

Convergent Validity of the Edinburgh Postnatal Depression Scale and the Patient Health Questionnaire (PHQ-9) in Pregnant and Postpartum Women: Their Construct Correlations with Functional Disability

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Assessing Depression, Anxiety, and Disability
2.3. Statistical Analysis
3. Results
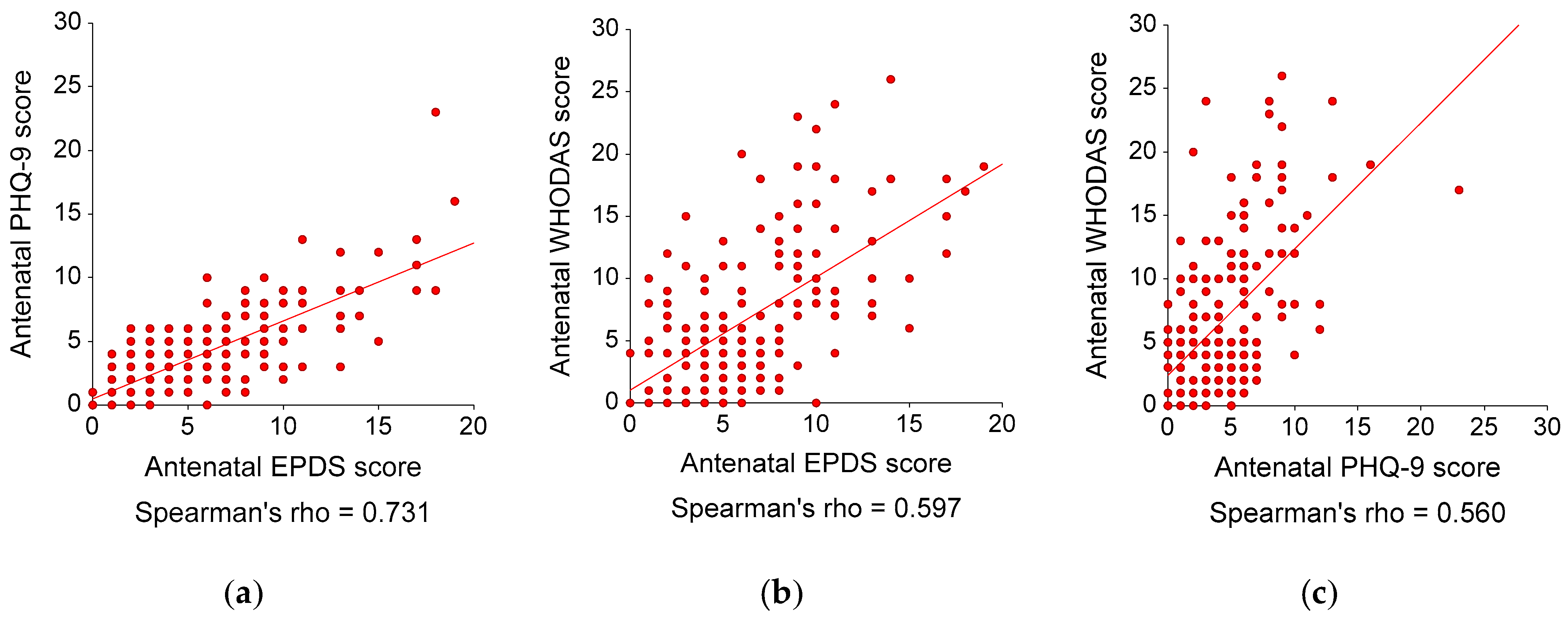
3.1. Antenatal Data Analysis
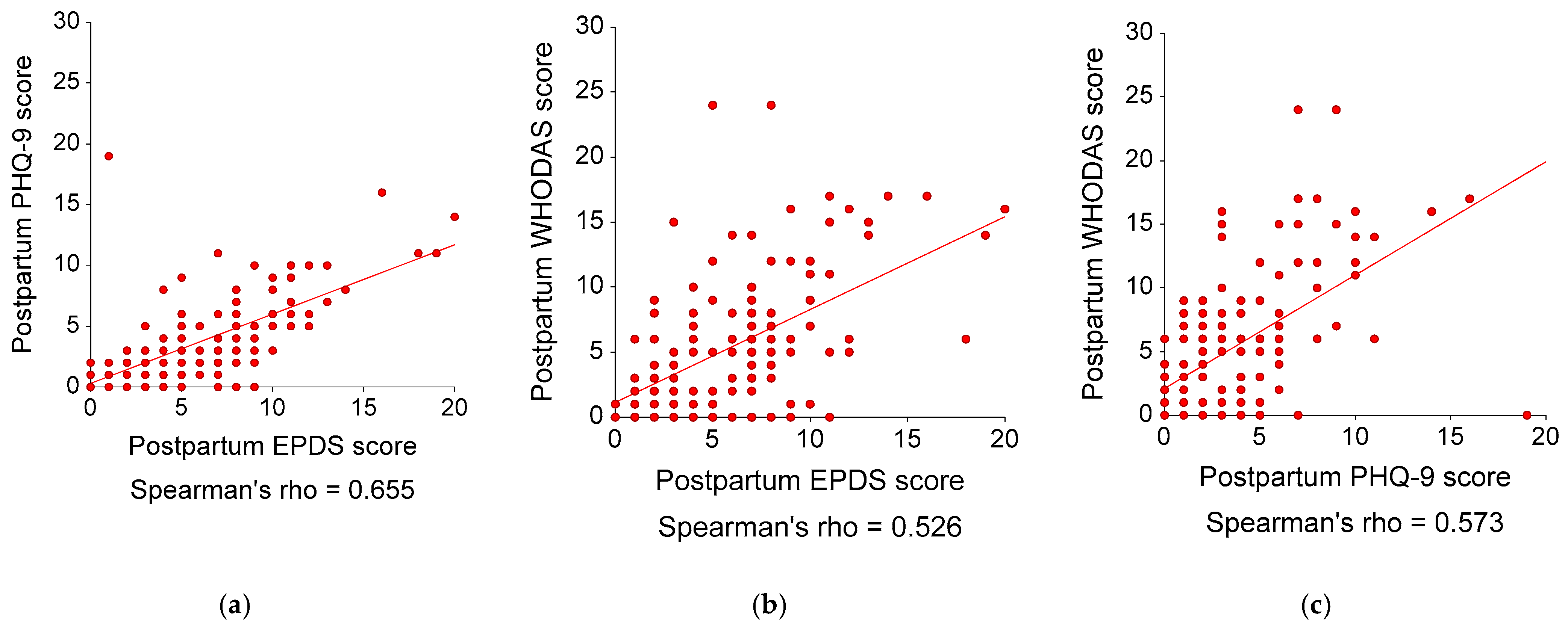
3.2. Postpartum Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anokye, R.; Acheampong, E.; Budu-Ainooson, A.; Obeng, E.I.; Akwasi, A.G. Prevalence of Postpartum Depression and Interventions Utilized for Its Management. Ann. Gen. Psychiatry 2018, 17, 18. [Google Scholar] [CrossRef] [PubMed]
- Okagbue, H.I.; Adamu, P.I.; Bishop, S.A.; Oguntunde, P.E.; Opanuga, A.A.; Akhmetshin, E.M. Systematic Review of Prevalence of Antepartum Depression during the Trimesters of Pregnancy. Open Access Maced J. Med. Sci. 2019, 7, 1555–1560. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.; Cabral de Mello, M.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and Determinants of Common Perinatal Mental Disorders in Women in Low- and Lower-Middle-Income Countries: A Systematic Review. Bull. World Health Organ. 2012, 90, 139G–149G. [Google Scholar] [CrossRef] [PubMed]
- ACOG Committee. ACOG Committee Opinion No. 757 Screening for Perinatal Depression. Obstet. Gynecol. 2018, 132, e208–e212. [Google Scholar] [CrossRef]
- Maurer, D.M.; Raymond, T.J.; Davis, B.N. Depression: Screening and Diagnosis. Am. Fam. Physician 2018, 98, 508–515. [Google Scholar]
- Smith, M.S.; Cairns, L.; Pullen, L.S.W.; Opondo, C.; Fellmeth, G.; Alderdice, F. Validated Tools to Identify Common Mental Disorders in the Perinatal Period: A Systematic Review of Systematic Reviews. J. Affect. Disord. 2022, 298, 634–643. [Google Scholar] [CrossRef]
- Zhong, Q.; Gelaye, B.; Rondon, M.; Sánchez, S.E.; García, P.J.; Sánchez, E.; Barrios, Y.V.; Simon, G.E.; Henderson, D.C.; Cripe, S.M.; et al. Comparative Performance of Patient Health Questionnaire-9 and Edinburgh Postnatal Depression Scale for Screening Antepartum Depression. J. Affect. Disord. 2014, 162, 1–7. [Google Scholar] [CrossRef]
- Hewitt, C.; Gilbody, S.; Brealey, S.; Paulden, M.; Palmer, S.; Mann, R.; Green, J.; Morrell, J.; Barkham, M.; Light, K.; et al. Methods to Identify Postnatal Depression in Primary Care: An Integrated Evidence Synthesis and Value of Information Analysis. Health Technol. Assess. 2009, 13, 147–230. [Google Scholar] [CrossRef]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D.; DEPRESsion Screening Data (DEPRESSD) EPDS Group; He, C.; Krishnan, A.; Wu, Y.; Bhandari, P.M.; et al. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for Screening to Detect Major Depression among Pregnant and Postpartum Women: Systematic Review and Meta-Analysis of Individual Participant Data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef]
- Bunevicius, A.; Kusminskas, L.; Pop, V.J.; Pedersen, C.A.; Bunevicius, R. Screening for Antenatal Depression with the Edinburgh Depression Scale. J. Psychosom. Obstet. Gynaecol. 2009, 30, 238–243. [Google Scholar] [CrossRef]
- Pitanupong, J.; Liabsuetrakul, T.; Vittayanont, A. Validation of the Thai Edinburgh Postnatal Depression Scale for Screening Postpartum Depression. Psychiatry Res. 2007, 149, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Kroenke, K.; Stump, T.E.; Monahan, P.O. Screening for Perinatal Depression with the Patient Health Questionnaire Depression Scale (PHQ-9): A Systematic Review and Meta-Analysis. Gen. Hosp. Psychiatry 2021, 68, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Aurpibul, L.; Tongprasert, F.; Wichasilp, U.; Tangmunkongvorakul, A. Depressive Symptoms Associated with Low Quality of Life Among Pregnant and Postpartum Women Living with HIV in Chiang Mai, Thailand. Int. J. MCH AIDS 2020, 9, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Velloza, J.; Njoroge, J.; Ngure, K.; Thuo, N.; Kiptinness, C.; Momanyi, R.; Ayub, S.; Gakuo, S.; Mugo, N.; Simoni, J.; et al. Cognitive Testing of the PHQ-9 for Depression Screening among Pregnant and Postpartum Women in Kenya. BMC Psychiatry 2020, 20, 31. [Google Scholar] [CrossRef] [PubMed]
- Üstün, T.B.; Kostanjsek, N.; Chatterji, S.; Rehm, J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010; ISBN 92-4-154759-6. [Google Scholar]
- Ustün, B.; Kennedy, C. What Is “Functional Impairment”? Disentangling Disability from Clinical Significance. World Psychiatry 2009, 8, 82–85. [Google Scholar] [CrossRef]
- Vázquez-Barquero, L.J. The Incorporation of the Disability Construct as an Independent Axis in the DSM-V and ICD-11 Diagnostic Systems. World Psychiatry 2009, 8, 92–94. [Google Scholar]
- Abma, I.L.; Rovers, M.; van der Wees, P.J. Appraising Convergent Validity of Patient-Reported Outcome Measures in Systematic Reviews: Constructing Hypotheses and Interpreting Outcomes. BMC Res. Notes 2016, 9, 226. [Google Scholar] [CrossRef]
- Weobong, B.; Akpalu, B.; Doku, V.; Owusu-Agyei, S.; Hurt, L.; Kirkwood, B.; Prince, M. The Comparative Validity of Screening Scales for Postnatal Common Mental Disorder in Kintampo, Ghana. J. Affect. Disord. 2009, 113, 109–117. [Google Scholar] [CrossRef]
- Barthel, D.; Barkmann, C.; Ehrhardt, S.; Schoppen, S.; Bindt, C. International CDS Study Group Screening for Depression in Pregnant Women from Côte D׳Ivoire and Ghana: Psychometric Properties of the Patient Health Questionnaire-9. J. Affect. Disord. 2015, 187, 232–240. [Google Scholar] [CrossRef]
- Oon-Arom, A.; Suradom, C.; Srichairatanakool, S.; Luewan, S.; Petiwathayakorn, T.; Maneeton, B.; Maneeton, N.; Kawilapat, S.; Srisurapanont, M. Serum Oxytocin and Corticotropin-Releasing Hormone Levels in the Third Trimester of Pregnancy for Predicting Postpartum Depression in Thai Women. Asian J. Psychiatry 2022, 80, 103392. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The Development and Validation of a Structured Diagnostic Psychiatric Interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33, quiz 34–57. [Google Scholar] [PubMed]
- Udomratn, P.; Kittirattanapaiboon, P. The Mini-International Neuropsychiatric Interview (Thai Version); Graphic Hut: Bangkok, Tailand, 2004. [Google Scholar]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Development of the 10-Item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Limlomwongse, N.; Liabsuetrakul, T. Cohort Study of Depressive Moods in Thai Women during Late Pregnancy and 6-8 Weeks of Postpartum Using the Edinburgh Postnatal Depression Scale (EPDS). Arch. Womens Ment. Health 2006, 9, 131–138. [Google Scholar] [CrossRef]
- Lotrakul, M.; Sumrithe, S.; Saipanish, R. Reliability and Validity of the Thai Version of the PHQ-9. BMC Psychiatry 2008, 8, 46. [Google Scholar] [CrossRef]
- Andrews, G.; Kemp, A.; Sunderland, M.; Von Korff, M.; Ustun, T.B. Normative Data for the 12 Item WHO Disability Assessment Schedule 2.0. PLoS ONE 2009, 4, e8343. [Google Scholar] [CrossRef] [PubMed]
- Parkitny, L.; McAuley, J. The Depression Anxiety Stress Scale (DASS). J. Physiother. 2010, 56, 204. [Google Scholar] [CrossRef]
- Loewenthal, K.; Eysenck, M.W. An Introduction to Psychological Tests and Scales, 2nd ed.; Psychology Press: Philadelphia, PA, USA, 2001; ISBN 978-1-84169-139-8. [Google Scholar]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires, 3rd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- NCSS, LLC NCSS 2021 Statistical Software 2021. Available online: https://www.ncss.com/software/ncss/ (accessed on 9 February 2023).
- Chiengthong, K.; Areeruk, W.; Santibenchakul, S.; Oranratanaphan, S.; Manchana, K. Universal COVID-19 Testing among Hospitalized Pregnant Women during the Initial COVID-19 Period in Thailand. Biomed. Sci. Clin. Med. 2022, 61, 121–126. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Pregnant Participants (N = 186) | Postpartum Participants (N = 136) |
|---|---|---|
| At the third-trimester visit during pregnancy | Mean (SD) | Mean (SD) |
| Age (years) | 29.46 (5.16) | 29.77 (5.34) |
| Education (years) | 14.06 (3.37) | 14.02 (3.34) |
| Body mass index (kg/m2) | 23.03 (4.46) | 23.23 (4.73) |
| DAS-depression score | 4.76 (5.20) | 4.23 (4.41) |
| DAS-anxiety score | 5.29 (5.08) | 4.94 (4.67) |
| DAS-stress score | 6.89 (6.97) | 6.76 (6.48) |
| Gestational number | 1.75 (0.88) | 1.75 (0.80) |
| Antenatal EPDS score | 6.35 (3.86) | 6.20 (3.61) |
| Antenatal PHQ-9 score | 4.38 (3.31) | 4.13 (2.82) |
| Antenatal WHODAS score | 6.79 (5.88) | 6.83 (5.89) |
| At the third-trimester visit during pregnancy | n (%) | n (%) |
| History of psychiatric disorders | 6 (3.23) | 5 (3.79) |
| Family history of psychiatric disorders | 12 (6.45) | 10 (7.58) |
| History of abortion | 40 (21.51) | 28 (21.21) |
| Labor characteristics | n (%) | |
| Assisted delivery/Cesarian section | 33 (25.00) | |
| Maternal complications | 51 (38.64) | |
| Newborn complications | 15 (11.36) | |
| 6 weeks postpartum | Mean (SD) | |
| Postpartum EPDS score | 5.83 (3.99) | |
| Postpartum PHQ-9 score | 3.62 (3.50) | |
| Postpartum WHODAS score | 5.27 (5.37) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srisurapanont, M.; Oon-arom, A.; Suradom, C.; Luewan, S.; Kawilapat, S. Convergent Validity of the Edinburgh Postnatal Depression Scale and the Patient Health Questionnaire (PHQ-9) in Pregnant and Postpartum Women: Their Construct Correlations with Functional Disability. Healthcare 2023, 11, 699. https://doi.org/10.3390/healthcare11050699
Srisurapanont M, Oon-arom A, Suradom C, Luewan S, Kawilapat S. Convergent Validity of the Edinburgh Postnatal Depression Scale and the Patient Health Questionnaire (PHQ-9) in Pregnant and Postpartum Women: Their Construct Correlations with Functional Disability. Healthcare. 2023; 11(5):699. https://doi.org/10.3390/healthcare11050699
Chicago/Turabian StyleSrisurapanont, Manit, Awirut Oon-arom, Chawisa Suradom, Suchaya Luewan, and Suttipong Kawilapat. 2023. "Convergent Validity of the Edinburgh Postnatal Depression Scale and the Patient Health Questionnaire (PHQ-9) in Pregnant and Postpartum Women: Their Construct Correlations with Functional Disability" Healthcare 11, no. 5: 699. https://doi.org/10.3390/healthcare11050699
APA StyleSrisurapanont, M., Oon-arom, A., Suradom, C., Luewan, S., & Kawilapat, S. (2023). Convergent Validity of the Edinburgh Postnatal Depression Scale and the Patient Health Questionnaire (PHQ-9) in Pregnant and Postpartum Women: Their Construct Correlations with Functional Disability. Healthcare, 11(5), 699. https://doi.org/10.3390/healthcare11050699