | Periodontitis and T2DM | NR | NSPT had the best therapeutic effect in patients without T2DM. |
| Study | Databases Consulted | Periodontal Intervention | Comparison | Intervention Effect | Meta-Analysis Software |
|---|---|---|---|---|---|
| Nicolini et al. [22] | MEDLINE-PubMed, Scopus and EMBASE | NSPT + metformin | NSPT alone or placebo | PPD; CAL; IBD | Stata 13.1 |
| Yap and Pulikkotil [23] | PubMed and Scopus | NSPT + doxycycline | NSPT alone | PPD; CAL; HbA1C | RevMan 5.3 |
| Garde et al. [24] | MEDLINE, EMBASE, PubMed, and WOS | Surgical or NSPT | NSPT or only supragingival scaling and polishing | PPD; BOP; TC; TG; LDL; HDL | NR |
| Cao et al. [25] | Pubmed, Embase, Cochrane Library and WOS | NSPT + adjuvant | No treatment | HbA1C | Network meta-analysis |
| Baeza et al. [26] | MEDLINE (PubMed) Cochrane Central Register of Controlled Trials | Conventional treatments, including oral hygiene instruction and SRP (with or without flap surgery) | Without periodontal treatment | HbA1C; CRP levels | RevMan 5.3 |
| Corbella et al. (**) [27] | MEDLINE/Pubmed, Scopus, ISI Web of Science, EMBASE and Cochrane Central | NSPT protocol combined with a systemically delivered host-modulator drugs | NSPT alone or in association with placebo | PPD; CAL; GI; PL; TNF-α; IL-1β | RevMan 5.3 |
| Esteves de Lima et al. [28] | PubMed, WOS, Scopus, Ovid and Lilacs | NSPT | Without periodontal treatment | BMI; HbA1C; Serum levels of TNF- α | RevMan 5.3 |
| Zhao et al. [29] | MEDLINE, EMBASE, Cochrane Central Register WOS and Chinese BioMedical Literature | NSPT + DL | NSPT or placebo | PPD; CAL; BOP; PL; HbA1C | RevMan 5.3 |
| Zhong et al. [30] | PubMed, Embase, The CENTRAL, WOS and Scopus | Antioxidant supplementation | NR | HbA1C; renal function; liver function; periodontitis | RevMan 5.4 |
| Corbella et al. (*) [31] | MEDLINE/PubMed, Scopus, (OVID) EMBASE, and Cochrane Central | NSPT + LT + PDT | NSPT + Placebo | PPD; CAL; CEJ; HbA1C; BOP; Extracted teeth during follow-up | RevMan 5.3 |
| Da Silva-Junior et al. [32] | PubMed, WOS, Cochrane, and LILACS | aPDT + NSPT | NSPT | BOP; PPD; CAL | NR |
| Elnour and Mirghani [33] | PubMed, Cochrane Library, and Google Scholar | NSPT | No treatment | HbA1C | RevMan 5.4 |
| Greggianin et al. [34] | PubMed, Embase, WOS, Scopus, Cochrane and LILACS. | NSPT | Pre-intervention insulin resistance parameters or with a group that did not receive NSPT | CAL; PPD; BOP; BMI; HbA1C | RevMan 5.4 |
| Freire et al. [35] | PubMed, WOS, Ovid, Cochrane, and LILACS | NSPT + Photobiomodulation | NSPT alone | BOP; PPD; CAL; HbA1C | NR |
| Carra et al. [36] | MEDLINE/PubMed, EMBASE, Cochrane Central Library, Base Search, Open Access Thesis and Dissertation (openthesis.org), and ClinicalTrials.gov | Preventive interventions | Patients who do not receive any preventive intervention | BOP; PPD; MBL | RevMan 5.3 |
| Oliveira et al. [37] | MEDLINE/PubMed, Scopus, Embase, WOS, Latin American and Caribbean Health Science Information—LILACS, Livivo, DOSS (through EBSCO host), CINAHL (through EBSCO host) and Cochrane Library | SPT or NSPT | No subgingival intervention | HbA1C; BMI; PPD; CAL | NR |
| Zanatta et al. [38] | MEDLINE/ PubMed, EMBASE, Cochrane Central, WOS and LILACS | NSPT + Metronidazole or ALA | No periodontal treatment or NSPT alone | PPD; CAL; BOP; HbA1C | Network meta-analysis |
| Kang et al. [39] | PubMed, Embase, and the Cochrane Central Register of Controlled Trails | NSPT with OHI | Normal and systemically healthy control group (without diabetes) but diagnosed only with periodontitis | PPD; CAL; BOP | Stata 14.2 |
| Study | Quality Level |
|---|---|
| Nicolini et al. [22] | Moderate |
| Yap and Pulikkotil [23] | Very Low |
| Garde et al. [24] | Moderate |
| Cao et al. [25] | Moderate |
| Baeza et al. [26] | High |
| Corbella et al. (**) [27] | Low |
| Esteves de Lima et al. [28] | High |
| Zhao et al. [29] | Moderate |
| Zhong et al. [30] | High |
| Corbella et al. (*) [31] | Moderate |
| Da Silva-Junior et al. [32] | Moderate |
| Elnour and Mirghani [33] | High |
| Greggianin et al. [34] | Very Low |
| Freire et al. [35] | High |
| Carra et al. [36] | Moderate |
| Oliveira et al. [37] | Moderate |
| Zanatta et al. [38] | Moderate |
| Kang et al. [39] | Very Low |
| Study | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Domain 6 | Domain 7 | Domain 8 | Domain 9 | Domain 10 | Domain 11 | Domain 12 | Domain 13 | Domain 14 | Domain 15 | Domain 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nicolini et al. [22] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Yap and Pulikkotil [23] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Garde et al. [24] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Cao et al. [25] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Baeza et al. [26] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Corbella et al. [27] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Esteves Lima et al. [28] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Zhao et al. [29] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Zhong et al. [30] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Corbella et al. [31] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Da Silva-Junior et al. [32] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Elnour and Mirghani [33] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Greggianin et al. [34] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Freire et al. [35] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Carra et al. [36] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Oliveira et al. [37] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Zanatta et al. [38] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Kang et al. [39] | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Phase 2 Concerns with Review Process | Phase 3 Risk of Bias in Review | ||||
|---|---|---|---|---|---|
| Study | Domain 1 (Study Eligibility Criteria) | Domain 2 (Identification and Selection of Studies) | Domain 3 (Data Collection and Study Appraisal) | Domain 4 (Synthesis and Findings) | |
| Nicolini et al. [22] |  | | ? | |  |
| Yap and Pulikkotil [23] | | ? | | | |
| Garde et al. [24] | | | | | |
| Cao et al. [25] | | | | | |
| Baeza et al. [26] | | ? | | | |
| Corbella et al. [27] | | | ? | | |
| Esteves Lima et al. [28] | | | ? | | |
| Zhao et al. [29] | | | | | |
| Zhong et al. [30] | | | | ? | |
| Corbella et al. [31] | | | ? | | |
| Da Silva-Junior et al. [32] | | | ? | | |
| Elnour and Mirghani [33] | ? | | ? | ? | |
| Greggianin et al. [34] | | | | | |
| Freire et al. [35] | | | | | |
| Carra et al. [36] | | | ? | ? | |
| Oliveira et al. [37] | | | | | |
| Zanatta et al. [38] | | | ? | | |
| Kang et al. [39] | | ? | | | |
Low risk; High risk; ? Unclear risk.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Valverde, N.; Rueda, J.A.B. Effect of Periodontal Treatment in Patients with Periodontitis and Diabetes: Review of Systematic Reviews with Meta-Analyses in the Last Five Years. Healthcare 2024, 12, 1844. https://doi.org/10.3390/healthcare12181844
López-Valverde N, Rueda JAB. Effect of Periodontal Treatment in Patients with Periodontitis and Diabetes: Review of Systematic Reviews with Meta-Analyses in the Last Five Years. Healthcare. 2024; 12(18):1844. https://doi.org/10.3390/healthcare12181844
Chicago/Turabian StyleLópez-Valverde, Nansi, and José Antonio Blanco Rueda. 2024. "Effect of Periodontal Treatment in Patients with Periodontitis and Diabetes: Review of Systematic Reviews with Meta-Analyses in the Last Five Years" Healthcare 12, no. 18: 1844. https://doi.org/10.3390/healthcare12181844
APA StyleLópez-Valverde, N., & Rueda, J. A. B. (2024). Effect of Periodontal Treatment in Patients with Periodontitis and Diabetes: Review of Systematic Reviews with Meta-Analyses in the Last Five Years. Healthcare, 12(18), 1844. https://doi.org/10.3390/healthcare12181844