
Exploring the Mediating Role of Self-Regulation in Bullying Victimization and Depressive Symptoms among Adolescents: A Cross-Regional and Gender Analysis


Abstract
1. Introduction
- Correlation Hypothesis: Bullying victimization has a positive correlation with depression. It was hypothesized that an adverse life event that potentially poses a threat to the mental development of adolescents and contributes to the development of depression;
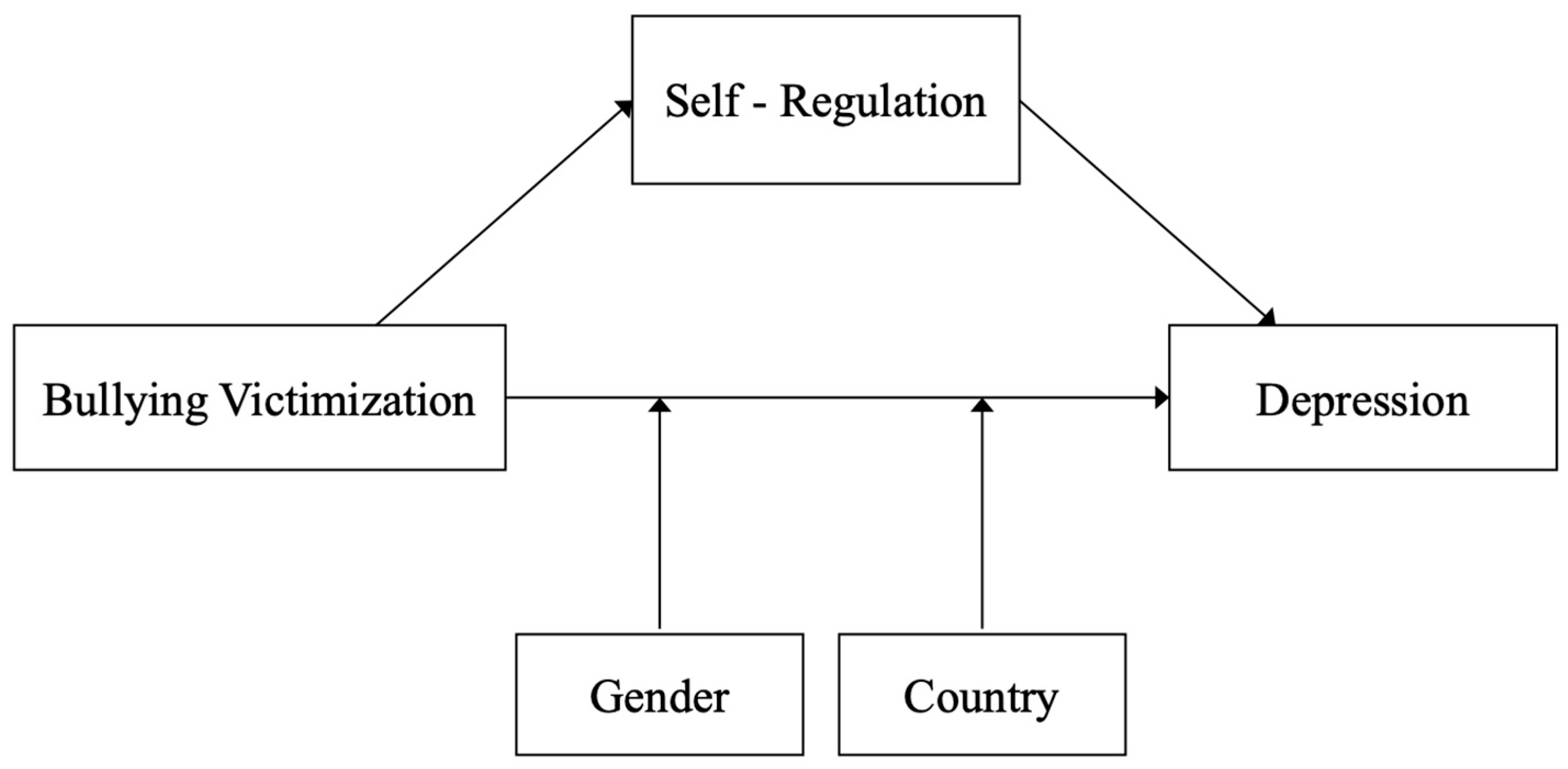
- Mediation Hypothesis: Self-regulation mediates the association between bullying victimization and depressive symptoms among adolescents. It was hypothesized that self-regulation would serve as a mechanism through which the experience of bullying victimization influences the development of depressive symptoms such that lowering levels of self-regulation would amplify the impact of bullying victimization on depressive symptoms;
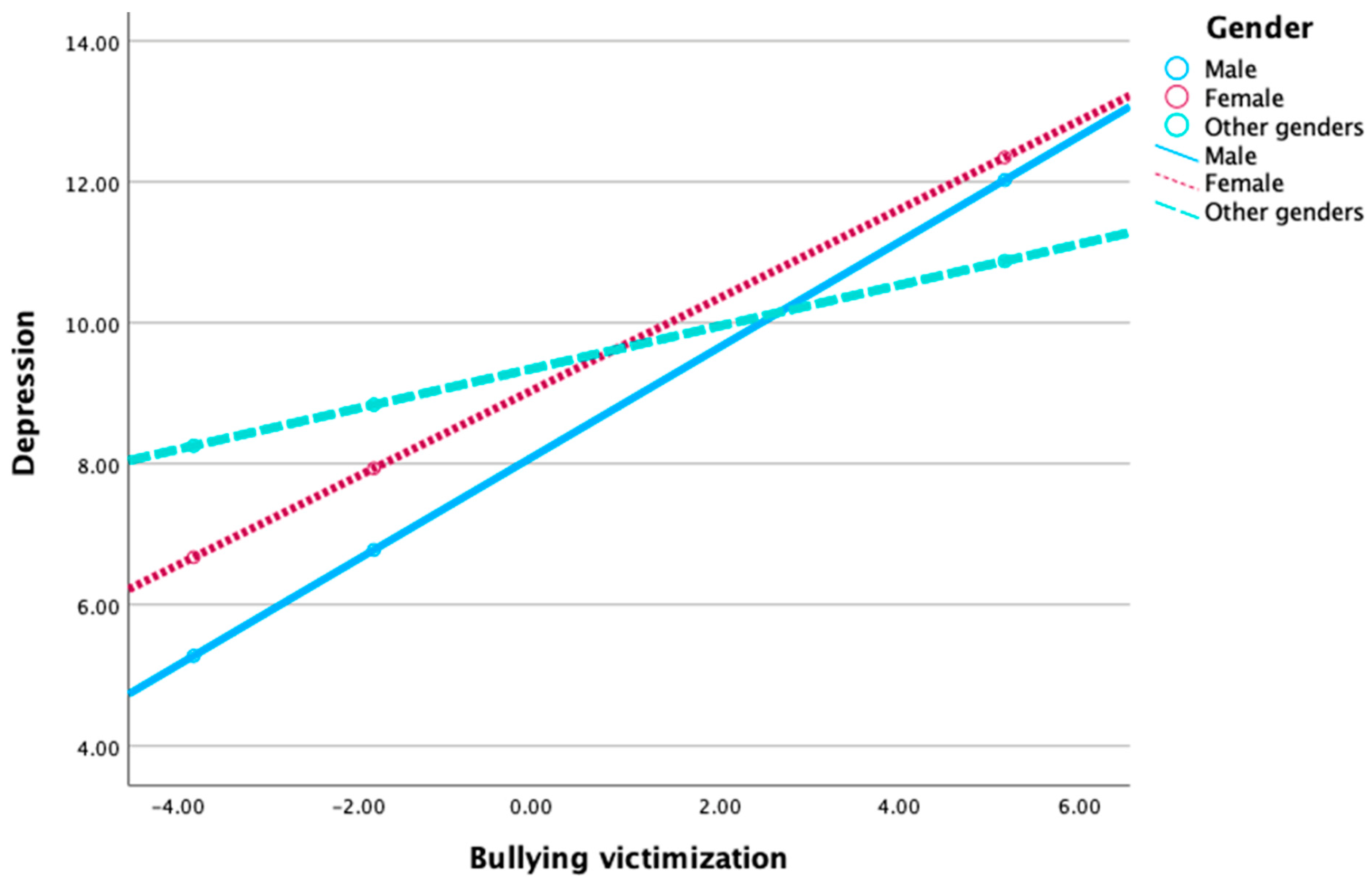
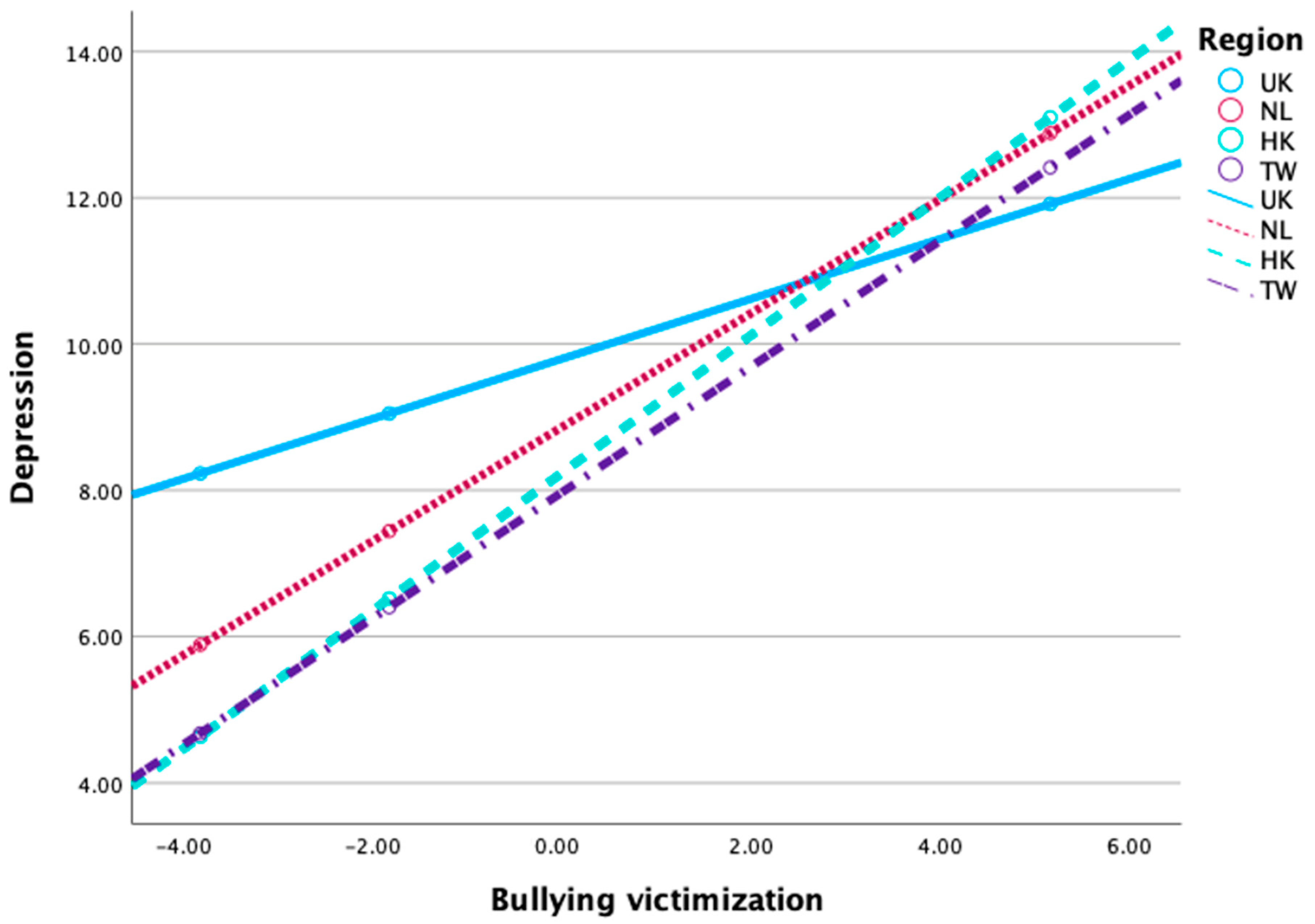
- Moderation Hypothesis: Gender and region moderate the relationship between bullying victimization and depressive symptoms. Specifically, it was hypothesized that the association between bullying victimization and depressive symptoms would vary depending on gender and region. For instance, males may exhibit a stronger association between bullying victimization and depressive symptoms compared to females, and the strength of this association may differ across regions.
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Correlational Analyses
3.2. Mediation Analyses
3.3. Cross-Region and Gender Comparisons: Moderation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kessler, R.C.; Avenevoli, S.; Merikangas, K.R. Mood disorders in children and adolescents: An epidemiologic perspective. Biol. Psychiatry 2001, 49, 1002–1014. [Google Scholar] [CrossRef]
- Olweus, D. Bullies on the Playground: The Role of Victimization, in Children on Playgrounds: Research Perspectives and Applications; State University of New York Press: Albany, NY, USA, 1993; pp. 85–128. [Google Scholar]
- World Health Organization (WHO). Mental Health of Adolescents. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 14 May 2024).
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Shorey, S.; Ng, E.D.; Wong, C.H.J. Global prevalence of depression and elevated depressive symptoms among adolescents: A systematic review and meta-analysis. Br. J. Clin. Psychol. 2022, 61, 287–305. [Google Scholar] [CrossRef] [PubMed]
- Modecki, K.L.; Minchin, J.; Harbaugh, A.G.; Guerra, N.G.; Runions, K.C. Bullying prevalence across contexts: A meta-analysis measuring cyber and traditional bullying. J. Adolesc. Health 2014, 55, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, A.; Oh, H.; Carvalho, A.F.; Smith, L.; Haro, J.M.; Vancampfort, D.; Stubbs, B.; DeVylder, J.E. Bullying Victimization and Suicide Attempt Among Adolescents Aged 12–15 Years from 48 Countries. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 907–918. [Google Scholar] [CrossRef] [PubMed]
- Neary, A.; Joseph, S. Peer victimization and its relationship to self-concept and depression among schoolgirls. Personal. Individ. Differ. 1994, 16, 183–186. [Google Scholar] [CrossRef]
- Sweeting, H.; Young, R.; West, P.; Der, G. Peer victimization and depression in early-mid adolescence: A longitudinal study. Br. J. Educ. Psychol. 2006, 76, 577–594. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Menaghan, E.G.; Lieberman, M.A.; Mullan, J.T. The stress process. J. Health Soc. Behav. 1981, 22, 337–356. [Google Scholar] [CrossRef] [PubMed]
- Zarate-Garza, P.P.; Biggs, B.K.; Croarkin, P.; Morath, B.; Leffler, J.; Cuellar-Barboza, A.; Tye, S.J. How Well Do We Understand the Long-Term Health Implications of Childhood Bullying? Harv. Rev. Psychiatry 2017, 25, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Knack, J.M.; Gomez, H.L.; Jensen-Campbell, L.A. Bullying and its long-term health implications. In Social Pain: Neuropsychological and Health Implications of Loss and Exclusion; American Psychological Association: Washington, DC, USA, 2011; pp. 215–236. [Google Scholar] [CrossRef]
- Patterson, G.R.; Stoolmiller, M. Replications of a dual failure model for boys’ depressed mood. J. Consult. Clin. Psychol. 1991, 59, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Dennehy, R.; Meaney, S.; Walsh, K.A.; Sinnott, C.; Cronin, M.; Arensman, E. Young people’s conceptualizations of the nature of cyberbullying: A systematic review and synthesis of qualitative research. Aggress. Violent Behav. 2020, 51, 101379. [Google Scholar] [CrossRef]
- Vohs, K.D.; Baumeister, R.F. Understanding Self-Regulation: An Introduction. In Handbook of Self-Regulation: Research, Theory, and Applications; Vohs, R.F.B.K.D., Ed.; The Guilford Press: New York, NY, USA, 2004; pp. 1–9. [Google Scholar]
- Brown, J.M. Self-Regulation and the Addictive Behaviors. In Treating Addictive Behaviors, 2nd ed.; Plenum Press: New York, NY, USA, 1998; pp. 61–73. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986; p. xiii, 617. [Google Scholar]
- Kurtovic, A.; Vrdoljak, G.; Hirnstein, M. Contribution to family, friends, school, and community is associated with fewer depression symptoms in adolescents—Mediated by self-regulation and academic performance. Front. Psychol. 2021, 11, 615249. [Google Scholar] [CrossRef]
- Williams, C.; Griffin, K.W.; Botvin, C.M.; Sousa, S.; Botvin, G.J. Self-Regulation as a Protective Factor against Bullying during Early Adolescence. Youth 2024, 4, 478–491. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory of self-regulation. Organ. Behav. Hum. Decis. Process. 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Higgins, E.T. Beyond pleasure and pain. Am. Psychol. 1997, 52, 1280–1300. [Google Scholar] [CrossRef]
- Higgins, E.T. Promotion and Prevention: Regulatory Focus as A Motivational Principle. In Advances in Experimental Social Psychology; Zanna, M.P., Ed.; Academic Press: Cambridge, MA, USA, 1998; pp. 1–46. [Google Scholar] [CrossRef]
- Due, P.; Holstein, B.E.; Lynch, J.; Diderichsen, F.; Nic Gabhain, S.; Scheidt, P.; Currie, C.; The Health Behaviour in School-Aged Children Bullying Working Group. Bullying and symptoms among school-aged children: International comparative cross sectional study in 28 countries. Eur. J. Public Health 2005, 15, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Chester, K.L.; Callaghan, M.; Cosma, A.; Donnelly, P.; Craig, W.; Walsh, S.; Molcho, M. Cross-national time trends in bullying victimization in 33 countries among children aged 11, 13 and 15 from 2002 to 2010. Eur. J. Public Health 2015, 25, 61–64. [Google Scholar] [CrossRef]
- Smith, P.K.; Cowie, H.; Olafsson, R.F.; Liefooghe, A.P.D. Definitions of bullying: A comparison of terms used, and age and gender differences, in a fourteen-country international comparison. Child Dev. 2002, 73, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.; Harel-Fisch, Y.; Fogel-Grinvald, H.; Dostaler, S.; Hetland, J.; Simons-Morton, B.; Molcho, M.; De Mato, M.G.; Overpeck, M.; Due, P.; et al. A cross-national profile of bullying and victimization among adolescents in 40 countries. Int. J. Public Health 2009, 54, 216–224. [Google Scholar] [CrossRef]
- Strohacker, E.; Wright, L.E.; Watts, S.J. Gender, Bullying Victimization, Depressive Symptoms, and Suicidality. Int. J. Offender Ther. Comp. Criminol. 2021, 65, 1123–1142. [Google Scholar] [CrossRef]
- Espelage, D.L.; Holt, M.K. Bullying and Victimization during Early Adolescence. J. Emot. Abus. 2001, 2, 123–142. [Google Scholar] [CrossRef]
- Moilanen, K.L. The Adolescent Self-Regulatory Inventory: The development and validation of a questionnaire of short-term and long-term self-regulation. J. Youth Adolesc. 2007, 36, 835–848. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Aiken, L.S.; West, S.G. Multiple regression: Testing and interpreting interactions. In Multiple Regression: Testing and Interpreting Interactions; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1991; p. xi, 212. [Google Scholar]
- Ye, Z.; Wu, D.; He, X.; Ma, Q.; Peng, J.; Mao, G.; Feng, L.; Tong, Y. Meta-analysis of the relationship between bullying and depressive symptoms in children and adolescents. BMC Psychiatry 2023, 23, 215. [Google Scholar] [CrossRef] [PubMed]
- Compas, B.E.; Connor-Smith, J.K.; Saltzman, H.; Thomsen, A.H.; Wadsworth, M.E. Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychol. Bull. 2001, 127, 87–127. [Google Scholar] [CrossRef] [PubMed]
- Skinner, E.A.; Zimmer-Gembeck, M.J. Challenges to the developmental study of coping. New Dir. Child Adolesc. Dev. 2009, 2009, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Skinner, E.A.; Zimmer-Gembeck, M.J. The development of coping. Annu. Rev. Psychol. 2007, 58, 119–144. [Google Scholar] [CrossRef]
- PISA 2015 Results; OECD: Paris, France, 2017; Volume III.
- Lam, S. Policy Measures to Combat Bullying in Schools; Research Office, Information Services Division, Legislative Council Secretariat, Ed.; Legislative Council: Hong Kong, China, 2019. [Google Scholar]
- Menken, M.S.; Isaiah, A.; Liang, H.; Rivera, P.R.; Cloak, C.C.; Reeves, G.; Lever, N.A.; Chang, L. Peer victimization (bullying) on mental health, behavioral problems, cognition, and academic performance in preadolescent children in the ABCD Study. Front. Psychol. 2022, 13, 925727. [Google Scholar] [CrossRef]
- Jewkes, R.; Morrell, R. Masculinities and violence: Using latent class analysis to investigate the origins and correlates of differences between men in the cross-sectional UN Multi-country Study on men and violence in Asia and the Pacific. J. Glob. Health 2020, 10, 020439. [Google Scholar] [CrossRef]
- Leone, R.M.; Parrott, D.J. Hegemonic masculinity and aggression. In The Routledge International Handbook of Human Aggression: Current Issues and Perspectives; Ireland, J., Birch, P., Ireland, C., Eds.; Routledge: London, UK, 2018; pp. 31–42. [Google Scholar] [CrossRef]
- Pleck, J.H. The Forty-Nine Percent Majority: The Male Sex Role. Psychol. Women Q. 1977, 2, 79–80. [Google Scholar] [CrossRef]
- Smith, P.K.; Salmivalli, C.; Cowie, H. Effectiveness of school-based programs to reduce bullying: A commentary. J. Exp. Criminol. 2012, 8, 433–441. [Google Scholar] [CrossRef]
- Fung, A.L.-C. Cognitive-Behavioural Group Therapy for Pure Victims with Internalizing Problems: An Evidence-based One-year Longitudinal Study. Appl. Res. Qual. Life 2018, 13, 691–708. [Google Scholar] [CrossRef]
- Unnever, J.D. Bullies, Aggressive Victims, and Victims: Are They Distinct Groups? Aggress. Behav. 2005, 31, 153–171. [Google Scholar] [CrossRef]
- Halliday, S.; Gregory, T.; Taylor, A.; Digenis, C.; Turnbull, D. The Impact of Bullying Victimization in Early Adolescence on Subsequent Psychosocial and Academic Outcomes across the Adolescent Period: A Systematic Review. J. Sch. Violence 2021, 20, 351–373. [Google Scholar] [CrossRef]
- Idsoe, T.; Vaillancourt, T.; Dyregrov, A.; Hagen, K.A.; Ogden, T.; Nærde, A. Bullying Victimization and Trauma. Front. Psychiatry 2021, 11, 480353. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | United Kingdom | The Netherlands | Hong Kong | Taiwan |
|---|---|---|---|---|
| (n = 1055) | (n = 959) | (n = 925) | (n = 1045) | |
| 26.5 (%) | 24.1 (%) | 23.2 (%) | 26.2 (%) | |
| Age | ||||
| Mean | 16.56 | 16.07 | 15.87 | 16.22 |
| SD | 1.49 | 1.57 | 1.8 | 1.56 |
| Gender | ||||
| Female | 639 (60.6) | 301 (31.4) | 324 (35.0) | 464 (44.4) |
| Male | 394 (37.3) | 651 (67.9) | 601 (65.0) | 581 (55.6) |
| Ethnicity | ||||
| Asian | 147 (13.9) | 71 (7.4) | 814 (88.0) | 965 (92.3) |
| Caucasian | 692 (65.6) | 808 (84.3) | 88 (9.5) | 67 (6.4) |
| Black | 114 (10.8) | 35 (3.6) | 13 (1.4) | 3 (0.3) |
| Hispanic | 4 (0.4) | 10 (1.0) | 3 (0.3) | 2 (0.2) |
| Mixed Race | 16 (1.5) | 27 (2.8) | 7 (0.8) | 8 (0.8) |
| History of mental disorders | ||||
| Yes | 223 (21.1) | 54 (5.6) | 23 (2.5) | 28 (2.7) |
| No | 832 (78.9) | 905 (94.4) | 902 (97.5) | 1017 (97.3) |
| Mental disorder treatments | ||||
| Yes | 92 (8.7) | 141 (14.7) | 8 (0.9) | 26 (2.5) |
| No | 963 (91.3) | 818 (85.3) | 917 (99.1) | 1019 (97.5) |
| Variables | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Bullying victimization | 3.83 | 4.11 | - | ||||||
| 2. Depression | 8.58 | 6.4 | 0.53 ** | ||||||
| 3. Self-regulation | 109.88 | 10.92 | −0.13 ** | −0.22 ** | |||||
| 4. Age | 16.19 | 1.63 | −0.06 ** | 0.05 ** | −0.01 ** | ||||
| 5. Gender | 1.45 | 0.51 | −0.09 ** | 0.09 ** | −0.02 ** | 0.14 ** | |||
| 6. Region | 5.49 | 1.14 | −0.22 ** | −0.28 ** | 0.1 ** | −0.09 ** | −0.13 ** | ||
| 7. History of mental disorder | 1.08 | 0.28 | 0.12 ** | 0.32 ** | −0.14 ** | 0.11 ** | 0.19 ** | −0.25 ** | - |
| Relationship | Total Effect | Direct Effect | Indirect Effect | Bootstrap 95% Confidence Interval | t-Statistic | Conclusion | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Bullying victimization -> Self-regulation -> Depression | 0.690 | 0.658 | 0.032 | 0.023 | 0.042 | 6.47 | Partial |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Q.-L.; Ho, W.-S.; Cheung, H.-N. Exploring the Mediating Role of Self-Regulation in Bullying Victimization and Depressive Symptoms among Adolescents: A Cross-Regional and Gender Analysis. Healthcare 2024, 12, 1486. https://doi.org/10.3390/healthcare12151486
Huang Q-L, Ho W-S, Cheung H-N. Exploring the Mediating Role of Self-Regulation in Bullying Victimization and Depressive Symptoms among Adolescents: A Cross-Regional and Gender Analysis. Healthcare. 2024; 12(15):1486. https://doi.org/10.3390/healthcare12151486
Chicago/Turabian StyleHuang, Qi-Lu, Wing-Shan Ho, and Ho-Nam Cheung. 2024. "Exploring the Mediating Role of Self-Regulation in Bullying Victimization and Depressive Symptoms among Adolescents: A Cross-Regional and Gender Analysis" Healthcare 12, no. 15: 1486. https://doi.org/10.3390/healthcare12151486
APA StyleHuang, Q.-L., Ho, W.-S., & Cheung, H.-N. (2024). Exploring the Mediating Role of Self-Regulation in Bullying Victimization and Depressive Symptoms among Adolescents: A Cross-Regional and Gender Analysis. Healthcare, 12(15), 1486. https://doi.org/10.3390/healthcare12151486