
Exploring the Critical Driving Forces and Strategy Adoption Paths of Professional Competency Development for Various Emergency Physicians Based on the Hybrid MCDM Approach

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Establishing the Contents of Core Competencies for EPs
2.1.1. The Aspect of Professional Knowledge (PK)
2.1.2. The Aspect of Professional Skills (PS)
2.1.3. The Aspect of Professional Literacy (PL)
2.1.4. The Aspect of Care Services (CS)
2.2. DEMATEL
2.3. PCA (Principal Component Analysis)
2.4. Analytic Network Procedure (ANP)
2.5. VIKOR
3. Results
3.1. The Demographic Profile of the Valid Samples
3.2. The Network Relation Map (NRM)
3.3. The Comparative Analysis of Competency Development for Emergency Physicians
3.3.1. The Overall Views of Competency Development for Emergency Physicians
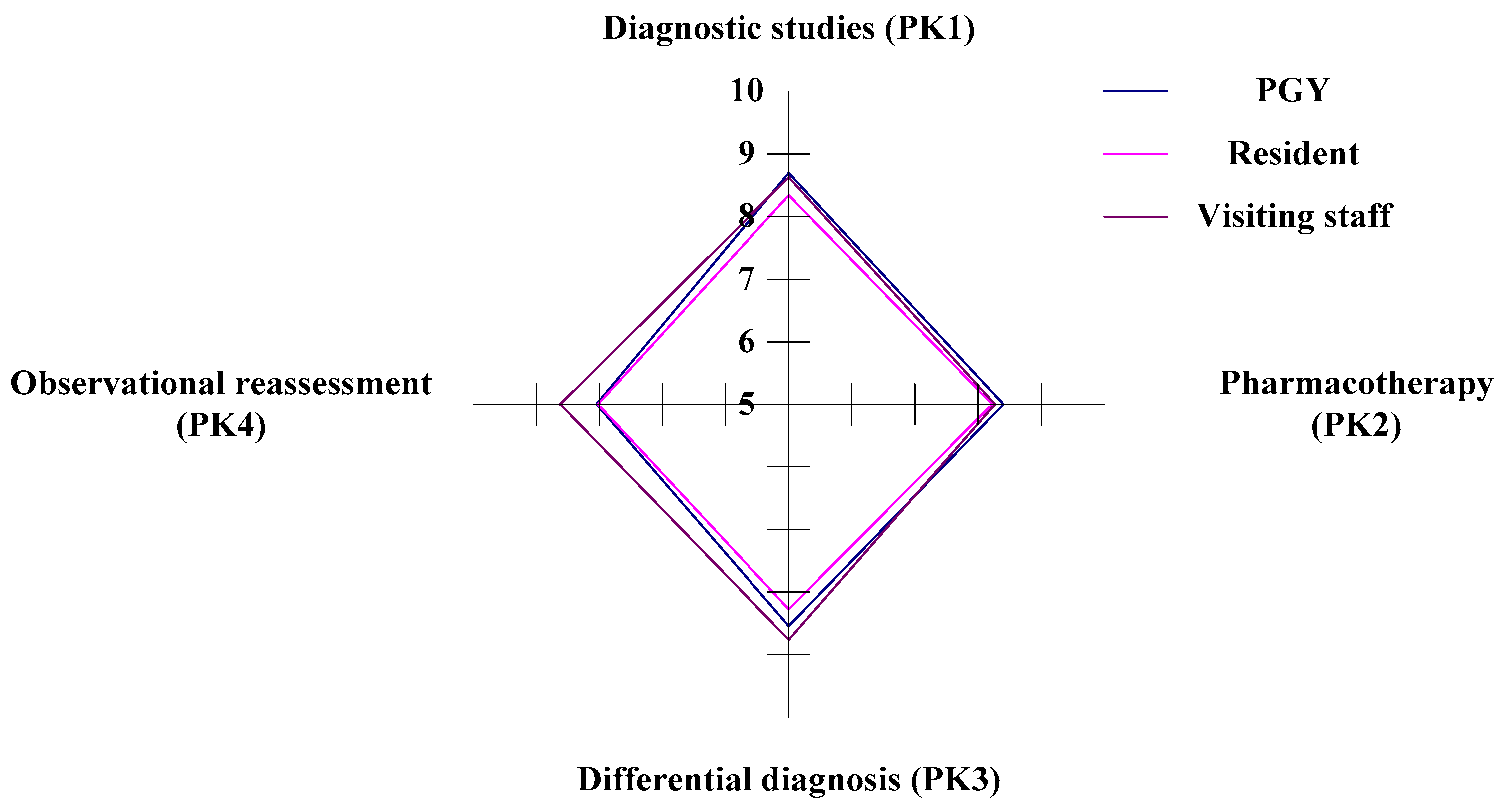
3.3.2. The PK (Professional Knowledge) Aspect of Competency Development for Emergency Physicians
3.3.3. The PS (Professional Skills) Aspect of Competency Development for Emergency Physicians
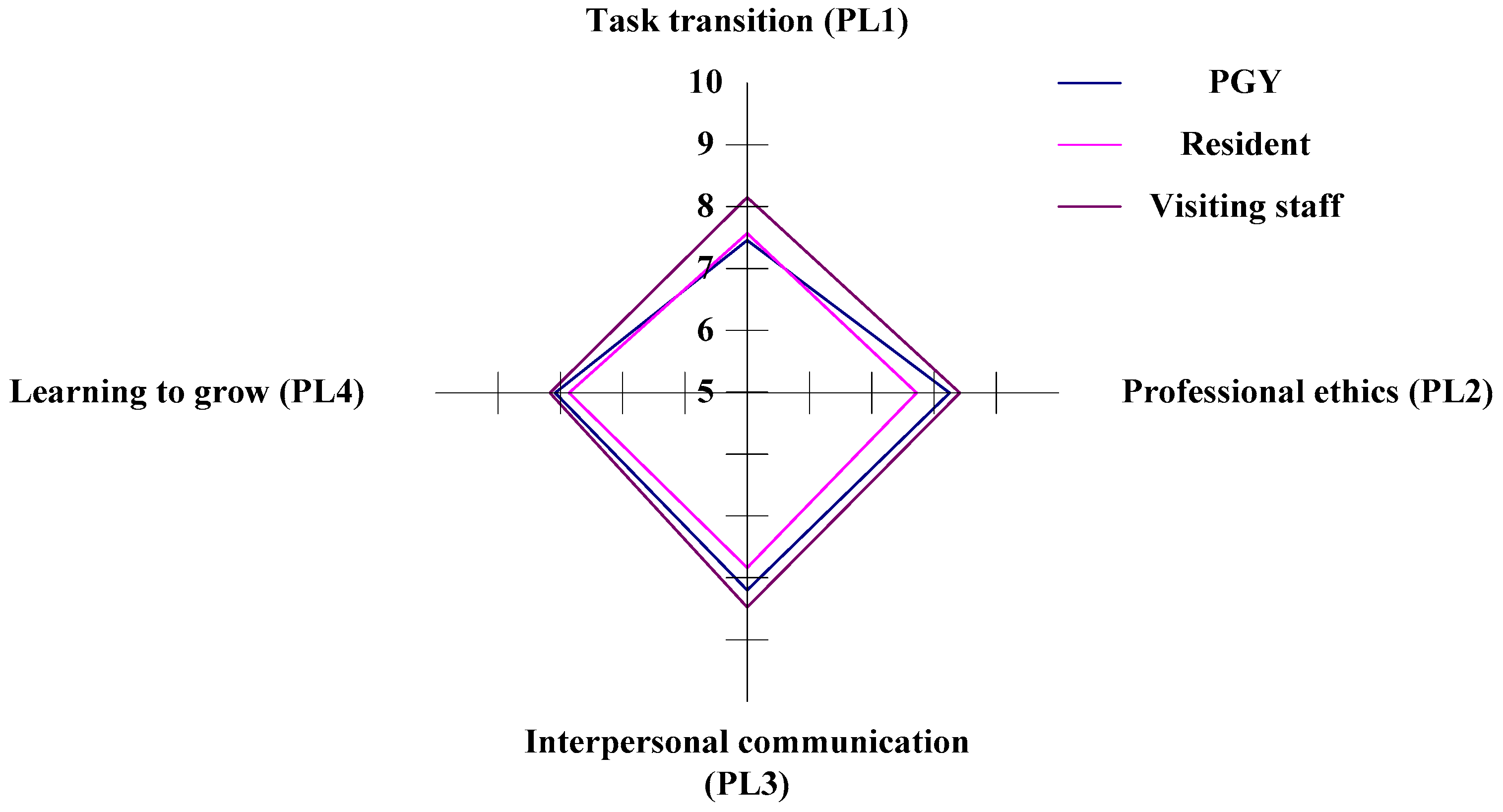
3.3.4. The PL (professional literacy) Aspect of Competency Development for Emergency Physicians
3.3.5. The CS (Care Services) Aspect of Competency Development for Emergency Physicians
3.4. PCA (Principal Component Analysis)
3.5. Analytic Network Procedure (ANP)
3.6. The Ranking of Professional Competency for Emergency Physicians under the VIKOR Approach
3.7. The Improving Paths Analysis for Different Stakeholders of Emergency Physicians
4. Discussion
4.1. Identifying the Gap in the Competency Development of EPs
4.2. Identifying Strategy Adoption Paths of the PGYs (Staff A)
4.3. Identifying Strategy Adoption Paths of the Residents (Staff B)
4.4. Identifying Strategy Adoption Paths of the Visiting Staff (Staff C)
4.5. Identifying Common Strategy Adoption Paths for the Three Stakeholders of EPs
4.6. Ranking of Professional Competency for Emergency Physicians Based on the VIKOR Approach
4.7. Comparing our Study with Previous Studies
5. Conclusions and Recommendations
5.1. Conclusions
5.2. Academic Contributions
5.3. Study Limitations
5.4. Future Studies
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CBME | competency-based medical education |
| CPD | continuing professional development |
| DEMATEL | decision-making trial and evaluation laboratory |
| PCA | principal component analysis |
| ANP | analytic network process |
| VIKOR | Vlse kriterijumska Optimizacija I Kompromisno Resenje |
| EPs | emergency physicians |
| PL | professional literacy |
| PS | professional skills |
| PK | personal knowledge |
| CS | care services |
| ACGME | Accreditation Council for Graduate Medical Education |
| ABMS | American Board of Medical Specialties |
| PCRS | The Physician Competency Reference Set |
| GME | graduate medical education |
| ABEM | The American Board of Emergency Medicine |
| KSABs | knowledge, skills, attitudes, and behaviors |
| PGYs | doctors in post-graduate years |
| NRM | network relation map |
| MCDM | multiple criteria decision making |
| PC | professional competency |
| ED | emergency department |
| POCUS | point-of-care ultrasound |
| IPC | inter-professional communication |
| SBP | systems-based practice |
| AI | artificial intelligence |
| CDI | competency development indicators |
References
- Carraccio, C.; Wolfsthal, S.D.; Englander, R.; Ferentz, K.; Martin, C. Shifting Paradigms. Acad. Med. 2002, 77, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.R.; Snell, L.S.; Cate, O.T.; Holmboe, E.S.; Carraccio, C.; Swing, S.R.; Harris, P.; Glasgow, N.; Campbell, C.; Dath, D.; et al. Competency-based medical education: Theory to practice. Med. Teach. 2010, 32, 638–645. [Google Scholar] [CrossRef] [PubMed]
- McGaghie, W.; Miller, G.E.; Sajid, A.W.; Telder, T.V. Competency-based curriculum development on medical education: An introduction. Public Health Pap. 1978, 68, 11–91. [Google Scholar]
- Frank, J.R.; Danoff, D. The CanMEDS initiative: Implementing an outcomes-based framework of physician competencies. Med. Teach. 2007, 29, 642–647. [Google Scholar] [CrossRef]
- Swing, S.R. The ACGME outcome project: Retrospective and prospective. Med. Teach. 2007, 29, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Englander, R.; Cameron, T.; Ballard, A.J.; Dodge, J.; Bull, J.; Aschenbrener, C.A. Toward a Common Taxonomy of Competency Domains for the Health Professions and Competencies for Physicians. Acad. Med. 2013, 88, 1088–1094. [Google Scholar] [CrossRef]
- Hart, D.; Franzen, D.; Beeson, M.; Bhat, R.; Kulkarni, M.; Thibodeau, L.; Weizberg, M.; Promes, S. Integration of Entrustable Professional Activities with the Milestones for Emergency Medicine Residents. WestJEM 21.2 March Issue 2018, 20, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-W.; Hsiao, C.-T.; Chou, F.C. Emergency Medicine Milestone Project for Residency Training in Taiwan. Yi Xue Jiao Yu 2017, 21, 73–80. [Google Scholar] [CrossRef]
- Beeson, M.S.; Carter, W.A.; Christopher, T.A.; Heidt, J.W.; Jones, J.H.; Meyer, L.E.; Promes, S.B.; Rodgers, K.G.; Shayne, P.H.; Swing, S.R.; et al. The Development of the Emergency Medicine Milestones. Acad. Emerg. Med. 2013, 20, 724–729. [Google Scholar] [CrossRef]
- Ni, B.; Gettler, E.; Stern, R.; Munro, H.M.; Steinwandel, M.; Aldrich, M.C.; Friedman, D.L.; Sanderson, M.; Schlundt, D.; Aronoff, D.M.; et al. Disruption of Medical Care among Individuals in the Southeastern United States during the COVID-19 Pandemic. J. Public Health Res. 2022, 11, 2497. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, M.; Routsi, E.; Tsamakis, K.; Fotis, L.; Marinos, G.; Lidoriki, I.; Karamanou, M.; Papaioannou, T.G.; Tsiptsios, D.; Smyrnis, N.; et al. Medical education challenges and innovations during COVID-19 pandemic. Postgrad. Med. J. 2021, 98, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; West, C.P.; Dyrbye, L.N.; Trockel, M.; Tutty, M.; Wang, H.; Carlasare, L.E.; Sinsky, C. Changes in Burnout and Satisfaction with Work-Life Integration in Physicians During the First 2 Years of the COVID-19 Pandemic. Mayo Clin. Proc. 2022, 97, 2248–2258. [Google Scholar] [CrossRef] [PubMed]
- Shreffler, J.; Petrey, J.; Huecker, M. The Impact of COVID-19 on Healthcare Worker Wellness: A Scoping Review. West J. Emerg. Med. 2020, 21, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.K.; Nousiainen, M.T.; Campisi, P.; Dagnone, J.D.; Frank, J.R.; Kroeker, K.I.; Brzezina, S.; Purdy, E.; Oswald, A. Training disrupted: Practical tips for supporting competency-based medical education during the COVID-19 pandemic. Med. Teach. 2020, 42, 756–761. [Google Scholar] [CrossRef]
- Stehman, C.; Hochman, S.; Fernández-Frackelton, M.; Volz, E.G.; Domingues, R.; Love, J.N.; Soares, W.B. Professionalism Milestones Assessments Used by Emergency Medicine Residency Programs: A Cross-sectional Survey. West. J. Emerg. Med. 2019, 21, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Shadid, A.M.; Bin Abdulrahman, A.K.; Bin Dahmash, A.; Aldayel, A.Y.; Alharbi, M.M.; AlGhamdi, A.; Al Asmri, A.; Qabha, H.M.; Al Madi, M.; Al Masri, M.; et al. SaudiMEDs and CanMEDS frameworks: Similarities and differences. Adv. Med. Educ. Pract. 2019, 10, 273–278. [Google Scholar] [CrossRef]
- Felzen, M.; Hirsch, F.; Brokmann, J.C.; Rossaint, R.; Beckers, S.K. Requirements and qualifications of emergency physicians in the prehospital telemedicine setting: Development of a competency-based model for qualification. Notf. Rett. 2018, 21, 590–597. [Google Scholar] [CrossRef]
- Stolz, L.A.; Stolz, U.; Fields, J.M.; Saul, T.; Secko, M.; Flannigan, M.J.; Sheele, J.M.; Rifenburg, R.P.; Weekes, A.J.; Josephson, E.B.; et al. Emergency Medicine Resident Assessment of the Emergency Ultrasound Milestones and Current Training Recommendations. Acad. Emerg. Med. 2017, 24, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Daouk-Öyry, L.; Mufarrij, A.; Khalil, M.; Sahakian, T.; Saliba, M.; Jabbour, R.; Hitti, E. Nurse-Led Competency Model for Emergency Physicians: A Qualitative Study. Ann. Emerg. Med. 2017, 70, 357–362. [Google Scholar] [CrossRef]
- Liu, Z.; Tian, L.; Chang, Q.; Sun, B.; Zhao, Y. A Competency Model for Clinical Physicians in China: A Cross-Sectional Survey. PLoS ONE 2016, 11, e0166252. [Google Scholar] [CrossRef] [PubMed]
- Stern, D.; Wojtczak, A.; Schwarz, M.R. The assessment of global minimum essential requirements in medical education. Med. Teach. 2003, 25, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, M.R.; Wojtczak, A. Global minimum essential requirements: A road towards competence-oriented medical education. Med. Teach. 2002, 24, 125–129. [Google Scholar] [CrossRef]
- Mockel, M.; Searle, J.; Muller, R.; Slagman, A.; Storchmann, H.; Oestereich, P.; Wyrwich, W.; Ale-Abaei, A.; Vollert, J.O.; Koch, M.; et al. Chief complaints in medical emergencies: Do they relate to underlying disease and outcome? Eur. J. Emerg. Med. 2013, 20, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Kemp, K.; Mertanen, R.; Lääperi, M.; Niemi-Murola, L.; Lehtonen, L.; Castren, M. Nonspecific complaints in the emergency department—A systematic review. Scand. J. Trauma, Resusc. Emerg. Med. 2020, 28, 6. [Google Scholar] [CrossRef]
- Kunz, T.; Meybohm, P. Drug interactions in emergency medicine. Anasthesiol. Intensivmed. Notf. Schmerzther. 2014, 49, 336–343. [Google Scholar] [CrossRef]
- DeWitt, S.; Chavez, S.A.; Perkins, J.; Long, B.; Koyfman, A. Evaluation of fever in the emergency department. Am. J. Emerg. Med. 2017, 35, 1755–1758. [Google Scholar] [CrossRef] [PubMed]
- Aml Yousif, E.; Aftab Mohammad, A. Resuscitation Procedures in Emergency Setting. In Essentials of Accident and Emergency Medicine; Ahmed Subhy, A., Ed.; IntechOpen: Rijeka, Croatia, 2018; Chapter 4. [Google Scholar] [CrossRef]
- Bell, E.; Fischer, M.A.; Sinatro, H. Procedural Competency in Academic Emergency Medicine Attending Physicians: How Is Competency Maintained and Evaluated by Academic Institutions in the US? Cureus 2021, 13, e16719. [Google Scholar] [CrossRef]
- Pelaccia, T.; Tardif, J.; Triby, E.; Charlin, B. A Novel Approach to Study Medical Decision Making in the Clinical Setting: The “Own-point-of-view” Perspective. Acad. Emerg. Med. 2017, 24, 785–795. [Google Scholar] [CrossRef]
- Steinkellner, C.; Schlömmer, C.; Dünser, M. Anamnese und klinische Untersuchung in der Notfall- und Intensivmedizin. Med. Klin. Intensiv. Notfallmedizin 2020, 115, 530–538. [Google Scholar] [CrossRef]
- Russell, F.M.; Kennedy, S.K.; Rood, L.K.; Nti, B.; Herbert, A.; Rutz, M.A.; Palmer, M.; Ferre, R.M. Design and implementation of a basic and global point of care ultrasound (POCUS) certification curriculum for emergency medicine faculty. Ultrasound J. 2022, 14, 10. [Google Scholar] [CrossRef]
- Ienghong, K.; Cheung, L.W.; Tiamkao, S.; Bhudhisawasdi, V.; Apiratwarakul, K. Integrating Point of Care Ultrasound Education into Clinical Practice at the Emergency Department. Tomography 2022, 8, 1052–1059. [Google Scholar] [CrossRef]
- Pirie, J.; Fayyaz, J.; Gharib, M.; Simone, L.; Glanfield, C.; Kempinska, A. Development and implementation of a novel, mandatory competency-based medical education simulation program for pediatric emergency medicine faculty. Adv. Simul. 2021, 6, 17. [Google Scholar] [CrossRef]
- Spruill, T.; Nazario, S.; Birenbaum, D.S. Interpersonal and communication skills and professionalism are the competencies most often noted in emergency medicine physicians judged as exemplary by their peers. J. Commun. Health 2020, 13, 27–34. [Google Scholar] [CrossRef]
- Fong, W.; Kwan, Y.H.; Yoon, S.; Phang, J.K.; Thumboo, J.; Leung, Y.Y.; Ng, S.C. Assessment of medical professionalism using the Professionalism Mini Evaluation Exercise (P-MEX) in a multi-ethnic society: A Delphi study. BMC Med. Educ. 2020, 20, 225. [Google Scholar] [CrossRef] [PubMed]
- Amirhajlou, L.; Bidari, A.; Alipour, F.; Yaseri, M.; Vaziri, S.; Rezai, M.; Tavakoli, N.; Farsi, D.; Yasinzadeh, M.R.; Mosaddegh, R.; et al. Validity, reliability and acceptability of Professionalism Mini-Evaluation Exercise (P-MEX) for emergency medicine residency training. J. Med. Ethic Hist. Med. 2019, 12, 12. [Google Scholar] [CrossRef]
- Li, H.; Ding, N.; Zhang, Y.; Liu, Y.; Wen, D. Assessing medical professionalism: A systematic review of instruments and their measurement properties. PLoS ONE 2017, 12, e0177321. [Google Scholar] [CrossRef] [PubMed]
- Alsabri, M.; Boudi, Z.; Lauque, D.M.; Dias, R.D.; Whelan, J.S.; Östlundh, L.M.; Alinier, G.; Onyeji, C.M.; Michel, P.M.; Liu, S.W.M.; et al. Impact of Teamwork and Communication Training Interventions on Safety Culture and Patient Safety in Emergency Departments: A Systematic Review. J. Patient Saf. 2020, 18, e351–e361. [Google Scholar] [CrossRef]
- Lyubovnikova, J.; West, M.; Dawson, J.F.; Carter, M. 24-Karat or fool’s gold? Consequences of real team and co-acting group membership in healthcare organizations. Eur. J. Work. Organ. Psychol. 2015, 24, 929–950. [Google Scholar] [CrossRef]
- Risser, D.T.; Rice, M.M.; Salisbury, M.L.; Simon, R.; Jay, G.D.; Berns, S.D. The Potential for Improved Teamwork to Reduce Medical Errors in the Emergency Department. Ann. Emerg. Med. 1999, 34, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Aouicha, W.; Tlili, M.A.; Sahli, J.; Ben Dhiab, M.; Chelbi, S.; Mtiraoui, A.; Latiri, H.S.; Ajmi, T.; Zedini, C.; Ben Rejeb, M.; et al. Exploring patient safety culture in emergency departments: A Tunisian perspective. Int. Emerg. Nurs. 2020, 54, 100941. [Google Scholar] [CrossRef]
- Salas, E.; DiazGranados, D.; Weaver, S.J.; King, H. Does Team Training Work? Principles for Health Care. Acad. Emerg. Med. 2008, 15, 1002–1009. [Google Scholar] [CrossRef]
- Gonzalo, J.D.M.; Wolpaw, D.R.; Cooney, R.; Mazotti, L.; Reilly, J.B.M.; Wolpaw, T.M. Evolving the Systems-Based Practice Competency in Graduate Medical Education to Meet Patient Needs in the 21st-Century Health Care System. Acad. Med. 2022, 97, 655–661. [Google Scholar] [CrossRef]
- Peterson, S.M.; Gurses, A.P.; Regan, L. Resident to Resident Handoffs in the Emergency Department: An Observational Study. J. Emerg. Med. 2014, 47, 573–579. [Google Scholar] [CrossRef]
- Kessler, C.; Scott, N.L.; Siedsma, M.; Jordan, J.; Beach, C.; Coletti, C.M. Interunit Handoffs of Patients and Transfers of Information: A Survey of Current Practices. Ann. Emerg. Med. 2014, 64, 343–349.e5. [Google Scholar] [CrossRef]
- Chen, E.H.; O’Sullivan, P.S.; Pfennig, C.L.; Leone, K.; Kessler, C.S. Assessing Systems-based Practice. Acad. Emerg. Med. 2012, 19, 1366–1371. [Google Scholar] [CrossRef]
- Terrell, K.M.; Miller, D.K. Strategies to Improve Care Transitions Between Nursing Homes and Emergency Departments. J. Am. Med. Dir. Assoc. 2010, 12, 602–605. [Google Scholar] [CrossRef] [PubMed]
- Vearrier, L.; Derse, A.R.; Basford, J.B.; Larkin, G.L.; Moskop, J.C. Artificial Intelligence in Emergency Medicine: Benefits, Risks, and Recommendations. J. Emerg. Med. 2022, 62, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Rider, A.C.; Kessler, C.S.; Schwarz, W.W.; Schmitz, G.R.; Oh, L.; Smith, M.D.; Gross, E.A.; House, H.; Wadman, M.C.; Lo, B.M. Transition of Care from the Emergency Department to the Outpatient Setting: A Mixed-Methods Analysis. West. J. Emerg. Med. 2018, 19, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Krittanawong, C. The rise of artificial intelligence and the uncertain future for physicians. Eur. J. Intern. Med. 2018, 48, e13–e14. [Google Scholar] [CrossRef]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.T.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef]
- Kilner, E.; Sheppard, L.A. The role of teamwork and communication in the emergency department: A systematic review. Int. Emerg. Nurs. 2010, 18, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.S.; Woods, R.; Bullard, M.; Holroyd, B.R.; Rowe, B.H. Consultations in the emergency department: A systematic review of the literature. Emerg. Med. J. 2008, 25, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Bashir, K.; Shah, Y. Using a Combination Approach in Imparting Effective Telephone Referral Skills to Emergency Medicine Residents in Qatar: A Pilot Study. Adv. Med. Educ. Pract. 2020, 11, 187–190. [Google Scholar] [CrossRef]
- Ong, Z.H.; Tan, L.H.E.; Ghazali, H.Z.B.; Ong, Y.T.; Koh, J.W.H.; Ang, R.Z.E.; Bok, C.; Chiam, M.; Lee, A.S.I.; Chin, A.M.C.; et al. A Systematic Scoping Review on Pedagogical Strategies of Interprofessional Communication for Physicians in Emergency Medicine. J. Med. Educ. Curric. Dev. 2021, 8, 23821205211041794. [Google Scholar] [CrossRef]
- Beeson, M.S.; Carter, W.A.; Christopher, T.A.; Heidt, J.W.; Jones, J.H.; Meyer, L.; Promes, S.B.; Rodgers, K.G.; Shayne, P.H.; Wagner, M.J.; et al. Emergency Medicine Milestones. J. Grad. Med. Educ. 2013, 5, 5–13. [Google Scholar] [CrossRef]
- Ling, L.J.; Beeson, M.S. Milestones in emergency medicine. J. Acute Med. 2012, 2, 65–69. [Google Scholar] [CrossRef]
- Lin, C.-L.; Tzeng, G.-H. A value-created system of science (technology) park by using DEMATEL. Expert Syst. Appl. 2009, 36, 9683–9697. [Google Scholar] [CrossRef]
- Tsai, W.-H.; Hsu, J.-L.; Chen, C.-H.; Lin, W.-R.; Chen, S.-P. An integrated approach for selecting corporate social responsibility programs and costs evaluation in the international tourist hotel. Int. J. Hosp. Manag. 2010, 29, 385–396. [Google Scholar] [CrossRef]
- Wang, W.-C.; Lin, Y.-H.; Lin, C.-L.; Chung, C.-H.; Lee, M.-T. DEMATEL-based model to improve the performance in a matrix organization. Expert Syst. Appl. 2012, 39, 4978–4986. [Google Scholar] [CrossRef]
- Bahadori, M.; Ravangard, R. Determining and Prioritizing the Organizational Determinants of Emergency Medical Services (EMS) in Iran. Iran. Red Crescent Med. J. 2013, 15, 307–311. [Google Scholar] [CrossRef]
- Wang, W.-C.; Lin, C.-L.; Wang, S.-H.; Liu, J.-J.; Lee, M.-T. Application of Importance-Satisfaction Analysis and Influence-Relations Map to Evaluate Design Delay Factors. J. Civ. Eng. Manag. 2014, 20, 497–510. [Google Scholar] [CrossRef]
- Ortíz, M.; Felizzola, H.; Isaza, S.N. A contrast between DEMATEL-ANP and ANP methods for six sigma project selection: A case study in healthcare industry. BMC Med. Inform. Decis. Mak. 2015, 15, S3. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-L. A novel hybrid decision-making model for determining product position under consideration of dependence and feedback. Appl. Math. Model. 2015, 39, 2194–2216. [Google Scholar] [CrossRef]
- Lin, C.-L.; Shih, Y.-H.; Tzeng, G.-H.; Yu, H.-C. A service selection model for digital music service platforms using a hybrid MCDM approach. Appl. Soft Comput. 2016, 48, 385–403. [Google Scholar] [CrossRef]
- Lin, C.-L.; Kuo, C.-L. A service position model of package tour services based on the hybrid MCDM approach. Curr. Issues Tour. 2019, 22, 2478–2510. [Google Scholar] [CrossRef]
- Lin, C.-L. The analysis of sustainable development strategies for industrial tourism based on IOA-NRM approach. J. Clean. Prod. 2019, 241, 118281. [Google Scholar] [CrossRef]
- Lin, C.-L.; Chang, K.-C. Establishing the service evaluation and selection system for emerging culture festival events using the hybrid MCDM technique. Curr. Issues Tour. 2020, 23, 2240–2272. [Google Scholar] [CrossRef]
- Lin, C.-L. Establishing environment sustentation strategies for urban and rural/town tourism based on a hybrid MCDM approach. Curr. Issues Tour. 2019, 23, 2360–2395. [Google Scholar] [CrossRef]
- Lin, C.-L. Evaluating the urban sustainable development strategies and common suited paths considering various stakeholders. Environ. Dev. Sustain. 2022, 24, 14033–14073. [Google Scholar] [CrossRef]
- Chuang, Y.-C.; Tung, T.-H.; Chen, J.-Y.; Chien, C.-W.; Shen, K.-Y. Exploration of the Relationship Among Key Risk Factors of Acute Kidney Injury for Elderly Patients Considering Covid-19. Front. Med. 2021, 8, 639250. [Google Scholar] [CrossRef]
- Xiong, L.; Sheng, G.; Fan, Z.-M.; Yang, H.; Hwang, F.-J.; Zhu, B.-W. Environmental Design Strategies to Decrease the Risk of Nosocomial Infection in Medical Buildings Using a Hybrid MCDM Model. J. Health Eng. 2021, 2021, 5534607. [Google Scholar] [CrossRef]
- Selerio, E.; Caladcad, J.A.; Catamco, M.R.; Capinpin, E.M.; Ocampo, L. Emergency preparedness during the COVID-19 pandemic: Modelling the roles of social media with fuzzy DEMATEL and analytic network process. Socioecon. Plan. Sci. 2022, 82, 101217. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.-F.; Wang, H.-T.; Chang, M.-W.; Cheng, T.-T.; Chen, J.-F.; Lin, C.-L.; Yu, H.-T. Determining the Development Strategy and Suited Adoption Paths for the Core Competence of Shared Decision-Making Tasks through the SAA-NRM Approach. Int. J. Environ. Res. Public Health 2022, 19, 13310. [Google Scholar] [CrossRef] [PubMed]
- Niemira, M.P.; Saaty, T.L. An Analytic Network Process model for financial-crisis forecasting. Int. J. Forecast. 2004, 20, 573–587. [Google Scholar] [CrossRef]
- Chang, C.-W.; Wu, C.-R.; Lin, C.-T.; Lin, H.-L. Evaluating digital video recorder systems using analytic hierarchy and analytic network processes. Inf. Sci. 2007, 177, 3383–3396. [Google Scholar] [CrossRef]
- Yang, J.L.; Chiu, H.N.; Tzeng, G.-H.; Yeh, R.H. Vendor selection by integrated fuzzy MCDM techniques with independent and interdependent relationships. Inf. Sci. 2008, 178, 4166–4183. [Google Scholar] [CrossRef]
- Yüksel, I.; Dagdeviren, M. Using the analytic network process (ANP) in a SWOT analysis—A case study for a textile firm. Inf. Sci. 2007, 177, 3364–3382. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Hsieh, H.-L.; Chen, H. Evaluating the Investment Projects of Spinal Medical Device Firms Using the Real Option and DANP-mV Based MCDM Methods. Int. J. Environ. Res. Public Health 2020, 17, 3335. [Google Scholar] [CrossRef]
- Shyur, H.-J. COTS evaluation using modified TOPSIS and ANP. Appl. Math. Comput. 2006, 177, 251–259. [Google Scholar] [CrossRef]
- Yu, R.; Tzeng, G.-H. A soft computing method for multi-criteria decision making with dependence and feedback. Appl. Math. Comput. 2006, 180, 63–75. [Google Scholar] [CrossRef]
- Shyur, H.-J.; Shih, H.-S. A hybrid MCDM model for strategic vendor selection. Math. Comput. Model. 2006, 44, 749–761. [Google Scholar] [CrossRef]
- Keramati, A.; Salehi, M. Website success comparison in the context of e-recruitment: An analytic network process (ANP) approach. Appl. Soft Comput. 2013, 13, 173–180. [Google Scholar] [CrossRef]
- Shih, H.-S.; Lee, E.S.; Chuang, S.-H.; Chen, C.-C. A forecasting decision on the sales volume of printers in Taiwan: An exploitation of the Analytic Network Process. Comput. Math. Appl. 2012, 64, 1545–1556. [Google Scholar] [CrossRef]
- Lin, C.-L.; Hsieh, M.-S.; Tzeng, G.-H. Evaluating vehicle telematics system by using a novel MCDM techniques with dependence and feedback. Expert Syst. Appl. 2010, 37, 6723–6736. [Google Scholar] [CrossRef]
- Chiu, W.-Y.; Tzeng, G.-H.; Li, H.-L. A new hybrid MCDM model combining DANP with VIKOR to improve e-store business. Knowl. Based Syst. 2012, 37, 48–61. [Google Scholar] [CrossRef]
- Wang, Y.-L.; Tzeng, G.-H. Brand marketing for creating brand value based on a MCDM model combining DEMATEL with ANP and VIKOR methods. Expert Syst. Appl. 2012, 39, 5600–5615. [Google Scholar] [CrossRef]
- Liu, H.-C.; Liu, L.; Liu, N.; Mao, L.-X. Risk evaluation in failure mode and effects analysis with extended VIKOR method under fuzzy environment. Expert Syst. Appl. 2012, 39, 12926–12934. [Google Scholar] [CrossRef]
- Liu, C.-H.; Tzeng, G.-H.; Lee, M.-H. Improving tourism policy implementation—The use of hybrid MCDM models. Tour. Manag. 2012, 33, 413–426. [Google Scholar] [CrossRef]
- Kuo, M.-S.; Liang, G.-S. A soft computing method of performance evaluation with MCDM based on interval-valued fuzzy numbers. Appl. Soft Comput. 2012, 12, 476–485. [Google Scholar] [CrossRef]
- Kudou, A.; Chen, Y.; Yeh, L. Comment on “Using a modified grey relation method for improving airline service quality”. Tour. Manag. 2012, 33, 717–718. [Google Scholar] [CrossRef]
- Tzeng, G.-H.; Lin, C.-W.; Opricovic, S. Multi-criteria analysis of alternative-fuel buses for public transportation. Energy Policy 2005, 33, 1373–1383. [Google Scholar] [CrossRef]
- Opricovic, S.; Tzeng, G.-H. Compromise solution by MCDM methods: A comparative analysis of VIKOR and TOPSIS. Eur. J. Oper. Res. 2004, 156, 445–455. [Google Scholar] [CrossRef]
- Ortiz-Barrios, M.; Gul, M.; Yucesan, M.; Alfaro-Sarmiento, I.; Navarro-Jiménez, E.; Jiménez-Delgado, G. A fuzzy hybrid decision-making framework for increasing the hospital disaster preparedness: The colombian case. Int. J. Disaster Risk Reduct. 2022, 72, 102831. [Google Scholar] [CrossRef] [PubMed]
- Alamroshan, F.; La’Li, M.; Yahyaei, M. The green-agile supplier selection problem for the medical devices: A hybrid fuzzy decision-making approach. Environ. Sci. Pollut. Res. 2022, 29, 6793–6811. [Google Scholar] [CrossRef]
- Yu, P.L. A Class of Solutions for Group Decision Problems. Manag. Sci. 1973, 19, 936–946. [Google Scholar] [CrossRef]
- Zeleny, M. Multiple Criteria Decision Making; McGraw-Hill: New York, NY, USA, 1982. [Google Scholar]
- Frank, J.R.; Mungroo, R.; Ahmad, Y.; Wang, M.; De Rossi, S.; Horsley, T. Toward a definition of competency-based education in medicine: A systematic review of published definitions. Med. Teach. 2010, 32, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, A. Oxford Dictionary of English; Oxford University Press: New York, NY, USA, 2010. [Google Scholar]
- Outcomes for Graduates. Available online: https://www.gmc-uk.org/-/media/documents/outcomes-for-graduates-2020_pdf-84622587.pdf?la=en&hash=35E569DEB208E71D666BA91CE58E5337CD569945 (accessed on 1 November 2020).
- Cooney, R.R.; Murano, T.; Ring, H.; Starr, R.; Beeson, M.S.; Edgar, L. The Emergency Medicine Milestones 2.0: Setting the stage for 2025 and beyond. AEM Educ. Train. 2021, 5, e10640. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Li, Z.; Wang, J.; Cao, E.; Zhuang, G.; Xiao, F.; Zheng, C.; Zhang, X.; Chen, M.; Gao, L.; et al. A KSA system for competency-based assessment of clinicians’ professional development in China and quality gap analysis. Med. Educ. Online 2022, 27, 2037401. [Google Scholar] [CrossRef]
- Alshyyab, M.A.; FitzGerald, G.; Albsoul, R.A.; Ting, J.; Kinnear, F.B.; Borkoles, E. Strategies and interventions for improving safety culture in Australian Emergency Departments: A modified Delphi study. Int. J. Health Plan. Manag. 2021, 36, 2392–2410. [Google Scholar] [CrossRef] [PubMed]
- McClelland, D.C. Testing for competence rather than for “intelligence”. Am. Psychol. 1973, 28, 1–14. [Google Scholar] [CrossRef]
- Arbuthnott, A.; Sharpe, D. The effect of physician–patient collaboration on patient adherence in non-psychiatric medicine. Patient Educ. Couns. 2009, 77, 60–67. [Google Scholar] [CrossRef]
- Del Canale, S.; Louis, D.Z.; Maio, V.; Wang, X.; Rossi, G.; Hojat, M.; Gonnella, J.S. The Relationship Between Physician Empathy and Disease Complications. Acad. Med. 2012, 87, 1243–1249. [Google Scholar] [CrossRef]
- Starmer, A.J.; Sectish, T.C.; Simon, D.W.; Keohane, C.; McSweeney, M.E.; Chung, E.Y.; Yoon, C.S.; Lipsitz, S.R.; Wassner, A.J.; Harper, M.B.; et al. Rates of Medical Errors and Preventable Adverse Events Among Hospitalized Children Following Implementation of a Resident Handoff Bundle. JAMA 2013, 310, 2262–2270. [Google Scholar] [CrossRef] [PubMed]
- Wadman, M.; Fago, B.; Hoffman, L.H.; Tran, T.P.; Muelleman, R.L. A comparison of emergency medicine resident clinical experience in a rural versus urban emergency department. Rural. Remote Health 2010, 10, 1442. [Google Scholar] [CrossRef]
- Kara, P.H.; Unluer, E.E.; Eser, U.; Colak, S.Z.; Kalaycı, O.T.; Demir, A.O. The Focused Assessment With Computerized Tomography for Trauma (FACT): Competancy of Emergency Physicians. Am. J. Emerg. Med. 2016, 34, 1721–1723. [Google Scholar] [CrossRef]
- Stoffman, J.M. Overcoming the barriers to implementation of competence-based medical education in post-graduate medical education: A narrative literature review. Med. Educ. Online 2022, 27, 2112012. [Google Scholar] [CrossRef] [PubMed]
- Cerasoli, C.P.; Nicklin, J.M.; Ford, M.T. Intrinsic motivation and extrinsic incentives jointly predict performance: A 40-year meta-analysis. Psychol. Bull. 2014, 140, 980–1008. [Google Scholar] [CrossRef]
- Malin, H.; Liauw, I.; Damon, W. Purpose and Character Development in Early Adolescence. J. Youth Adolesc. 2017, 46, 1200–1215. [Google Scholar] [CrossRef]
- Goldman, S. The SAGE Encyclopedia of Out-of-School Learning; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2017; Available online: https://sk.sagepub.com/reference/the-sage-encyclopedia-of-out-of-school-learning (accessed on 25 January 2023).
- Cooley, S.J.; Burns, V.; Cumming, J. Using Outdoor Adventure Education to Develop Students’ Groupwork Skills: A Quantitative Exploration of Reaction and Learning. J. Exp. Educ. 2016, 39, 329–354. [Google Scholar] [CrossRef]
- Grossman, R.; Salas, E. The transfer of training: What really matters. Int. J. Train. Dev. 2011, 15, 103–120. [Google Scholar] [CrossRef]
- Leach, S.; Immekus, J.C.; French, B.F.; Hand, B. The factorial validity of the Cornell Critical Thinking Tests: A multi-analytic approach. Think. Ski. Creat. 2020, 37, 100676. [Google Scholar] [CrossRef]
- Huang, X.; Lee, J.C.-K.; Dong, X. Mapping the factors influencing creative teaching in mainland China: An exploratory study. Think. Ski. Creat. 2018, 31, 79–90. [Google Scholar] [CrossRef]
- Anderson, R.C.; Graham, M. Creative potential in flux: The leading role of originality during early adolescent development. Think. Ski. Creat. 2021, 40, 100816. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Aspects/Criteria | Descriptions | References |
|---|---|---|
| Professional knowledge (PK) | ||
| Diagnostic studies (PK1) | Knowledge of diagnostic studies selection can help EPs improve their ability to diagnose and provide patient care. | [23,24] |
| Pharmacotherapy (PK2) | The development of pharmacotherapy knowledge can help EPs select appropriate agents for therapeutic intervention. | [19,25,26] |
| Differential diagnosis (PK3) | The development of differential diagnosis knowledge can help EPs prioritize the potential diagnosis based on the initial assessment. | [24,26] |
| Observational reassessment (PK4) | Developing knowledge of disposition decisions and patient education plans can improve patient safety and maximize resources. | [19,25,26] |
| Professional skills (PS) | ||
| Emergency stabilization (PS1) | The development of emergency stabilization can help EPs to identify unstable patients and perform immediate interventions to stabilize patients before deterioration. | [27,28] |
| Clinical assessment (PS2) | Performing a focused history and physical exam can help EPs to effectively guide the diagnosis and management of the patient’s urgent issues and minimize the need for further diagnostic testing. | [29,30] |
| Procedure management (PS3) | Performing and interpreting procedures (e.g., endotracheal intubation, suturing, splinting, and vascular access) can help EPs to optimize aggregate patient outcomes within the system. | [27,28] |
| Ultrasound use (PS4) | Performing goal-directed focused ultrasound exams can help EPs to manage patient assessment and invasive procedures promptly. | [31,32] |
| Professional literacy (PL) | ||
| Task transition (PL1) | The development of task transition can help EPs to manage available ED team members and resources efficiently under high volume or surge situations in the ED. | [33] |
| Professional ethics (PL2) | The development of professional ethics can ensure that EPs respect workplace ethical principles, demonstrate professional responsibilities, and optimize their personal and professional well-being. | [34,35,36,37] |
| Interpersonal communication (PL3) | Developing interpersonal communication strategies helps EPs mitigate stress, conflict, and miscommunication. | [28,29,30] |
| Performance improvement (PL4) | EPs apply evidence-based care to complex patients and commit to personal growth to facilitate individual and institutional improvement. | [33] |
| Care services (CS) | ||
| Teamwork (CS1) | The development of teamwork management can facilitate EPs to resolve specific ED challenges through effective communication and mutual respect among team members. | [38,39,40] |
| Patient safety (CS2) | EPs engage the emergency department and hospital system to offer error-prevention strategies and prevent patient safety events. | [38,41,42] |
| System management (CS3) | EPs should develop and apply strategies to evaluate and improve healthcare supply to provide optimal healthcare in the system. | [43,44,45,46,47] |
| Technology applications (CS4) | EPs use electronic devices to provide efficient and effective medical practice, the transition of care, computerized processes, and learning. | [48,49,50,51] |
| Characteristics | Number (%) | |
|---|---|---|
| Gender | Male | 85 (72.6) |
| Female | 32 (27.4) | |
| Age | 20~25 | 12 (10.3) |
| 26~30 | 59 (50.4) | |
| 31~35 | 10 (8.5) | |
| 36~40 | 9 (7.7) | |
| 41~45 | 9 (7.7) | |
| 46~50 | 13 (11.1) | |
| >51 | 5 (4.3) | |
| Workplace institution | Medical center | 90 (76.9) |
| Regional hospital | 27 (23.1) | |
| Stakeholders | PGYs | 44 (37.6) |
| Residents | 36 (30.8) | |
| Visiting staff | 37 (31.6) |
| Aspects | PGYs | Residents | Visiting Staff |
|---|---|---|---|
| (Staff A) | (Staff B) | (Staff C) | |
| Horizontal analysis | |||
| Professional knowledge (PK) | 8.426 [2] | 8.215 [3] | 8.568 [1] |
| Professional skills (PS) | 8.051 [3] | 8.299 [1] | 8.257 [2] |
| Professional literacy (PL) | 8.000 [2] | 7.750 [3] | 8.297 [1] |
| Care services (CS) | 7.955 [2] | 7.535 [3] | 8.014 [1] |
| Vertical analysis | |||
| Professional knowledge (PK) | 8.426 [1] | 8.215 [2] | 8.568 [1] |
| Professional skills (PS) | 8.051 [2] | 8.299 [1] | 8.257 [3] |
| Professional literacy (PL) | 8.000 [3] | 7.750 [3] | 8.297 [2] |
| Care services (CS) | 7.955 [4] | 7.535 [4] | 8.014 [4] |
| Staffs Criteria | PGYs | Residents | Visiting Staff |
|---|---|---|---|
| (Staff A) | (Staff B) | (Staff C) | |
| Horizontal analysis | |||
| Diagnostic studies (PK1) | 8.705 [1] | 8.333 [3] | 8.622 [2] |
| Pharmacotherapy (PK2) | 8.409 [1] | 8.222 [3] | 8.270 [2] |
| Differential diagnosis (PK3) | 8.545 [2] | 8.278 [3] | 8.757 [1] |
| Observational reassessment (PK4) | 8.045 [2] | 8.028 [3] | 8.622 [1] |
| Vertical analysis | |||
| Diagnostic studies (PK1) | 8.705 [1] | 8.333 [1] | 8.622 [2] |
| Pharmacotherapy (PK2) | 8.409 [3] | 8.222 [3] | 8.270 [4] |
| Differential diagnosis (PK3) | 8.545 [2] | 8.278 [2] | 8.757 [1] |
| Observational reassessment (PK4) | 8.045 [4] | 8.028 [4] | 8.622 [2] |
| Staffs Criteria | PGYs | Residents | Visiting Staff |
|---|---|---|---|
| (Staff A) | (Staff B) | (Staff C) | |
| Horizontal analysis | |||
| Emergency stabilization (PS1) | 8.136 [3] | 8.528 [2] | 8.838 [1] |
| Clinical assessment (PS2) | 8.750 [1] | 8.139 [3] | 8.622 [2] |
| Procedure management (PS3) | 7.818 [3] | 8.500 [1] | 8.297 [2] |
| Ultrasound use (PS4) | 7.500 [2] | 8.028 [1] | 7.270 [3] |
| Vertical analysis | |||
| Emergency stabilization (PS1) | 8.136 [2] | 8.528 [1] | 8.838 [1] |
| Clinical assessment (PS2) | 8.750 [1] | 8.139 [3] | 8.622 [2] |
| Procedure management (PS3) | 7.818 [3] | 8.500 [2] | 8.297 [3] |
| Ultrasound use (PS4) | 7.500 [4] | 8.028 [4] | 7.270 [4] |
| Staffs Criteria | PGYs | Residents | Visiting Staff |
|---|---|---|---|
| (Staff A) | (Staff B) | (Staff C) | |
| Horizontal analysis | |||
| Task transition (PL1) | 7.477 [3] | 7.583 [2] | 8.162 [1] |
| Professional ethics (PL2) | 8.250 [2] | 7.722 [3] | 8.405 [1] |
| Interpersonal communication (PL3) | 8.182 [2] | 7.833 [3] | 8.459 [1] |
| Performance improvement (PL4) | 8.091 [2] | 7.861 [3] | 8.162 [1] |
| Vertical analysis | |||
| Task transition (PL1) | 7.477 [4] | 7.583 [4] | 8.162 [3] |
| Professional ethics (PL2) | 8.250 [1] | 7.722 [3] | 8.405 [2] |
| Interpersonal communication (PL3) | 8.182 [2] | 7.833 [2] | 8.459 [1] |
| Performance improvement (PL4) | 8.091 [3] | 7.861 [1] | 8.162 [3] |
| Staffs Criteria | PGYs | Resident | Visiting Staff |
|---|---|---|---|
| (Staff A) | (Staff B) | (Staff C) | |
| Horizontal analysis | |||
| Teamwork (CS1) | 8.045 [2] | 7.722 [3] | 8.324 [1] |
| Patient safety (CS2) | 8.455 [1] | 7.889 [3] | 8.351 [2] |
| System management (CS3) | 7.932 [1] | 7.361 [3] | 7.784 [2] |
| Technology applications (CS4) | 7.386 [2] | 7.167 [3] | 7.595 [1] |
| Vertical analysis | |||
| Teamwork (CS1) | 8.045 [2] | 7.722 [2] | 8.324 [2] |
| Patient safety (CS2) | 8.455 [1] | 7.889 [1] | 8.351 [1] |
| System management (CS3) | 7.932 [3] | 7.361 [3] | 7.784 [3] |
| Technology applications (CS4) | 7.386 [4] | 7.167 [4] | 7.595 [4] |
| Components | ||||
|---|---|---|---|---|
| Aspects | Components | Criteria | 1 | Community |
| Professional knowledge (PK) | Diagnostic and therapeutic knowledge (PKP1) | Diagnostic studies (PK1) | 0.915 | 0.838 |
| Pharmacotherapy (PK2) | 0.911 | 0.830 | ||
| Differential diagnosis (PK3) | 0.897 | 0.805 | ||
| Observational reassessment (PK4) | 0.852 | 0.726 | ||
| Eigenvalue λ | 3.200 | |||
| % of Variance | 79.993 | |||
| Cumulative (%) | 79.993 | |||
| Cronbach’s α | 0.916 | |||
| Professional skills (PS) | Stabilization and procedural skills (PSP1) | Emergency stabilization (PS1) | 0.874 | 0.764 |
| Procedure management (PS3) | 0.847 | 0.717 | ||
| Ultrasound use (PS4) | 0.820 | 0.673 | ||
| Clinic assessment (PS2) | 0.739 | 0.547 | ||
| Eigenvalue λ | 2.700 | |||
| % of Variance | 67.506 | |||
| Cumulative (%) | 67.506 | |||
| Cronbach’s α | 0.838 | |||
| Professional literacy (PL) | Professionalism and interpersonal communication (PLP1) | Professional ethics (PL2) | 0.909 | 0.826 |
| Interpersonal communication (PL3) | 0.897 | 0.805 | ||
| Task transition (PL1) | 0.888 | 0.788 | ||
| Performance improvement (PL4) | 0.875 | 0.765 | ||
| Eigenvalue λ | 3.184 | |||
| % of Variance | 79.599 | |||
| Cumulative (%) | 79.599 | |||
| Cronbach’s α | 0.914 | |||
| Care services (CS) | System management & teamwork (CSP1) | System management (CS3) | 0.939 | 0.881 |
| Teamwork (CS1) | 0.927 | 0.859 | ||
| Patient safety (CS2) | 0.846 | 0.716 | ||
| Technology applications (CS4) | 0.840 | 0.706 | ||
| Eigenvalue λ | 3.162 | |||
| % of Variance | 79.038 | |||
| Cumulative (%) | 79.038 | |||
| Cronbach’s α | 0.911 |
| Aspects | Components | Component Weights |
|---|---|---|
| Professional knowledge (PK) | Diagnostic studies & Pharmacotherapy (PKP1) | 0.257 |
| Professional skills (PS) | Emergency stabilization & Management (PSP1) | 0.259 |
| Professional literacy (PL) | Professional ethics & communication (PLP1) | 0.238 |
| Care services (CS) | Care management & Teamwork (CSP1) | 0.246 |
| Total | 1.000 |
| PGYs | Residents | Visiting Staff | ||
|---|---|---|---|---|
| (Staff A) | (Staff B) | (Staff C) | ||
| v = 0.0 | Rvk | 0.205 | 0.247 | 0.199 |
| CDI | 0.795 | 0.753 | 0.801 | |
| Rank | 2 | 3 | 1 | |
| v = 0.5 | Rvk | 0.197 | 0.225 | 0.185 |
| CDI | 0.803 | 0.775 | 0.815 | |
| Rank | 2 | 3 | 1 | |
| v = 1.0 | Rvk | 0.189 | 0.204 | 0.171 |
| CDI | 0.811 | 0.796 | 0.829 | |
| Rank | 2 | 3 | 1 | |
| Advantage and Disadvantageous Aspects/Components | Strategy Adoption Paths (SAPs) | |
|---|---|---|
| PGYs (Staff A) | Professional knowledge (PK) > Professional skills (PS) > Professional literacy (PL) > Care services (CS) | 1. PL(3)→PS(2) {N} 2. PL(3)→PK(1)→PS(2) {Y} 3. PL(3)→CS(4)→PS(2) {Y} 4. PL(3)→CS(4)→PK(1)→PS(2) {Y} |
| Residents (Staff B) | Professional skills (PS) > Professional knowledge (PK) > Professional literacy (PL) > Care services (CS) | 1. PL(3)→PS(1) {N} 2. PL(3)→PK(2)→PS(1) {N} 3. PL(3)→CS(4)→PS(1) {Y} 4. PL(3)→CS(4)→PK(2)→PS(1) {Y} |
| Visiting staff (Staff C) | Professional knowledge (PK) > Professional literacy (PL) > Professional skills (PS) > Care services (CS) | 1. PL(2)→PS(3) {Y} 2. PL(2)→PK(1)→PS(3) {Y} 3. PL(2)→CS(4)→PS(3) {Y} 4. PL(2)→CS(4)→PK(1)→PS(3) {Y} |
| Common strategy adoption paths (Common SAPs) | 3. PL→CS→PS 4. PL→CS→PK→PS | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, M.-W.; Kung, C.-T.; Yu, S.-F.; Wang, H.-T.; Lin, C.-L. Exploring the Critical Driving Forces and Strategy Adoption Paths of Professional Competency Development for Various Emergency Physicians Based on the Hybrid MCDM Approach. Healthcare 2023, 11, 471. https://doi.org/10.3390/healthcare11040471
Chang M-W, Kung C-T, Yu S-F, Wang H-T, Lin C-L. Exploring the Critical Driving Forces and Strategy Adoption Paths of Professional Competency Development for Various Emergency Physicians Based on the Hybrid MCDM Approach. Healthcare. 2023; 11(4):471. https://doi.org/10.3390/healthcare11040471
Chicago/Turabian StyleChang, Meng-Wei, Chia-Te Kung, Shan-Fu Yu, Hui-Ting Wang, and Chia-Li Lin. 2023. "Exploring the Critical Driving Forces and Strategy Adoption Paths of Professional Competency Development for Various Emergency Physicians Based on the Hybrid MCDM Approach" Healthcare 11, no. 4: 471. https://doi.org/10.3390/healthcare11040471
APA StyleChang, M.-W., Kung, C.-T., Yu, S.-F., Wang, H.-T., & Lin, C.-L. (2023). Exploring the Critical Driving Forces and Strategy Adoption Paths of Professional Competency Development for Various Emergency Physicians Based on the Hybrid MCDM Approach. Healthcare, 11(4), 471. https://doi.org/10.3390/healthcare11040471