
Healthcare Professionals’ Perceptions, Barriers, and Facilitators towards Adopting Computerised Clinical Decision Support Systems in Antimicrobial Stewardship in Jordanian Hospitals

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Compliance with Ethical Standards
2.2. Hospital Setting and Participants
2.3. Questionnaire Development and Data Collection
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Questionnaire
Appendix A.1. Section A. Demographics
- Please indicate your gender
- Male
- Female
- 2.
- Please indicate your age group
- 20–30
- 31–40
- 41–50
- 51–60
- >60
- 3.
- Please indicate your speciality that you have attained at this point in time:
- Internal medicine doctor
- Paediatric doctor
- Surgery doctor
- Infectious diseases doctor
- Haematology/oncology doctor
- Critical care doctor
- Clinical pharmacist
- Nurse
- Infection control specialist
- Microbiologist
- Other, please specify
- 4.
- Job grade
- Senior doctor
- Junior doctor
- Other allied health care professionals
Appendix A.2. Section B. Perception of Participants towards Antimicrobial Stewardship (AMS)

{kind=link}
{kind=link}
{kind=link}
| Strongly Disagree–Strongly Agree (1–5) | |||||
|---|---|---|---|---|---|
| Perceptions towards Antimicrobial Stewardship | Strongly Disagree | Disagree | Neither Disagree or Agree | Agree | Strongly Agree |
| Check your level of agreement with the following sentences: | |||||
| Antimicrobial prescribing at your hospital is already as good as it can be | 1 | 2 | 3 | 4 | 5 |
| Antimicrobial stewardship programs may improve patient care. | 1 | 2 | 3 | 4 | 5 |
| Antimicrobial stewardship should be incorporated at a hospital level | 1 | 2 | 3 | 4 | 5 |
| Antimicrobial stewardship programs may reduce the problem of antimicrobial resistance. | 1 | 2 | 3 | 4 | 5 |
| Adequate training should be provided to health care professionals on antimicrobial use | 1 | 2 | 3 | 4 | 5 |
Appendix A.3. Section C. Perceptions towards Electronic Prescribing and Electronic Health Record SystemAwareness and Previous Use
| Awareness and Previous Use | Yes | No | Don’t Know |
|---|---|---|---|
| Have you previously used electronic prescribing and electronic health record system? | 1 | 2 | 3 |
| Are you aware that electronic prescribing and electronic health record system can be used to facilitate antibiotic prescribing? | 1 | 2 | 3 |
| Are you aware that electronic prescribing and electronic health record system is capable of providing clinical decision support function in order to support evidence-based practice? | 1 | 2 | 3 |
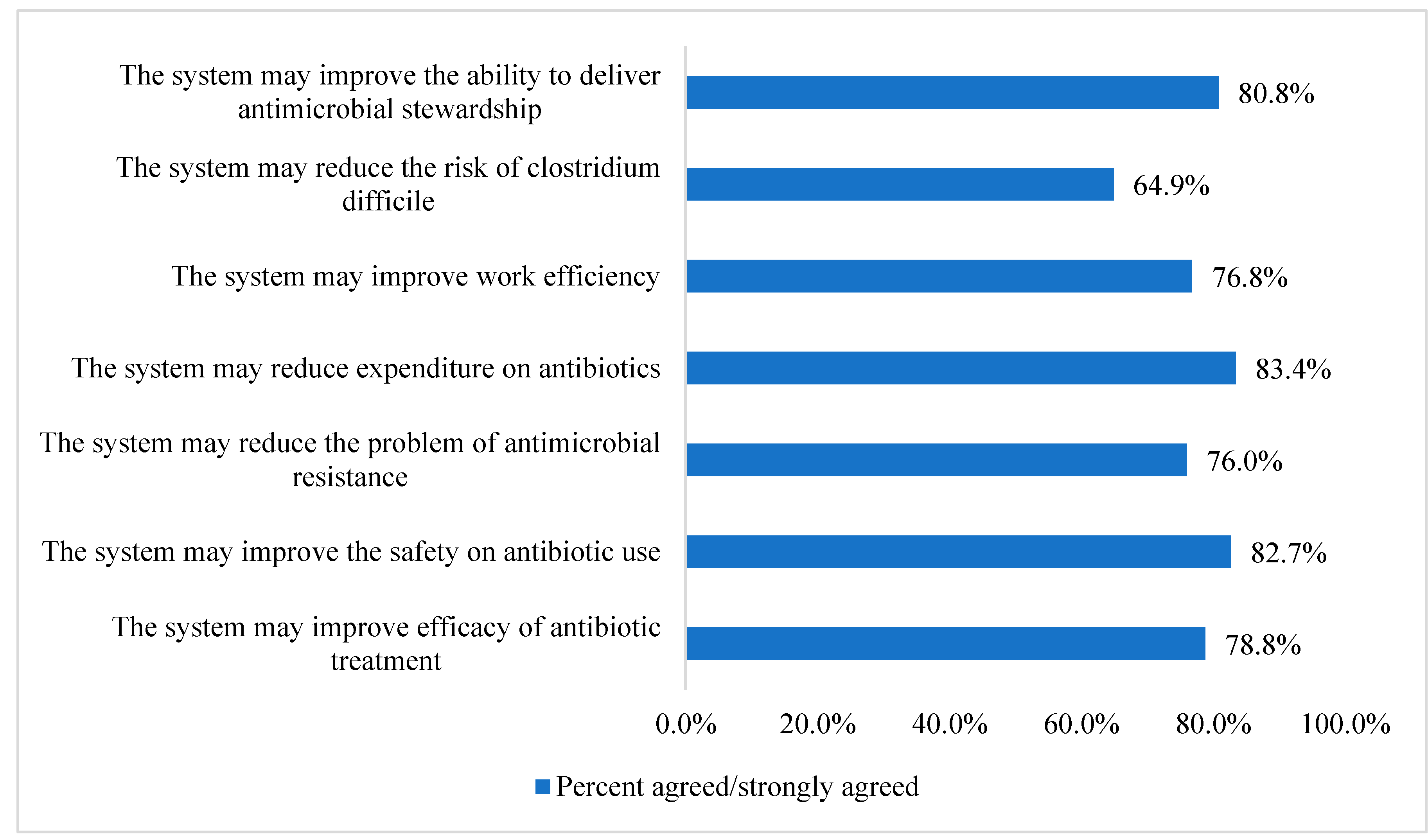
| Perceived Benefits of Using Electronic Prescribing and Electronic Health Record System in Antimicrobial Stewardship | Strongly Disagree | Disagree | Neither Disagree nor Agree | Agree | Strongly Agree |
|---|---|---|---|---|---|
| In my opinion, I believe my use of the electronic prescribing and electronic health record system may have the following benefits: | |||||
| The system may improve efficacy of antibiotic treatment | 1 | 2 | 3 | 4 | 5 |
| The system may improve the safety on antibiotic use | 1 | 2 | 3 | 4 | 5 |
| The system may reduce the problem of antimicrobial resistance | 1 | 2 | 3 | 4 | 5 |
| The system may reduce expenditure on antibiotics | 1 | 2 | 3 | 4 | 5 |
| The system may improve work efficiency | 1 | 2 | 3 | 4 | 5 |
| The system may reduce the risk of clostridium difficile | 1 | 2 | 3 | 4 | 5 |
| The system may improve the ability to deliver antimicrobial stewardship | 1 | 2 | 3 | 4 | 5 |
Appendix A.4. Section D. Perceived Barriers and Facilitators to Use Electronic Prescribing and Electronic Health Record System in Antim Crobial Stewardship
| Perceived Barriers | Strongly Disagree | Disagree | Neither Disagree nor Agree | Agree | Strongly Agree |
|---|---|---|---|---|---|
| In my opinion, I believe my use of electronic prescribing and electronic health record system is limited because of the following reason(s): | |||||
| Low level of awareness to the system | 1 | 2 | 3 | 4 | 5 |
| Unfamiliarity of using the system | 1 | 2 | 3 | 4 | 5 |
| Insufficient training to use the system | 1 | 2 | 3 | 4 | 5 |
| Lack of access to reliable technical support to solve day to day problems related to the system | 1 | 2 | 3 | 4 | 5 |
| Lack of enough time to use the system | 1 | 2 | 3 | 4 | 5 |
| Rigidity of the system to be applicable for individual patients | 1 | 2 | 3 | 4 | 5 |
| Disruption of usual workflow pattern | 1 | 2 | 3 | 4 | 5 |
| Lack of sufficient computer terminals available to use the system | 1 | 2 | 3 | 4 | 5 |
| Lack of benefit of using the system | 1 | 2 | 3 | 4 | 5 |
| Limitation of medical autonomy | 1 | 2 | 3 | 4 | 5 |
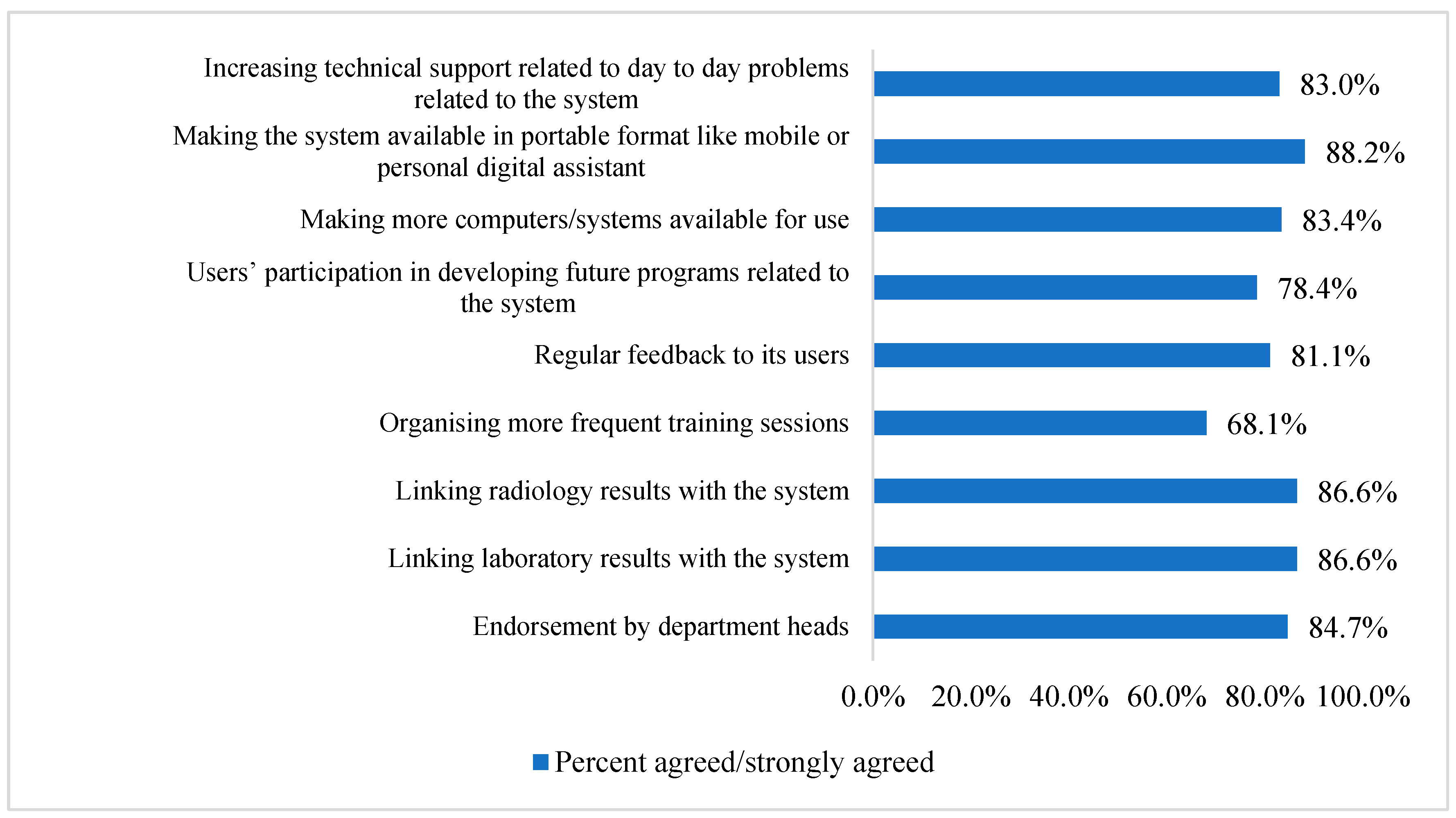
| Perceived Facilitators | Strongly Disagree | Disagree | Neither Agree nor Disagree | Agree | Strongly Agree |
|---|---|---|---|---|---|
| In my opinion, I believe that my use of electronic prescribing and electronic health record system will be facilitated because of the following reason(s) | |||||
| Endorsement by department heads | 1 | 2 | 3 | 4 | 5 |
| Linking laboratory results with the system | 1 | 2 | 3 | 4 | 5 |
| Linking radiology results with the system | 1 | 2 | 3 | 4 | 5 |
| Organising more frequent training sessions | 1 | 2 | 3 | 4 | 5 |
| Regular feedback to its users | 1 | 2 | 3 | 4 | 5 |
| Users’ participation in developing future programs related to the system | 1 | 2 | 3 | 4 | 5 |
| Making more computers/systems available for use | 1 | 2 | 3 | 4 | 5 |
| Making the system available in portable format like mobile or personal digital assistant | 1 | 2 | 3 | 4 | 5 |
| Increasing technical support related to day-to-day problems related to the system | 1 | 2 | 3 | 4 | 5 |
References
- Johnson, S.V.; Hoey, L.L.; Vance-Bryan, K. Inappropriate vancomycin prescribing based on criteria from the Centers for Disease Control and Prevention. Pharm. J. Hum. Pharm. Drug. Ther. 1995, 15, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Talbot, G.H.; Bradley, J.; Edwards, J.E., Jr.; Gilbert, D.; Scheld, M.; Bartlett, J.G. Bad bugs need drugs: An update on the development pipeline from the Antimicrobial Availability Task Force of the Infectious Diseases Society of America. Clin. Infect. Dis. 2006, 42, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Nusair, M.B.; Al-azzam, S.; Alhamad, H.; Momani, M.Y. The prevalence and patterns of self-medication with antibiotics in Jordan: A community-based study. Int. J. Clin. Pract. 2021, 75, e13665. [Google Scholar] [CrossRef] [PubMed]
- WHO. Antimicrobial Stewardship Programmes in Health-Care Facilities in Low- and Middle-Income Countries: A WHO Practical Toolkit [Internet]. 2019. Available online: https://apps.who.int/iris/handle/10665/329404 (accessed on 24 February 2023).
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef]
- Hashemite Kingdom of Jordan. National Action Plan to Combat Antimicrobial Resistance [Internet]. 2018. Available online: https://www.who.int/publications/m/item/jordan-national-action-plan-for-combating-antimicrobial-resistance-in-the-hashemite-kingdom-of-jordan (accessed on 24 February 2023).
- English, B.K.; Gaur, A.H. The use and abuse of antibiotics and the development of antibiotic resistance. Hot. Top Infect. Immun. Child. VI 2010, 659, 73–82. [Google Scholar]
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277. [Google Scholar]
- Alhamad, H.; Jaber, D.; Abu-Farha, R.; Albahar, F.; Edaily, S.M.; Donyai, P. Factors Influencing Public Willingness to Reuse the Unused Stored Medications in Jordan: A Cross-Sectional Study. Healthcare 2023, 11, 75. [Google Scholar] [CrossRef]
- Al-Azzam, S.I.; Al-Husein, B.A.; Alzoubi, F.; Masadeh, M.M. Self-medication with antibiotics in Jordanian population. Int. J. Occup. Med. Environ. Health 2007, 20, 373. [Google Scholar] [CrossRef]
- Sutton, R.T.; Pincock, D.; Baumgart, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An overview of clinical decision support systems: Benefits, risks, and strategies for success. NPJ Digit Med. 2020, 3, 1–10. [Google Scholar] [CrossRef]
- Curtis, C.E.; Al Bahar, F.; Marriott, J.F. The effectiveness of computerised decision support on antibiotic use in hospitals: A systematic review. PLoS ONE 2017, 12, e0183062. [Google Scholar] [CrossRef]
- Al Bahar, F.; Curtis, C.E.; Alhamad, H.; Marriott, J.F. The impact of a computerised decision support system on antibiotic usage in an English hospital. Int. J. Clin. Pharm. 2020, 42, 765–771. [Google Scholar] [CrossRef]
- Van Biesen, W.; Van Cauwenberge, D.; Decruyenaere, J.; Leune, T.; Sterckx, S. An exploration of expectations and perceptions of practicing physicians on the implementation of computerized clinical decision support systems using a Qsort approach. BMC Med. Inform. Decis. Mak. 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Oliver, K.; Egan, B.; Li, L.; Richardson, K.; Sandaradura, I.; Westbrook, J.I.; Day, R.O.; Baysari, M.T. Audit and feedback of antibiotic use. Appl. Clin. Inform. 2013, 4, 583–595. [Google Scholar] [CrossRef]
- Pawloski, P.A.; Brooks, G.A.; Nielsen, M.E.; Olson-Bullis, B.A. A systematic review of clinical decision support systems for clinical oncology practice. J. Natl. Compr. Cancer. Netw. 2019, 17, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Klarenbeek, S.E.; Weekenstroo, H.H.A.; Sedelaar, J.P.; Fütterer, J.J.; Prokop, M.; Tummers, M. The effect of higher level computerized clinical decision support systems on oncology care: A systematic review. Cancers 2020, 12, 1032. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Hernandez, B.; Charani, E.; Castro-Sanchez, E.; Herrero, P.; Hayhoe, B.; Hope, W.; Georgiou, P.; Holmes, A.H. A systematic review of clinical decision support systems for antimicrobial management: Are we failing to investigate these interventions appropriately? Clin. Microbiol. Infect. 2017, 23, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.J.; Wong, A.; Dhurjati, R.; Bristow, E.; Bastian, L.; Coeytaux, R.R.; Samsa, G.; Hasselblad, V.; Williams, J.W.; Musty, M.D.; et al. Effect of clinical decision-support systems: A systematic review. Ann. Intern. Med. 2012, 157, 29–43. [Google Scholar] [CrossRef]
- Roshanov, P.S.; Misra, S.; Gerstein, H.C.; Garg, A.X.; Sebaldt, R.J.; A Mackay, J.; Weise-Kelly, L.; Navarro, T.; Wilczynski, N.L.; Haynes, R.B.; et al. Computerized clinical decision support systems for chronic disease management: A decision-maker-researcher partnership systematic review. Implement. Sci. 2011, 6, 1–16. [Google Scholar] [CrossRef]
- Garg, A.X.; Adhikari, N.K.J.; McDonald, H.; Rosas-Arellano, M.P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, R.B. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: A systematic review. JAMA 2005, 293, 1223–1238. [Google Scholar] [CrossRef]
- Kawamoto, K.; Houlihan, C.A.; Balas, E.A.; Lobach, D.F. Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. BMJ 2005, 330, 765. [Google Scholar] [CrossRef]
- Rosenbloom, S.T.; Talbert, D.; Aronsky, D. Clinicians’ perceptions of clinical decision support integrated into computerized provider order entry. Int. J. Med. Inform. 2004, 73, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Satsangi, S.; Weir, C.R.; Morris, A.H.; Warner, H.R. Cognitive evaluation of the predictors of use of computerized protocols by clinicians. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Washington, DC, USA, 2003; p. 574. [Google Scholar]
- Zheng, K.; Padman, R.; Johnson, M.P.; Diamond, H.S. Understanding technology adoption in clinical care: Clinician adoption behavior of a point-of-care reminder system. Int. J. Med. Inform. 2005, 74, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Short, D.; Frischer, M.; Bashford, J. Barriers to the adoption of computerised decision support systems in general practice consultations: A qualitative study of GPs’ perspectives. Int. J. Med. Inform. 2004, 73, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, A.; Simon, S.R.; Schneider, J.; Krall, M.; Laferriere, D.; Smith, D.H.; Dean, F.; Stephen, B. How to design computerized alerts to ensure safe prescribing practices. Jt. Comm. J. Qual. Saf. 2004, 30, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Moxey, A.; Robertson, J.; Newby, D.; Hains, I.; Williamson, M.; Pearson, S.-A. Computerized clinical decision support for prescribing: Provision does not guarantee uptake. J. Am. Med. Informatics. Assoc. 2010, 17, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, S.T.R.; Marriott, J.L. Barriers and facilitators to adoption of a web-based antibiotic decision support system. S. Med. Rev. 2012, 5, 42. [Google Scholar]
- Paskovaty, A.; Pflomm, J.M.; Myke, N.; Seo, S.K. A multidisciplinary approach to antimicrobial stewardship: Evolution into the 21st century. Int. J. Antimicrob. Agents 2005, 25, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.L. The role of antimicrobial management programs in optimizing antibiotic prescribing within hospitals. Clin. Infect. Dis. 2006, 42 (Suppl. S2), S90–S95. [Google Scholar] [CrossRef] [PubMed]
- Bearden, D.T.; Allen, G.P. Impact of antimicrobial control programs on patient outcomes: Pharmacy perspective. Dis. Manag. Health Outcomes 2003, 11, 723–736. [Google Scholar] [CrossRef]
- Samore, M.H.; Bateman, K.; Alder, S.C.; Hannah, E.; Donnelly, S.; Stoddard, G.J.; Haddadinet, B.; Rubin, M.A.; Williamson, J.; Stults, B.; et al. Clinical decision support and appropriateness of antimicrobial prescribing: A randomized trial. JAMA 2005, 294, 2305–2314. [Google Scholar] [CrossRef] [PubMed]
- McGregor, J.C.; Weekes, E.; Forrest, G.N.; Standiford, H.C.; Perencevich, E.N.; Furuno, J.P.; Harris, A.D. Impact of a computerized clinical decision support system on reducing inappropriate antimicrobial use: A randomized controlled trial. J. Am. Med. Inform. Assoc. 2006, 13, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Albarillo, F.S.; Labuszewski, L.; Lopez, J.; Santarossa, M.; Bhatia, N.K. Use of a Clinical Decision Support System (CDSS) to improve antimicrobial stewardship efforts at a single academic medical center. Germs 2019, 9, 106. [Google Scholar] [CrossRef] [PubMed]
- Nassar, H.; Abu-Farha, R.; Barakat, M.; Alefishat, E. Antimicrobial Stewardship from Health Professionals’ Perspective: Awareness, Barriers, and Level of Implementation of the Program. Antibiotics 2022, 11, 99. [Google Scholar] [CrossRef] [PubMed]
- Laka, M.; Milazzo, A.; Merlin, T. Factors That Impact the Adoption of Clinical Decision Support Systems (CDSS) for Antibiotic Management. Int. J. Environ. Res. Public Health 2021, 18, 1901. [Google Scholar] [CrossRef]
- Lugtenberg, M.; Weenink, J.-W.; van der Weijden, T.; Westert, G.P.; Kool, R.B. Implementation of multiple-domain covering computerized decision support systems in primary care: A focus group study on perceived barriers. BMC Med. Inform. Decis. Mak. 2015, 15, 1–11. [Google Scholar] [CrossRef]
- Varonen, H.; Kortteisto, T.; Kaila, M.; Group Ebm, S. What may help or hinder the implementation of computerized decision support systems (CDSSs): A focus group study with physicians. Fam. Pract. 2008, 25, 162–167. [Google Scholar] [CrossRef]
- Khairat, S.; Marc, D.; Crosby, W.; Al Sanousi, A. Reasons for physicians not adopting clinical decision support systems: Critical analysis. JMIR Med. Inform. 2018, 6, e24. [Google Scholar] [CrossRef]
- Westerbeek, L.; Ploegmakers, K.J.; de Bruijn, G.-J.; Linn, A.J.; van Weert, J.C.; Daams, J.G.; van der Velde, N.; van Weert, H.C.; Abu-Hanna, A.; Medlock, S. Barriers and Facilitators Influencing Medication-Related CDSS Acceptance According to Clinicians: A Systematic Review. Int. J. Med. Inform. 2021, 152, 104506. [Google Scholar] [CrossRef]
- Lai, F.; Macmillan, J.; Daudelin, D.H.; Kent, D.M. The potential of training to increase acceptance and use of computerized decision support systems for medical diagnosis. Hum. Factors 2006, 48, 95–108. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Kern, J.K.; Marcee, A.; Grannemann, B.; Kleiber, B.; Bettinger, T.; Altshuler, K.Z.; McClelland, A. Development and implementation of computerized clinical guidelines: Barriers and solutions. Methods Inf. Med. 2002, 41, 435–442. [Google Scholar] [CrossRef]
- Tsiknakis, M.; Kouroubali, A. Organizational factors affecting successful adoption of innovative eHealth services: A case study employing the FITT framework. Int. J. Med. Inform. 2009, 78, 39–52. [Google Scholar] [CrossRef]
- Rahal, R.M.; Mercer, J.; Kuziemsky, C.; Yaya, S. Factors affecting the mature use of electronic medical records by primary care physicians: A systematic review. BMC Med. Inform. Decis. Mak. 2021, 21, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Randhawa, G.K.; Shachak, A.; Courtney, K.L.; Kushniruk, A. Evaluating a post-implementation electronic medical record training intervention for diabetes management in primary care. BMJ Health Care Inform. 2019, 26, e100086. [Google Scholar] [CrossRef] [PubMed]
- Msiska, K.E.M.; Kumitawa, A.; Kumwenda, B. Factors affecting the utilisation of electronic medical records system in Malawian central hospitals. Malawi Med. J. 2017, 29, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Paré, G.; Raymond, L.; de Guinea, A.O.; Poba-Nzaou, P.; Trudel, M.-C.; Marsan, J.; Micheneau, T. Electronic health record usage behaviors in primary care medical practices: A survey of family physicians in Canada. Int. J. Med. Inform. 2015, 84, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Sorgner, A. The impact of new digital technologies on gender equality in developing countries. Incl. Sustain. Ind. Dev. Work. Pap. Ser. 2019, 20, 2019. [Google Scholar]
- Asch, D.A.; Jedrziewski, M.K.; Christakis, N.A. Response rates to mail surveys published in medical journals. J. Clin. Epidemiol. 1997, 50, 1129–1136. [Google Scholar] [CrossRef] [PubMed]



| Parameter | n (%) |
|---|---|
| Age (years) | |
| 20–30 | 193 (76.0) |
| 31–40 | 54 (21.3) |
| 41–50 | 5 (2.0) |
| 51–60 | 0 (0.0) |
| >61 | 2 (0.8) |
| Gender | |
| Males | 104 (40.9) |
| Females | 150 (59.1) |
| Speciality | |
| Clinical pharmacist | 60 (23.6) |
| Physicians | 154 (60.6) |
| Nurse | 40 (15.7) |
| Statements | Strongly Agreed/Agreed |
|---|---|
| Have you previously used electronic prescribing and electronic health record systems? | |
| Yes | 220 (86.6) |
| No/Not sure | 34 (13.4) |
| Are you aware that electronic prescribing and electronic health record systems can be used to facilitate antibiotic prescribing? | |
| Yes | 184 (72.4) |
| No/Not sure | 70 (27.6) |
| Are you aware that electronic prescribing and electronic health record system is capable of providing clinical decision support function in order to support evidence-based practice? | |
| Yes | 161 (63.4) |
| No/Not sure | 93 (36.6) |
| Strongly Agreed/Agreed n (%) | |||||
|---|---|---|---|---|---|
| Statements | Total | Clinical Pharmacists n = 60 | Nurses n = 40 | Physicians n = 154 | p-Value # |
| Antimicrobial prescribing at your hospital is already as good as it can be | 133 (52.4) | 19 (31.7) | 26 (65.0) | 88 (57.1) | 0.001 * |
| Antimicrobial stewardship programs may improve patient care. | 224 (88.2) | 59 (98.3) | 31 (77.5) | 134 (87.0) | 0.005 * |
| Antimicrobial stewardship should be incorporated at a hospital level | 229 (90.2) | 56 (93.3) | 27 (67.5) | 146 (94.8) | <0.001 * |
| Antimicrobial stewardship programs may reduce the problem of antimicrobial resistance. | 228 (89.7) | 57 (95.0) | 31 (77.5) | 140 (90.9) | 0.014 * |
| Adequate training should be provided to healthcare professionals on antimicrobial use | 235 (92.5) | 58 (96.7) | 30 (75.0) | 147 (95.5) | <0.001 * |
| Parameter | Awareness [0: No, 1: Yes] | |||
|---|---|---|---|---|
| OR | p-Value # | OR | p-Value $ | |
| Age (years) 20–30 years >31 years | Reference 3.135 | 0.005 ^ | 2.130 | 0.079 |
| Gender Male Female | Reference 0.394 | 0.003 ^ | 0.402 | 0.006 * |
| Speciality Physicians Clinical pharmacists Nurses | Reference 1.322 4.327 | 0.410 0.008 ^ | 1.636 3.249 | 0.172 0.041 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albahar, F.; Abu-Farha, R.K.; Alshogran, O.Y.; Alhamad, H.; Curtis, C.E.; Marriott, J.F. Healthcare Professionals’ Perceptions, Barriers, and Facilitators towards Adopting Computerised Clinical Decision Support Systems in Antimicrobial Stewardship in Jordanian Hospitals. Healthcare 2023, 11, 836. https://doi.org/10.3390/healthcare11060836
Albahar F, Abu-Farha RK, Alshogran OY, Alhamad H, Curtis CE, Marriott JF. Healthcare Professionals’ Perceptions, Barriers, and Facilitators towards Adopting Computerised Clinical Decision Support Systems in Antimicrobial Stewardship in Jordanian Hospitals. Healthcare. 2023; 11(6):836. https://doi.org/10.3390/healthcare11060836
Chicago/Turabian StyleAlbahar, Fares, Rana K. Abu-Farha, Osama Y. Alshogran, Hamza Alhamad, Chris E. Curtis, and John F. Marriott. 2023. "Healthcare Professionals’ Perceptions, Barriers, and Facilitators towards Adopting Computerised Clinical Decision Support Systems in Antimicrobial Stewardship in Jordanian Hospitals" Healthcare 11, no. 6: 836. https://doi.org/10.3390/healthcare11060836
APA StyleAlbahar, F., Abu-Farha, R. K., Alshogran, O. Y., Alhamad, H., Curtis, C. E., & Marriott, J. F. (2023). Healthcare Professionals’ Perceptions, Barriers, and Facilitators towards Adopting Computerised Clinical Decision Support Systems in Antimicrobial Stewardship in Jordanian Hospitals. Healthcare, 11(6), 836. https://doi.org/10.3390/healthcare11060836