

Long-Term Effectiveness of Physical Exercise-Based Swallowing Interventions for Older Adults with Dementia in a Day-Care Center
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cases
2.2. Physical Exercise-Based Swallowing Interventions
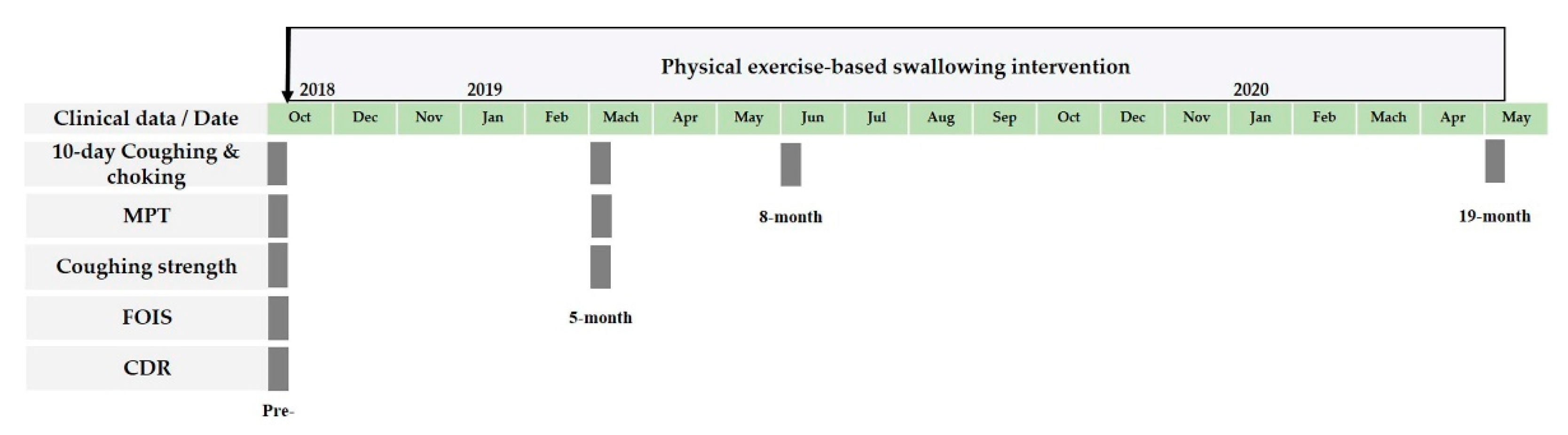
2.3. Clinical Data Related to Safe Swallowing
2.4. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics in Two Groups
3.2. Short-Term Changes in 10-Day Coughing-Choking, MPT, and Coughing Strength
3.3. Long-Term Changes in 10-Day Coughing-Choking
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fact Sheet on Dementia (20 September 2022). World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 20 January 2023).
- Espinosa-Val, M.C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O.J.N. Prevalence, risk factors, and complications of oropharyngeal dysphagia in older patients with dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef] [PubMed]
- Baijens, L.W.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [PubMed]
- Ney, D.M.; Weiss, J.M.; Kind, A.J.; Robbins, J. Senescent swallowing: Impact, strategies, and interventions. Nutr. Clin. Pract. 2009, 24, 395–413. [Google Scholar] [CrossRef] [PubMed]
- Kayser-Jones, J.; Pengilly, K. Dysphagia among nursing home residents. Geriatr. Nurs. 1999, 20, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Rogus-Pulia, N.M.; Plowman, E.K. Shifting tides toward a proactive patient-centered approach in dysphagia management of neurodegenerative disease. Am. J. Speech Lang. Pathol. 2020, 29, 1094–1109. [Google Scholar] [CrossRef]
- Rogus-Pulia, N.; Malandraki, G.A.; Johnson, S.; Robbins, J.A. Understanding dysphagia in dementia: The present and the future. Curr. Phys. Med. Rehabil. Rep. 2015, 3, 86–97. [Google Scholar] [CrossRef]
- Dipietro, L.; Campbell, W.W.; Buchner, D.M.; Erickson, K.I.; Powell, K.E.; Bloodgood, B.; Hughes, T.; Day, K.R.; Piercy, K.L.; Vaux-Bjerke, A.J.M. Physical activity, injurious falls, and physical function in aging: An umbrella review. Med. Sci. Sports Exerc. 2019, 51, 1303. [Google Scholar] [CrossRef]
- Erickson, K.I.; Donofry, S.D.; Sewell, K.R.; Brown, B.M.; Stillman, C.M. Cognitive aging and the promise of physical activity. Annu. Rev. Clin. Psychol. 2022, 18, 417–442. [Google Scholar] [CrossRef]
- Chen, S.; Kent, B.; Cui, Y. Interventions to prevent aspiration in older adults with dysphagia living in nursing homes: A scoping review. BMC Geriatr. 2021, 21, 429. [Google Scholar] [CrossRef]
- Chen, M.A.; Liu, C.K.; Yang, Y.H.; Huang, S.T.; Yen, C.W.; Kabasawa, Y.; Huang, H.L. Clinical-based oral rehabilitation programme improved the oral diadochokinesis and swallowing function of older patients with dementia: A randomised controlled trial. J. Oral Rehabil. 2022, 49, 1163–1172. [Google Scholar] [CrossRef]
- Grand, J.H.; Caspar, S.; MacDonald, S.W. Clinical features and multidisciplinary approaches to dementia care. J. Multidiscip. Healthc. 2011, 4, 125. [Google Scholar] [PubMed]
- Muñoz-Bermejo, L.; González-Becerra, M.J.; Barrios-Fernández, S.; Postigo-Mota, S.; Jerez-Barroso, M.D.R.; Martínez, J.A.F.; Suárez-Lantarón, B.; Marín, D.M.; Martín-Bermúdez, N.; Ortés-Gómez, R.; et al. Cost-Effectiveness of the Comprehensive Interdisciplinary Program-Care in Informal Caregivers of People with Alzheimer’s Disease. Int. J. Environ. Res. Public Health 2022, 19, 15243. [Google Scholar] [CrossRef]
- Hsu, H.C.; Chen, C.F. LTC 2.0: The 2017 reform of home-and community-based long-term care in Taiwan. Health Policy 2019, 123, 912–916. [Google Scholar] [CrossRef]
- Hsiao, Y.H.; Kuo, T.A.; Tai, C.J.; Lee, S.S.; Lee, M.C. Integrated care for dementia in Taiwan: Policy, system and services. Int. J. Gerontol. 2019, 13, S73–S77. [Google Scholar]
- Taiwan-SLPU Swallowing Exercises, Taiwan Speech Language Pathologist Union. Available online: https://www.youtube.com/watch?v=ACFX7q8VQRU (accessed on 20 January 2023).
- Berg, L. Clinical Dementia Rating. Br. J. Psychiatry 1984, 145, 339. [Google Scholar] [CrossRef] [PubMed]
- Crary, M.A.; Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef]
- Ko, E.J.; Chae, M.; Cho, S.R. Relationship Between Swallowing Function and Maximum Phonation Time in Patients With Parkinsonism. Ann. Rehabil. Med. 2018, 42, 425–432. [Google Scholar] [CrossRef]
- Ibrahim, A.S.; Aly, M.G.; Abdel-Rahman, K.A.; Mohamed, M.A.; Mehany, M.M.; Aziz, E.M. Semi-quantitative Cough Strength Score as a Predictor for Extubation Outcome in Traumatic Brain Injury: A Prospective Observational Study. Neurocritical. Care 2018, 29, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Humbert, I.A.; McLaren, D.G.; Kosmatka, K.; Fitzgerald, M.; Johnson, S.; Porcaro, E.; Kays, S.; Umoh, E.O.; Robbins, J. Early deficits in cortical control of swallowing in Alzheimer’s disease. J. Alzheimer’s Dis. 2010, 19, 1185–1197. [Google Scholar] [CrossRef]
- Brach, J.S.; Simonsick, E.M.; Kritchevsky, S.; Yaffe, K.; Newman, A.B. The association between physical function and lifestyle activity and exercise in the health, aging and body composition study. J. Am. Geriatr. Soc. 2004, 52, 502–509. [Google Scholar] [CrossRef]
- Rogers, N.T.; Steptoe, A.; Cadar, D. Frailty is an independent predictor of incident dementia: Evidence from the English Longitudinal Study of Ageing. Sci. Rep. 2017, 7, 15746. [Google Scholar] [CrossRef] [PubMed]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2015, 2015, Cd006489. [Google Scholar] [CrossRef]
- Chang, S.H.; Chen, C.Y.; Shen, S.H.; Chiou, J.H. The effectiveness of an exercise programme for elders with dementia in a Taiwanese day-care centre. Int. J. Nurs. Pract. 2011, 17, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Langmore, S.E.; Pisegna, J.M. Efficacy of exercises to rehabilitate dysphagia: A critique of the literature. Int. J. Speech Lang. Pathol. 2015, 17, 222–229. [Google Scholar] [CrossRef]
- Balou, M.; Herzberg, E.G.; Kamelhar, D.; Molfenter, S.M. An intensive swallowing exercise protocol for improving swallowing physiology in older adults with radiographically confirmed dysphagia. Clin. Interv. Aging 2019, 14, 283–288. [Google Scholar] [CrossRef]
- Hong, S.Y.; Hughes, S.; Prohaska, T. Factors affecting exercise attendance and completion in sedentary older adults: A meta-analytic approach. J. Phys. Act. Health 2008, 5, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Lamb, S.E.; Sheehan, B.; Atherton, N.; Nichols, V.; Collins, H.; Mistry, D.; Dosanjh, S.; Slowther, A.M.; Khan, I.; Petrou, S.; et al. Dementia And Physical Activity (DAPA) trial of moderate to high intensity exercise training for people with dementia: Randomised controlled trial. BMJ 2018, 361, k1675. [Google Scholar] [CrossRef] [PubMed]
- Telenius, E.W.; Engedal, K.; Bergland, A. Effect of a high-intensity exercise program on physical function and mental health in nursing home residents with dementia: An assessor blinded randomized controlled trial. PloS ONE 2015, 10, e0126102. [Google Scholar] [CrossRef]
- Littbrand, H.; Stenvall, M.; Rosendahl, E. Applicability and effects of physical exercise on physical and cognitive functions and activities of daily living among people with dementia: A systematic review. Am. J. Phys. Med. Rehabil. 2011, 90, 495–518. [Google Scholar] [CrossRef]
- Tretteteig, S.; Vatne, S.; Rokstad, A.M. The influence of day care centres for people with dementia on family caregivers: An integrative review of the literature. Aging Ment. Health 2016, 20, 450–462. [Google Scholar] [CrossRef]
- Schmitt, E.M.; Sands, L.P.; Weiss, S.; Dowling, G.; Covinsky, K. Adult day health center participation and health-related quality of life. Gerontologist 2010, 50, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.F.; Wu, J.J.; Huang, Y.H.; Ju, L.Y.; Lin, S.Y.; Chou, Y.C.; Lin, C.S. Impact of day care services on physical and cognitive functions in old people with dementia in a medical center in central Taiwan. Health Qual. Life Outcomes 2021, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Exercises | Objectives of the Exercises | Instructions for the Exercises |
|---|---|---|
| Maintain a Straight Sitting Posture in the Chair Throughout All Exercises. | ||
| Exercises of the head, neck, and shoulder | To warm up and reduce tension in the muscles related to swallowing in the head, neck, and shoulder areas. | 5–10 sets of neck forward stretching, side stretching, shoulder shrugging, and shoulder rolling. |
| Oral exercises of the lip and tongue | To maintain or enhance the functional reserve of the muscles required for the transition from chewing to swallowing. | 5–10 sets of lip stretching, lip puckering, tongue protruding, and tongue side-to-side moving. |
| Effortful swallow | To maintain or enhance the functional reserve of the muscles used in swallowing. | 5–10 sets of effortful swallowing. |
| Vocal function exercise | To maintain or enhance the functional reserve of the muscles involved in vocal fold regulation for swallowing safety. | 5–10 sets of effortful pitch gliding, and sustained humming. |
| Chin tuck against resistance (CTAR) | To strengthen the suprahyoid muscles involved in opening the upper esophageal sphincter at the late stage of swallowing. | 5 sets of sustained CTAR and repetitive CTAR. |
| Breathing exercises | To help improve respiratory function and support swallowing function. | 5 sets of abdominal breathing. |
| Total | Exercise-Based | Non-Exercise-Based | p-Value | |
|---|---|---|---|---|
| N | 29 | 22 | 7 | |
| Proportion | 75.8% | 24.2% | ||
| Age | 78.93 ± 7.03 | 77.09 ± 6.84 | 84.71 ± 3.90 | 0.010 * |
| Gender | - | - | - | 0.071 |
| Male | 11(37.9%) | 6(27.3%) | 5(71.4%) | |
| Female | 18(62.1%) | 16(72.7%) | 2(28.6%) | |
| CDR | - | - | - | 0.001 * |
| 0.5 | 1(3.4%) | 0(0.0%) | 1(14.3%) | |
| 1 | 15(51.7%) | 15(68.2%) | 0(0.0%) | |
| 2 | 9(31.0%) | 6(27.3%) | 3(42.9%) | |
| 3 | 4(13.8%) | 1(4.5%) | 3(42.9%) | |
| FOIS | 6.31 ± 0.89 | 6.50 ± 0.86 | 5.71 ± 0.76 | 0.040 * |
| 10-day coughing-choking | 3.86 ± 5.38 | 3.55 ± 5.85 | 4.86 ± 3.72 | 0.583 |
| MPT (s) | 8.03 ± 5.17 | 9.27 ± 5.11 | 4.14 ± 3.18 | 0.019 * |
| Coughing strength | 1.93 ± 0.81 | 2.09 ± 0.61 | 1.33 ± 1.21 | 0.041 * |
| Item | Group | N | Pre | 5M | Delta (5M-Pre) | Within Group p-Value | Between Group p-Value |
|---|---|---|---|---|---|---|---|
| 10-day coughing-choking | Exercise-based | 22 | 3.55 ± 5.85 | 1.41 ± 1.99 | −2.14 ± 4.14 | 0.003 * | 0.348 |
| Non-exercise-based | 7 | 4.86 ± 3.72 | 2.71 ± 1.80 | −2.14 ± 2.27 | 0.041 * | ||
| MPT (s) | Exercise-based | 22 | 9.27 ± 5.11 | 11.46 ± 5.77 | 2.19 ± 4.94 | 0.0497 * | 0.713 |
| Non-exercise-based | 6 | 4.67 ± 3.14 | 6.08 ± 3.65 | 1.42 ± 1.94 | 0.133 | ||
| Coughing strength | Exercise-based | 22 | 2.09 ± 0.61 | 2.41 ± 0.65 | 0.32 ± 0.73 | 0.039 * | 0.723 |
| Non-exercise-based | 6 | 1.33 ± 1.21 | 1.50 ± 1.05 | 0.17 ± 0.41 | 0.317 |
| Item | Group | N | Pre | 5M | 8M | 19M | p-Value Pre vs. 5M | p-Value Pre vs. 8M | p-Value Pre vs. 19M |
|---|---|---|---|---|---|---|---|---|---|
| 10-day coughing-choking | Exercise-based | 22 | 3.55 ± 5.85 | 1.41 ± 1.99 | 1.86 ± 2.15 | 1.13 ± 1.67 | 0.003 * | 0.091 | 0.040 * |
| Non-exercise-based | 7 | 4.86 ± 3.72 | 2.71 ± 1.80 | 2.86 ± 1.95 | 4.00 ± 3.41 | 0.041 * | 0.246 | 0.892 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Lin, C.-Y.; Chen, C.-L.; Chen, K.-T.; Lee, C.; Yu, Y.-H.; Shih, C.-Y. Long-Term Effectiveness of Physical Exercise-Based Swallowing Interventions for Older Adults with Dementia in a Day-Care Center. Healthcare 2023, 11, 1262. https://doi.org/10.3390/healthcare11091262
Chen C-H, Lin C-Y, Chen C-L, Chen K-T, Lee C, Yu Y-H, Shih C-Y. Long-Term Effectiveness of Physical Exercise-Based Swallowing Interventions for Older Adults with Dementia in a Day-Care Center. Healthcare. 2023; 11(9):1262. https://doi.org/10.3390/healthcare11091262
Chicago/Turabian StyleChen, Chia-Hui, Chia-Yu Lin, Chiao-Ling Chen, Kuan-Ting Chen, Cho Lee, Ya-Hsin Yu, and Chiao-Yu Shih. 2023. "Long-Term Effectiveness of Physical Exercise-Based Swallowing Interventions for Older Adults with Dementia in a Day-Care Center" Healthcare 11, no. 9: 1262. https://doi.org/10.3390/healthcare11091262
APA StyleChen, C.-H., Lin, C.-Y., Chen, C.-L., Chen, K.-T., Lee, C., Yu, Y.-H., & Shih, C.-Y. (2023). Long-Term Effectiveness of Physical Exercise-Based Swallowing Interventions for Older Adults with Dementia in a Day-Care Center. Healthcare, 11(9), 1262. https://doi.org/10.3390/healthcare11091262