
Evaluation of Health Care Professionals’ Knowledge, Attitudes, and Practice to Prevent the Pandemic Spread of COVID-19: A Questionnaire-Based Cross-Sectional Study from Abha, Saudi Arabia

 ,
,  and
and
Abstract
:1. Introduction
2. Methodology
2.1. Design of the Research
2.2. Participants
2.3. Study Tool
2.4. Statistics
2.5. Ethical Approval
3. Results
3.1. Socio-Demographic Characteristics
3.2. Knowledge of HCPs about COVID-19
3.3. HCPs’ Attitudes towards COVID-19
3.4. Mean Score of Knowledge, Attitude, and Practice (KAP)
3.5. HCPs’ Practices towards COVID-19
4. Discussion
4.1. Summary and Comparisons
4.2. Study Limitations
4.3. Implications of Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yin, Y.; Wunderink, R.G. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology 2018, 23, 130–137. [Google Scholar]
- Schoeman, D.; Fielding, B.C. Coronavirus envelope protein: Current knowledge. Virol. J. 2019, 16, 69. [Google Scholar] [CrossRef]
- Kooli, C.; lock Son, M.; Beloufa, I. Business ethics in the era of COVID 19: How to protect jobs and employment rights through innovation. Avicenna 2022, 2022, 7. [Google Scholar] [CrossRef]
- Sirajudeen, J.; Nair, A.P.; Hassany, R.W.; Purayil, N.K.; Mathew, J.V.; Elmadhoun, I.T.; Mustafa, M. All those exanthematous fevers are not COVID-19. Avicenna 2021, 2021, 1. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease 2019 (COVID-19): World Health Organization. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 20 January 2021).
- Stephens, G.M.; Woo, P.C.; Zaki, A.M.; Memish, M.; Perlman, S.; Poon, L.L.; Snijder, E.J.; Fouchier, M.G.; Gorbalenya, A.E.; Ziad, A.; et al. Middle East Respiratory Syndrome. J. Virol. 2013, 87, 7790. [Google Scholar]
- Carlos, W.G.; Dela Cruz, C.S.; Cao, B.; Pasnick, S.; Jamil, S. Novel Wuhan (2019-nCoV) Coronavirus. Am. J. Respir. Crit. Care Med. 2020, 201, 7–8. [Google Scholar] [CrossRef]
- WHO. Situation Reports. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200306-sitrep-46-COVID-19.pdf?sfvrsn=96b04adf_2 (accessed on 7 December 2020).
- Memish, Z.A.; Zumla, A.; Alhakeem, R.F.; Assiri, A.; Turkestani, A.; Al Harby, K.D.; Alyemni, M.; Dhafar, K.; Gautret, P.; Barbeschi, M.; et al. Hajj: Infectious disease surveillance and control. Lancet 2014, 383, 2073–2082. [Google Scholar] [PubMed]
- Saudi Center for Disease Prevention and Control (SCDC). Available online: https://covid19.cdc.gov.sa/daily-updates/ (accessed on 20 February 2021).
- Kooli, C. COVID-19: Public health issues and ethical dilemmas. Ethics Med. Public Health 2021, 17, 100635. [Google Scholar] [CrossRef]
- Kooli, C. COVID-19 and the mental health of professionals in the health sector in the UAE: An analytical study. Avicenna 2021, 2021, 9. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [PubMed]
- Kooli, C. COVID-19: Challenges and opportunities. Avicenna 2021, 2021, 5. [Google Scholar] [CrossRef]
- Batool, M.; Hassan, J.; Shahzad, R.; Iqbal, S.; Butt, M.S.; Haider, S. A crisis within a crisis: Role of COVID-19 pandemic in poor compliance of Community-based Management of Severe Acute Malnutrition among children younger than five years in Pakistan. Avicenna 2023, 2023, 2. [Google Scholar] [CrossRef]
- World Health Organization. Responding to COVID-19: Real-Time Training for the Coronavirus Disease Outbreak. Available online: https://openwho.org/channels/COVID-19 (accessed on 18 February 2021).
- Hoffman, S.J.; Silverberg, S.L. Delays in global disease outbreak responses: Lessons from H1N1, Ebola, and Zika. Am. J. Public Health 2018, 108, 329–333. [Google Scholar]
- Bowdle, A.; Munoz-Price, L.S. Preventing infection of patients and healthcare workers should be the new normal in the era of novel coronavirus epidemics. Anesthesiology 2020, 132, 1292–1295. [Google Scholar] [CrossRef]
- World Health Organization. Infection Prevention and Control during Health Care When Novel Coronavirus (nCoV) Infection Is Suspected: Interim Guidance. 2020. Available online: https://www.who.int/publications-detail/infectionprevention-and-control-during-health-care-when-novel-coronavirus(ncov)-infection-issuspected-20200125 (accessed on 12 February 2021).
- Selvaraj, S.A.; Lee, K.E.; Harrell, M.; Ivanov, I.; Allegranzi, B. Infection rates and risk factors for infection among health workers during Ebola and Marburg virus outbreaks: A systematic review. J. Infect. Dis. 2018, 218 (Suppl. 5), S679–S689. [Google Scholar] [CrossRef]
- McCloskey, B.; Heymann, D.L. SARS to novel coronavirus—Old lessons and new lessons. Epidemiol. Infect. 2020, 148, e22. [Google Scholar]
- McEachan, R.; Taylor, N.; Harrison, R.; Lawton, R.; Gardner, P.; Conner, M. Meta-analysis of the reasoned action approach (RAA) to understanding health behaviors. Ann. Behav. Med. 2016, 50, 592–612. [Google Scholar]
- Cacciapaglia, G.; Cot, C.; Sannino, F. Second wave COVID-19 pandemics in Europe: A temporal playbook. Sci. Rep. 2020, 10, 15514. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: UK government must “get its act together” as modelling suggests 85 000 deaths in second wave, experts say. BMJ 2020, 371, m4242. [Google Scholar] [CrossRef]
- Ghanbari, B. On forecasting the spread of the COVID-19 in Iran: The second wave. Chaos Solitons Fractals 2020, 140, 110176. [Google Scholar] [CrossRef]
- Alshrari, A.S. Awareness of COVID-19 among the general population of the northern border region of Saudi Arabia. J. Pharm. Res. Int. 2020, 32, 23–34. [Google Scholar]
- Kassie, B.A.; Adane, A.; Tilahun, Y.T.; Kassahun, E.A.; Ayele, A.S.; Belew, A.K. Knowledge and attitude towards COVID-19 and associated factors among health care providers in Northwest Ethiopia. PLoS ONE 2020, 15, e0238415. [Google Scholar]
- Olum, R.; Chekwech, G.; Wekha, G. Dianah Rhoda Nassozi, Felix Bongomin. Coronavirus disease-2019: Knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Front. Public Health 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Asemahagn, M.A. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: A cross-sectional survey. Trop. Med. Health 2020, 48, 72. [Google Scholar] [PubMed]
- Limbu, D.K.; Piryani, R.M.; Sunny, A.K. Healthcare workers’ knowledge, attitude and practices during the COVID-19 pandemic response in a tertiary care hospital of Nepal. PLoS ONE 2020, 15, e0242126. [Google Scholar] [CrossRef]
- Temsah, M.H.; Al Huzaimi, A.; Alrabiaah, A.; Alamro, N.; Al-Sohime, F.; Al-Eyadhy, A.; Alhasan, K.; Kari, J.A.; Alhaboob, A.; Alsalmi, A.; et al. Changes in healthcare workers’ knowledge, attitudes, practices, and stress during the COVID-19 pandemic. Medicine 2021, 100, e25825. [Google Scholar] [PubMed]
- Khan, M.U.; Shah, S.; Ahmad, A.; Fatokun, O. Knowledge and attitude of healthcare workers about middle east respiratory syndrome in multispecialty hospitals of Qassim, Saudi Arabia. BMC Public Health 2014, 14, 1281. [Google Scholar]
- Huynh, G.; Nguyen, T.N.; Vo, K.N.; Pham, L.A. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac. J. Trop. Med. 2020, 13, 260. [Google Scholar]
- Bhagavathula, A.S.; Aldhaleei, W.A.; Rahmani, J.; Mahabadi, M.A.; Bandari, D.K. Novel coronavirus (COVID-19) knowledge and perceptions: A survey on healthcare workers. MedRxiv 2020. [Google Scholar] [CrossRef]
- Rapparini, C.; Barroso, P.F.; Saraceni, V.; Machado, A.A.; Fernandes, G.C. Occupationally acquired infectious diseases among health care workers in Brazil: Use of internet tools to improve management, prevention, and surveillance. Am. J. Infect. Control. 2007, 35, 267–270. [Google Scholar] [PubMed]
- Imai, T.; Takahashi, K.; Hoshuyama, T.; Hasegawa, N.; Lim, M.K.; Koh, D. SARS risk perceptions in healthcare workers, Japan. Emerg. Infect. Dis. 2005, 11, 404. [Google Scholar]
- Quah, S.R.; Hin-Peng, L. Crisis prevention and management during SARS outbreak, Singapore. Emerg. Infect. Dis. 2004, 10, 364. [Google Scholar] [PubMed]
- Thu, T.A.; Anh, N.Q.; Chau, N.Q.; Hung, N.V. Knowledge, attitude and practices regarding standard and isolation precautions among Vietnamese health care workers: A multicenter cross-sectional survey. Intern. Med. 2012, 2, 115. [Google Scholar]
- Joukar, F.; Mansour-Ghanaei, F.; Soati, F.; Meskinkhoda, P. Knowledge levels and attitudes of health care professionals toward patients with hepatitis C infection. World J. Gastroenterol. WJG 2012, 18, 2238. [Google Scholar] [CrossRef] [PubMed]
- Richmond, J.A.; Dunning, T.L.; Desmond, P.V. Health professionals’ attitudes toward caring for people with hepatitis C. J. Viral Hepat. 2007, 14, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Tamang, N.; Rai, P.; Dhungana, S.; Sherchan, B.; Shah, B.; Pyakurel, P.; Rai, S. COVID-19: A National Survey on perceived level of knowledge, attitude and practice among frontline healthcare Workers in Nepal. BMC Public Health 2020, 20, 1905. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Socio-Demographic Characteristics | Health Care Professionals | |
|---|---|---|
| n (491) | % | |
| Age | ||
| Less than 30 years | 396 | 80.7 |
| 30–39 years | 69 | 14.1 |
| 40–49 years | 19 | 3.9 |
| More than 50 years | 7 | 1.4 |
| Sex | ||
| Male | 273 | 55.6 |
| Female | 218 | 44.4 |
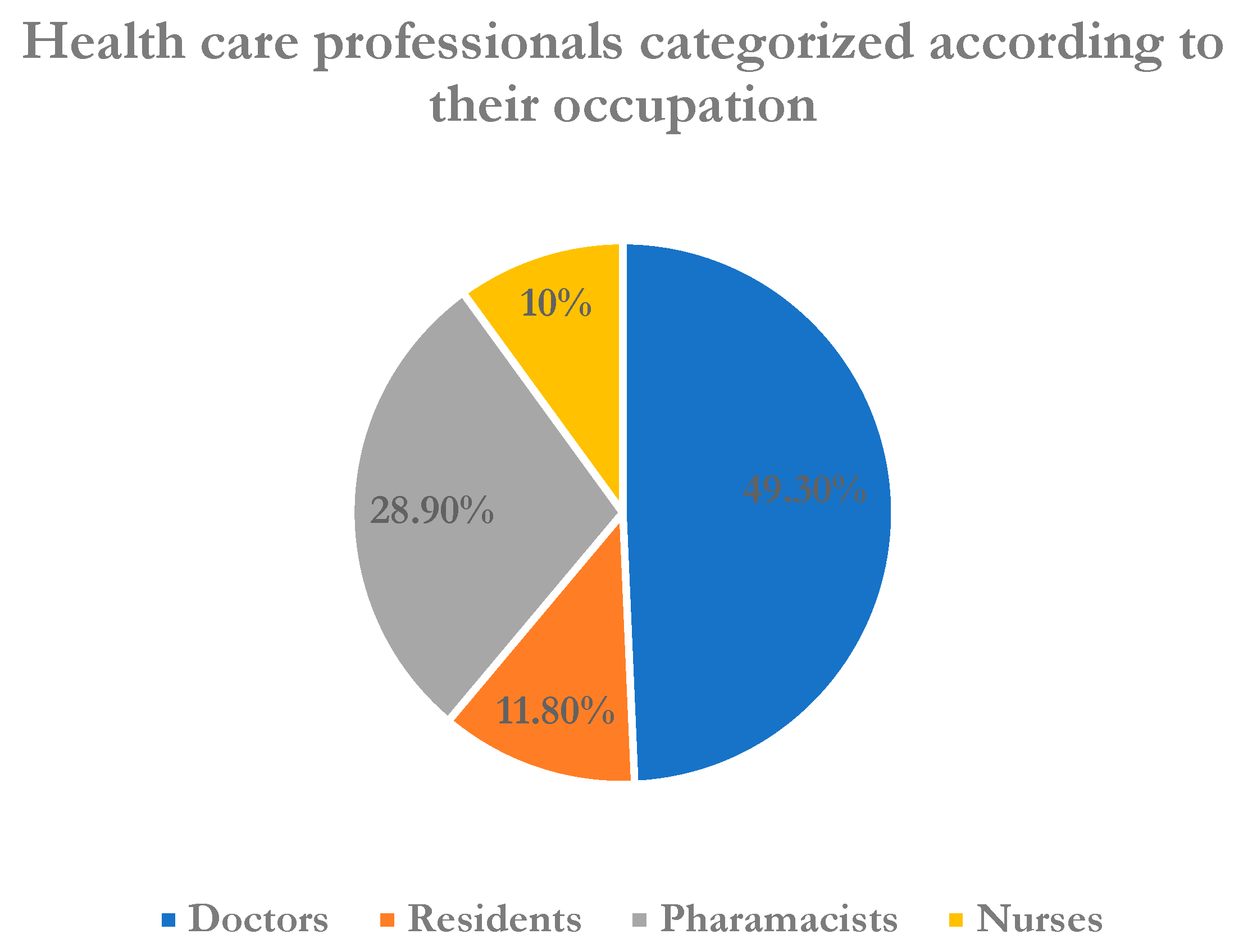
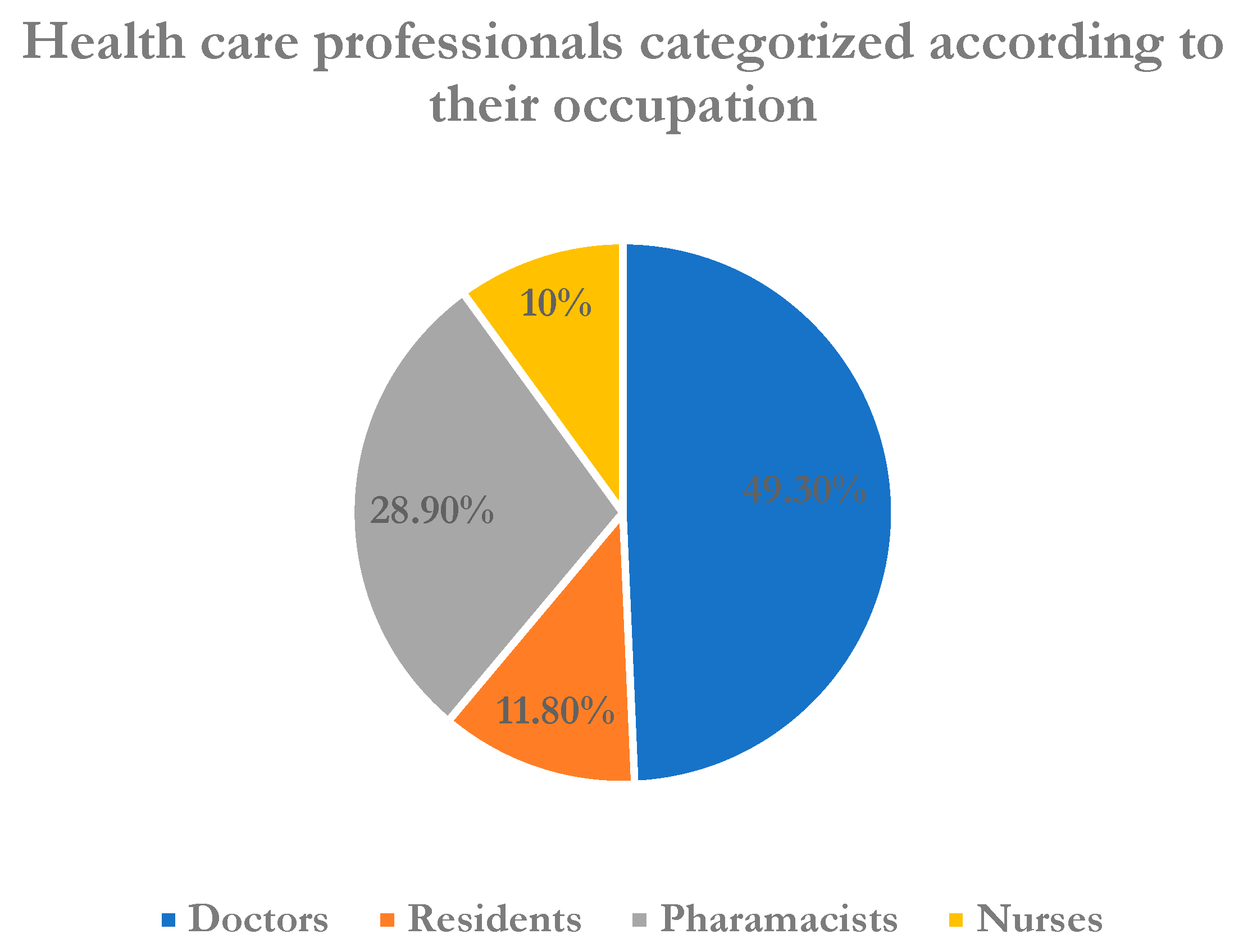
| Occupation | ||
| Doctors | 242 | 49.3 |
| Residents | 58 | 11.8 |
| Pharmacists | 142 | 28.9 |
| Nurses | 49 | 10 |
| Category of healthcare professionals | ||
| Frontline HCPs | 180 | 36.7 |
| Non-frontline HCPs | 311 | 63.1 |
| Experience | ||
| Less than 3 years | 371 | 75.6 |
| 3–6 years | 51 | 10.4 |
| 7–10 years | 21 | 4.3 |
| More than 10 years | 48 | 9.8 |
| Attended lectures/discussions about novel COVID-19 | ||
| Yes | 381 | 77.2 |
| No | 110 | 22.8 |
| Questions Related to Knowledge of COVID-19 | Correct Response | True n (%) | False n (%) | Chi Square Test (X2) |
|---|---|---|---|---|
| Coronavirus is a viral disease caused by a beta coronavirus thought to be originated from bats. | True | 407 (82.89) | 84 (17.1) | 0.059 |
| Incubation period for virus is 2–14 days. | True | 460 (93.68) | 31 (6.31) | 0.329 |
| Fever, dry cough, shortness of breath, and tiredness are hallmark symptoms of COVID-19. | True | 471 (95.9) | 20 (5.1) | 0.589 |
| Not all persons with COVID-19 will develop severe cases. Only those who are elderly having chronic illnesses are more likely to be severe cases. | True | 402 (81.8) | 89 (18.1) | 0.486 |
| Majority of COVID-19 infective patient will not develop severe illness but elderly, patient having chronic illness, DM, COPD are likely to develop severe illness. | True | 429 (87.37) | 62 (12.6) | 0.498 |
| Persons with COVID-19 cannot transmit to others if fever and dry cough is not present. | False | 138 (28.1) | 353 (71.89) | 0.432 |
| Polymerase chain reaction (PCR) can be used to diagnose COVID-19. | True | 406 (82.68) | 85 (17.31) | 0.048 * |
| Currently there is no treatment of COVID-19 infection, but early symptomatic and supportive treatment can help most patient recover from infection. | True | 460 (93.68) | 31 (6.3) | 0.385 |
| Supportive care and specific treatment for COVID-19 is available in Asir region. | True | 355 (72.3) | 136 (27.6) | 0.447 |
| Suspected COVID-19 patient should be sent to a quarantine center or home quarantine. | True | 445 (90.6) | 46 (9.4) | 0.168 |
| Wearing general medical masks can prevent one from acquiring infection by the COVID-19 virus. | True | 416 (84.73) | 75 (15.27) | 0.416 |
| It is not necessary for children and young adults to take measures to prevent the infection by the COVID-19 virus. | False | 146 (29.7) | 345 (70.3) | 0.288 |
| Questions Pertaining to Attitude | HCPs’ Responses N (%) | p-Value * | |||||||
|---|---|---|---|---|---|---|---|---|---|
| SA | A | N | D | SD | Age | Sex | Prof. | Exp. | |
| Transmission of COVID-19 infection can be prevented by using universal precautions given by the CDC, WHO, etc. a | 224 (45.6) | 190 (38.7) | 58 (11.8) | 12 (2.4) | 7 (1.4) | 0.655 | 0.902 | 0.148 | 0.443 |
| The prevalence of COVID-19 can be reduced by the active participation of healthcare professionals in the hospital infection control program. b | 196 (39.9) | 196 (39.9) | 78 (15.8) | 13 (2.6) | 7 (1.4) | 0.911 | 0.702 | 0.06 | 0.043 |
| Any related information about COVID-19 should be disseminated among peers and other healthcare professionals. c | 206 (41.9) | 177 (36) | 82 (16.7) | 14 (2.8) | 12 (2.4) | 0.870 | 0.770 | 0.045 | 0.294 |
| Intensive and emergency treatment should be given to diagnosed patients. d | 142 (28.9) | 152 (30.9) | 113 (23) | 58 (11.8) | 26 (5.2) | 0.549 | 0.116 | 0.257 | 0.995 |
| Do you think quarantine of suspected COVID-19 cases for 14 days can reduce the spread of the infection? e | 266 (54.1) | 137 (27.9) | 51 (10.3) | 29 (5.9) | 8 (1.6) | 0.350 | 0.855 | 0.334 | 0.437 |
| Level of fear of COVID-19 is very high. f | 135 (27.4) | 168 (34.2) | 139 (28.3) | 41 (8.3) | 8 (1.6) | 0.250 | 0.573 | 0.811 | 0.328 |
| Gowns, gloves, mask, and goggles must be used when dealing with COVID-19 patients. g | 352 (71.6) | 82 (16.7) | 40 (8.1) | 15 (3) | 2 (0.1) | 0.910 | 0.166 | 0.200 | 0.608 |
| Regulation taken by the government is enough to combat disease. h | 207 (42.1) | 151 (30.7) | 78 (15.8) | 42 (8.5) | 13 (2.6) | 0.593 | 0.382 | 0.012 | 0.006 |
| Characteristics | N | Knowledge Score (Mean ± S.D) | p Value | Attitude Score (Mean ± S.D) | p Value | Practice Score (Mean ± S.D) | p Value |
|---|---|---|---|---|---|---|---|
| Age | |||||||
| Less than 30 years | 396 | 9.15 ± 1.21 | 0.542 | 1.90 ± 0.45 | 0.544 | 2.09 ± 0.31 | 0.741 |
| 30–39 years | 69 | 9.22 ± 1.35 | 1.87 ± 0.44 | 2.02 ± 0.21 | |||
| 40–49 years | 19 | 8.94 ± 1.62 | 1.90 ± 0.18 | 2.18 ± 0.45 | |||
| More than 50 years | 7 | 9.57 ± 1.16 | 1.68 ± 0.34 | 1.89 ± 0.22 | |||
| Gender | |||||||
| Male | 273 | 9.22 ± 1.25 | 0.453 | 1.89 ± 0.12 | 0.892 | 2.06 ± 0.34 | 0.653 |
| Female | 218 | 9.05 ± 1.39 | 1.89 ± 0.19 | 2.10 ± 0.47 | |||
| Profession * | |||||||
| Doctors | 242 | 9.20 ± 1.16 | 0.044 | 1.85 ± 0.37 | 0.058 | 1.95 ± 0.19 | 0.052 |
| Residents | 58 | 9.05 ± 1.31 | 1.99 ± 0.25 | 2.02 ± 0.42 | |||
| Paramedics | 142 | 9.15 ± 1.26 | 2.13 ± 0.31 | 2.07 ± 0.41 | |||
| Nurses | 49 | 8.91 ±1.34 | 1.76 ± 0.41 | 1.83 ± 0.21 | |||
| Experience | |||||||
| Less than 3 years | 371 | 9.19 ± 1.23 | 0.064 | 1.88 ± 0.12 | 0.482 | 2.06 ± 0.23 | 0.851 |
| 3–6 years | 51 | 9.14 ± 1.44 | 1.98 ± 0.31 | 2.08 ± 0.44 | |||
| 7–10 years | 21 | 8.57 ± 1.37 | 1.99 ± 0.27 | 2.14 ± 0.32 | |||
| More than 10 years | 48 | 9.15 ± 1.21 | 1.89 ± 0.15 | 2.09 ± 0.21 | |||
| Category of respondents * | |||||||
| Frontline HCPs | 180 | 9.28 ± 1.19 | 0.054 * | 1.68 ± 0.12 | 0.045 * | 1.98 ± 0.14 | 0.051 |
| Non-frontline HCPs | 311 | 8.98 ± 1.26 | 1.99 ± 0.34 | 2.12 ± 0.17 |
| Questions Pertaining to Practice | HCPs’ Responses N (%) | p-Value * | |||||||
|---|---|---|---|---|---|---|---|---|---|
| SA | A | N | D | SD | Age | Sex | Prof. | Exp. | |
| Preventive measures against COVID-19 are adequately followed by healthcare professionals. 1 | 180 (36.6) | 197 (40.1) | 89 (18.1) | 20 (4) | 5 (1) | 0.503 | 0.264 | 0.177 | 0.166 |
| Do you think diagnostic centers are approachable and the results are accurate? 2 | 119 (24.2) | 206 (41.9) | 128 (26.1) | 32 (6.5) | 6 (1.2) | 0.888 | 0.720 | 0.464 | 0.718 |
| Do you think all the healthcare professionals follow all the five steps (WHO recommended) of the hand washing technique? 3 | 110 (22.4) | 170 (34.6) | 123 (25.6) | 70 (14.2) | 13 (2.6) | 0.286 | 0.462 | 0.017* | 0.481 |
| Attended training on hand hygiene, wearing and removing facemask during COVID-19 pandemic. 4 | 184 (37.5) | 163 (33.1) | 98 (19.9) | 33 (6.7) | 13 (2.6) | 0.582 | 0.052 | 0.152 | 0.067 |
| Attended training on performing nasopharyngeal swab safely. 5 | 128 (26.1) | 148 (30.1) | 113 (23) | 69 (14.1) | 33 (6) | 0.911 | 0.002* | 0.188 | 0.879 |
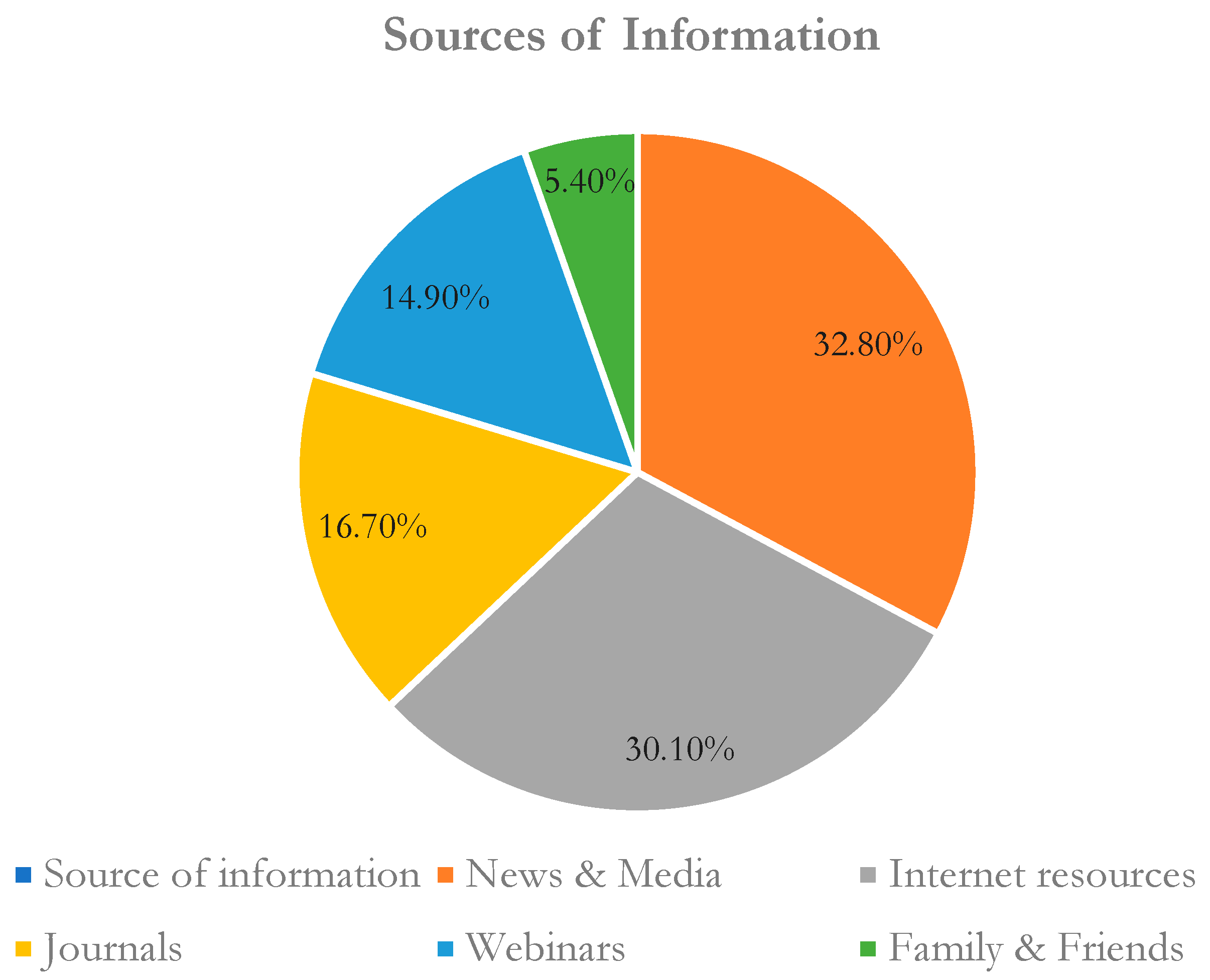
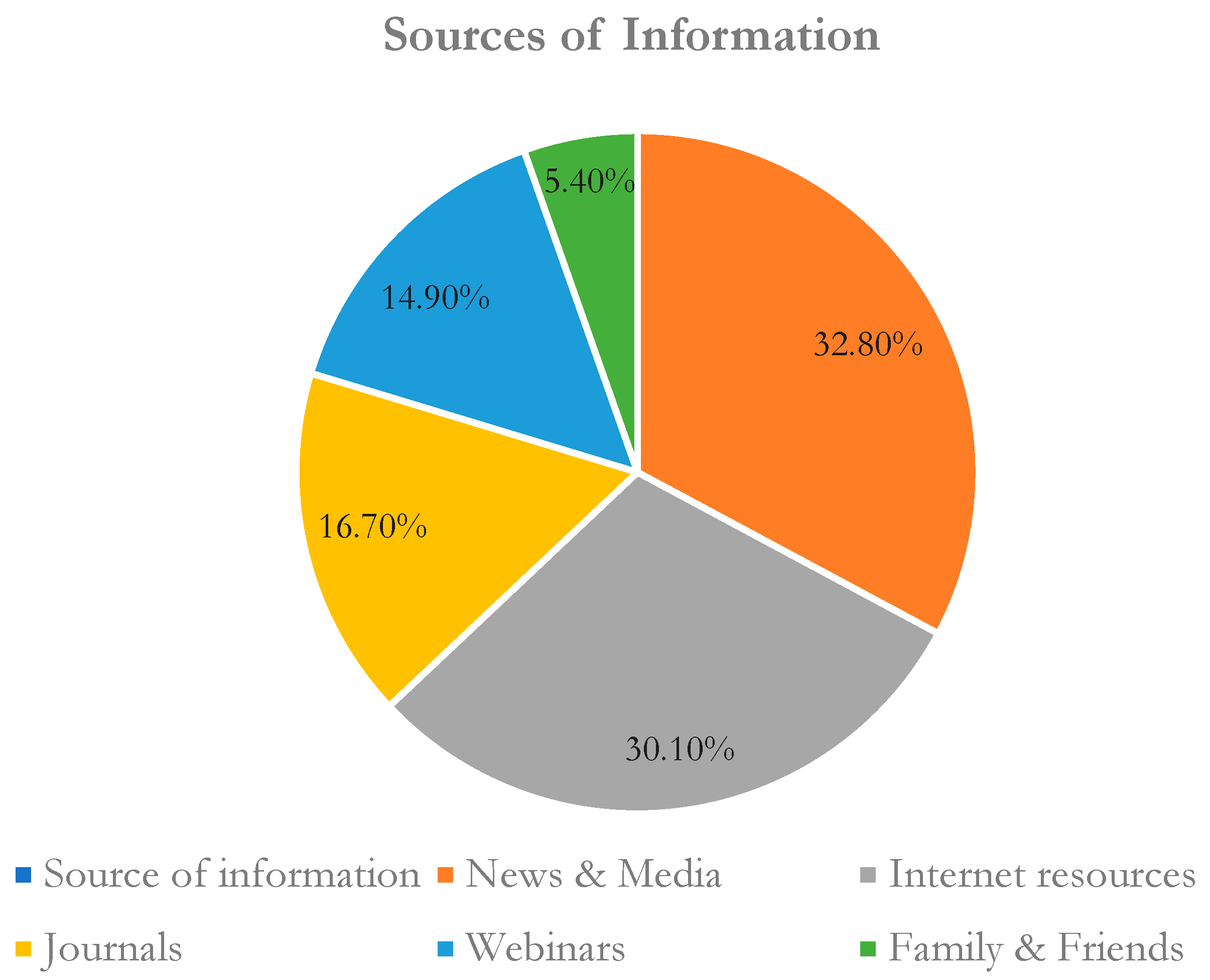
| Obtained knowledge about COVID-19 pandemic mainly from social websites of Saudi MOH, WHO, CDC. 6 | 206 (41.9) | 189 (38.5) | 69 (13.8) | 22 (4) | 5 (1) | 0.303 | 0.255 | 0.083 | 0.746 |
| During the outbreak, whether you maintained quarantine with family? 7 | 215 (43.8) | 144 (29.3) | 86 (17.5) | 39 (7.9) | 7 (1.4) | 0.976 | 0.384 | 0.102 | 0.925 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khobrani, M.; Vasudevan, R.; Kandasamy, G.; Gramish, J.A.; Prabahar, K.; Paulsamy, P. Evaluation of Health Care Professionals’ Knowledge, Attitudes, and Practice to Prevent the Pandemic Spread of COVID-19: A Questionnaire-Based Cross-Sectional Study from Abha, Saudi Arabia. Healthcare 2023, 11, 509. https://doi.org/10.3390/healthcare11040509
Khobrani M, Vasudevan R, Kandasamy G, Gramish JA, Prabahar K, Paulsamy P. Evaluation of Health Care Professionals’ Knowledge, Attitudes, and Practice to Prevent the Pandemic Spread of COVID-19: A Questionnaire-Based Cross-Sectional Study from Abha, Saudi Arabia. Healthcare. 2023; 11(4):509. https://doi.org/10.3390/healthcare11040509
Chicago/Turabian StyleKhobrani, Moteb, Rajalakshimi Vasudevan, Geetha Kandasamy, Jawaher A. Gramish, Kousalya Prabahar, and Premalatha Paulsamy. 2023. "Evaluation of Health Care Professionals’ Knowledge, Attitudes, and Practice to Prevent the Pandemic Spread of COVID-19: A Questionnaire-Based Cross-Sectional Study from Abha, Saudi Arabia" Healthcare 11, no. 4: 509. https://doi.org/10.3390/healthcare11040509
APA StyleKhobrani, M., Vasudevan, R., Kandasamy, G., Gramish, J. A., Prabahar, K., & Paulsamy, P. (2023). Evaluation of Health Care Professionals’ Knowledge, Attitudes, and Practice to Prevent the Pandemic Spread of COVID-19: A Questionnaire-Based Cross-Sectional Study from Abha, Saudi Arabia. Healthcare, 11(4), 509. https://doi.org/10.3390/healthcare11040509