
IL-6 Enhances the Negative Impact of Cortisol on Cognition among Community-Dwelling Older People without Dementia

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
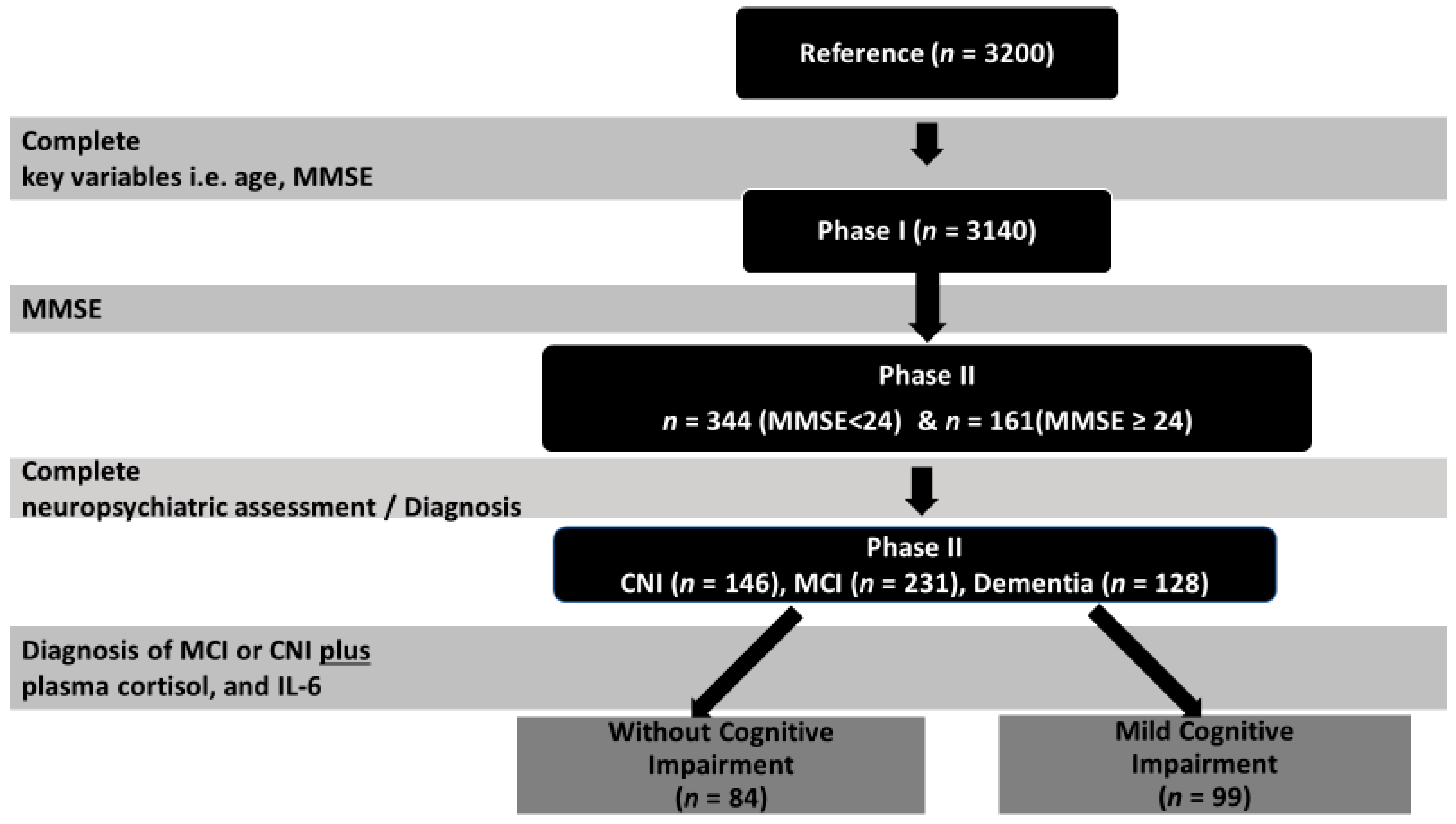
2.1. Study Design
2.2. Participants
2.3. Measurements
2.3.1. Cortisol and Inflammatory Markers
2.3.2. Executive Function Tests
- (a)
- Digit Reverse subtest from the Greek Memory Scale [53]. This subtest is considered a working memory index. The task requires the repetition of single digit sequences in reverse order, with seven difficulty levels, ranging from 2 to 8 digits. Successful repetition of all digits without additions and in correct reverse order is scored with two points, while successful repetition of all digits in correct reverse order with only one switch in the correct (reverse) order of two digits is scored with one point, with a maximum of 24 points.
- (b)
- Semantic Verbal Fluency test (SVF; [54]). In this task, the participant has to name as many words as possible that begin with a given letter within 60 s. The participant should not give words with the same root but different endings, proper names, or numbers.
- (c)
- Symbol Digit Modalities test assessing visuomotor processing speed and sustained attention (SDMT; [55]).
- (d)
- Trail Making Test Part B (TMT-B assessing set-shifting ability; [56]). The task requires the participants to trace a line that connects circled numbers and circled letters in consecutive order while alternating between numbers and letters (e.g., 1-A-2-B-3-C).
2.3.3. Emotional Status
2.4. Statistical Analysis
3. Results
3.1. Is the Relation of Basal Cortisol Levels with Executive Function Moderated by IL-6 Levels?
3.2. Is the Moderation by IL-6 Levels of the Relation of Basal Cortisol Levels with Executive Function Moderated by Diagnostic Group (CNI vs. MCI)?
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and meta-analysis. Alzheimers Dement. 2013, 9, 63–75.e2. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Dintica, C.S.; Yaffe, K. Epidemiology and Risk Factors for Dementia. Psychiatry Clin. North Am. 2022, 45, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Roozendaal, B.; McGaugh, J.L. Memory modulation. Behav. Neurosci. 2011, 125, 797–824. [Google Scholar] [CrossRef] [PubMed]
- Het, S.; Ramlow, G.; Wolf, O.T. A meta-analytic review of the effects of acute cortisol administration on human memory. Psychoneuroendocrinology 2005, 30, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Shields, G.S.; Bonner, J.C.; Moons, W.G. Does cortisol influence core executive functions? A meta-analysis of acute cortisol administration effects on working memory, inhibition, and set-shifting. Psychoneuroendocrinology 2015, 58, 91–103. [Google Scholar] [CrossRef]
- Shields, G.S.; Sazma, M.A.; McCullough, A.M.; Yonelinas, A.P. The effects of acute stress on episodic memory: A meta-analysis and integrative review. Psychol. Bull. 2017, 143, 636–675. [Google Scholar] [CrossRef]
- Segerstrom, S.; Geiger, P.; Boggero, I.; Schmitt, F.; Sephton, S. Endogenous Cortisol Exposure and Declarative Verbal Memory a Longitudinal Study of Healthy Older Adults. Psychosom. Med. 2016, 78, 182–191. [Google Scholar] [CrossRef]
- Crosswell, A.D.; Whitehurst, L.; Mendes, W.B. Effects of acute stress on cognition in older versus younger adults. Psychol. Aging 2021, 36, 241–251. [Google Scholar] [CrossRef]
- Peavy, G.M.; Santiago, D.P.; Edland, S.D. Subjective memory complaints are associated with diurnal measures of salivary cortisol in cognitively intact older adults. Am. J. Geriatr. Psychiatry 2013, 21, 925–928. [Google Scholar] [CrossRef]
- Karlamangla, A.S.; Singer, B.H.; Chodosh, J.; McEwen, B.S.; Seeman, T.E. Urinary cortisol excretion as a predictor of incident cognitive impairment. Neurobiol. Aging 2005, 26 (Suppl. S1), 80–84. [Google Scholar] [CrossRef]
- Comijs, H.C.; Gerritsen, L.; Penninx, B.W.J.H.; Bremmer, M.A.; Deeg, D.J.H.; Geerlings, M.I. The association between serum cortisol and cognitive decline in older persons. Am. J. Geriatr. Psychiatry 2010, 18, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Sudheimer, K.D.; O’Hara, R.; Spiegel, D.; Powers, B.; Kraemer, H.C.; Neri, E.; Weiner, M.; Hardan, A.; Hallmayer, J.; Dhabhar, F.S. Cortisol, cytokines, and hippocampal volume interactions in the elderly. Front. Aging Neurosci. 2014, 6, 153. [Google Scholar] [CrossRef]
- Lee, B.K.; Glass, T.A.; McAtee, M.J.; Wand, G.S.; Bandeen-Roche, K.; Bolla, K.I.; Schwartz, B.S. Associations of salivary cortisol with cognitive function in the Baltimore memory study. Arch. Gen. Psychiatry 2007, 64, 810–818. [Google Scholar] [CrossRef]
- Li, G.; Cherrier, M.M.; Tsuang, D.W.; Petrie, E.C.; Colasurdo, E.A.; Craft, S.; Schellenberg, G.D.; Peskind, E.R.; Raskind, M.A.; Wilkinson, C.W. Salivary cortisol and memory function in human aging. Neurobiol. Aging 2006, 27, 1705–1714. [Google Scholar] [CrossRef]
- Marsland, A.L.; Gianaros, P.J.; Abramowitch, S.M.; Manuck, S.B.; Hariri, A.R. Interleukin-6 covaries inversely with hippocampal grey matter volume in middle-aged adults. Biol. Psychiatry 2008, 64, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Antypa, D.; Basta, M.; Vgontzas, A.; Zaganas, I.; Panagiotakis, S.; Vogiatzi, E.; Kokosali, E.; Simos, P. The association of basal cortisol levels with episodic memory in older adults is mediated by executive function. Neurobiol. Learn Mem. 2022, 190, 107600. [Google Scholar] [CrossRef]
- Basta, M.; Vgontzas, A.N.; Fernandez-Mendoza, J.; Antypa, D.; Li, Y.; Zaganas, I.; Panagiotakis, S.; Karagkouni, E.; Simos, P. Basal Cortisol Levels Are Increased in Patients with Mild Cognitive Impairment: Role of Insomnia and Short Sleep Duration. J. Alzheimers Dis. 2022, 87, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Regen, F.; Hellmann-Regen, J.; Costantini, E.; Reale, M. Neuroinflammation and Alzheimer’s Disease: Implications for Microglial Activation. Curr. Alzheimer Res. 2017, 14, 1140–1148. [Google Scholar] [CrossRef]
- Casoli, T.; Di Stefano, G.; Balietti, M.; Solazzi, M.; Giorgetti, B.; Fattoretti, P. Peripheral inflammatory biomarkers of Alzheimer’s disease: The role of platelets. Biogerontology 2010, 11, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Grammas, P.; Martinez, J.; Miller, B. Cerebral microvascular endothelium and the pathogenesis of neurodegenerative diseases. Expert Rev. Mol. Med. 2011, 13, e19. [Google Scholar] [CrossRef] [PubMed]
- Bagyinszky, E.; Giau, V.V.; Shim, K.; Suk, K.; An, S.S.A.; Kim, S. Role of inflammatory molecules in the Alzheimer’s disease progression and diagnosis. J. Neurol. Sci. 2017, 376, 242–254. [Google Scholar] [CrossRef] [PubMed]
- Kaplin, A.; Carroll, K.A.; Cheng, J.; Allie, R.; Lyketsos, C.G.; Calabresi, P.; Rosenberg, P.B. IL-6 release by LPS-stimulated peripheral blood mononuclear cells as a potential biomarker in Alzheimer’s disease. Int. Psychogeriatr. 2009, 21, 413–414. [Google Scholar] [CrossRef]
- Yang, L.; Lu, R.; Jiang, L.; Liu, Z.; Peng, Y. Expression and genetic analysis of tumor necrosis factor-alpha (TNF-alpha) G-308A polymorphism in sporadic Alzheimer’s disease in a Southern China population. Brain Res. 2009, 1247, 178–181. [Google Scholar] [CrossRef]
- Basta, M.; Koutentaki, E.; Vgontzas, A.; Zaganas, I.; Vogiatzi, E.; Gouna, G.; Bourbouli, M.; Panagiotakis, S.; Kapetanaki, S.; Fernandez-Mendoza, J.; et al. Objective Daytime Napping is Associated with Disease Severity and Inflammation in Patients with Mild to Moderate Dementia1. J. Alzheimers Dis. 2020, 74, 803–815. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Kono, K.; Umegaki, H.; Yamada, K.; Iguchi, A.; Fukatsu, T.; Nakashima, N.; Nishiwaki, H.; Shimada, Y.; Sugita, Y.; et al. Decreased interleukin-6 level in the cerebrospinal fluid of patients with Alzheimer-type dementia. Neurosci. Lett. 1995, 186, 219–221. [Google Scholar] [CrossRef]
- Richartz, E.; Stransky, E.; Batra, A.; Simon, P.; Lewczuk, P.; Buchkremer, G.; Bartels, M.; Schott, K. Decline of immune responsiveness: A pathogenetic factor in Alzheimer’s disease? J. Psychiatry Res. 2005, 39, 535–543. [Google Scholar] [CrossRef]
- Yasutake, C.; Kuroda, K.; Yanagawa, T.; Okamura, T.; Yoneda, H. Serum BDNF, TNF-alpha and IL-1beta levels in dementia patients: Comparison between Alzheimer’s disease and vascular dementia. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 402–406. [Google Scholar] [CrossRef]
- Tarkowski, E.; Liljeroth, A.M.; Minthon, L.; Tarkowski, A.; Wallin, A.; Blennow, K. Cerebral pattern of pro-and anti-inflammatory cytokines in dementias. Brain Res. Bull. 2003, 61, 255–260. [Google Scholar] [CrossRef]
- Geerlings, M.I.; Sigurdsson, S.; Eiriksdottir, G.; Garcia, M.E.; Harris, T.B.; Gudnason, V.; Launer, L.J. Salivary cortisol, brain volumes, and cognition in community-dwelling elderly without dementia. Neurology 2015, 85, 976–983. [Google Scholar] [CrossRef]
- Yeram, N.; Dalvi, S.; Mankeshwar, R.; Patil, V.; Kale, V.; Jagiasi, K.; Abichandani, L. Relationship between cortisol, Interleukin-6 and homocysteine in Alzheimer’s disease. Qatar Med. J. 2021, 2021, 1–10. [Google Scholar] [CrossRef]
- Seeman, T.E.; McEwen, B.S.; Singer, B.H.; Albert, M.S.; Rowe, J.W. Increase in urinary cortisol excretion and memory declines: MacArthur studies of successful aging. J. Clin. Endocrinol. Metab. 1997, 82, 2458–2465. [Google Scholar] [CrossRef]
- Tanabe, J.L.; Amend, D.; Schuff, N.; DiSclafani, V.; Ezekiel, F.; Norman, D.; Fein, G.; Weiner, M.W. Tissue segmentation of the brain in Alzheimer disease. AJNR Am. J. Neuroradiol. 1997, 18, 115–123. [Google Scholar] [PubMed]
- Elenkov, I.J.; Chrousos, G.P. Stress hormones, proinflammatory and antiinflammatory cytokines, and autoimmunity. Ann. N. Y. Acad. Sci. 2002, 966, 290–303. [Google Scholar] [CrossRef]
- Marques-Deak, A.; Cizza, G.; Sternberg, E. Brain-immune interactions and disease susceptibility. Mol. Psychiatry 2005, 10, 239–250. [Google Scholar] [CrossRef]
- Hermann, C.; von Aulock, S.; Dehus, O.; Keller, M.; Okigami, H.; Gantner, F.; Wendel, A.; Hartung, T. Endogenous cortisol determines the circadian rhythm of lipopolysaccharide–but not lipoteichoic acid–inducible cytokine release. Eur. J. Immunol. 2006, 36, 371–379. [Google Scholar] [CrossRef]
- Chapman, P.B.; Lester, T.J.; Casper, E.S.; Gabrilove, J.L.; Wong, G.Y.; Kempin, S.J.; Gold, P.J.; Welt, S.; Warren, R.S.; Starnes, H.F. Clinical pharmacology of recombinant human tumor necrosis factor in patients with advanced cancer. J. Clin. Oncol. 1987, 5, 1942–1951. [Google Scholar] [CrossRef] [PubMed]
- Spath-Schwalbe, E.; Hansen, K.; Schmidt, F.; Schrezenmeier, H.; Marshall, L.; Burger, K.; Fehm, H.L.; Born, J. Acute effects of recombinant human interleukin-6 on endocrine and central nervous sleep functions in healthy men. J. Clin. Endocrinol. Metab. 1998, 83, 1573–1579. [Google Scholar] [CrossRef]
- Jonat, C.; Rahmsdorf, H.J.; Park, K.K.; Cato, A.C.; Gebel, S.; Ponta, H.; Herrlich, P. Antitumor promotion and antiinflammation: Down-modulation of AP-1 (Fos/Jun) activity by glucocorticoid hormone. Cell 1990, 62, 1189–1204. [Google Scholar] [CrossRef] [PubMed]
- Pariante, C.M.; Pearce, B.D.; Pisell, T.L.; Sanchez, C.I.; Po, C.; Su, C.; Miller, A.H. The proinflammatory cytokine, interleukin-1alpha, reduces glucocorticoid receptor translocation and function. Endocrinology 1999, 140, 4359–4366. [Google Scholar] [CrossRef]
- Pace, T.W.W.; Hu, F.; Miller, A.H. Cytokine-effects on glucocorticoid receptor function: Relevance to glucocorticoid resistance and the pathophysiology and treatment of major depression. BrainBehav. Immun. 2007, 21, 9–19. [Google Scholar] [CrossRef]
- Weaver, J.D.; Huang, M.H.; Albert, M.; Harris, T.; Rowe, J.W.; Seeman, T.E. Interleukin-6 and risk of cognitive decline: MacArthur studies of successful aging. Neurology 2002, 59, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Cabeza, R.; Nyberg, L. Neural bases of learning and memory: Functional neuroimaging evidence. Curr. Opin. Neurol. 2000, 13, 415–421. [Google Scholar] [CrossRef]
- Lupien, S.; de Leon, M.; de Santi, S.; Convit, A.; Tarshish, C.; Nair, N.; Thakur, M.; McEwen, B.S.; Hauger, R.; Meaney, M. Cortisol levels during human aging predict hippocampal atrophy and memory deficits. Nat. Neurosci. 1998, 1, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Stomby, A.; Boraxbekk, C.J.; Lundquist, A.; Nordin, A.; Nilsson, L.G.; Adolfsson, R.; Nyberg, L.; Olsson, T. Higher diurnal salivary cortisol levels are related to smaller prefrontal cortex surface area in elderly men and women. Eur. J. Endocrinol. 2016, 175, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Zaganas, I.V.; Simos, P.; Basta, M.; Kapetanaki, S.; Panagiotakis, S.; Koutentaki, I.; Fountoulakis, N.; Bertsias, A.; Duijker, G.; Tziraki, C.; et al. The Cretan Aging Cohort: Cohort Description and Burden of Dementia and Mild Cognitive Impairment. Am. J. Alzheimer’s Dis. Other Dement. 2019, 34, 23–33. [Google Scholar] [CrossRef]
- Basta, M.; Simos, P.; Vgontzas, A.; Koutentaki, E.; Tziraki, S.; Zaganas, I.; Panagiotakis, S.; Kapetanaki, S.; Fountoulakis, N.; Lionis, C. Associations between sleep duration and cognitive impairment in mild cognitive impairment. J. Sleep Res. 2019, 28, e12864. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Tsolaki, M.; Iacovides, A.; Yesavage, J.; O’Hara, R.; Kazis, A.; Ierodiakonou, C. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging 1999, 11, 367–372. [Google Scholar] [CrossRef]
- Dardiotis, E.; Kosmidis, M.H.; Yannakoulia, M.; Hadjigeorgiou, G.M.; Scarmeas, N. The Hellenic Longitudinal Investigation of Aging and Diet (HELIAD): Rationale, Study Design, and Cohort Description. Neuroepidemiology 2014, 43, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.-O.; Nordberg, A.; Backman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment-beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Zink, N.; Lenartowicz, A.; Markett, S. A new era for executive function research: On the transition from centralized to distributed executive functioning. Neurosci. Biobehav. Rev. 2021, 124, 235–244. [Google Scholar] [CrossRef]
- Simos, P.; Papastefanakis, E.; Panou, T.; Kasselimis, D. The Greek Memory Scale; Laboratory of Applied Psychology, University of Crete: Rethymno, Greece, 2011. [Google Scholar]
- Kosmidis, M.H.; Vlahou, C.H.; Panagiotaki, P.; Kiosseoglou, G. The verbal fluency task in the Greek population: Normative data, and clustering and switching strategies. J. Int. Neuropsychol. Soc. 2004, 10, 164–172. [Google Scholar] [CrossRef]
- Constantinidou, F.; Wertheimer, J.C.; Tsanadis, J.; Evans, C.; Paul, D.R. Assessment of executive functioning in brain injury: Collaboration between speech-language pathology and neuropsychology for an integrative neuropsychological perspective. Brain Inj. 2012, 26, 1549–1563. [Google Scholar] [CrossRef]
- Zalonis, I.; Kararizou, E.; Triantafyllou, N.I.; Kapaki, E.; Papageorgiou, S.; Sgouropoulos, P.; Vassilopoulos, D. A normative study of the trail making test A and B in Greek adults. Clin. Neuropsychol. 2008, 22, 842–850. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.; Kokmen, E.; Ivnik, R.J.; Tangalos, E.G. Memory function in normal aging. Neurology 1992, 42, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Constantinidou, F.; Zaganas, I.; Papastefanakis, E.; Kasselimis, D.; Nidos, A.; Simos, P.G. Age-related decline in verbal learning is moderated by demographic factors, working memory capacity, and presence of amnestic mild cognitive impairment. J. Int. Neuropsychol. Soc. 2014, 20, 822–835. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Steptoe, A.; Owen, N.; Kunz-Ebrecht, S.; Mohamed-Ali, V. Inflammatory cytokines, socioeconomic status, and acute stress responsivity. Brain Behav. Immun. 2002, 16, 774–784. [Google Scholar] [CrossRef] [PubMed]
- Tian, R.; Hou, G.; Li, D.; Yuan, T.F. A possible change process of inflammatory cytokines in the prolonged chronic stress and its ultimate implications for health. Sci. World J. 2014, 2014, 780616. [Google Scholar] [CrossRef]
- Mastorakos, G.; Chrousos, G.P.; Weber, J.S. Recombinant interleukin-6 activates the hypothalamic-pituitary-adrenal axis in humans. J. Clin. Endocrinol. Metab. 1993, 77, 1690–1694. [Google Scholar] [CrossRef] [PubMed]
- Besedovsky, H.O.; del Rey, A. The cytokine-HPA axis feed-back circuit. Z. Für Rheumatol. 2000, 59 (Suppl. S2), II26–II30. [Google Scholar] [CrossRef]
- Lara, V.P.; Caramelli, P.; Teixeira, A.L.; Barbosa, M.T.; Carmona, K.C.; Carvalho, M.G.; Fernandes, A.P.; Gomes, K.B. High cortisol levels are associated with cognitive impairment no-dementia (CIND) and dementia. Clin. Chim. Acta 2013, 423, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.Y.; Schuff, N.; Du, A.T.; Mark, K.; Zhu, X.; Hardin, D.; Weiner, M.W. Comparison of automated and manual MRI volumetry of hippocampus in normal aging and dementia. J. Magn. Reson. Imaging 2002, 16, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Pickering, M.; O’Connor, J.J. Pro-inflammatory cytokines and their effects in the dentate gyrus. Prog. Brain Res. 2007, 163, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Baune, B.T.; Konrad, C.; Grotegerd, D.; Suslow, T.; Ohrmann, P.; Bauer, J.; Arolt, V.; Heindel, W.; Domschke, K.; Schöning, S.; et al. Tumor necrosis factor gene variation predicts hippocampus volume in healthy individuals. Biol. Psychiatry 2012, 72, 655–662. [Google Scholar] [CrossRef]
- Kunz-Ebrecht, S.R.; Mohamed-Ali, V.; Feldman, P.J.; Kirschbaum, C.; Steptoe, A. Cortisol responses to mild psychological stress are inversely associated with proinflammatory cytokines. Brain Behav. Immun. 2003, 17, 373–383. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; Preacher, K.J.; MacCallum, R.C.; Atkinson, C.; Malarkey, W.B.; Glaser, R. Chronic stress and age-related increases in the proinflammatory cytokine IL-6. Proc. Natl. Acad. Sci. USA 2003, 100, 9090–9095. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Zoumakis, M.; Bixler, E.O.; Lin, H.M.; Prolo, P.; Vela-Bueno, A.; Kales, A.; Chrousos, G.P. Impaired nighttime sleep in healthy old versus young adults is associated with elevated plasma interleukin-6 and cortisol levels: Physiologic and therapeutic implications. J. Clin. Endocrinol. Metab. 2003, 88, 2087–2095. [Google Scholar] [CrossRef]
- Casaletto, K.B.; Staffaroni, A.M.; Elahi, F.; Fox, E.; Crittenden, P.A.; You, M.; Neuhaus, J.; Glymour, M.; Bettcher, B.M.; Yaffe, K.; et al. Perceived Stress is Associated with Accelerated Monocyte/Macrophage Aging Trajectories in Clinically Normal Adults. Am. J. Geriatr. Psychiatry 2018, 26, 952–963. [Google Scholar] [CrossRef]
- Franceschi, C.; Bonafè, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging: An Evolutionary Perspective on Immunosenescence. Ann. N. Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef]
- Gomez, C.R.; Boehmer, E.D.; Kovacs, E.J. The aging innate immune system. Curr. Opin. Immunol. 2005, 17, 457–462. [Google Scholar] [CrossRef]
- Franz, C.E.; O’Brien, R.C.; Hauger, R.L.; Mendoza, S.P.; Panizzon, M.S.; Prom-Wormley, E.; Eaves, L.J.; Jacobson, K.; Lyons, M.J.; Lupien, S.; et al. Cross-sectional and 35-year longitudinal assessment of salivary cortisol and cognitive functioning: The Vietnam Era Twin Study of Aging. Psychoneuroendocrinology 2011, 36, 1040–1052. [Google Scholar] [CrossRef]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef]
- Nikisch, G. Involvement and role of antidepressant drugs of the hypothalamic-pituitary-adrenal axis and glucocorticoid receptor function. Neuro. Endocrinol. Lett. 2009, 30, 11–16. [Google Scholar]
- Budziszewska, B. Effect of antidepressant drugs on the hypothalamic-pituitary-adrenal axis activity and glucocorticoid receptor function. Pol. J. Pharmacol. 2002, 54, 343–349. [Google Scholar] [PubMed]
- Tafet, G.E.; Nemeroff, C.B. Pharmacological Treatment of Anxiety Disorders: The Role of the HPA Axis. Front. Psychiatry 2020, 11, 443. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Puzino, K.; Fernandez-Mendoza, J.; Krishnamurthy, V.B.; Basta, M.; Bixler, E.O. Effects of Trazodone vs. Cognitive Behavioral Therapy in the Insomnia with Short Sleep Duration Phenotype: A Preliminary Study. J. Clin. Sleep Med. 2020, 16, 2009–2019. [Google Scholar] [CrossRef]
- Oberman, K.; Hovens, I.; de Haan, J.; Falcao-Salles, J.; van Leeuwen, B.; Schoemaker, R. Acute pre-operative ibuprofen improves cognition in a rat model for postoperative cognitive dysfunction. J. Neuroinflammation 2021, 18, 156. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.T.; Liu, C.C.; Zhao, N.; Wang, J.; Putzke, T.; Yang, L.; Shinohara, M.; Fryer, J.D.; Kanekiyo, T.; Bu, G. Subacute ibuprofen treatment rescues the synaptic and cognitive deficits in advanced-aged mice. Neurobiol. Aging. 2017, 53, 112–121. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Sample | CNI Group | MCI Group | p Value | |
|---|---|---|---|---|
| N | 183 | 84 | 99 | |
| Age (years) | 73.8 ± 7.0 | 72.7 ± 7.4 | 75.3 ± 6.4 | 0.01 |
| Education (years) | 5.37 ± 3.1 | 5.82 ± 2.93 | 4.83 ± 3.25 | 0.2 |
| Gender (%) | 0.2 | |||
| Women | 67.7 | 65.5 | 74.7 | |
| Men | 32.2 | 34.5 | 25.3 | |
| BMI (kg/m2) | 30.0 ± 4.79 | 30.32 ± 5.06 | 29.59 ± 4.44 | 0.4 |
| Waist circumference (cm) | 102.8 ± 3.5 | 103.4 ± 13.2 | 102.3 ± 11.3 | 0.6 |
| Marital status (%) | 0.3 | |||
| Single/divorced | 5.0 | 3.6 | 7.1 | |
| Married | 73.2 | 77.1 | 67.7 | |
| Widowed | 21.8 | 21.4 | 25.3 | |
| GDS | 3.71 ± 3.50 | 3.22 ± 3.46 | 4.12 ± 3.53 | 0.09 |
| MMSE score | 24.72 ± 3.56 | 26.89 ± 2.90 | 22.89 ± 3.00 | <0.001 |
| Cortisol (ng/mL) | 76.4 ± 123.6 | 60.5 ± 137.6 | 72.7 ± 118.2 | 0.024 |
| IL6 (pg/mL) | 1.31 ± 0.81 | 1.28 ± 0.91 | 1.34 ± 0.71 | 0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koutentaki, E.; Basta, M.; Antypa, D.; Zaganas, I.; Panagiotakis, S.; Simos, P.; Vgontzas, A.N. IL-6 Enhances the Negative Impact of Cortisol on Cognition among Community-Dwelling Older People without Dementia. Healthcare 2023, 11, 951. https://doi.org/10.3390/healthcare11070951
Koutentaki E, Basta M, Antypa D, Zaganas I, Panagiotakis S, Simos P, Vgontzas AN. IL-6 Enhances the Negative Impact of Cortisol on Cognition among Community-Dwelling Older People without Dementia. Healthcare. 2023; 11(7):951. https://doi.org/10.3390/healthcare11070951
Chicago/Turabian StyleKoutentaki, Eirini, Maria Basta, Despina Antypa, Ioannis Zaganas, Symeon Panagiotakis, Panagiotis Simos, and Alexandros N. Vgontzas. 2023. "IL-6 Enhances the Negative Impact of Cortisol on Cognition among Community-Dwelling Older People without Dementia" Healthcare 11, no. 7: 951. https://doi.org/10.3390/healthcare11070951
APA StyleKoutentaki, E., Basta, M., Antypa, D., Zaganas, I., Panagiotakis, S., Simos, P., & Vgontzas, A. N. (2023). IL-6 Enhances the Negative Impact of Cortisol on Cognition among Community-Dwelling Older People without Dementia. Healthcare, 11(7), 951. https://doi.org/10.3390/healthcare11070951