
Breathing Control Exercises Delivered in a Group Setting for Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Control Group
2.4. Intervention Group
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
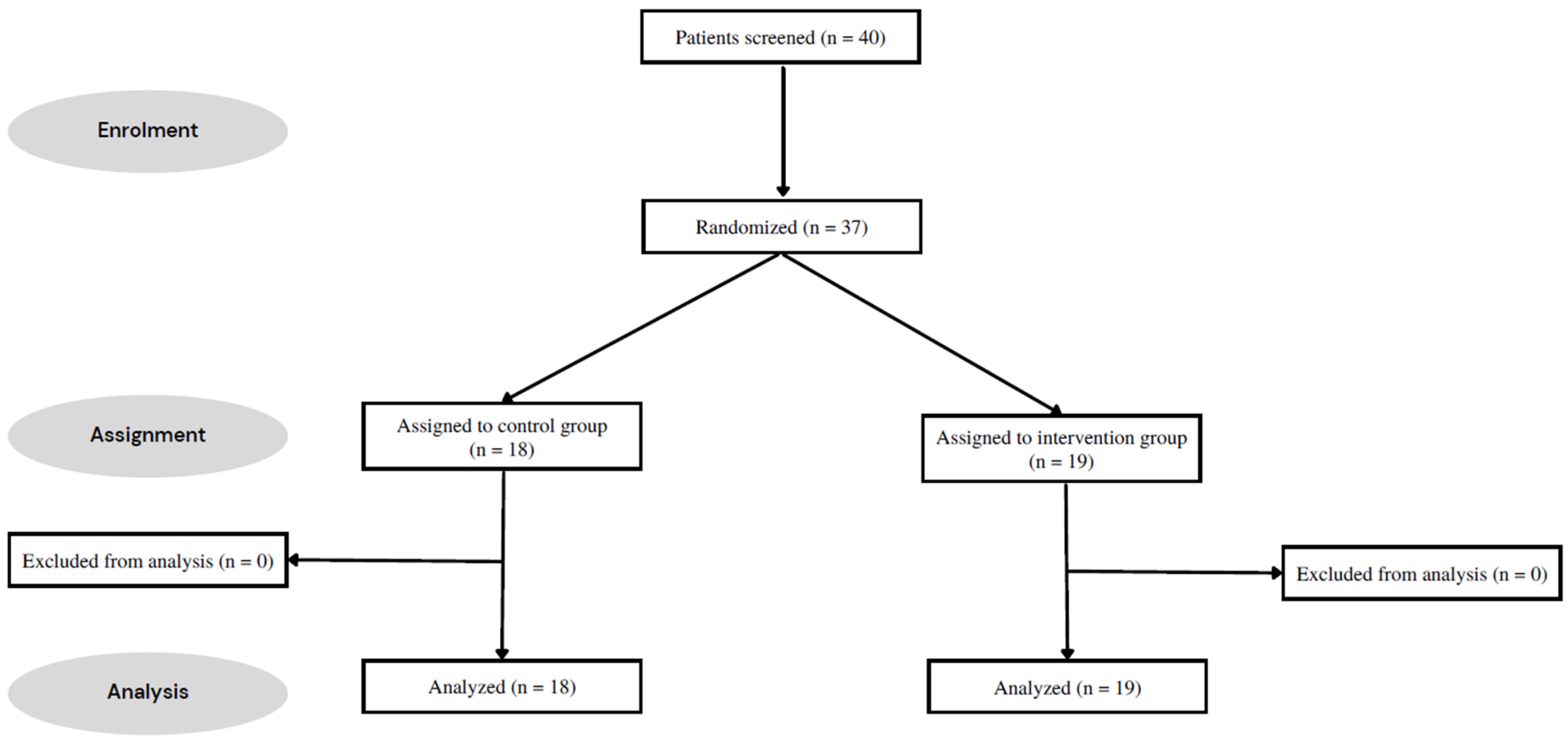
3.1. Participants
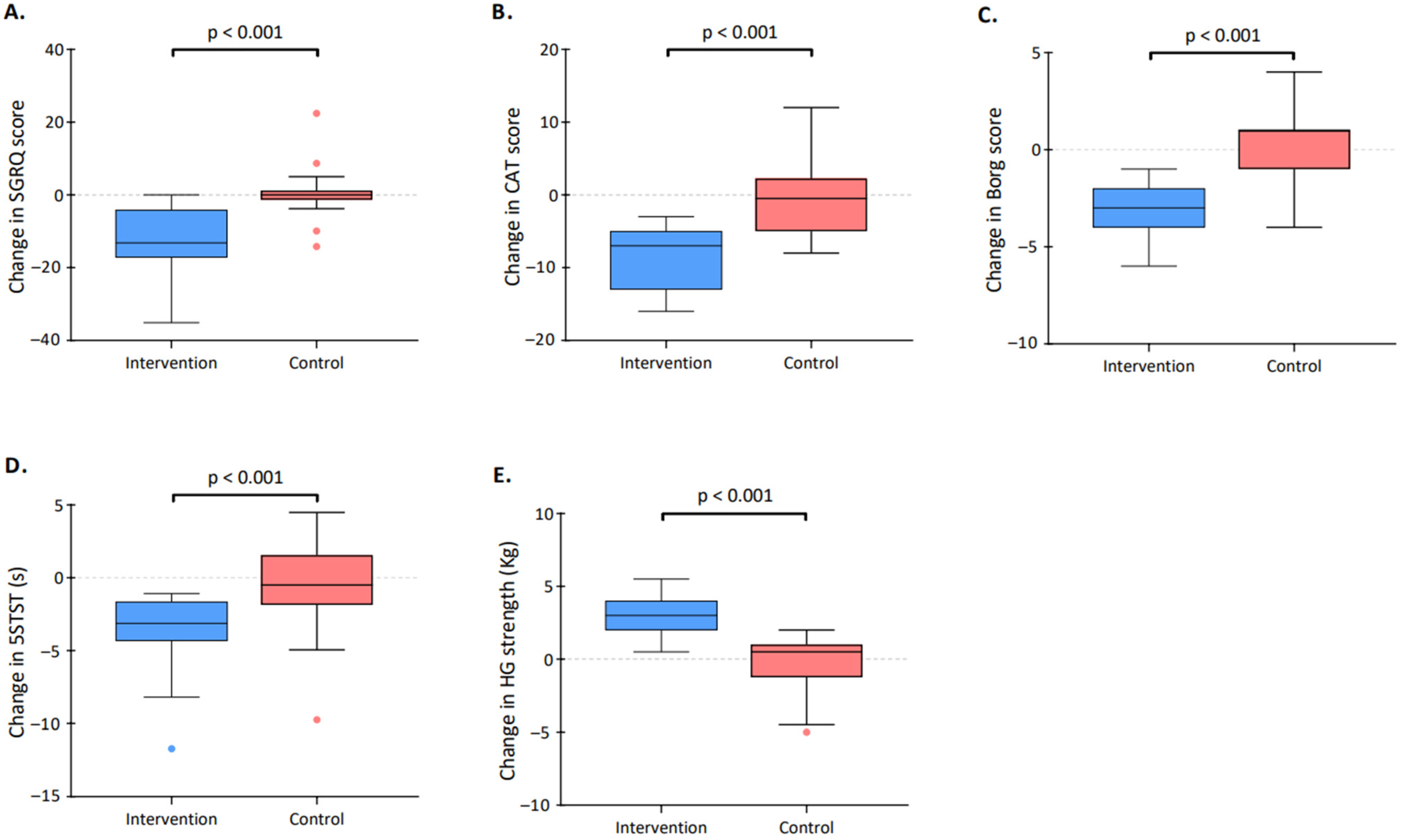
3.2. Primary Outcome
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kessler, R.; Partridge, M.R.; Miravitlles, M.; Cazzola, M.; Vogelmeier, C.; Leynaud, D.; Ostinelli, J. Symptom variability in patients with severe COPD: A pan-European cross-sectional study. Eur. Respir. J. 2011, 37, 264–272. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E.; Milne, K.M.; James, M.D.; de Torres, J.P.; Neder, J.A. Dyspnea in COPD: New Mechanistic Insights and Management Implications. Adv. Ther. 2020, 37, 41–60. [Google Scholar] [CrossRef] [PubMed]
- Wingårdh, A.S.L.; Göransson, C.; Larsson, S.; Slinde, F.; Vanfleteren, L. Effectiveness of Energy Conservation Techniques in Patients with COPD. Respiration 2020, 99, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Cavalheri, V.; Straker, L.; Gucciardi, D.F.; Gardiner, P.A.; Hill, K. Changing physical activity and sedentary behaviour in people with COPD. Respirology 2016, 21, 419–426. [Google Scholar] [CrossRef]
- Schneider, L.P.; Furlanetto, K.C.; Rodrigues, A.; Lopes, J.R.; Hernandes, N.A.; Pitta, F. Sedentary Behaviour and Physical Inactivity in Patients with Chronic 0Obstructive Pulmonary Disease: Two Sides of the Same Coin? COPD 2018, 15, 432–438. [Google Scholar] [CrossRef]
- Putcha, N.; Puhan, M.A.; Hansel, N.N.; Drummond, M.B.; Boyd, C.M. Impact of co-morbidities on self-rated health in self-reported COPD: An analysis of NHANES 2001–2008. COPD 2013, 10, 324–332. [Google Scholar] [CrossRef]
- Roche, N. Activity limitation: A major consequence of dyspnoea in COPD. Eur. Respir. Rev. 2009, 18, 54–57. [Google Scholar] [CrossRef]
- McSweeny, A.J.; Grant, I.; Heaton, R.K.; Adams, K.M.; Timms, R.M. Life quality of patients with chronic obstructive pulmonary disease. Arch. Intern. Med. 1982, 142, 473–478. [Google Scholar] [CrossRef]
- Lacasse, Y.; Cates, C.J.; McCarthy, B.; Welsh, E.J. This Cochrane Review is closed: Deciding what constitutes enough research and where next for pulmonary rehabilitation in COPD. Cochrane Database Syst. Rev. 2015, 11, Ed000107. [Google Scholar]
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 2, Cd003793. [Google Scholar] [CrossRef]
- Martinsen, U.; Bentzen, H.; Holter, M.K.; Nilsen, T.; Skullerud, H.; Mowinckel, P.; Kjeken, I. The effect of occupational therapy in patients with chronic obstructive pulmonary disease: A randomized controlled trial. Scand. J. Occup. Ther. 2017, 24, 89–97. [Google Scholar] [CrossRef]
- Bendstrup, K.E.; Ingemann Jensen, J.; Holm, S.; Bengtsson, B. Out-patient rehabilitation improves activities of daily living, quality of life and exercise tolerance in chronic obstructive pulmonary disease. Eur. Respir. J. 1997, 10, 2801–2806. [Google Scholar] [CrossRef] [PubMed]
- Finch, L.; Frankel, D.; Gallant, B.; Landa, C.; Snyder, N.; Wilson, R.; Packham, T.; Brooks, D.; Oliveira, A. Occupational therapy in pulmonary rehabilitation programs: A scoping review. Respir. Med. 2022, 199, 106881. [Google Scholar] [CrossRef]
- Vaes, A.W.; Delbressine, J.M.L.; Mesquita, R.; Goertz, Y.M.J.; Janssen, D.J.A.; Nakken, N.; Franssen, F.M.E.; Vanfleteren, L.; Wouters, E.F.M.; Spruit, M.A. Impact of pulmonary rehabilitation on activities of daily living in patients with chronic obstructive pulmonary disease. J. Appl. Physiol. 2019, 126, 607–615. [Google Scholar] [CrossRef]
- Graupensperger, S.; Gottschall, J.S.; Benson, A.J.; Eys, M.; Hastings, B.; Evans, M.B. Perceptions of groupness during fitness classes positively predict recalled perceptions of exertion, enjoyment, and affective valence: An intensive longitudinal investigation. Sport Exerc. Perform. Psychol. 2019, 8, 290–304. [Google Scholar] [CrossRef]
- Yorks, D.M.; Frothingham, C.A.; Schuenke, M.D. Effects of Group Fitness Classes on Stress and Quality of Life of Medical Students. J. Am. Osteopath Assoc. 2017, 117, e17–e25. [Google Scholar] [CrossRef] [PubMed]
- Velloso, M.; Jardim, J.R. Functionality of patients with chronic obstructive pulmonary disease: Energy conservation techniques. J. Bras. Pneumol. 2006, 32, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Palomba, B. Question 4-7. Activities of daily living in patients with chronic obstructive pulmonary disease. Rev. Mal. Respir. 2005, 22, 7s86. [Google Scholar] [PubMed]
- Yun, R.; Bai, Y.; Lu, Y.; Wu, X.; Lee, S.D. How Breathing Exercises Influence on Respiratory Muscles and Quality of Life among Patients with COPD? A Systematic Review and Meta-Analysis. Can. Respir. J. 2021, 2021, 1904231. [Google Scholar] [CrossRef]
- Bouchet, C.; Guillemin, F.; Hoang Thi, T.H.; Cornette, A.; Briançon, S. Validation of the St George’s questionnaire for measuring the quality of life in patients with chronic obstructive pulmonary disease. Rev. Mal. Respir. 1996, 13, 43–46. [Google Scholar]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M. The St George’s Respiratory Questionnaire. Respir. Med. 1991, 85, 25–31, Discussion 33–37. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.E.; Kon, S.S.; Canavan, J.L.; Patel, M.S.; Clark, A.L.; Nolan, C.M.; Polkey, M.I.; Man, W.D. The five-repetition sit-to-stand test as a functional outcome measure in COPD. Thorax 2013, 68, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- Borg, E.; Borg, G.; Larsson, K.; Letzter, M.; Sundblad, B.M. An index for breathlessness and leg fatigue. Scand. J. Med. Sci. Sports 2010, 20, 644–650. [Google Scholar] [CrossRef]
- Alma, H.; de Jong, C.; Jelusic, D.; Wittmann, M.; Schuler, M.; Flokstra-de Blok, B.; Kocks, J.; Schultz, K.; van der Molen, T. Health status instruments for patients with COPD in pulmonary rehabilitation: Defining a minimal clinically important difference. NPJ Prim. Care Respir. Med. 2016, 26, 16041. [Google Scholar] [CrossRef]
- Puhan, M.A.; Guyatt, G.H.; Goldstein, R.; Mador, J.; McKim, D.; Stahl, E.; Griffith, L.; Schünemann, H.J. Relative responsiveness of the Chronic Respiratory Questionnaire, St. Georges Respiratory Questionnaire and four other health-related quality of life instruments for patients with chronic lung disease. Respir. Med. 2007, 101, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Smid, D.E.; Franssen, F.M.; Houben-Wilke, S.; Vanfleteren, L.E.; Janssen, D.J.; Wouters, E.F.; Spruit, M.A. Responsiveness and MCID Estimates for, C.A.T.; CCQ, and HADS in Patients With COPD Undergoing Pulmonary Rehabilitation: A Prospective Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 53–58. [Google Scholar] [CrossRef]
- Maltais, F.; Decramer, M.; Casaburi, R.; Barreiro, E.; Burelle, Y.; Debigaré, R.; Dekhuijzen, P.N.; Franssen, F.; Gayan-Ramirez, G.; Gea, J.; et al. An official American Thoracic Society/European Respiratory Society statement: Update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2014, 189, e15–e62. [Google Scholar] [CrossRef]
- Ries, A.L. Minimally clinically important difference for the UCSD Shortness of Breath Questionnaire, Borg Scale, and Visual Analog Scale. COPD 2005, 2, 105–110. [Google Scholar] [CrossRef]
- Karagiannis, C.; Savva, C.; Korakakis, V.; Matheou, I.; Adamide, T.; Georgiou, A.; Xanthos, T. Test-Retest Reliability of Handgrip Strength in Patients with Chronic Obstructive Pulmonary Disease. COPD 2020, 17, 568–574. [Google Scholar] [CrossRef]
- Migliore, A. Management of dyspnea guidelines for practice for adults with chronic obstructive pulmonary disease. Occup Ther. Health Care 2004, 18, 1–20. [Google Scholar] [CrossRef]
- Bourbeau, J.; Nault, D.; Dang-Tan, T. Self-management and behaviour modification in COPD. Patient Educ. Couns. 2004, 52, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.; Lieschke, J.; Cruwys, T.; Cárdenas, D.; Platow, M.J.; Reynolds, K.J. Better together: How group-based physical activity protects against depression. Soc. Sci. Med. 2021, 286, 114337. [Google Scholar] [CrossRef] [PubMed]
- Estabrooks, P.A. Sustaining exercise participation through group cohesion. Exerc. Sport Sci. Rev. 2000, 28, 63–67. [Google Scholar] [PubMed]
- Madureira, M.M.; Bonfá, E.; Takayama, L.; Pereira, R.M. A 12-month randomized controlled trial of balance training in elderly women with osteoporosis: Improvement of quality of life. Maturitas 2010, 66, 206–211. [Google Scholar] [CrossRef]
- Langoni, C.D.S.; Resende, T.L.; Barcellos, A.B.; Cecchele, B.; da Rosa, J.N.; Knob, M.S.; Silva, T.D.N.; Diogo, T.S.; da Silva, I.G.; Schwanke, C.H.A. The effect of group exercises on balance, mobility, and depressive symptoms in older adults with mild cognitive impairment: A randomized controlled trial. Clin. Rehabil. 2019, 33, 439–449. [Google Scholar] [CrossRef]
- Jaitovich, A.; Barreiro, E. Skeletal Muscle Dysfunction in Chronic Obstructive Pulmonary Disease. What We Know and Can Do for Our Patients. Am. J. Respir. Crit. Care Med. 2018, 198, 175–186. [Google Scholar] [CrossRef]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Bjørnshave, B.; Korsgaard, J. Comparison of two different levels of physical training in patients with moderate to severe COPD. Lung 2005, 183, 101–108. [Google Scholar] [CrossRef]
- Holland, A.E.; Hill, C.J.; Jones, A.Y.; McDonald, C.F. Breathing exercises for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2012, 10, Cd008250. [Google Scholar] [CrossRef]
- Marillier, M.; Bernard, A.C.; Vergès, S.; Neder, J.A. Locomotor Muscles in COPD: The Rationale for Rehabilitative Exercise Training. Front. Physiol. 2019, 10, 1590. [Google Scholar] [CrossRef] [PubMed]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef]
- Prieur, G.; Combret, Y.; Medrinal, C.; Arnol, N.; Bonnevie, T.; Gravier, F.E.; Quieffin, J.; Lamia, B.; Reychler, G.; Borel, J.C. Energy conservation technique improves dyspnoea when patients with severe COPD climb stairs: A randomised crossover study. Thorax 2020, 75, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Dal Corso, S.; Spruit, M.A. Pulmonary Rehabilitation; (ERS Monogram); European Respiratory Society: Lausanne, Switzerland, 2021. [Google Scholar]
- Figueiredo, R.I.N.; Azambuja, A.M.; Cureau, F.V.; Sbruzzi, G. Inspiratory Muscle Training in COPD. Respir. Care 2020, 65, 1189–1201. [Google Scholar] [CrossRef]
- Beaumont, M.; Forget, P.; Couturaud, F.; Reychler, G. Effects of inspiratory muscle training in COPD patients: A systematic review and meta-analysis. Clin. Respir. J. 2018, 12, 2178–2188. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intervention Group | Control Group | ||
|---|---|---|---|
| n = 19 | n = 18 | p Value | |
| Demographic data | |||
| Age, years | 67 [63–71] | 68 [63–75] | 0.760 |
| Female sex, n (%) | 8 (42) | 7 (39) | 0.842 |
| BMI, kg/m2 | 20.9 [20.2–22.4] | 22.6 [18.9–27.5] | 0.261 |
| Comorbidities, n (%) | |||
| Gastroesophageal reflux | 7 (37) | 4 (22) | 0.476 |
| Chronic heart failure | 8 (42) | 8 (44) | 0.886 |
| Angina/myocardial infarction | 6 (32) | 6 (33) | 0.909 |
| Diabetes | 6 (32) | 3 (17) | 0.447 |
| Lung malignancy | 2 (11) | 0 (0) | 0.486 |
| Osteoporosis | 2 (11) | 11 (61) | 0.002 |
| Hypertension | 10 (53) | 7 (39) | 0.402 |
| Lung function | |||
| FEV1 (% pred) | 33.0 [26.0–44.5] | 33.5 [24.0–48.0] | 0.951 |
| FEV1/FVC (%) | 56.0 [42.5–60.0] | 49.0 [37.0–60.0] | 0.484 |
| RV (% pred) | 160.0 [155.0–206.5] | 171.0 [157.0–205.0] | 0.637 |
| Clinical characteristics | |||
| Dyspnea (Borg 0–10) | 8 [7–8] | 8 [8–8] | 0.349 |
| 5STST (s) | 15.4 [12.0–19.0] | 15.1 [13.5–26.4] | 0.412 |
| HG strength (kg) | 23.5 [20.5–26.8] | 23.3 [17.5–27.5] | 0.715 |
| CAT score | 25.0 [14.0–27.5] | 22.5 [18.0–26.0] | 0.808 |
| SGRQ score | 60.4 [43.6–71.8] | 61.2 [47.6–72.0] | 0.927 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazorla, S.; Busegnies, Y.; D’Ans, P.; Héritier, M.; Poncin, W. Breathing Control Exercises Delivered in a Group Setting for Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Healthcare 2023, 11, 877. https://doi.org/10.3390/healthcare11060877
Cazorla S, Busegnies Y, D’Ans P, Héritier M, Poncin W. Breathing Control Exercises Delivered in a Group Setting for Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Healthcare. 2023; 11(6):877. https://doi.org/10.3390/healthcare11060877
Chicago/Turabian StyleCazorla, Sibylle, Yves Busegnies, Pierre D’Ans, Marielle Héritier, and William Poncin. 2023. "Breathing Control Exercises Delivered in a Group Setting for Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial" Healthcare 11, no. 6: 877. https://doi.org/10.3390/healthcare11060877
APA StyleCazorla, S., Busegnies, Y., D’Ans, P., Héritier, M., & Poncin, W. (2023). Breathing Control Exercises Delivered in a Group Setting for Patients with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Healthcare, 11(6), 877. https://doi.org/10.3390/healthcare11060877