


Study the Effect of an Innovative Educational Program Promoting Healthy Food Habits on Eating Disorders, Mediterranean Diet Adherence and Body Composition in University Students

 ,
, 
 , ,
, ,  ,
,  ,
,  , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Procedures
2.3. Materials
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnett, J. Emerging Adulthood: The Winding Road from the Late Teens Through the Twenties, 2nd ed.; Oxford University Press: Oxford, UK, 2019; ISBN 978-0199929382. [Google Scholar]
- Hudson, J.I.; Hiripi, E.; Pope, H.G.J.; Kessler, R.C. The Prevalence and Correlates of Eating Disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef]
- Sim, L.A.; McAlpine, D.E.; Grothe, K.B.; Himes, S.M.; Cockerill, R.G.; Clark, M.M. Identification and Treatment of Eating Disorders in the Primary Care Setting. Mayo Clin. Proc. 2010, 85, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Jahrami, H.; Sater, M.; Abdulla, A.; Faris, M.A.-I.; AlAnsari, A. Eating Disorders Risk among Medical Students: A Global Systematic Review and Meta-Analysis. Eat. Weight Disord. 2019, 24, 397–410. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Lu, M.; Tian, L.; Lu, W.; Meng, F.; Chen, C.; Tang, T.; He, L.; Yao, Y. Prevalence of Disordered Eating Attitudes among University Students In Wuhu, China. Nutr. Hosp. 2015, 32, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Tavolacci, M.-P.; Déchelotte, P.; Ladner, J. Eating Disorders among College Students in France: Characteristics, Help-and Care-Seeking. Int. J. Environ. Res. Public Health 2020, 17, 5914. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, A.R.; Carrobles, J.A.; Gandarillas, A.M. Gender, School and Academic Year Differences among Spanish University Students at High-Risk for Developing an Eating Disorder: An Epidemiologic Study. BMC Public Health 2008, 8, 102. [Google Scholar] [CrossRef]
- Vila-Martí, A.; Elío, I.; Sumalla-Cano, S. Eating Behavior during First-Year College Students, Including Eating Disorders-RUVIC-RUNEAT-TCA Project. Protocol of an Observational Multicentric Study. Int. J. Environ. Res. Public Health 2021, 18, 9457. [Google Scholar] [CrossRef] [PubMed]
- Maillet, M.A.; Grouzet, F.M.E. Understanding changes in eating behavior during the transition to university from a self-determination theory perspective: A systematic review. J. Am. Coll Health 2023, 71, 422–439. [Google Scholar] [CrossRef]
- Harrer, M.; Adam, S.H.; Messner, E.M.; Baumeister, H.; Cuijpers, P.; Bruffaerts, R.; Auerbach, R.P.; Kessler, R.C.; Jacobi, C.; Taylor, C.B.; et al. Prevention of Eating Disorders at Universities: A Systematic Review and Meta-Analysis. Int. J. Eat. Disord. 2020, 53, 813–833. [Google Scholar] [CrossRef]
- Freitas, D.; Oliveira, B.M.; Correia, F.; Pinhão, S.; Poínhos, R. Eating Behaviour among Nutrition Students and Social Desirability as a Confounder. Appetite 2017, 113, 187–192. [Google Scholar] [CrossRef]
- Trindade, A.P.; Appolinario, J.C.; Mattos, P.; Treasure, J.; Nazar, B.P. Eating Disorder Symptoms in Brazilian University Students: A Systematic Review and Meta-Analysis. Rev. Bras. Psiquiatr. 2019, 41, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Grammatikopoulou, M.G.; Gkiouras, K.; Markaki, A.; Theodoridis, X.; Tsakiri, V.; Mavridis, P.; Dardavessis, T.; Chourdakis, M. Food Addiction, Orthorexia, and Food-Related Stress among Dietetics Students. Eat. Weight Disord. 2018, 23, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Mahn, H.M.; Lordly, D. A Review of Eating Disorders and Disordered Eating amongst Nutrition Students and Dietetic Professionals. Can. J. Diet. Pract. Res. 2015, 76, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Fiates, G.M.R.; Salles, R.K. de Fatores de Risco Para o Desenvolvimento de Distúrbios Alimentares: Um Estudo Em Universitárias. Rev. Nutr. 2001, 14, 3–6. [Google Scholar] [CrossRef]
- Penz, L.; Dal Bosco, S.; Vieira, J. Risk for Development of Eating Disorders in Students of Nutrition. Sci. Med. 2008, 18, 124–128. [Google Scholar]
- Hughes, R.; Desbrow, B. Aspiring Dietitians Study: A Pre-Enrolment Study of Students Motivations, Awareness and Expectations Relating to Careers in Nutrition and Dietetics. Nutr. Diet. 2005, 62, 106–109. [Google Scholar] [CrossRef]
- Rouzitalab, T.; Pourghassem Gargari, B.; Amirsasan, R.; Asghari Jafarabadi, M.; Farsad Naeimi, A.; Sanoobar, M. The Relationship of Disordered Eating Attitudes With Body Composition and Anthropometric Indices in Physical Education Students. Iran. Red Crescent Med. J. 2015, 17, e20727. [Google Scholar] [CrossRef]
- Plichta, M.; Jezewska-Zychowicz, M. Eating Behaviors, Attitudes toward Health and Eating, and Symptoms of Orthorexia Nervosa among Students. Appetite 2019, 137, 114–123. [Google Scholar] [CrossRef]
- Gropper, S.S.; Arsiwalla, D.D.; Lord, D.C.; Huggins, K.W.; Simmons, K.P.; Ulrich, P. V Associations among Eating Regulation and Body Mass Index, Weight, and Body Fat in College Students: The Moderating Role of Gender. Eat. Behav. 2014, 15, 321–327. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Merino, J.; Sun, Q.; Fitó, M.; Salas-Salvadó, J. Dietary Polyphenols, Mediterranean Diet, Prediabetes, and Type 2 Diabetes: A Narrative Review of the Evidence. Oxid. Med. Cell. Longev. 2017, 2017, 6723931. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health: A Critical Review. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Alacid, F.; Vaquero-Cristóbal, R.; Sánchez-Pato, A.; Muyor, J.M.; López-Miñarro, P.Á. Adhesión a La Dieta Mediterránea y Relación Con Los Parámetros Antropométricos de Mujeres Jóvenes Kayakistas. Nutr. Hosp. 2014, 29, 121–127. [Google Scholar] [CrossRef]
- Rosa, A.; Loy, F.; Pinna, I.; Masala, C. Role of Aromatic Herbs and Spices in Salty Perception of Patients with Hyposmia. Nutrients 2022, 14, 4976. [Google Scholar] [CrossRef] [PubMed]
- San Román Mata, S.; Zurita Ortega, F.; Martínez Martínez, A.; Padial Ruz, R.; Chacón Cuberos, R.; Linares Manrique, M. Adherencia a La Dieta Mediterránea En Estudiantes Universitarios Del Sur de España Según Factores Sociales, Académicos y Religiosos. Rev. Española Nutr. Humana y Dietética 2018, 22, 141–148. [Google Scholar] [CrossRef]
- Sundgot-Borgen, C.; Bratland-Sanda, S.; Engen, K.M.E.; Pettersen, G.; Friborg, O.; Torstveit, M.K.; Kolle, E.; Piran, N.; Sundgot-Borgen, J.; Rosenvinge, J.H. The Norwegian Healthy Body Image Programme: Study Protocol for a Randomized Controlled School-Based Intervention to Promote Positive Body Image and Prevent Disordered Eating among Norwegian High School Students. BMC Psychol. 2018, 6, 8. [Google Scholar] [CrossRef]
- Wadolowska, L.; Hamulka, J.; Kowalkowska, J.; Ulewicz, N.; Hoffmann, M.; Gornicka, M.; Bronkowska, M.; Leszczynska, T.; Glibowski, P.; Korzeniowska-Ginter, R. Changes in Sedentary and Active Lifestyle, Diet Quality and Body Composition Nine Months after an Education Program in Polish Students Aged 11−12 Years: Report from the ABC of Healthy Eating Study. Nutrients 2019, 11, 331. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, C.G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Constaín, G.A.; Ricardo Ramírez, C.; de Rodríguez-Gázquez, M.L.Á.; Alvarez Gómez, M.; Marín Múnera, C.; Agudelo Acosta, C. Diagnostic validity and usefulness of the Eating Attitudes Test-26 for the assessment of eating disorders risk in a Colombian female population. Aten. Primaria 2014, 46, 283–289. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988; ISBN 9789896540821. [Google Scholar]
- Yu, Z.; Tan, M. Disordered Eating Behaviors and Food Addiction among Nutrition Major College Students. Nutrients 2016, 8, 673. [Google Scholar] [CrossRef]
- Fekih-Romdhane, F.; Daher-Nashif, S.; Alhuwailah, A.H.; Al Gahtani, H.M.S.; Hubail, S.A.; Shuwiekh, H.A.M.; Khudhair, M.F.; Alhaj, O.A.; Bragazzi, N.L.; Jahrami, H. The Prevalence of Feeding and Eating Disorders Symptomology in Medical Students: An Updated Systematic Review, Meta-Analysis, and Meta-Regression. Eat. Weight Disord. 2022, 27, 1991–2010. [Google Scholar] [CrossRef]
- Matusik, A.; Grajek, M.; Szlacheta, P.; Korzonek-Szlacheta, I. Comparison of the Prevalence of Eating Disorders among Dietetics Students and Students of Other Fields of Study at Selected Universities (Silesia, Poland). Nutrients 2022, 14, 3210. [Google Scholar] [CrossRef] [PubMed]
- Gonidakis, F.; Sigala, A.; Varsou, E.; Papadimitriou, G. A Study of Eating Attitudes and Related Factors in a Sample of First-Year Female Nutrition and Dietetics Students of Harokopion University in Athens, Greece. Eat. Weight Disord. 2009, 14, e121-7. [Google Scholar] [CrossRef] [PubMed]
- Korinth, A.; Schiess, S.; Westenhoefer, J. Eating Behaviour and Eating Disorders in Students of Nutrition Sciences. Public Health Nutr. 2010, 13, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Poínhos, R.; Alves, D.; Vieira, E.; Pinhão, S.; Oliveira, B.M.P.M.; Correia, F. Eating Behaviour among Undergraduate Students. Comparing Nutrition Students with Other Courses. Appetite 2015, 84, 28–33. [Google Scholar] [CrossRef]
- Wilfley, D.E.; Bishop, M.E.; Wilson, G.T.; Agras, W.S. Classification of Eating Disorders: Toward DSM-V. Int. J. Eat. Disord. 2007, 40, S123–S129. [Google Scholar] [CrossRef]
- Kinzl, J.F.; Hauer, K.; Traweger, C.; Kiefer, I. Orthorexia Nervosa in Dieticians. Psychother. Psychosom. 2006, 75, 395–396. [Google Scholar] [CrossRef] [PubMed]
- Messent, P. DSM-5. Clin. Child Psychol. Psychiatry 2013, 18, 479–482. [Google Scholar]
- Yager, Z.; O’;Dea, J.A. The Role of Teachers and Other Educators in the Prevention of Eating Disorders and Child Obesity: What Are the Issues? Eat. Disord. 2005, 13, 261–278. [Google Scholar] [CrossRef]
- Plotnikoff, R.C.; Costigan, S.A.; Williams, R.L.; Hutchesson, M.J.; Kennedy, S.G.; Robards, S.L.; Allen, J.; Collins, C.E.; Callister, R.; Germov, J. Effectiveness of Interventions Targeting Physical Activity, Nutrition and Healthy Weight for University and College Students: A Systematic Review and Meta-Analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 45. [Google Scholar] [CrossRef]
- Vanderwall, C.; Eickhoff, J.; Randall Clark, R.; Carrel, A.L. BMI Z-Score in Obese Children Is a Poor Predictor of Adiposity Changes over Time. BMC Pediatr. 2018, 18, 187. [Google Scholar] [CrossRef]
- Yahia, N.; Wang, D.; Rapley, M.; Dey, R. Assessment of Weight Status, Dietary Habits and Beliefs, Physical Activity, and Nutritional Knowledge among University Students. Perspect. Public Health 2016, 136, 231–244. [Google Scholar] [CrossRef] [PubMed]
- von Bothmer, M.I.K.; Fridlund, B. Gender Differences in Health Habits and in Motivation for a Healthy Lifestyle among Swedish University Students. Nurs. Health Sci. 2005, 7, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Del Río, M.P.R.; Silleras, B.D.M.; Enciso, L.C.; De Miguelsanz, J.M.M.; McPhee, M.F.; Martín, M.A.C. Ingesta Dietética y Adherencia a La Dieta Mediterránea En Un Grupo de Estudiantes Universitarios En Función de La Práctica Deportiva. Nutr. Hosp. 2016, 33, 1172–1178. [Google Scholar] [CrossRef]
- Tárraga Marcos, A.; Panisello Royo, J.M.; Carbayo Herencia, J.A.; López Gil, J.F.; García Cantó, E.; Tárraga López, P.J. Nutrición Hospitalaria. Nutr. Hosp. 2021, 38, 814–820. [Google Scholar] [CrossRef]
- Montero Bravo, A.; Úbeda Martín, N.; García González, A. Evaluación de Los Hábitos Alimentarios de Una Población de Estudiantes Universitarios En Relación Con Sus Conocimientos Nutricionales. Nutr. Hosp. 2006, 21, 466–473. [Google Scholar]
- Rodríguez Méndez, M.; Echemendía Tocabens, B. La Prevención En Salud: Posibilidad y Realidad. Rev. Cubana Hig. Epidemiol. 2011, 49, 135–150. [Google Scholar]



{kind=link}
{kind=link}
| Topics in the Education Program | |
|---|---|
| Nutrition topic | Essential nutrients in the diet of young adults, quantities, and portions. Health consequences of processed products and alcohol consumption. Healthy snacking. |
| Healthy lifestyle (physical activity) | Influence of physical activity on physical and intellectual development and healthy well-being. Recommendations based on the WHO guidelines [28]. |
| Risk behaviors and eating disorders | Factors that influence body perception. What promotes and reduces positive body image and how can we enforce health-promoting factors? Strengthen acceptance and love for individual differences, defining characteristics of self and friends. |
| CONTROL GROUP | EDUCATED GROUP | ANOVA | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | PRE | POST | Effect Time | Effect Time × Group | |||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F | p | η2p | F | p | η2p | |
| Weight | 58.7 | 10.4 | 57.9 | 12.5 | 59.9 | 11.1 | 59.0 | 11.7 | 10.00 | 0.002 | 0.065 | 6.36 | 0.013 | 0.042 |
| BMI | 21.9 | 3.24 | 21.6 | 4.13 | 22.9 | 4.17 | 22.5 | 4.30 | 10.62 | 0.001 | 0.069 | 7.23 | 0.008 | 0.048 |
| FM constant hydration (%) | 26.4 | 5.62 | 26.4 | 5.94 | 27.6 | 6.13 | 26.7 | 6.61 | 9.83 | 0.002 | 0.063 | 6.65 | 0.011 | 0.044 |
| Crude FM (Kg) | 16.4 | 6.74 | 16.4 | 6.99 | 28.2 | 6.47 | 27.3 | 6.95 | 10.10 | 0.002 | 0.065 | 9.20 | 0.003 | 0.060 |
| SMM (Kg) | 21.3 | 3.06 | 21.3 | 2.99 | 12.5 | 1.77 | 14.2 | 4.77 | 11.3 | 0.001 | 0.072 | 10.2 | 0.002 | 0.066 |
| ASMM (Kg) | 16.2 | 2.33 | 16.2 | 2.27 | 21.4 | 2.75 | 24.5 | 8.11 | 11.1 | 0.001 | 0.071 | 10.6 | 0.001 | 0.068 |
| Hydration without grass (%) | 68.5 | 2.12 | 68.6 | 2.53 | 68.9 | 2.29 | 67.7 | 12.5 | 10.02 | 0.002 | 0.065 | 6.82 | 0.010 | 0.045 |
| Total Water (L) | 29.6 | 3.49 | 29.6 | 3.39 | 31.8 | 5.30 | 32.2 | 5.42 | 8.58 | 0.004 | 0.057 | 6.71 | 0.011 | 0.045 |
| CONTROL GROUP | EDUCATED GROUP | ANOVA | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | PRE | POST | Effect Time | Effect Time × Group | |||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F | p | η2p | F | p | η2p | |
| Weight | 68.8 | 12.2 | 68.7 | 12.3 | 72.6 | 10.5 | 71.6 | 11.1 | 3.76 | 0.058 | 0.071 | 2.73 | 0.105 | 0.053 |
| BMI | 22.3 | 3.34 | 22.3 | 3.45 | 24.2 | 2.85 | 23.9 | 3.09 | 3.54 | 0.066 | 0.069 | 2.90 | 0.095 | 0.057 |
| FM constant hydration (%) | 16.4 | 7.56 | 16.3 | 8.05 | 17.7 | 6.31 | 16.7 | 6.65 | 3.63 | 0.063 | 0.070 | 2.60 | 0.114 | 0.051 |
| Crude FM (Kg) | 11.8 | 7.19 | 11.8 | 7.65 | 18.0 | 6.57 | 16.9 | 6.87 | 4.00 | 0.051 | 0.077 | 3.22 | 0.079 | 0.063 |
| SMM (Kg) | 29.8 | 4.29 | 29.9 | 4.55 | 16.8 | 1.47 | 18.8 | 4.83 | 4.19 | 0.046 | 0.080 | 3.85 | 0.055 | 0.074 |
| ASMM (Kg) | 22.8 | 3.33 | 22.9 | 3.51 | 32.0 | 3.23 | 35.5 | 8.46 | 3.61 | 0.064 | 0.070 | 3.49 | 0.068 | 0.068 |
| Hydration without grass (%) | 70.3 | 1.34 | 70.5 | 2.29 | 69.8 | 1.86 | 65.5 | 19.4 | 4.09 | 0.049 | 0.082 | 3.01 | 0.090 | 0.061 |
| Total Water (L) | 40.1 | 5.29 | 40.2 | 5.49 | 37.1 | 6.67 | 37.7 | 6.60 | 3.75 | 0.059 | 0.075 | 2.24 | 0.141 | 0.046 |
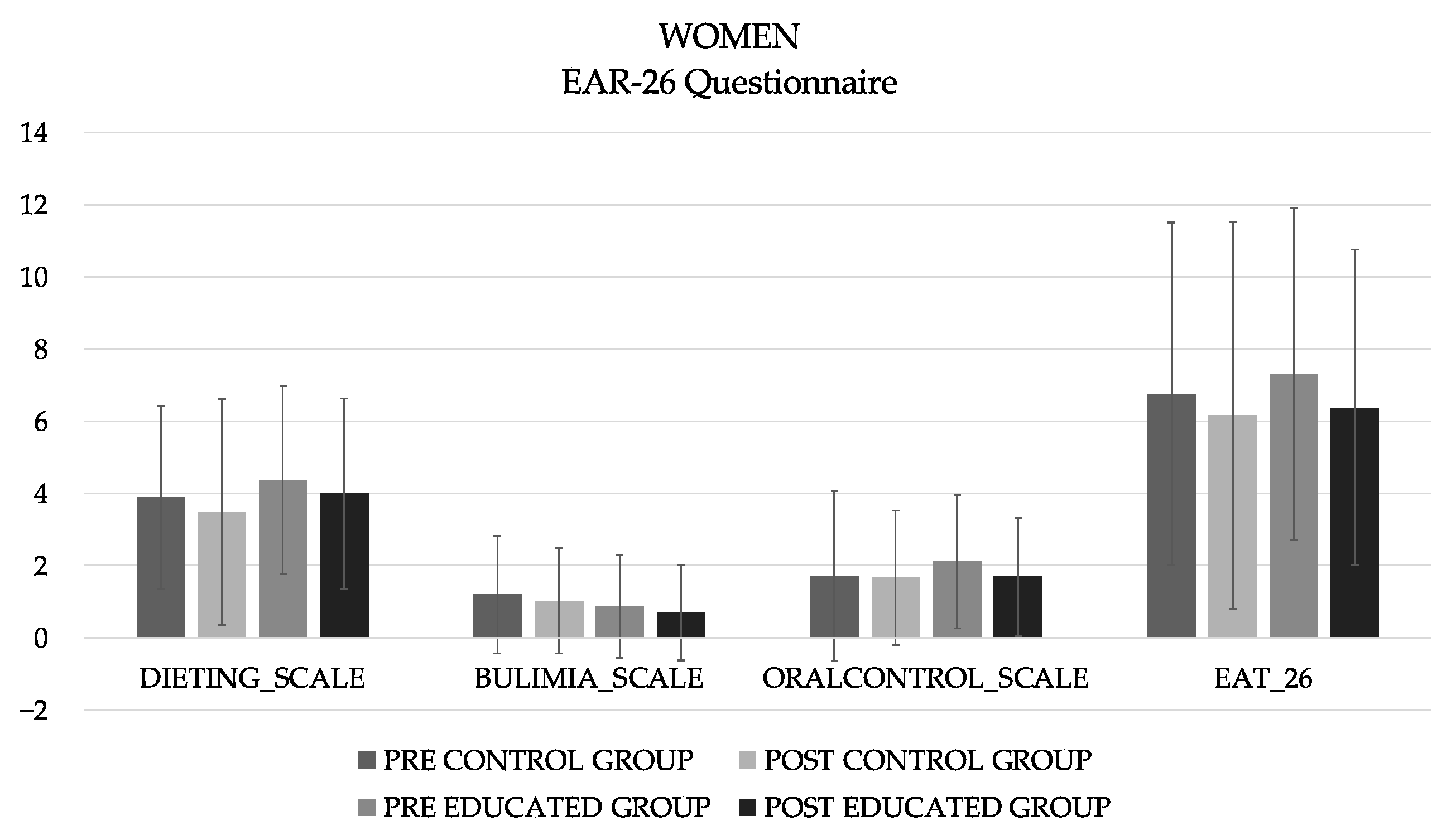
| CONTROL GROUP | EDUCATED GROUP | ANOVA | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | PRE | POST | Effect Time | Effect Time × Group | ||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | F | p | η2p | F | p | η2p |
| FEMALES | |||||||||||||
| 6.67 | 2.82 | 7.67 | 2.82 | 6.78 | 2.83 | 8.09 | 2.97 | 400.87 | < 0.001 | 0.774 | 7.13 | 0.009 | 0.057 |
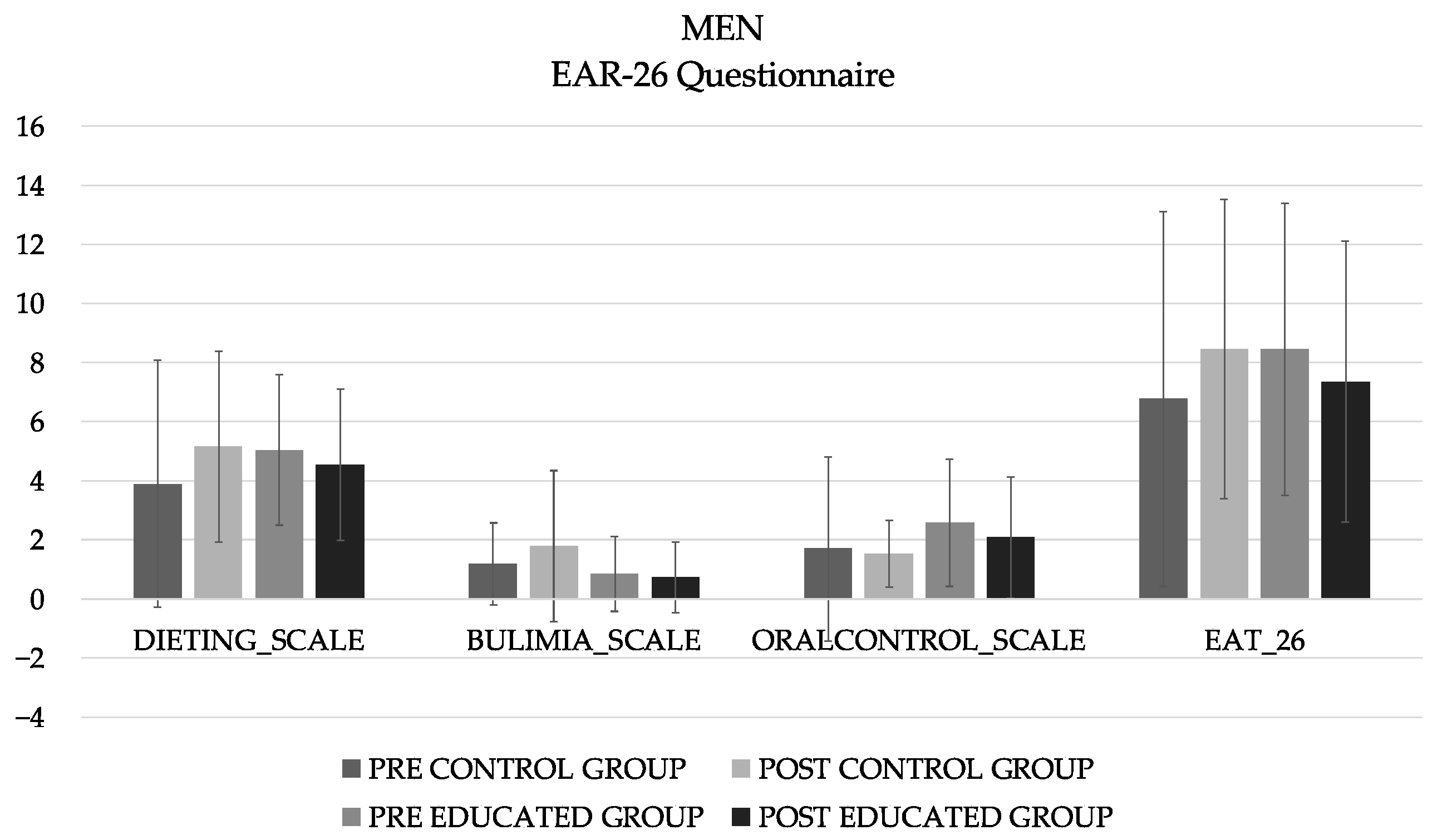
| MALES | |||||||||||||
| 7.26 | 3.19 | 8.26 | 3.19 | 7.15 | 2.62 | 8.23 | 2.61 | 135.39 | 0.001 | 0.069 | 0.18 | 0.008 | 0.048 |
| PMED | Dieting | B-F p | O-C | EAT 26 | |
|---|---|---|---|---|---|
| Weight (kg) | 0.040 | −0.177 | 0.034 | −0.202 * | −0.168 |
| BMI (kg/m2) | 0.087 | −0.179 | 0.023 | −0.159 | −0.157 |
| FMCH (%) | 0.017 | −0.200 * | −0.010 | −0.165 | −0.181 * |
| CFM (Kg) | 0.069 | −0.095 | −0.064 | −0.137 | −0.124 |
| SMM (Kg) | −0.011 | −0.076 | 0.120 | −0.163 | −0.069 |
| ASMM (Kg) | 0.117 | 0.069 | −0.025 | −0.110 | −0.006 |
| HWF (%) | 0.010 | 0.128 | 0.010 | 0.086 | 0.109 |
| TW (L) | −0.021 | 0.032 | 0.015 | −0.096 | −0.011 |
| PMED | Dieting | B-F p | O-C | EAT 26 | |
|---|---|---|---|---|---|
| Weight (kg) | −0.463 * | −0.314 * | −0.001 | −0.133 | −0.231 |
| BMI (kg/m2) | −0.475 ** | −0.409 * | −0.104 | −0.269 | −0.375 * |
| FMCH (%) | −0.359 * | −0.226 | −0.031 | −0.147 | −0.196 |
| CFM (Kg) | −0.421 * | −0.279 | −0.095 | −0.095 | −0.234 |
| SMM (Kg) | 0.023 | 0.191 | 0.309 | −0.165 | 0.175 |
| ASMM (Kg) | 0.080 | 0.071 | −0.077 | 0.029 | 0.021 |
| HWF (%) | 0.113 | 0.164 | 0.144 | 0.210 | 0.227 |
| TW (L) | −0.211 | −0.195 | 0.164 | −0.239 | −0.133 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rodríguez, A.; Vidal-Martínez, L.; Martínez-Olcina, M.; Miralles-Amorós, L.; Sánchez-Sáez, J.A.; Ramos-Campo, D.J.; Sánchez-Sánchez, J.; Martínez-Amorós, N.; Cheikh-Moussa, K.; Asencio-Mas, N.; et al. Study the Effect of an Innovative Educational Program Promoting Healthy Food Habits on Eating Disorders, Mediterranean Diet Adherence and Body Composition in University Students. Healthcare 2023, 11, 965. https://doi.org/10.3390/healthcare11070965
Martínez-Rodríguez A, Vidal-Martínez L, Martínez-Olcina M, Miralles-Amorós L, Sánchez-Sáez JA, Ramos-Campo DJ, Sánchez-Sánchez J, Martínez-Amorós N, Cheikh-Moussa K, Asencio-Mas N, et al. Study the Effect of an Innovative Educational Program Promoting Healthy Food Habits on Eating Disorders, Mediterranean Diet Adherence and Body Composition in University Students. Healthcare. 2023; 11(7):965. https://doi.org/10.3390/healthcare11070965
Chicago/Turabian StyleMartínez-Rodríguez, Alejandro, Lorena Vidal-Martínez, María Martínez-Olcina, Laura Miralles-Amorós, Juan Antonio Sánchez-Sáez, Domingo Jesús Ramos-Campo, Javier Sánchez-Sánchez, Natalia Martínez-Amorós, Kamela Cheikh-Moussa, Nuria Asencio-Mas, and et al. 2023. "Study the Effect of an Innovative Educational Program Promoting Healthy Food Habits on Eating Disorders, Mediterranean Diet Adherence and Body Composition in University Students" Healthcare 11, no. 7: 965. https://doi.org/10.3390/healthcare11070965
APA StyleMartínez-Rodríguez, A., Vidal-Martínez, L., Martínez-Olcina, M., Miralles-Amorós, L., Sánchez-Sáez, J. A., Ramos-Campo, D. J., Sánchez-Sánchez, J., Martínez-Amorós, N., Cheikh-Moussa, K., Asencio-Mas, N., Andreu-Caravaca, L., & Rubio-Arias, J. Á. (2023). Study the Effect of an Innovative Educational Program Promoting Healthy Food Habits on Eating Disorders, Mediterranean Diet Adherence and Body Composition in University Students. Healthcare, 11(7), 965. https://doi.org/10.3390/healthcare11070965