


Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood



Abstract
1. Laying the Groundwork
2. A Life Course Perspective
2.1. Autism Spectrum Disorder
2.2. Attention-Deficit/Hyperactivity Disorder
2.3. Specific Learning Disorders
2.4. Intellectual Disability
2.5. Communication Disorders
2.6. Motor Disorders
2.6.1. Developmental Coordination Disorder
2.6.2. Tic Disorders and Tourette Syndrome
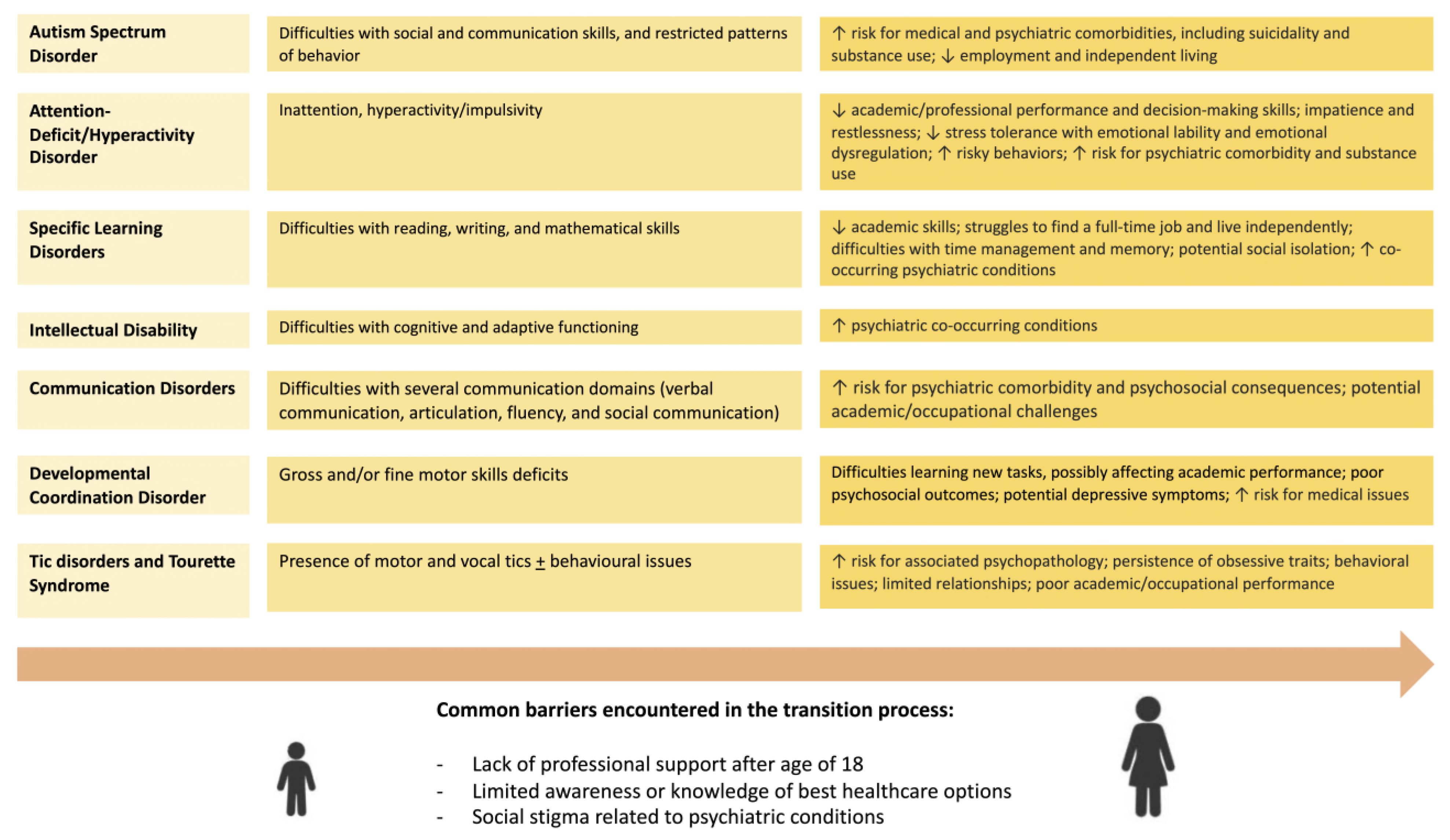
3. Raising Concern about the Transition Process: The State of the Art and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parenti, I.; Rabaneda, L.G.; Schoen, H.; Novarino, G. Neurodevelopmental Disorders: From Genetics to Functional Pathways. Trends Neurosci. 2020, 43, 608–621. [Google Scholar] [CrossRef] [PubMed]
- Morris-Rosendahl, D.J.; Crocq, M.A. Neurodevelopmental Disorders-the History and Future of a Diagnostic Concept. Dialogues Clin. Neurosci. 2020, 22, 65–72. [Google Scholar] [CrossRef]
- Thapar, A.; Cooper, M.; Rutter, M. Neurodevelopmental Disorders. Lancet Psychiatry 2017, 4, 339–346. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar]
- Dougnon, G.; Matsui, H. Modelling Autism Spectrum Disorder (ASD) and Attention-Deficit/Hyperactivity Disorder (ADHD) Using Mice and Zebrafish. Int. J. Mol. Sci. 2022, 23, 7550. [Google Scholar] [CrossRef]
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, D. ADHD in Children and Young People: Prevalence, Care Pathways, and Service Provision. Lancet Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Water-Related Diseases and Contaminants in Public Water Systems. U.S. Department of Health and Human Services. 2014. Available online: https://www.cdc.gov/healthywater/drinking/public/water_diseases.html (accessed on 25 March 2023).
- Groth, C. Tourette Syndrome in a Longitudinal Perspective. Clinical Course of Tics and Comorbidities, Coexisting Psychopathologies, Phenotypes and Predictors. Dan. Med. J. 2018, 65, B5465. [Google Scholar] [PubMed]
- Bosia, M.; Seghi, F.; Bigai, G.; Martini, F.; Fregna, L.; Fazio, V.; Cavallaro, R. Adult Consequences of Neurodevelopmental Disorders. In Fundamentals of Psychiatry for Health Care Professionals; Cavallaro, R., Colombo, C., Eds.; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Barahona Corrêa, B.; van der Gaag, R.-J. Autism Spectrum Disorders in Adults; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Salvador-Carulla, L.; Reed, G.M.; Vaez-Azizi, L.M.; Cooper, S.A.; Martinez-Leal, R.; Bertelli, M.; Adnams, C.; Cooray, S.; Deb, S.; Akoury-Dirani, L.; et al. Intellectual Developmental Disorders: Towards a New Name, Definition and Framework for “Mental Retardation/Intellectual Disability” in ICD-11. World Psychiatry 2011, 10, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Maulik, P.K.; Mascarenhas, M.N.; Mathers, C.D.; Dua, T.; Saxena, S. Prevalence of Intellectual Disability: A Meta-Analysis of Population-Based Studies. Res. Dev. Disabil. 2011, 32, 419–436. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, P.; Carlström, E.; Råstam, M.; Gillberg, C.; Anckarsäter, H. The Genetics of Autism Spectrum Disorders and Related Neuropsychiatric Disorders in Childhood. Am. J. Psychiatry 2010, 167, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Chiurazzi, P.; Pirozzi, F. Advances in Understanding—Genetic Basis of Intellectual Disability. F1000Research 2016, 5, 599. [Google Scholar] [CrossRef]
- Wright, C.F.; Fitzgerald, T.W.; Jones, W.D.; Clayton, S.; McRae, J.F.; Van Kogelenberg, M.; King, D.A.; Ambridge, K.; Barrett, D.M.; Bayzetinova, T.; et al. Genetic Diagnosis of Developmental Disorders in the DDD Study: A Scalable Analysis of Genome-Wide Research Data. Lancet 2015, 385, 1305–1314. [Google Scholar] [CrossRef]
- Roessner, V.; Hoekstra, P.J. European Multicenter Tics in Children Studies (EMTICS): Exploring the Onset and Course of Tic Disorders. Eur. Child Adolesc. Psychiatry 2013, 22, 451–452. [Google Scholar] [CrossRef] [PubMed]
- Kalkbrenner, A.E.; Braun, J.M.; Durkin, M.S.; Maenner, M.J.; Cunniff, C.; Lee, L.C.; Pettygrove, S.; Nicholas, J.S.; Daniels, J.L. Maternal Smoking during Pregnancy and the Prevalence of Autism Spectrum Disorders, Using Data from the Autism and Developmental Disabilities Monitoring Network. Environ. Health Perspect. 2012, 120, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Atladóttir, H.Ó.; Thorsen, P.; Østergaard, L.; Schendel, D.E.; Lemcke, S.; Abdallah, M.; Parner, E.T. Maternal Infection Requiring Hospitalization during Pregnancy and Autism Spectrum Disorders. J. Autism Dev. Disord. 2010, 40, 1423–1430. [Google Scholar] [CrossRef]
- Maher, G.M.; O’Keeffe, G.W.; Kearney, P.M.; Kenny, L.C.; Dinan, T.G.; Mattsson, M.; Khashan, A.S. Association of Hypertensive Disorders of Pregnancy with Risk of Neurodevelopmental Disorders in Offspring a Systematic Review and Meta-Analysis. JAMA Psychiatry 2018, 75, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Ornoy, A.; Becker, M.; Weinstein-Fudim, L.; Ergaz, Z. Diabetes during Pregnancy: A Maternal Disease Complicating the Course of Pregnancy with Long-Term Deleterious Effects on the Offspring. a Clinical Review. Int. J. Mol. Sci. 2021, 22, 2965. [Google Scholar] [CrossRef]
- Carlsson, T.; Molander, F.; Taylor, M.J.; Jonsson, U.; Bölte, S. Early Environmental Risk Factors for Neurodevelopmental Disorders-A Systematic Review of Twin and Sibling Studies. Dev. Psychopathol. 2020, 33, 1448–1495. [Google Scholar] [CrossRef]
- Van Karnebeek, C.D.M.; Shevell, M.; Zschocke, J.; Moeschler, J.B.; Stockler, S. The Metabolic Evaluation of the Child with an Intellectual Developmental Disorder: Diagnostic Algorithm for Identification of Treatable Causes and New Digital Resource. Mol. Genet. Metab. 2014, 111, 428–438. [Google Scholar] [CrossRef]
- Patel, D.R.; Cabral, M.D.; Ho, A.; Merrick, J. A Clinical Primer on Intellectual Disability. Transl. Pediatr. 2020, 9, S23–S35. [Google Scholar] [CrossRef]
- Rutter, M.; Kim-Cohen, J.; Maughan, B. Continuities and Discontinuities in Psychopathology between Childhood and Adult Life. J. Child Psychol. Psychiatry Allied Discip. 2006, 47, 276–295. [Google Scholar] [CrossRef]
- Magiati, I.; Tay, X.W.; Howlin, P. Cognitive, Language, Social and Behavioural Outcomes in Adults with Autism Spectrum Disorders: A Systematic Review of Longitudinal Follow-up Studies in Adulthood. Clin. Psychol. Rev. 2014, 34, 78–86. [Google Scholar] [CrossRef]
- Faraone, S.V.; Biederman, J.; Mick, E. The Age-Dependent Decline of Attention Deficit Hyperactivity Disorder: A Meta-Analysis of Follow-up Studies. Psychol. Med. 2006, 36, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Simon, V.; Czobor, P.; Bálint, S.; Mészáros, Á.; Bitter, I. Prevalence and Correlates of Adult Attention-Deficit Hyperactivity Disorder: Meta-Analysis. Br. J. Psychiatry 2009, 194, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Howlin, P.; Goode, S.; Hutton, J.; Rutter, M. Adult Outcome for Children with Autism. J. Child Psychol. Psychiatry Allied Discip. 2004, 45, 212–229. [Google Scholar] [CrossRef]
- Anderson, D.K.; Liang, J.W.; Lord, C. Predicting Young Adult Outcome among More and Less Cognitively Able Individuals with Autism Spectrum Disorders. J. Child Psychol. Psychiatry 2014, 55, 485–494. [Google Scholar] [CrossRef]
- Klein, R.H.; Mannuzza, S.; Olazagasti, M.A.R.; Roizen, E.; Hutchison, J.A.; Lashua, E.C.; Castellanos, F.X. Clinical and Functional Outcome of Childhood Attention-Deficit/Hyperactivity Disorder 33 Years Later. Arch. Gen. Psychiatry 2012, 69, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Posar, A.; Visconti, P. Long-Term Outcome of Autism Spectrum Disorder. Turk. Pediatr. Ars. 2019, 54, 207–212. [Google Scholar] [CrossRef]
- Bennett, A.E.; Miller, J.S.; Stollon, N.; Prasad, R.; Blum, N.J.; Bennett, A.E. Autism Spectrum Disorder and Transition-Aged Youth. Curr. Psychiatry Rep. 2018, 20, 103. [Google Scholar] [CrossRef]
- Wise, E.A. Aging in Autism Spectrum Disorder. Am. J. Geriatr. Psychiatry 2020, 28, 339–349. [Google Scholar] [CrossRef]
- Cheak-Zamora, N.; Yang, X.; Farmer, J.; Clark, M. Disparities in Transition Planning for Youth with Autism Spectrum Disorder. Pediatrics 2013, 131, 447–454. [Google Scholar] [CrossRef]
- Volkmar, F.R.; Jackson, S.L.; Hart, L. Transition Issues and Challenges for Youth with Autism Spectrum Disorders. Pediatr. Ann. 2017, 46, e219–e223. [Google Scholar] [CrossRef]
- Croen, L.A.; Zerbo, O.; Qian, Y.; Massolo, M.L.; Rich, S.; Sidney, S.; Kripke, C. The Health Status of Adults on the Autism Spectrum. Autism 2015, 19, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Tyler, C.V.; Schramm, S.C.; Karafa, M.; Tang, A.S.; Jain, A.K. Chronic Disease Risks in Young Adults with Autism Spectrum Disorder: Forewarned Is Forearmed. Am. J. Intellect. Dev. Disabil. 2011, 116, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Fortuna, R.J.; Robinson, L.; Smith, T.H.; Meccarello, J.; Bullen, B.; Nobis, K.; Davidson, P.W. Health Conditions and Functional Status in Adults with Autism: A Cross-Sectional Evaluation. J. Gen. Intern. Med. 2016, 31, 77–84. [Google Scholar] [CrossRef]
- Vasa, R.A.; Mazurek, M.O. An Update on Anxiety in Youth with Autism Spectrum Disorders. Curr. Opin. Psychiatry 2015, 28, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric Disorders in Children with Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef]
- Kraper, C.K.; Kenworthy, L.; Popal, H.; Martin, A.; Wallace, G.L. The Gap Between Adaptive Behavior and Intelligence in Autism Persists into Young Adulthood and Is Linked to Psychiatric Co-Morbidities. J. Autism Dev. Disord. 2017, 47, 3007–3017. [Google Scholar] [CrossRef]
- Gotham, K.; Marvin, A.R.; Taylor, J.L.; Warren, Z.; Anderson, C.M.; Law, P.A.; Law, J.K.; Lipkin, P.H. Characterizing the Daily Life, Needs, and Priorities of Adults with Autism Spectrum Disorder from Interactive Autism Network Data. Autism 2015, 19, 794–804. [Google Scholar] [CrossRef]
- Buck, T.R.; Viskochil, J.; Farley, M.; Coon, H.; McMahon, W.M.; Morgan, J.; Bilder, D.A. Psychiatric Comorbidity and Medication Use in Adults with Autism Spectrum Disorder. J. Autism Dev. Disord. 2014, 44, 3063–3071. [Google Scholar] [CrossRef]
- Lever, A.G.; Geurts, H.M. Psychiatric Co-Occurring Symptoms and Disorders in Young, Middle-Aged, and Older Adults with Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 1916–1930. [Google Scholar] [CrossRef]
- Howlin, P. Outcome in Adult Life for More Able Individuals with Autism or Asperger Syndrome. Autism 2000, 4, 63–83. [Google Scholar] [CrossRef]
- Richa, S.; Fahed, M.; Khoury, E.; Mishara, B. Suicide in Autism Spectrum Disorders. Arch. Suicide Res. 2014, 18, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Mayes, S.D.; Gorman, A.A.; Hillwig-Garcia, J.; Syed, E. Suicide Ideation and Attempts in Children with Autism. Res. Autism Spectr. Disord. 2013, 7, 109–119. [Google Scholar] [CrossRef]
- Shavelle, R.; Strauss, D.; Pickett, J. Causes of Death in Autism. J. Autism Dev. Disord. 2001, 31, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Schendel, D.E.; Overgaard, M.; Christensen, J.; Hjort, L.; Jørgensen, M.; Vestergaard, M.; Parner, E.T. Association of Psychiatric and Neurologic Comorbidity With Mortality Among Persons With Autism Spectrum Disorder in a Danish Population. JAMA Pediatr. 2016, 170, 243–250. [Google Scholar] [CrossRef]
- Hirvikoski, T.; Mittendorfer-Rutz, E.; Boman, M.; Larsson, H.; Lichtenstein, P.; Bölte, S. Premature Mortality in Autism Spectrum Disorder. Br. J. Psychiatry 2016, 208, 232–238. [Google Scholar] [CrossRef]
- Isager, T.; Mouridsen, S.E.; Rich, B. Mortality and Causes of Death in Pervasive Developmental Disorders. Autism 1999, 3, 7–16. [Google Scholar] [CrossRef]
- Mouridsen, S.E.; Brønnum-Hansen, H.; Rich, B.; Isager, T. Mortality and Causes of Death in Autism Spectrum Disorders: An Update. Autism 2008, 12, 403–414. [Google Scholar] [CrossRef]
- Guan, J.; Li, G. Injury Mortality in Individuals with Autism. Am. J. Public Health 2017, 107, 791–793. [Google Scholar] [CrossRef]
- Smith DaWalt, L.; Hong, J.; Greenberg, J.S.; Mailick, M.R. Mortality in Individuals with Autism Spectrum Disorder: Predictors over a 20-Year Period. Autism 2019, 23, 1732–1739. [Google Scholar] [CrossRef]
- Caamaño, M.; Boada, L.; Merchán-Naranjo, J.; Moreno, C.; Llorente, C.; Moreno, D.; Arango, C.; Parellada, M. Psychopathology in Children and Adolescents with ASD Without Mental Retardation. J. Autism Dev. Disord. 2013, 43, 2442–2449. [Google Scholar] [CrossRef]
- Hofvander, B.; Delorme, R.; Chaste, P.; Nydén, A.; Wentz, E.; Ståhlberg, O.; Herbrecht, E.; Stopin, A.; Anckarsäter, H.; Gillberg, C.; et al. Psychiatric and Psychosocial Problems in Adults with Normal-Intelligence Autism Spectrum Disorders. BMC Psychiatry 2009, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Lugnegård, T.; Hallerbäck, M.U.; Gillberg, C. Psychiatric Comorbidity in Young Adults with a Clinical Diagnosis of Asperger Syndrome. Res. Dev. Disabil. 2011, 32, 1910–1917. [Google Scholar] [CrossRef] [PubMed]
- Skokauskas, N.; Gallagher, L. Psychosis, Affective Disorders and Anxiety in Autistic Spectrum Disorder: Prevalence and Nosological Considerations. Psychopathology 2009, 43, 8–16. [Google Scholar] [CrossRef]
- Fowler, J.C. Suicide Risk Assessment in Clinical Practice: Pragmatic Guidelines for Imperfect Assessments. Psychotherapy 2012, 49, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Oquendo, M.A.; Dragatsi, D.; Harkavy-Friedman, J.; Dervic, K.; Currier, D.; Burke, A.K.; Grunebaum, M.F.; Mann, J.J. Protective Factors against Suicidal Behavior in Latinos. J. Nerv. Ment. Dis. 2005, 193, 438–443. [Google Scholar] [CrossRef]
- Chioqueta, A.P.; Stiles, T.C. The Relationship between Psychological Buffers, Hopelessness, and Suicidal Ideation: Identification of Protective Factors. Crisis 2007, 28, 67–73. [Google Scholar] [CrossRef]
- Sizoo, B.; van den Brink, W.; Koeter, M.; Gorissen van Eenige, M.; van Wijngaarden-Cremers, P.; van der Gaag, R.J. Treatment Seeking Adults with Autism or ADHD and Co-Morbid Substance Use Disorder: Prevalence, Risk Factors and Functional Disability. Drug Alcohol Depend. 2010, 107, 44–50. [Google Scholar] [CrossRef]
- Butwicka, A.; Långström, N.; Larsson, H.; Lundström, S.; Serlachius, E.; Almqvist, C.; Frisén, L.; Lichtenstein, P. Increased Risk for Substance Use-Related Problems in Autism Spectrum Disorders: A Population-Based Cohort Study. J. Autism Dev. Disord. 2017, 47, 80–89. [Google Scholar] [CrossRef]
- Clarke, T.; Tickle, A.; Gillott, A. Substance Use Disorder in Asperger Syndrome: An Investigation into the Development and Maintenance of Substance Use Disorder by Individuals with a Diagnosis of Asperger Syndrome. Int. J. Drug Policy 2016, 27, 154–163. [Google Scholar] [CrossRef]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism Spectrum Disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef]
- Poon, K.K.; Sidhu, D.J.K. Adults with Autism Spectrum Disorders: A Review of Outcomes, Social Attainment, and Interventions. Curr. Opin. Psychiatry 2017, 30, 77–84. [Google Scholar] [CrossRef]
- Howlin, P.; Moss, P. Adults with Autism Spectrum Disorders. Can. J. Psychiatry 2012, 57, 275–283. [Google Scholar] [CrossRef] [PubMed]
- White, S.W.; Elias, R.; Capriola-Hall, N.N.; Smith, I.C.; Conner, C.M.; Asselin, S.B.; Howlin, P.; Getzel, E.E.; Mazefsky, C.A. Development of a College Transition and Support Program for Students with Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 3072–3078. [Google Scholar] [CrossRef] [PubMed]
- Howlin, P.; Moss, P.; Savage, S.; Rutter, M. Social Outcomes in Mid- to Later Adulthood among Individuals Diagnosed with Autism and Average Nonverbal IQ as Children. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 572–581.e1. [Google Scholar] [CrossRef]
- Roux, A.M.; Shattuck, P.T.; Cooper, B.P.; Anderson, K.A.; Wagner, M.; Narendorf, S.C. Postsecondary Employment Experiences among Young Adults with an Autism Spectrum Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, S.; Costley, D.; Warren, A. Employment Activities and Experiences of Adults with High-Functioning Autism and Asperger’s Disorder. J. Autism Dev. Disord. 2014, 44, 2440–2449. [Google Scholar] [CrossRef] [PubMed]
- Wehman, P.H.; Schall, C.M.; McDonough, J.; Kregel, J.; Brooke, V.; Molinelli, A.; Ham, W.; Graham, C.W.; Erin Riehle, J.; Collins, H.T.; et al. Competitive Employment for Youth with Autism Spectrum Disorders: Early Results from a Randomized Clinical Trial. J. Autism Dev. Disord. 2014, 44, 487–500. [Google Scholar] [CrossRef]
- Farley, M.; Cottle, K.J.; Bilder, D.; Viskochil, J.; Coon, H.; McMahon, W. Mid-Life Social Outcomes for a Population-Based Sample of Adults with ASD. Autism Res. 2018, 11, 142–152. [Google Scholar] [CrossRef]
- Gray, K.M.; Keating, C.M.; Taffe, J.R.; Brereton, A.V.; Einfeld, S.L.; Reardon, T.C.; Tonge, B.J. Adult Outcomes in Autism: Community Inclusion and Living Skills. J. Autism Dev. Disord. 2014, 44, 3006–3015. [Google Scholar] [CrossRef]
- Anderson, K.A.; Shattuck, P.T.; Cooper, B.P.; Roux, A.M.; Wagner, M. Prevalence and Correlates of Postsecondary Residential Status among Young Adults with an Autism Spectrum Disorder. Autism 2014, 18, 562–570. [Google Scholar] [CrossRef]
- Hewitt, A.S.; Stancliffe, R.J.; Hall-Lande, J.; Nord, D.; Pettingell, S.L.; Hamre, K.; Hallas-Muchow, L. Characteristics of Adults with Autism Spectrum Disorder Who Use Residential Services and Supports through Adult Developmental Disability Services in the United States. Res. Autism Spectr. Disord. 2017, 34, 1–9. [Google Scholar] [CrossRef]
- Weibel, S.; Menard, O.; Ionita, A.; Boumendjel, M.; Cabelguen, C.; Kraemer, C.; Micoulaud-Franchi, J.A.; Bioulac, S.; Perroud, N.; Sauvaget, A.; et al. Practical Considerations for the Evaluation and Management of Attention Deficit Hyperactivity Disorder (ADHD) in Adults. Encephale 2020, 46, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Asherson, P.; Buitelaar, J.; Faraone, S.V.; Rohde, L.A. Adult Attention-Deficit Hyperactivity Disorder: Key Conceptual Issues. Lancet Psychiatry 2016, 3, 568–578. [Google Scholar] [CrossRef]
- Schatz, D.B.; Rostain, A.L. ADHD with Comorbid Anxiety. A Review of the Current Literature. J. Atten. Disord. 2006, 10, 141–149. [Google Scholar] [CrossRef]
- Larsson, H.; Dilshad, R.; Lichtenstein, P.; Barker, E.D. Developmental Trajectories of DSM-IV Symptoms of Attention-Deficit/Hyperactivity Disorder: Genetic Effects, Family Risk and Associated Psychopathology. J. Child Psychol. Psychiatry Allied Discip. 2011, 52, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Faraone, S.V. The Effects of Attention-Deficit/Hyperactivity Disorder on Employment and Household Income. Medscape Gen. Med. 2006, 8, 12. [Google Scholar]
- Doshi, J.A.; Hodgkins, P.; Kahle, J.; Sikirica, V.; Cangelosi, M.J.; Setyawan, J.; Erder, M.H.; Neumann, P.J. Economic Impact of Childhood and Adult Attention-Deficit/Hyperactivity Disorder in the United States. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 990–1002.e2. [Google Scholar] [CrossRef]
- Lichtenstein, P.; Halldner, L.; Zetterqvist, J.; Sjölander, A.; Serlachius, E.; Fazel, S.; Långström, N.; Larsson, H. Medication for Attention Deficit–Hyperactivity Disorder and Criminality. N. Engl. J. Med. 2012, 367, 2006–2014. [Google Scholar] [CrossRef]
- Chang, Z.; Lichtenstein, P.; D’Onofrio, B.M.; Sjölander, A.; Larsson, H. Serious Transport Accidents in Adults with Attention-Deficit/Hyperactivity Disorder and the Effect of Medication: A Population-Based Study. JAMA Psychiatry 2014, 71, 319–325. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Kooij, J.J.S. Adult ADHD: Diagnostic Assessment and Treatment, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Sobanski, E. Psychiatric Comorbidity in Adults with Attention-Deficit/Hyperactivity Disorder (ADHD). Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, i26–i31. [Google Scholar] [CrossRef]
- Perroud, N.; Cordera, P.; Zimmermann, J.; Michalopoulos, G.; Bancila, V.; Prada, P.; Dayer, A.; Aubry, J.M. Comorbidity between Attention Deficit Hyperactivity Disorder (ADHD) and Bipolar Disorder in a Specialized Mood Disorders Outpatient Clinic. J. Affect. Disord. 2014, 168, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Nierenberg, A.A.; Miyahara, S.; Spencer, T.; Wisniewski, S.R.; Otto, M.W.; Simon, N.; Pollack, M.H.; Ostacher, M.J.; Yan, L.; Siegel, R.; et al. Clinical and Diagnostic Implications of Lifetime Attention-Deficit/Hyperactivity Disorder Comorbidity in Adults with Bipolar Disorder: Data from the First 1000 STEP-BD Participants. Biol. Psychiatry 2005, 57, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Wingo, A.P.; Ghaemi, S.N. A Systematic Review of Rates and Diagnostic Validity of Comorbid Adult Attention-Deficit/Hyperactivity Disorder and Bipolar Disorder. J. Clin. Psychiatry 2007, 68, 1776–1784. [Google Scholar] [CrossRef]
- Jacob, C.P.; Romanos, J.; Dempfle, A.; Heine, M.; Windemuth-Kieselbach, C.; Kruse, A.; Reif, A.; Walitza, S.; Romanos, M.; Strobel, A.; et al. Co-Morbidity of Adult Attention-Deficit/Hyperactivity Disorder with Focus on Personality Traits and Related Disorders in a Tertiary Referral Center. Eur. Arch. Psychiatry Clin. Neurosci. 2007, 257, 309–317. [Google Scholar] [CrossRef]
- Kessler, R.; Adler, L.; Barkley, R.; Biederman, J.; Conners, K.; Demler, O.; Faraone, S.V.; Greenhill, L.L.; Howes, M.J.; Secnik, K.; et al. The Prevalence and Correlates of Adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am. Psychiatr. Assoc. 2006, 163, 716–723. [Google Scholar] [CrossRef]
- Biederman, J.; Ball, S.W.; Monuteaux, M.C.; Mick, E.; Spencer, T.J.; McCreary, M.; Cote, M.; Faraone, S.V. New Insights into the Comorbidity between ADHD and Major Depression in Adolescent and Young Adult Females. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 426–434. [Google Scholar] [CrossRef]
- Giupponi, G.; Giordano, G.; Maniscalco, I.; Erbuto, D.; Berardelli, I.; Conca, A.; Lester, D.; Girardi, P.; Pompili, M. Suicide Risk in Attention-Deficit/Hyperactivity Disorder. Psychiatr. Danub. 2018, 30, 2–10. [Google Scholar] [CrossRef]
- Capusan, A.J.; Kuja-Halkola, R.; Bendtsen, P.; Viding, E.; McCrory, E.; Marteinsdottir, I.; Larsson, H. Childhood Maltreatment and Attention Deficit Hyperactivity Disorder Symptoms in Adults: A Large Twin Study. Psychol. Med. 2016, 46, 2637–2646. [Google Scholar] [CrossRef]
- Gjervan, B.; Torgersen, T.; Nordahl, H.M.; Rasmussen, K. Functional Impairment and Occupational Outcome in Adults with ADHD. J. Atten. Disord. 2012, 16, 544–552. [Google Scholar] [CrossRef]
- Estévez, N.; Dey, M.; Eich-Höchli, D.; Foster, S.; Gmel, G.; Mohler-Kuo, M. Adult Attention-Deficit/Hyperactivity Disorder and Its Association with Substance Use and Substance Use Disorders in Young Men. Epidemiol. Psychiatr. Sci. 2016, 25, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Notzon, D.P.; Pavlicova, M.; Glass, A.; Mariani, J.J.; Mahony, A.L.; Brooks, D.J.; Levin, F.R. ADHD Is Highly Prevalent in Patients Seeking Treatment for Cannabis Use Disorders. J. Atten. Disord. 2020, 24, 1487–1492. [Google Scholar] [CrossRef]
- Mariani, J.J.; Khantzian, E.J.; Levin, F.R. The Self-Medication Hypothesis and Psychostimulant Treatment of Cocaine Dependence: An Update. Am. J. Addict. 2014, 23, 189–193. [Google Scholar] [CrossRef]
- Solanto, M.V.; Marks, D.J.; Wasserstein, J.; Mitchell, K.; Abikoff, H.; Alvir, J.M.J.; Kofman, M.D. Efficacy of Meta-Cognitive Therapy for Adult ADHD. Am. J. Psychiatry 2010, 167, 958–968. [Google Scholar] [CrossRef] [PubMed]
- Lopez, P.L.; Torrente, F.M.; Ciapponi, A.; Lischinsky, A.G.; Cetkovich-Bakmas, M.; Rojas, J.I.; Romano, M.; Manes, F.F. Cognitive-Behavioural Interventions for Attention Deficit Hyperactivity Disorder (ADHD) in Adults. Cochrane Database Syst. Rev. 2018, 2018, CD010840. [Google Scholar] [CrossRef]
- Safren, S.A.; Sprich, S.; Mimiaga, M.J.; Surman, C.; Knouse, L.; Groves, M.; Otto, M.W. Cognitive Behavioral Therapy vs Relaxation with Educational Support for Medication-Treated Adults with ADHD and Persistent Symptoms: A Randomized Controlled Trial. JAMA 2010, 304, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Bonti, E.; Giannoglou, S.; Georgitsi, M.; Sofologi, M.; Porfyri, G.N.; Mousioni, A.; Konsta, A.; Tatsiopoulou, P.; Kamari, A.; Vavetsi, S.; et al. Clinical Profiles and Socio-Demographic Characteristics of Adults with Specific Learning Disorder in Northern Greece. Brain Sci. 2021, 11, 602. [Google Scholar] [CrossRef]
- Gerber, P.J. The Impact of Learning Disabilities on Adulthood: A Review of the Evidenced-Based Literature for Research and Practice in Adult Education. J. Learn. Disabil. 2012, 45, 31–46. [Google Scholar] [CrossRef]
- Seo, Y.; Abbott, R.D.; Hawkins, J.D. Outcome Status of Students with Learning Disabilities at Ages 21 and 24. J. Learn. Disabil. 2008, 41, 300–314. [Google Scholar] [CrossRef]
- Geary, D.C. Consequences, Characteristics, and Causes of Mathematical Learning Disabilities and Persistent Low Achievement in Mathematics. J. Dev. Behav. Pediatr. 2011, 32, 250–263. [Google Scholar] [CrossRef] [PubMed]
- Sharfi, K.; Rosenblum, S. Executive Functions, Time Organization and Quality of Life among Adults with Learning Disabilities. PLoS ONE 2016, 11, e0166939. [Google Scholar] [CrossRef] [PubMed]
- Sharfi, K.; Rosenblum, S. Activity and Participation Characteristics of Adults with Learning Disabilities—A Systematic Review. PLoS ONE 2014, 9, e106657. [Google Scholar] [CrossRef] [PubMed]
- Hendren, R.L.; Haft, S.L.; Black, J.M.; White, N.C.; Hoeft, F. Recognizing Psychiatric Comorbidity with Reading Disorders. Front. Psychiatry 2018, 9, 101. [Google Scholar] [CrossRef] [PubMed]
- Alexander, R.; Cooray, S. Diagnosis of Personality Disorders in Learning Disability. Br. J. Psychiatry 2003, 182, 28–31. [Google Scholar] [CrossRef]
- McKenzie, K.; Milton, M.; Smith, G.; Ouellette-Kuntz, H. Systematic Review of the Prevalence and Incidence of Intellectual Disabilities: Current Trends and Issues. Curr. Dev. Disord. Rep. 2016, 3, 104–115. [Google Scholar] [CrossRef]
- Sharma, N.; O’Hare, K.; Antonelli, R.C.; Sawicki, G.S. Transition Care: Future Directions in Education, Health Policy, and Outcomes Research. Acad. Pediatr. 2014, 14, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Frueh, J.S.; Press, D.Z.; Sanders, J.S. Diagnosis and Workup of Intellectual Disability in Adults. Neurol. Clin. Pract. 2021, 11, 534–540. [Google Scholar] [CrossRef]
- Bakken, T.L.; Sageng, H. Mental Health Nursing of Adults With Intellectual Disabilities and Mental Illness: A Review of Empirical Studies 1994-2013. Arch. Psychiatr. Nurs. 2016, 30, 286–291. [Google Scholar] [CrossRef]
- Kendall, K.; Owen, M.J. Intellectual Disability and Psychiatric Comorbidity: Challenges and Clinical Issues. Psychiatr. Times 2015, 32, 60–63. [Google Scholar]
- Ferrell, R.B.; Wolinsky, E.J.; Kauffman, C.I.; Flashman, L.A.; McAllister, T.W. Neuropsychiatric Syndromes in Adults with Intellectual Disability: Issues in Assessment and Treatment. Curr. Psychiatry Rep. 2004, 6, 380–390. [Google Scholar] [CrossRef]
- Antonacci, D.J.; Attiah, N. Diagnosis and Treatment of Mood Disorders in Adults with Developmental Disabilities. Psychiatr. Q. 2008, 79, 171–192. [Google Scholar] [CrossRef]
- Simms, M.D. Language Disorders in Children: Classification and Clinical Syndromes. Pediatr. Clin. North Am. 2007, 54, 437–467. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, M.L.; Mody, M.; Klykylo, W.M.; McDougle, C.J.; Guenther, F.H. Neurodevelopmental Disorders: Communication Disorders. In Psychiatry, 4th ed.; Tasman, A., Kay, J., Lieberman, J.A., First, M.B., Riba, M.B., Eds.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015; pp. 706–721. [Google Scholar]
- Cantwell, D.P.; Baker, L. Psychiatric and Developmental Disorders in Children with Communication Disorder; American Psychiatric Press: Washington, DC, USA, 1991; Volume 43, pp. 289–290. [Google Scholar] [CrossRef]
- Beitchman, J. Speech and Language Impairment and Psychiatric Risk. Psychiatr. Clin. N. Am. 1985, 8, 721–735. [Google Scholar] [CrossRef]
- Zwicker, J.G.; Missiuna, C.; Harris, S.R.; Boyd, L.A. Developmental Coordination Disorder: A Review and Update. Eur. J. Paediatr. Neurol. 2012, 16, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Gillberg, C. Deficits in Attention, Motor Control, and Perception: A Brief Review. Arch. Dis. Child. 2003, 88, 904–910. [Google Scholar] [CrossRef]
- Missiuna, C.; Gaines, R.; Mclean, J.; Delaat, D.; Egan, M.; Soucie, H. Description of Children Identified by Physicians as Having Developmental Coordination Disorder. Dev. Med. Child Neurol. 2008, 50, 839–844. [Google Scholar] [CrossRef]
- Kadesjö, B.; Gillberg, C. Developmental Coordination Disorder in Swedish 7-Year-Old Children. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 820–828. [Google Scholar] [CrossRef]
- Dewey, D.; Kaplan, B.J.; Crawford, S.G.; Wilson, B.N. Developmental Coordination Disorder: Associated Problems in Attention, Learning, and Psychosocial Adjustment. Hum. Mov. Sci. 2002, 21, 905–918. [Google Scholar] [CrossRef] [PubMed]
- Piek, J.P.; Dyck, M.J. Sensory-Motor Deficits in Children with Developmental Coordination Disorder, Attention Deficit Hyperactivity Disorder and Autistic Disorder. Hum. Mov. Sci. 2004, 23, 475–488. [Google Scholar] [CrossRef]
- Piek, J.P.; Dyck, M.J.; Nieman, A.; Anderson, M.; Hay, D.; Smith, L.M.; McCoy, M.; Hallmayer, J. The Relationship between Motor Coordination, Executive Functioning and Attention in School Aged Children. Arch. Clin. Neuropsychol. 2004, 19, 1063–1076. [Google Scholar] [CrossRef]
- Watemberg, N.; Waiserberg, N.; Zuk, L.; Lerman-Sagie, T. Developmental Coordination Disorder in Children with Attention-Deficit-Hyperactivity Disorder and Physical Therapy Intervention. Dev. Med. Child Neurol. 2007, 49, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.C.; Piek, J.P.; Hay, D. DCD and ADHD: A Genetic Study of Their Shared Aetiology. Hum. Mov. Sci. 2006, 25, 110–124. [Google Scholar] [CrossRef] [PubMed]
- Fliers, E.; Vermeulen, S.; Rijsdijk Mar, F.; Altink, I.; Buschgens, C.; Rommelse, N.; Faraone, S.; Sergeant, J.; Buitelaar, J.; Franke, B. ADHD and Poor Motor Performance from a Family Genetic Perspective. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 25–34. [Google Scholar] [CrossRef]
- Iversen, S.; Berg, K.; Ellertsen, B.; Tønnessen, F.E. Motor Coordination Difficulties in a Municipality Group and in a Clinical Sample of Poor Readers. Dyslexia 2005, 11, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Jongmans, M.J.; Smits-Engelsman, B.C.M.; Schoemaker, M.M. Consequences of Comorbidity of Developmental Coordination Disorders and Learning Disabilities for Severity and Pattern of Perceptual-Motor Dysfunction. J. Learn. Disabil. 2003, 36, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Alloway, T.P.; Archibald, L. Working Memory and Learning in Children with Developmental Coordination Disorder and Specific Language Impairment. J. Learn. Disabil. 2008, 41, 251–262. [Google Scholar] [CrossRef]
- Cheng, H.C.; Chen, H.Y.; Tsai, C.L.; Chen, Y.J.; Cherng, R.J. Comorbidity of Motor and Language Impairments in Preschool Children of Taiwan. Res. Dev. Disabil. 2009, 30, 1054–1061. [Google Scholar] [CrossRef]
- Cantell, M.H.; Smyth, M.M.; Ahonen, T.P. Two Distinct Pathways for Developmental Coordination Disorder: Persistence and Resolution. Hum. Mov. Sci. 2003, 22, 413–431. [Google Scholar] [CrossRef]
- Skinner, R.A.; Piek, J.P. Psychosocial Implications of Poor Motor Coordination in Children and Adolescents. Hum. Mov. Sci. 2001, 20, 73–94. [Google Scholar] [CrossRef]
- Missiuna, C.; Moll, S.; King, G.; Stewart, D.; Macdonald, K. Life Experiences of Young Adults Who Have Coordination Difficulties. Can. J. Occup. Ther. 2008, 75, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Piek, J.P.; Baynam, G.B.; Barrett, N.C. The Relationship between Fine and Gross Motor Ability, Self-Perceptions and Self-Worth in Children and Adolescents. Hum. Mov. Sci. 2006, 25, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Baird, G.; Sugden, D. A Pilot Study of Psychopathology in Developmental Coordination Disorder. Child. Care. Health Dev. 2006, 32, 741–750. [Google Scholar] [CrossRef]
- Missiuna, C.; Moll, S.; King, S.; King, G.; Law, M. A Trajectory of Troubles: Parents’ Impressions of the Impact of Developmental Coordination Disorder. Phys. Occup. Ther. Pediatr. 2007, 27, 81–101. [Google Scholar] [CrossRef] [PubMed]
- Cousins, M.; Smyth, M.M. Developmental Coordination Impairments in Adulthood. Hum. Mov. Sci. 2003, 22, 433–459. [Google Scholar] [CrossRef]
- Losse, A.; Henderson, S.E.; Elliman, D.; Hall, D.; Knight, E.; Jongmans, M. Clumsiness in Children-Do They Grow out Of It? A 10-Year Follow-Up Study. Dev. Med. Child Neurol. 1991, 33, 55–68. [Google Scholar] [CrossRef]
- Rasmussen, P.; Gillberg, C. Natural Outcome of ADHD with Developmental Coordination Disorder at Age 22 Years: A Controlled, Longitudinal, Community-Based Study. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1424–1431. [Google Scholar] [CrossRef]
- Piek, J.P.; Rigoli, D.; Pearsall-Jones, J.G.; Martin, N.C.; Hay, D.A.; Bennett, K.S.; Levy, F. Depressive Symptomatology in Child and Adolescent Twins with Attention-Deficit Hyperactivity Disorder and/or Developmental Coordination Disorder. Twin Res. Hum. Genet. 2007, 10, 587–596. [Google Scholar] [CrossRef]
- Cairney, J.; Hay, J.A.; Faught, B.E.; Hawes, R. Developmental Coordination Disorder and Overweight and Obesity in Children Aged 9–14y. Int. J. Obes. 2005, 29, 369–372. [Google Scholar] [CrossRef]
- Faught, B.E.; Hay, J.A.; Cairney, J.; Flouris, A. Increased Risk for Coronary Vascular Disease in Children with Developmental Coordination Disorder. J. Adolesc. Health 2005, 37, 376–380. [Google Scholar] [CrossRef]
- Cavanna, A.E.; Servo, S.; Monaco, F.; Robertson, M.M. The Behavioral Spectrum of Gilles de La Tourette Syndrome. J. Neuropsychiatry Clin. Neurosci. 2009, 21, 13–23. [Google Scholar] [CrossRef]
- Gill, C.E.; Kompoliti, K. Clinical Features of Tourette Syndrome. J. Child Neurol. 2020, 35, 166–174. [Google Scholar] [CrossRef]
- Scahill, L.; Specht, M.; Page, C. The Prevalence of Tic Disorders and Clinical Characteristics in Children. J. Obs. Compuls. Relat. Disord. 2014, 3, 394–400. [Google Scholar] [CrossRef]
- Knight, T.; Steeves, T.; Day, L.; Lowerison, M.; Jette, N.; Pringsheim, T. Prevalence of Tic Disorders: A Systematic Review and Meta-Analysis. Pediatr. Neurol. 2012, 47, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.M.; Eapen, V.; Cavanna, A.E. The International Prevalence, Epidemiology, and Clinical Phenomenology of Tourette Syndrome: A Cross-Cultural Perspective. J. Psychosom. Res. 2009, 67, 475–483. [Google Scholar] [CrossRef]
- Kompoliti, K. Sources of Disability in Tourette Syndrome: Children vs. Adults. Tremor Other Hyperkinetic Mov. 2015, 2016, 318. [Google Scholar] [CrossRef]
- Freeman, R.D.; Fast, D.K.; Burd, L.; Kerbeshian, J.; Robertson, M.M.; Sandor, P. An International Perspective on Tourette Syndrome: Selected Findings from 3500 Individuals in 22 Countries. Dev. Med. Child Neurol. 2000, 42, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Bloch, M.H.; Leckman, J.F. Clinical Course of Tourette Syndrome. J. Psychosom. Res. 2009, 67, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Burd, L.; Kerbeshian, J.; Klug, M.G.; Burd, L.; Avery, K.; Benz, B.; Barth, A. Long-Term Follow-up of an Epidemiologically Defined Cohort of Patients with Tourette Syndrome. J. Child Neurol. 2001, 16, 431–437. [Google Scholar] [CrossRef]
- Groth, C.; Mol Debes, N.; Rask, C.U.; Lange, T.; Skov, L. Course of Tourette Syndrome and Comorbidities in a Large Prospective Clinical Study. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 304–312. [Google Scholar] [CrossRef]
- Ganos, C.; Münchau, A.; Bhatia, K.P. The Semiology of Tics, Tourette’s, and Their Associations. Mov. Disord. Clin. Pract. 2014, 1, 145–153. [Google Scholar] [CrossRef]
- Khan, K.; Hollis, C.; Murphy, T.; Hall, C.L. Digital and Remote Behavioral Therapies for Treating Tic Disorders: Recent Advances and next Steps. Front. Psychiatry 2022, 13, 1533. [Google Scholar] [CrossRef] [PubMed]
- Groth, C.; Skov, L.; Lange, T.; Debes, N.M. Predictors of the Clinical Course of Tourette Syndrome: A Longitudinal Study. J. Child Neurol. 2019, 34, 913–921. [Google Scholar] [CrossRef] [PubMed]
- Bloch, M.H.; Peterson, B.S.; Scahill, L.; Otka, J.; Katsovich, L.; Zhang, H.; Leckman, J.F. Adulthood Outcome of Tic and Obsessive-Compulsive Symptom Severity in Children with Tourette Syndrome. Arch. Pediatr. Adolesc. Med. 2006, 160, 65–69. [Google Scholar] [CrossRef]
- Bloch, M.H.; Sukhodolsky, D.G.; Dombrowski, P.A.; Panza, K.E.; Craiglow, B.G.; Landeros-Weisenberger, A.; Leckman, J.F.; Peterson, B.S.; Schultz, R.T. Poor Fine-Motor and Visuospatial Skills Predict Persistence of Pediatric-Onset Obsessive-Compulsive Disorder into Adulthood. J. Child. Psychol. Psychiatry 2011, 52, 974. [Google Scholar] [CrossRef]
- Mittal, S.O. Tics and Tourette’s Syndrome. Drugs Context 2020, 9, 115–136. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.M. A Personal 35 Year Perspective on Gilles de La Tourette Syndrome: Prevalence, Phenomenology, Comorbidities, and Coexistent Psychopathologies. Lancet Psychiatry 2015, 2, 68–87. [Google Scholar] [CrossRef]
- Hirschtritt, M.E.; Lee, P.C.; Pauls, D.L.; Dion, Y.; Grados, M.A.; Illmann, C.; King, R.A.; Sandor, P.; McMahon, W.M.; Lyon, G.J.; et al. Lifetime Prevalence, Age of Risk, and Etiology of Comorbid Psychiatric Disorders in Tourette Syndrome. JAMA Psychiatry 2015, 72, 325–333. [Google Scholar] [CrossRef]
- Rizzo, R.; Gulisano, M.; Calì, P.V.; Curatolo, P. Long Term Clinical Course of Tourette Syndrome. Brain Dev. 2012, 34, 667–673. [Google Scholar] [CrossRef]
- Debes, N.M. Co-Morbid Disorders in Tourette Syndrome. Behav. Neurol. 2013, 27, 7–14. [Google Scholar] [CrossRef]
- Robertson, M.M. Attention Deficit Hyperactivity Disorder, Tics and Tourette’s Syndrome: The Relationship and Treatment Implications. A Commentary. Eur. Child Adolesc. Psychiatry 2006, 15, 1–11. [Google Scholar] [CrossRef]
- Ganos, C.; Martino, D. Tics and Tourette Syndrome. Neurol Clin. 2015, 33, 115–136. [Google Scholar] [CrossRef]
- Roessner, V.; Becker, A.; Banaschewski, T.; Rothenberger, A. Psychopathological Profile in Children with Chronic Tic Disorder and Co-Existing ADHD: Additive Effects. J. Abnorm. Child Psychol. 2007, 35, 79–85. [Google Scholar] [CrossRef]
- Wanderer, S.; Roessner, V.; Freeman, R.; Bock, N.; Rothenberger, A.; Becker, A. Relationship of Obsessive-Compulsive Disorder to Age-Related Comorbidity in Children and Adolescents with Tourette Syndrome. J. Dev. Behav. Pediatr. 2012, 33, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Street, C.; Wheeler, N.; Singh, S.P. Transition to Adult Services for Young People with Mental Health Needs: A Systematic Review. Clin. Child Psychol. Psychiatry 2015, 20, 436–457. [Google Scholar] [CrossRef] [PubMed]
- Embrett, M.G.; Randall, G.E.; Longo, C.J.; Nguyen, T.; Mulvale, G. Effectiveness of Health System Services and Programs for Youth to Adult Transitions in Mental Health Care: A Systematic Review of Academic Literature. Adm. Policy Ment. Health Ment. Health Serv. Res. 2016, 43, 259–269. [Google Scholar] [CrossRef]
- Hofstra, M.B.; Van Der Ende, J.; Verhulst, F.C. Continuity and Change of Psychopathology from Childhood into Adulthood: A 14-Year Follow-up Study. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Kerr, H.; Price, J.; O’Halloran, P. A Cross-Sectional Survey of Services for Young Adults with Life-Limiting Conditions Making the Transition from Children’s to Adult Services in Ireland. Ir. J. Med. Sci. 2020, 189, 33–42. [Google Scholar] [CrossRef] [PubMed]
- McGorry, P.D.; Purcell, R.; Hickie, I.B.; Jorm, A.F. Investing in Youth Mental Health Is a Best Buy. Med. J. Aust. 2007, 187, 5–7. [Google Scholar] [CrossRef]
- Singh, S.P. Transition of Care from Child to Adult Mental Health Services: The Great Divide. Curr. Opin. Psychiatry 2009, 22, 386–390. [Google Scholar] [CrossRef]
- Paul, M.; Ford, T.; Kramer, T.; Islam, Z.; Harley, K.; Singh, S.P. Transfers and Transitions between Child and Adult Mental Health Services. Br. J. Psychiatry 2013, 202, s36–s40. [Google Scholar] [CrossRef]
- Coleman, E.A.; Berenson, R.A. Lost in Transition: Challenges and Opportunities for Improving the Quality of Transitional Care. Ann. Intern. Med. 2004, 141, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Dimitropoulos, G.; Tran, A.F.; Agarwal, P.; Sheffield, B.; Woodside, B. Challenges in Making the Transition Between Pediatric and Adult Eating Disorder Programs: A Qualitative Study From the Perspective of Service Providers. Eat. Disord. 2013, 21, 1–15. [Google Scholar] [CrossRef]
- Kim, H.S.; Munson, M.R.; McKay, M.M. Engagement in Mental Health Treatment among Adolescents and Young Adults: A Systematic Review. Child Adolesc. Soc. Work J. 2012, 29, 241–266. [Google Scholar] [CrossRef]
- Harpaz-Rotem, I.; Leslie, D.; Rosenheck, R.A. Treatment Retention among Children Entering a New Episode of Mental Health Care. Psychiatr. Serv. 2004, 55, 1022–1028. [Google Scholar] [CrossRef]
- Davis, M.; Koroloff, N.; Sabella, K.; Sarkis, M. Crossing the Age Divide: Cross-Age Collaboration Between Programs Serving Transition-Age Youth. J. Behav. Health Serv. Res. 2018, 45, 356–369. [Google Scholar] [CrossRef] [PubMed]
- Beresford, B.; Stuttard, L. Young Adults as Users of Adult Healthcare: Experiences of Young Adults with Complex or Life-Limiting Conditions. Clin. Med. J. R. Coll. Physicians Lond. 2014, 14, 404–408. [Google Scholar] [CrossRef]
- Kerr, H.; Widger, K.; Cullen-Dean, G.; Price, J.; O’Halloran, P. Transition from Children’s to Adult Services for Adolescents/Young Adults with Life-Limiting Conditions: Developing Realist Programme Theory through an International Comparison. BMC Palliat. Care 2020, 19, 115. [Google Scholar] [CrossRef]
- Singh, S.P.; Paul, M.; Ford, T.; Kramer, T.; Weaver, T.; McLaren, S.; Hovish, K.; Islam, Z.; Belling, R.; White, S. Process, Outcome and Experience of Transition from Child to Adult Mental Healthcare: Multiperspective Study. Br. J. Psychiatry 2010, 197, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Mcnamara, N.; Mcnicholas, F.; Ford, T.; Paul, M.; Gavin, B.; Coyne, I.; Cullen, W.; O’Connor, K.; Ramperti, N.; Dooley, B.; et al. Transition from Child and Adolescent to Adult Mental Health Services in the Republic of Ireland: An Investigation of Process and Operational Practice. Early Interv. Psychiatry 2014, 8, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Ogundele, M.; Omenaka, I. An Audit of Transitional Care for Adolescents with ADHD in a North West England District. Arch. Dis. Child. 2012, 97, A129. [Google Scholar] [CrossRef]
- Swift, K.D.; Sayal, K.; Hollis, C. ADHD and Transitions to Adult Mental Health Services: A Scoping Review. Child. Care. Health Dev. 2014, 40, 775–786. [Google Scholar] [CrossRef]
- McGorry, P.D.; Goldstone, S.D.; Parker, A.G.; Rickwood, D.J.; Hickie, I.B. Cultures for Mental Health Care of Young People: An Australian Blueprint for Reform. Lancet Psychiatry 2014, 1, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.P.; Tuomainen, H. Transition from Child to Adult Mental Health Services: Needs, Barriers, Experiences and New Models of Care. World Psychiatry 2015, 14, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Hendrickx, G.; De Roeck, V.; Maras, A.; Dieleman, G.; Gerritsen, S.; Purper-Ouakil, D.; Russet, F.; Schepker, R.; Signorini, G.; Singh, S.P.; et al. Challenges during the Transition from Child and Adolescent Mental Health Services to Adult Mental Health Services. BJPsych Bull. 2020, 44, 163–168. [Google Scholar] [CrossRef]
- Davis, M.; Sondheimer, D.L. State Child Mental Health Efforts to Support Youth in Transition to Adulthood. J. Behav. Health Serv. Res. 2005, 32, 27–42. [Google Scholar] [CrossRef]
- Hovish, K.; Weaver, T.; Islam, Z.; Paul, M.; Singh, S.P. Transition Experiences of Mental Health Service Users, Parents, and Professionals in the United Kingdom: A Qualitative Study. Psychiatr. Rehabil. J. 2012, 35, 251–257. [Google Scholar] [CrossRef]
- Smith, L.; Newton, R. Systematic Review of Case Management. Aust. N. Z. J. Psychiatry 2007, 41, 2–9. [Google Scholar] [CrossRef]
- Cameron, A.; Lart, R. Revisiting Joint Working. J. Integr. Care 2012, 20, 89–93. [Google Scholar] [CrossRef]
- Horvitz-Lennon, M.; Kilbourne, A.M.; Pincus, H.A. From Silos to Bridges: Meeting the General Health Care Needs of Adults with Severe Mental Illnesses. Health Aff. 2006, 25, 659–669. [Google Scholar] [CrossRef]
- Chugani, C.D.; Goldstein, T.R.; Salk, R.H.; Poling, K.; Sakolksy, D.; Brent, D. Group Intervention for Young Adults with Mood and Anxiety Disorders Transitioning to College. J. Psychiatr. Pract. 2020, 26, 120–125. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Child & Adolescent Psychiatry. 2023. Available online: https://www.aacap.org (accessed on 11 March 2023).
- NSW Health. NSW Health. Australian Government. 2023. Available online: https://www.health.nsw.gov.au (accessed on 11 March 2023).
- McLaren, S.; Belling, R.; Paul, M.; Ford, T.; Kramer, T.; Weaver, T.; Hovish, K.; Islam, Z.; White, S.; Singh, S.P. “Talking a Different Language”: An Exploration of the Influence of Organizational Cultures and Working Practices on Transition from Child to Adult Mental Health Services. BMC Health Serv. Res. 2013, 13, 254. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| NDD | Core Features | Prevalence Rates | Age at Onset | Evolution |
|---|---|---|---|---|
| Autism spectrum disorder | Qualitative impairment in social communication skills, with stereotyped and restrictive patterns of behavior. | Around 1.5% | Early developmental period | Lifelong; adults with autism spectrum disorder frequently have to face several challenges with respect to co-occurring medical and psychiatric conditions, education, work, and living situations. |
| Attention-deficit/hyperactivity disorder | Inattention, hyperactivity, and impulsivity. | 5% | Before 12 y.o. | Some symptoms may persist into adulthood, although the clinical presentations may change with time and concomitant psychiatric issues may emerge. |
| Specific learning disorders | Significant deficits in basic writing, reading, or mathematical skills. | 5% | Within the first years of elementary school | May improve with early, adequate interventions or may persist into adulthood. |
| Intellectual disability | Limited cognitive and adaptive functioning. | 1–3% | Within the first 3 years of life | Lifelong; frequently associates with psychiatric comorbidities in adult age. |
| Communication disorders |
|
| Early developmental period |
|
| Developmental coordination disorder | Difficulties with gross and/or fine motor skills, interfering with daily life activities | 5–8% in children ages 5–11 y.o. | Early developmental period | Symptoms may improve; however, coordination difficulties may persist throughout adolescence and adulthood, along with issues in learning new tasks, which may affect professional performance. |
| Tic disorders | Involuntary, repetitive, sudden twitches, movements, or vocalizations (tics) | 1% | Between 2 and 15 y.o. (average around 6 y.o.) | Tic severity improves after adolescence for most patients; tics may persist into adulthood in a relevant minority of subjects who may report low self-esteem, limited peer relationships, high anxiety rates, and poor school or work performance. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antolini, G.; Colizzi, M. Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood. Healthcare 2023, 11, 1015. https://doi.org/10.3390/healthcare11071015
Antolini G, Colizzi M. Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood. Healthcare. 2023; 11(7):1015. https://doi.org/10.3390/healthcare11071015
Chicago/Turabian StyleAntolini, Giulia, and Marco Colizzi. 2023. "Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood" Healthcare 11, no. 7: 1015. https://doi.org/10.3390/healthcare11071015
APA StyleAntolini, G., & Colizzi, M. (2023). Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood. Healthcare, 11(7), 1015. https://doi.org/10.3390/healthcare11071015