

Protocol for a Randomized Crossover Trial to Evaluate the Effect of Soft Brace and Rigid Orthosis on Performance and Readiness to Return to Sport Six Months Post-ACL-Reconstruction


 ,
,  ,
,  , ,
, ,  ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
- The influence of rigid orthoses and soft braces on the performance of the knee joint
- The activation of the gluteus medius and semitendinosus muscles and the associated influence on the cumulative DKV during landing maneuvers
- Conclusions on feedforward and feedback mechanisms during the test battery
Objectives and Hypothesis
2. Methods
2.1. Study Design
2.2. Participants
2.2.1. Inclusion Criteria
- six months (+/−1 month) after post-traumatic primary unilateral arthroscopically assisted ACLR, with the use of autologous ipsilateral semitendinosus graft;
- no additional procedures including meniscus sutures during the arthroscopically assisted ACLR;
- no osteoarthritis surgery during the arthroscopically assisted ACLR other than shaving;
- no history of injury or disease in the ACL-reconstructed limb prior to the ACL injury within the last 6 months;
- no history of injury or disease in the adjacent joints, contralateral limb, or spine within the last 6 months;
- age 18–40 years;
- Body Mass Index (BMI) smaller or equal to 24.9 kg/m2;
- moderate activity with regard to the rehabilitation plan, physiotherapy, and training therapy;
- frequent recreational sporting activity prior to the ACL injury.
2.2.2. Exclusion Criteria
- secondary ACLR;
- ACLR with the use of a method other than autologous ipsilateral semitendinosus tendon graft;
- diagnosed additional systematic diseases;
- current impaired performance due to previous injuries apart from the ACL injury;
- current permanent knee pain or swelling.
2.3. Procedure
3. The Extended Back in Action Battery Protocol
3.1. Balance Test
3.2. Jumps
3.2.1. General Criteria
- One practice trial with submaximal power (80% of the maximal power) is given, followed by three subsequent test trials
- Hands are placed on the hips during the jumps
- Starting position in the center of the plate, with feet parallel and shoulder-width apart
- Knee and hip joints are extended during the flight phase
- Soft landing in the center of the 3D force plate with knee over toe position, stable leg axis
- Single-leg landing: the contralateral leg is not allowed to touch the ground, otherwise the test is stopped immediately
3.2.2. Double-Leg Countermovement Jump (DL-CMJ)
3.2.3. Single-Leg Countermovement Jump (SL-CMJ)
3.2.4. Double-Leg Drop Jump (DL-DJ)
3.2.5. Single-Leg Landing (SL-Landing)
3.3. Jump Coordination
3.3.1. Speedy Jump (SL-SJ)
3.3.2. Quick-Feet-Test (SL-QFT)
3.4. Isometric Strength Tests
Gluteus Medius (G Med)
3.5. Questionnaire
3.6. Biomechanical Measurements
3.6.1. SEMG and MVC
3.6.2. 3D Force Plate
3.6.3. Motion Capture Camera Setup
4. Data Analysis and Planned Statistical Analysis
5. Discussion and Expected Results
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J.; Larson, D.R.; Dahm, D.L.; Levy, B.A.; Stuart, M.J.; Krych, A.J. Incidence of Anterior Cruciate Ligament Tears and Reconstruction: A 21-Year Population-Based Study. Am. J. Sports Med. 2016, 44, 1502–1507. [Google Scholar] [CrossRef] [PubMed]
- Gans, I.; Retzky, J.S.; Jones, L.C.; Tanaka, M.J. Epidemiology of Recurrent Anterior Cruciate Ligament Injuries in National Collegiate Athletic Association Sports: The Injury Surveillance Program, 2004–2014. Orthop J. Sports Med 2018, 6, 2325967118777823. [Google Scholar] [CrossRef]
- Acevedo, R.J.; Rivera-Vega, A.; Miranda, G.; Micheo, W. Anterior cruciate ligament injury: Identification of risk factors and prevention strategies. Curr. Sports Med. Rep. 2014, 13, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Andrä, K.; Kayaalp, E.; Prill, R.; Irlenbusch, L.; Liesaus, E.; Trommer, T.; Ullmann, P.; Becker, R. Joint effusion, anteroposterior stability, muscle strength and degree of patellofemoral osteoarthritis significantly impact outcome following revision ACL reconstruction. J. Exp. Orthop. 2021, 8, 70. [Google Scholar] [CrossRef]
- Prill, R.; Michel, S.; Schulz, R.; Coriolano, H.A. Body Composition and Strength Parameters in Elite Judo Athletes 5 Years after Anterior Cruciate Ligament Reconstruction. Int. J. Sports Med. 2019, 40, 38–42. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The long-term consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. Am. J. Sports Med. 2007, 35, 1756–1769. [Google Scholar] [CrossRef] [PubMed]
- Andrä, K.; Prill, R.; Kayaalp, E.; Irlenbusch, L.; Liesaus, E.; Trommer, T.; Ullmann, P.; Becker, R. Increase in cartilage degeneration in all knee compartments after failed ACL reconstruction at 4 years of follow-up. J. Orthop. Traumatol. 2021, 22, 54. [Google Scholar] [CrossRef]
- McHugh, M.P.; Tyler, T.F.; Browne, M.G.; Gleim, G.W.; Nicholas, S.J. Electromyographic predictors of residual quadriceps muscle weakness after anterior cruciate ligament reconstruction. Am. J. Sports Med. 2002, 30, 334–339. [Google Scholar] [CrossRef]
- Gokeler, A.; Neuhaus, D.; Benjaminse, A.; Grooms, D.R.; Baumeister, J. Principles of Motor Learning to Support Neuroplasticity After ACL Injury: Implications for Optimizing Performance and Reducing Risk of Second ACL Injury. Sports Med. 2019, 49, 853–865. [Google Scholar] [CrossRef]
- Larwa, J.; Stoy, C.; Chafetz, R.S.; Boniello, M.; Franklin, C. Stiff Landings, Core Stability, and Dynamic Knee Valgus: A Systematic Review on Documented Anterior Cruciate Ligament Ruptures in Male and Female Athletes. Int. J. Environ Res. Public Health 2021, 18, 3826. [Google Scholar] [CrossRef]
- Middlebrook, A.; Bekker, S.; Middlebrook, N.; Rushton, A.B. Physical prognostic factors predicting outcome following anterior cruciate ligament reconstruction: Protocol for a systematic review. BMJ Open 2020, 10, e033429. [Google Scholar] [CrossRef]
- Królikowska, A.; Czamara, A.; Szuba, Ł.; Reichert, P. The Effect of Longer versus Shorter Duration of Supervised Physiotherapy after ACL Reconstruction on the Vertical Jump Landing Limb Symmetry. Biomed Res. Int. 2018, 2018, 7519467. [Google Scholar] [CrossRef] [PubMed]
- Ashigbi, E.Y.K.; Banzer, W.; Niederer, D. Return to Sport Tests’ Prognostic Value for Reinjury Risk after Anterior Cruciate Ligament Reconstruction: A Systematic Review. Med. Sci. Sports Exerc. 2020, 52, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Cheney, S.; Chiaia, T.A.; de Mille, P.; Boyle, C.; Ling, D. Readiness to Return to Sport After ACL Reconstruction: A Combination of Physical and Psychological Factors. Sports Med. Arthrosc. Rev. 2020, 28, 66–70. [Google Scholar] [CrossRef]
- Padua, D.A.; DiStefano, L.J.; Beutler, A.I.; de la Motte, S.J.; DiStefano, M.J.; Marshall, S.W. The Landing Error Scoring System as a Screening Tool for an Anterior Cruciate Ligament Injury–Prevention Program in Elite-Youth Soccer Athletes. J. Athl. Train. 2015, 50, 589–595. [Google Scholar] [CrossRef]
- Paterno, M.V.; Schmitt, L.C.; Ford, K.R.; Rauh, M.J.; Myer, G.D.; Huang, B.; Hewett, T.E. Biomechanical Measures during Landing and Postural Stability Predict Second Anterior Cruciate Ligament Injury after Anterior Cruciate Ligament Reconstruction and Return to Sport. Am. J. Sport. Med. 2010, 38, 1968–1978. [Google Scholar] [CrossRef] [PubMed]
- Herbst, E.; Hoser, C.; Hildebrandt, C.; Raschner, C.; Hepperger, C.; Pointner, H.; Fink, C. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part II: Clinical application of a new test battery. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1283–1291. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Hewett, T.E. What is the Evidence for and Validity of Return-to-Sport Testing after Anterior Cruciate Ligament Reconstruction Surgery? A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 917–929. [Google Scholar] [CrossRef]
- Ebert, J.R.; Edwards, P.; Currie, J.; Smith, A.; Joss, B.; Ackland, T.; Buelow, J.U.; Hewitt, B. COMPARISON OF THE ‘BACK IN ACTION’ TEST BATTERY TO STANDARD HOP TESTS AND ISOKINETIC KNEE DYNAMOMETRY IN PATIENTS FOLLOWING ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION. Int. J. Sports Phys. Ther. 2018, 13, 389–400. [Google Scholar]
- Sugimoto, D.; LeBlanc, J.C.; Wooley, S.E.; Micheli, L.J.; Kramer, D.E. The Effectiveness of a Functional Knee Brace on Joint-Position Sense in Anterior Cruciate Ligament-Reconstructed Individuals. J. Sport Rehabil. 2016, 25, 190–194. [Google Scholar] [CrossRef]
- Prill, R.; Cruysen, C.; Królikowska, A.; Kopf, S.; Becker, R. Knee Orthotics Do Not Influence Coordinative Skills—A Randomized Controlled Crossover Pilot Trial. J. Pers. Med. 2022, 12, 1509. [Google Scholar] [PubMed]
- Salata, M.J.; Gibbs, A.E.; Sekiya, J.K. The effectiveness of prophylactic knee bracing in american football: A systematic review. Sports Health 2010, 2, 375–379. [Google Scholar] [CrossRef]
- Riemann, B.L.; Lephart, S.M. The sensorimotor system, part I: The physiologic basis of functional joint stability. J. Athl. Train 2002, 37, 71–79. [Google Scholar]
- Riemann, B.L.; Lephart, S.M. The Sensorimotor System, Part II: The Role of Proprioception in Motor Control and Functional Joint Stability. J. Athl. Train 2002, 37, 80–84. [Google Scholar]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar]
- Cross, M.J.; Roger, G.; Kujawa, P.; Anderson, I.F. Regeneration of the semitendinosus and gracilis tendons following their transection for repair of the anterior cruciate ligament. Am. J. Sports Med. 1992, 20, 221–223. [Google Scholar] [CrossRef]
- Suijkerbuijk, M.A.M.; Reijman, M.; Lodewijks, S.J.; Punt, J.; Meuffels, D.E. Hamstring Tendon Regeneration After Harvesting: A Systematic Review. Am. J. Sports Med. 2015, 43, 2591–2598. [Google Scholar] [CrossRef]
- Rinaldi, V.G.; Prill, R.; Jahnke, S.; Zaffagnini, S.; Becker, R. The influence of gluteal muscle strength deficits on dynamic knee valgus: A scoping review. J. Exp. Orthop. 2022, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Antico, M.; Balletti, N.; Laudato, G.; Lazich, A.; Notarantonio, M.; Oliveto, R.; Ricciardi, S.; Scalabrino, S.; Simeone, J. Postural control assessment via Microsoft Azure Kinect DK: An evaluation study. Comput. Methods Programs Biomed 2021, 209, 106324. [Google Scholar] [CrossRef]
- Królikowska, A.; Maj, A.; Dejnek, M.; Prill, R.; Skotowska-Machaj, A.; Kołcz, A. Wrist motion assessment using Microsoft Azure Kinect DK: A reliability study in healthy individuals. Adv. Clin. Exp. Med. 2003. [Google Scholar] [CrossRef]
- Albert, J.A.; Owolabi, V.; Gebel, A.; Brahms, C.M.; Granacher, U.; Arnrich, B. Evaluation of the Pose Tracking Performance of the Azure Kinect and Kinect v2 for Gait Analysis in Comparison with a Gold Standard: A Pilot Study. Sensors (Basel) 2020, 20, 5104. [Google Scholar] [CrossRef]
- Cuthbert, S.C.; Goodheart, G.J. On the reliability and validity of manual muscle testing: A literature review. Chiropr. Osteopathy 2007, 15, 4. [Google Scholar] [CrossRef]
- Kaplan, Y.; Witvrouw, E. When Is It Safe to Return to Sport After ACL Reconstruction? Reviewing the Criteria. Sports Health 2019, 11, 301–305. [Google Scholar] [CrossRef]
- Crowell, K.R.; Nokes, R.D.; Cosby, N.L. Weak Hip Strength Increases Dynamic Knee Valgus in Single-Leg Tasks of Collegiate Female Athletes. J. Sport Rehabil. 2021, 30, 1220–1223. [Google Scholar] [CrossRef] [PubMed]
- Group K. MARS (Measurement, Analysis & Reporting Software). 2022. Available online: http://mars.s2p.si/ (accessed on 1 February 2023).
- Hildebrandt, C.; Müller, L.; Zisch, B.; Huber, R.; Fink, C.; Raschner, C. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part I: Development of a new test battery. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 1273–1281. [Google Scholar] [CrossRef]
- MARS. (Measurement, Analysis & Reporting Software) Module: Counter Movement Jump. Available online: http://mars.s2p.si/e_files/content/Counter%20Movement%20Jump.pdf (accessed on 1 February 2023).
- MARS. (Measurement, Analysis & Reporting Software) Module: Drop Jump. Available online: http://mars.s2p.si/e_files/content/Drop%20Jump.pdf (accessed on 1 February 2023).
- Ueno, R.; Navacchia, A.; DiCesare, C.A.; Ford, K.R.; Myer, G.D.; Ishida, T.; Tohyama, H.; Hewett, T.E. Knee abduction moment is predicted by lower gluteus medius force and larger vertical and lateral ground reaction forces during drop vertical jump in female athletes. J. Biomech. 2020, 103, 109669. [Google Scholar] [CrossRef]
- Llurda-Almuzara, L.; Pérez-Bellmunt, A.; López-de-Celis, C.; Aiguadé, R.; Seijas, R.; Casasayas-Cos, O.; Labata-Lezaun, N.; Alvarez, P. Normative data and correlation between dynamic knee valgus and neuromuscular response among healthy active males: A cross-sectional study. Sci. Rep. 2020, 10, 17206. [Google Scholar] [CrossRef]

| Run | Group A | Group B | Group C |
|---|---|---|---|
| 1 | orthosis | brace | no aid |
| 2 | brace | no aid | orthosis |
| 3 | no aid | orthosis | brace |
| Participants | |
| Signing informed consent and randomization ↓ IKDC, ACL-RSI, Tegner activity scale ↓ Placement EMG (both legs): Gluteus medius muscle and semitendinosus muscle ↓ Knee and hip range of motion measurement using standard goniometer ↓ Warm-up: 5 min. ergometer at 75 watts, 3 × 5 squats ↓ Putting on rigid orthosis or soft brace or leaving with no aid | |
| Functional—Biomechanical Assessment | |
| 1. Stability tests Equipment: Zebris, sEMG Variables: level of stability, center of pressure, muscle activity |  Picture 1
|
| 2. Jumps Equipment: 3D force plate Bertec, Azure Kinect, sEMG, vaulting box Variables: jump height (cm), power (W/kg), ground contact time (ms), reactivity (mm/ms), muscle activity, knee-angle |  Picture 2
|
| 3. Jump coordination Equipment: speedy basic jump set, quick feet jump set, stopwatch, tapping rate counter, sEMG, Azure Kinect Variables: time (s), tapping rate, muscle activity, knee-angle | 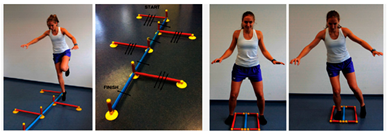 Picture 3
|
| 4. Isometric hip abductor strength test (rt/lt) Equipment: sEMG, Expander Variables: strength (N) muscle activity |  Picture 4
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jahnke, S.; Cruysen, C.; Prill, R.; Kittmann, F.; Pflug, N.; Albert, J.A.; de Camargo, T.; Arnrich, B.; Królikowska, A.; Kołcz, A.; et al. Protocol for a Randomized Crossover Trial to Evaluate the Effect of Soft Brace and Rigid Orthosis on Performance and Readiness to Return to Sport Six Months Post-ACL-Reconstruction. Healthcare 2023, 11, 513. https://doi.org/10.3390/healthcare11040513
Jahnke S, Cruysen C, Prill R, Kittmann F, Pflug N, Albert JA, de Camargo T, Arnrich B, Królikowska A, Kołcz A, et al. Protocol for a Randomized Crossover Trial to Evaluate the Effect of Soft Brace and Rigid Orthosis on Performance and Readiness to Return to Sport Six Months Post-ACL-Reconstruction. Healthcare. 2023; 11(4):513. https://doi.org/10.3390/healthcare11040513
Chicago/Turabian StyleJahnke, Sonja, Caren Cruysen, Robert Prill, Fabian Kittmann, Nicola Pflug, Justin Amadeus Albert, Tibor de Camargo, Bert Arnrich, Aleksandra Królikowska, Anna Kołcz, and et al. 2023. "Protocol for a Randomized Crossover Trial to Evaluate the Effect of Soft Brace and Rigid Orthosis on Performance and Readiness to Return to Sport Six Months Post-ACL-Reconstruction" Healthcare 11, no. 4: 513. https://doi.org/10.3390/healthcare11040513
APA StyleJahnke, S., Cruysen, C., Prill, R., Kittmann, F., Pflug, N., Albert, J. A., de Camargo, T., Arnrich, B., Królikowska, A., Kołcz, A., Reichert, P., Oleksy, Ł., Michel, S., Kopf, S., Wagner, M., Scheffler, S., & Becker, R. (2023). Protocol for a Randomized Crossover Trial to Evaluate the Effect of Soft Brace and Rigid Orthosis on Performance and Readiness to Return to Sport Six Months Post-ACL-Reconstruction. Healthcare, 11(4), 513. https://doi.org/10.3390/healthcare11040513