
The Effect of a Nurse-Led Family Involvement Program on Anxiety and Depression in Patients with Advanced-Stage Hepatocellular Carcinoma

Abstract
1. Introduction
Conceptual Framework and Literature Review
2. Materials and Methods
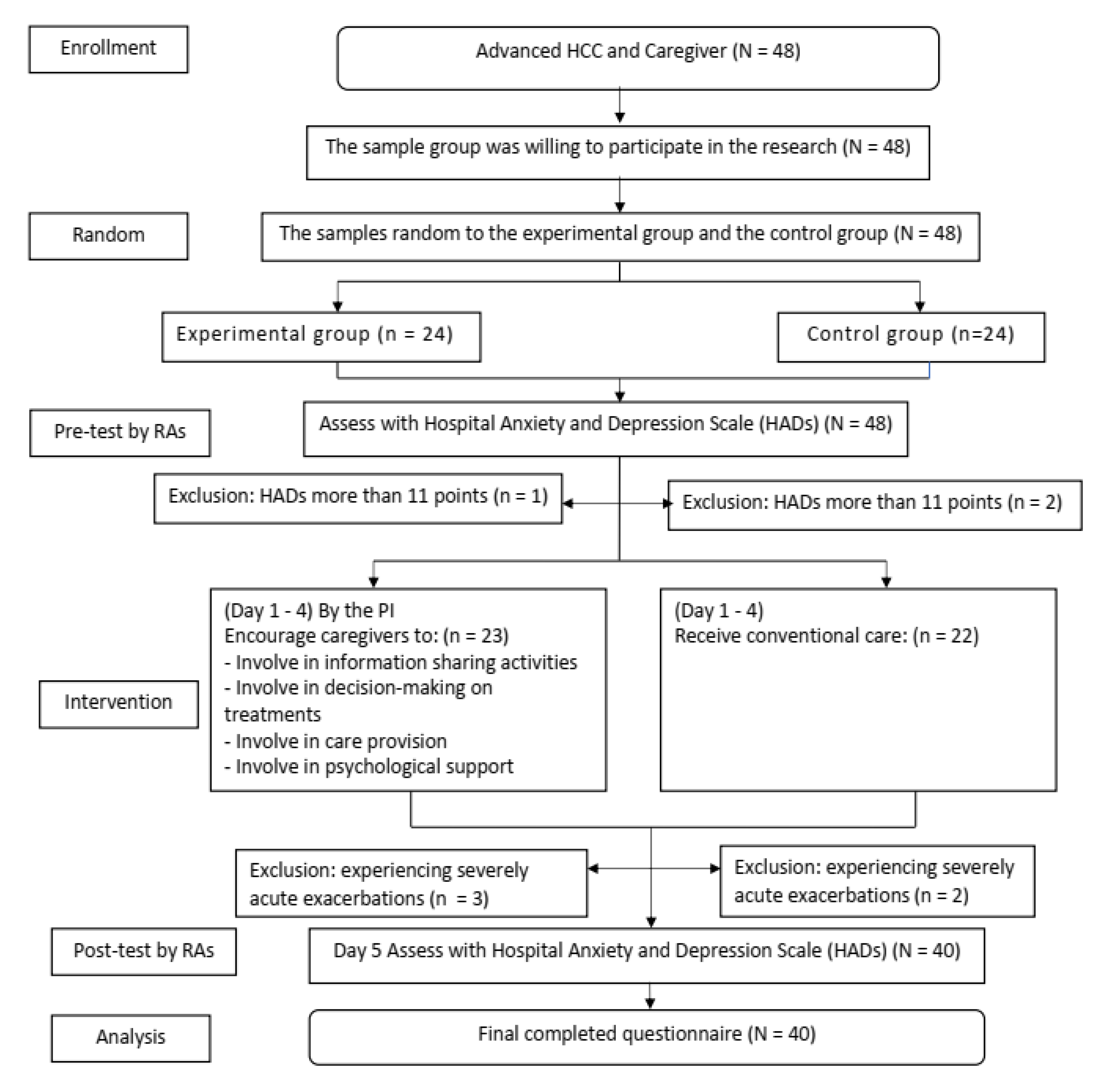
2.1. Design
2.2. Participants
2.3. Interventions
2.4. Instruments
2.5. Ethical Considerations
2.6. Data Collection and Intervention
2.7. Data Analysis
3. Results
4. Discussion
5. Limitation of the Study
6. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Laube, R.; Sabih, A.H.; Strasser, S.I.; Lim, L.; Cigolini, M.; Liu, K. Palliative care in hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2021, 36, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Huang, S.S.; Li, I.F.; Lin, K.P.; Tsay, S.L. Prognostic association of demographic and clinical factors with the change rates of symptoms and depression among patients with hepatocellular carcinoma. Support Care Cancer 2019, 27, 4665–4674. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Panda, D. Role of supportive care for terminal stage hepatocellular carcinoma. J. Clin. Exp. Hepatol. 2014, 4 (Suppl. S3), S130–S139. [Google Scholar] [CrossRef] [PubMed]
- Ayman, A.; Azza, A.; Kamel, Y.; Rasul, K.; Jonas, F.; Mohammed, A.; Zeinab, M. The role of palliative care in the management of patients with advanced hepatocellular carcinoma: A single institution experience. J. Patient Care 2017, 2, 1000112. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Knifton, L.; Robb, K.A.; Katikireddi, S.V.; Smith, D.J. Depression and anxiety among people living with and beyond cancer: A growing clinical and research priority. BMC Cancer 2019, 19, 943. [Google Scholar] [CrossRef] [PubMed]
- Graf, J.; Stengel, A. Psychological burden and psycho-oncological interventions for patients with hepatobiliary cancers–a systematic review. Front Psychol. 2021, 12, 662777. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Chen, S.J.; Liu, C.Y. Risk of developing depressive disorders following hepatocellular carcinoma: A nationwide population-based study. PLoS ONE 2015, 10, e0135417. [Google Scholar] [CrossRef]
- Riedl, D.; Schüßler, G. Factors associated with and risk factors for depression in cancer patients - a systematic literature review. Transl Oncol. 2022, 16, 101328. [Google Scholar] [CrossRef]
- Hart, N.H.; Crawford-Williams, F.; Crichton, M.; Yee, J.; Smith, T.J.; Koczwara, B.; Fitch, M.I.; Crawford, G.B.; Mukhopadhyay, S.; Mahony, J.; et al. Unmet supportive care needs of people with advanced cancer and their caregivers: A systematic scoping review. Crit. Rev. Oncol. Hematol. 2022, 176, 103728. [Google Scholar] [CrossRef]
- Wang, T.; Molassiotis, A.; Chung, B.P.M.; Tan, J.Y. Unmet care needs of advanced cancer patients and their informal caregivers: A systematic review. BMC Palliat Care 2018, 17, 96. [Google Scholar] [CrossRef]
- National Cancer Institute. Hospital-Based Cancer Registry; 2021. Available online: https://www.nci.go.th/e_book/hosbased_2564/index.html (accessed on 5 December 2022).
- Somboon, K.; Siramolpiwat, S.; Vilaichone, R.K. Epidemiology and survival of hepatocellular carcinoma in the central region of Thailand. Asian Pac. J. Cancer Prev. 2014, 15, 3567–3570. [Google Scholar] [CrossRef] [PubMed]
- Temtap, S.; Nilmanat, K. The relationship between psychological distress and coping strategies in patients with advanced or terminal stage hepatocellular carcinoma: A cross-sectional descriptive study. Songklanagarind Med. J. 2017, 35, 313. [Google Scholar] [CrossRef]
- Weis, J. Psychosocial Care for Cancer Patients. Breast Care (Basel) 2015, 10, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yan, C.; Fu, A. A randomized clinical trial of comprehensive education and care program compared to basic care for reducing anxiety and depression and improving quality of life and survival in patients with hepatocellular carcinoma who underwent surgery. Medicine (Baltimore) 2019, 98, e17552. [Google Scholar] [CrossRef]
- Aprilianto, E.; Lumadi, S.A.; Handian, F.I. Family social support and the self-esteem of breast cancer patients undergoing neoadjuvant chemotherapy. J. Public Health Res. 2021, 10, jphr-2021. [Google Scholar] [CrossRef]
- Moghaddam Tabrizi, F.; Alizadeh, S. Family intervention based on the FOCUS program effects on cancer coping in Iranian breast cancer patients: A Randomized Control Trial. Asian Pac. J. Cancer. Prev. 2018, 19, 1523–1528. [Google Scholar] [CrossRef]
- Sari, D.K.; Dewi, R.; Daulay, W. Association between family support, coping strategies and anxiety in cancer patients undergoing chemotherapy at general hospital in Medan, North Sumatera, Indonesia. Asian Pac. J. Cancer Prev. 2019, 20, 3015–3019. [Google Scholar] [CrossRef]
- Hopkinson, J.B.; Brown, J.C.; Okamoto, I.; Addington-Hall, J.M. The effectiveness of patient-family carer (couple) intervention for the management of symptoms and other health-related problems in people affected by cancer: A systematic literature search and narrative review. J. Pain Symptom Manage 2012, 43, 111–142. [Google Scholar] [CrossRef]
- Gwaza, E.; Msiska, G. Family involvement in caring for inpatients in acute care hospital settings: A systematic review of literature. SAGE Open Nurs. 2022, 8, 23779608221089541. [Google Scholar] [CrossRef]
- Dijkman, B.L.; Luttik, M.L.; Van der Wal-Huisman, H.; Paans, W.; van Leeuwen, B.L. Factors influencing family involvement in treatment decision-making for older patients with cancer: A scoping review. J. Geriatr. Oncol. 2022, 13, 391–397. [Google Scholar] [CrossRef]
- Chien, C.H.; Liu, K.L.; Chien, H.T.; Liu, H.E. The effects of psychosocial strategies on anxiety and depression of patients diagnosed with prostate cancer: A systematic review. Int. J. Nurs. Stud. 2014, 51, 28–38. [Google Scholar] [CrossRef]
- Newby, T.A.; Graff, J.N.; Ganzini, L.K.; McDonagh, M.S. Interventions that may reduce depressive symptoms among prostate cancer patients: A systematic review and meta-analysis. Psychooncology 2015, 24, 1686–1693. [Google Scholar] [CrossRef]
- Guarino, A.; Polini, C.; Forte, G.; Favieri, F.; Boncompagni, I.; Casagrande, M. The effectiveness of psychological treatments in women with breast cancer: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 209. [Google Scholar] [CrossRef]
- Xiao, F.; Song, X.; Chen, Q.; Dai, Y.; Xu, R.; Qiu, C.; Guo, Q. Effectiveness of psychological interventions on depression in patients after breast cancer surgery: A meta-analysis of randomized controlled trials. Clin. Breast Cancer 2017, 17, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Kamaryati, N.P.; Malathum, P. Family support: A concept analysis. PRIJNR 2020, 24, 403–411. [Google Scholar]
- Coyne, E.; Heynsbergh, N.; Dieperink, K.B. Acknowledging cancer as a family disease: A systematic review of family care in the cancer setting. Eur. J. Oncol. Nurs. 2020, 49, 101841. [Google Scholar] [CrossRef] [PubMed]
- Laidsaar-Powell, R.; Butow, P.; Boyle, F.; Juraskova, I. Facilitating collaborative and effective family involvement in the cancer setting: Guidelines for clinicians (TRIO Guidelines-1). Patient Educ. Couns. 2018, 101, 970–982. [Google Scholar] [CrossRef]
- Virdun, C.; Luckett, T.; Davidson, P.M.; Phillips, J. Dying in the hospital setting: A systematic review of quantitative studies identifying the elements of end-of-life care that patients and their families rank as being most important. Palliat. Med. 2015, 29, 774–796. [Google Scholar] [CrossRef]
- Hobbs, G.S.; Landrum, M.B.; Arora, N.K.; Ganz, P.A.; van Ryn, M.; Weeks, J.C.; Mack, J.W.; Keating, N.L. The role of families in decisions regarding cancer treatments. Cancer 2015, 121, 1079–1087. [Google Scholar] [CrossRef]
- Hien, L.T.; Chanruangvanich, W.; Thosingha, O. Factors related to needs in palliative care among patients with hepatocellular carcinoma. Nurs. Sci. J. Thail 2017, 35, 87–95. [Google Scholar]
- Woodrell, C.D.; Hansen, L.; Schiano, T.D.; Goldstein, N.E. Palliative care for people with hepatocellular carcinoma, and specific benefits for older adults. Clin. Ther. 2018, 40, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.; Eng, D.; Ang, Q.; Clarke, E.; Sinha, A. Goals of care discussions in acute hospital admissions-qualitative description of perspectives from patients, family and their doctors. Patient Educ. Couns 2021, 104, 2877–2887. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.L.; Roter, D.L. Family presence in routine medical visits: A meta-analytical review. Soc. Sci. Med 2011, 72, 823–831. [Google Scholar] [CrossRef]
- Kaiser, K.; Mallick, R.; Butt, Z.; Mulcahy, M.F.; Benson, A.B.; Cella, D. Important and relevant symptoms including pain concerns in hepatocellular carcinoma (HCC): A patient interview study. Support Care Cancer 2014, 22, 919–926. [Google Scholar] [CrossRef]
- Li, L.; Mo, F.K.; Chan, S.L.; Hui, E.P.; Tang, N.S.; Koh, J.; Leung, L.K.S.; Poon, A.N.Y.; Hui, J.; Chu, C.M.; et al. Prognostic values of EORTC QLQ-C30 and QLQ-HCC18 index-scores in patients with hepatocellular carcinoma-clinical application of health-related quality-of-life data. BMC Cancer 2017, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, S.; Malhotra, C.; Teo, I.; Tan, S.N.G.; Wong, W.H.M.; Joad, A.S.K.; Hapuara, T.; Gayatri, P.; Tuong, P.N.; Bhatnagar, S.; et al. Patient-reported roles in decision-making among Asian patients with advanced cancer: A multicountry study. MDM Policy Pract. 2021, 6, 23814683211061398. [Google Scholar] [CrossRef]
- Christie, K.M.; Meyerowitz, B.E.; Giedzinska-Simons, A.; Gross, M.; Agus, D.B. Predictors of affect following treatment decision-making for prostate cancer: Conversations, cognitive processing, and coping. Psychooncology 2009, 18, 508–514. [Google Scholar] [CrossRef]
- Kvåle, K. Do cancer patients always want to talk about difficult emotions? A qualitative study of cancer inpatients communication needs. Eur. J. Oncol. Nurs. 2007, 11, 320–327. [Google Scholar] [CrossRef]
- Zeilani, R.S.; Abdalrahim, M.S.; Hamash, K.; Albusoul, R.M. The experience of family support among patients newly diagnosed with cancer in Jordan. Eur. J. Oncol. Nurs. 2022, 60, 102173. [Google Scholar] [CrossRef]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef]
- Nilchaikovit, T.; Lortrakul, M.; Phisansuthideth, U. Development of Thai version of Hospital Anxiety and Depression Scale in cancer patients. J. Psychiatr. Assoc. Thailand 1996, 41, 18–30. [Google Scholar]
- Polit, D.F.; Beck, C.T. Nursing Research: Principles and Methods, 7th ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2003. [Google Scholar]
- Chewaskulyong, B.; Sapinun, L.; Downing, G.M.; Intaratat, P.; Lesperance, M.; Leautrakul, S.; Somwangprasert, T.; Leerapun, T. Reliability and validity of the Thai translation (Thai PPS Adult Suandok) of the Palliative Performance Scale (PPSv2). Palliat. Med. 2012, 26, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Tsoris, A.; Marlar, C.A. Use of the Child Pugh score in liver disease. In StatPearls; StatPearls Publishing Copyright © 2023; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- McCorkle, R.; Ercolano, E.; Lazenby, M.; Schulman-Green, D.; Schilling, L.S.; Lorig, K.; Wagner, E.H. Self-management: Enabling and empowering patients living with cancer as a chronic illness. CA Cancer J. Clin. 2011, 61, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Cincidda, C.; Pizzoli, S.F.M.; Ongaro, G.; Oliveri, S.; Pravettoni, G. Caregiving and shared decision making in breast and prostate cancer patients: A systematic review. Curr. Oncol. 2023, 30, 803–823. [Google Scholar] [CrossRef]
- Pitceathly, C.; Maguire, P.; Fletcher, I.; Parle, M.; Tomenson, B.; Creed, F. Can a brief psychological intervention prevent anxiety or depressive disorders in cancer patients? A randomised controlled trial. Ann. Oncol. 2009, 20, 928–934. [Google Scholar] [CrossRef]


{kind=link}
| Day | Duration (Minutes) | Key Aspects of Involvement | Activities |
|---|---|---|---|
| 1 | 15–20 | Pretest |
|
| 30–40 |
|
| |
| 2–4 | 40–60 |
|
|
| 5 | 15–20 | Post-test |
|
| Characteristics | Group | Statistic Results | p-Value | |
|---|---|---|---|---|
| Intervention (20) n(%) | Control (20) n(%) | |||
| Religious affiliation # | 0.404 | 0.525 | ||
| Buddhism | 10 (50) | 12 (60) | ||
| Islam | 10 (50) | 8 (40) | ||
| Educational level # | 6 (30) 8 (40) 6 (30) | 5 (25) 9 (45) 6 (30) | 0.150 | 0.928 |
| Primary school | ||||
| Secondary school/high school/diploma | ||||
| Bachelor degree/or higher | ||||
| Marital status ## | 1.619 | 0.695 | ||
| Single | 1 (5) | 1 (5) | ||
| Married | 17 (85) | 14 (70) | ||
| Widowed/divorced/separated | 2 (10) | 5 (25) | ||
| Occupation ## | 0.648 | 0.878 | ||
| Unemployed | 15 (75) | 13 (65) | ||
| Government officer | 3 (15) | 5 (25) | ||
| Merchant | 2 (10) | 2 (10) | ||
| Caregivers’ age (years) # | 0.784 | 0.661 | ||
| <60 | 16 (80) | 18 (90) | ||
| ≥60 | 4 (20) | 2 (10) | ||
| Relationship with patients # | 0.114 | 0.736 | ||
| Spouse | 14 (70) | 13 (65) | ||
| Daughter/son | 6 (30) | 7 (35) | ||
| Caregivers’ gender ## | 0.173 | 0.500 | ||
| Female | 16 (80) | 17 (85) | ||
| Male | 4 (20) | 3 (15) | ||
| Caregivers’ occupation # | 3.552 | 0.314 | ||
| Farmer/gardener | 9 (45) | 12 (60) | ||
| Merchant | 9 (45) | 4 (20) | ||
| Government officer | 2 (10) | 3 (15) | ||
| Unemployed | 0 | 1 (5) | ||
| PPS ## | 1.726 | 1.000 | ||
| End-of-life phase | 0 (0) | 1 (5) | ||
| Transition phase | 18 (90) | 18 (90) | ||
| Stable phase | 2 (10) | 1 (5) | ||
| Severity of disease (Child Pugh | 0.100 | 0.752 | ||
| score) # | ||||
| Child Pugh score B | 11 (55) | 10 (50) | ||
| Child Pugh score C | 9 (45) | 10 (50) | ||
| Duration since diagnosis with | 1.245 | 0.776 | ||
| advanced stage (days) ## | ||||
| ≤30 | 4 (20) | 6 (30) | ||
| 31–60 | 8 (40) | 5 (25) | ||
| 61–90 | 5 (25) | 5 (25) | ||
| >90 | 3 (15) | 4 (20) | ||
| Variables | Group | Mean | SD | df | t | p-Value |
|---|---|---|---|---|---|---|
| Anxiety | Experiment | 10.65 | 0.67 | 19 | 0.24 | 0.813 |
| Control | 10.70 | 0.65 | ||||
| Depression | Experiment | 10.40 | 0.82 | 19 | 1.59 | 0.119 |
| Control | 9.70 | 1.78 |
| Variables | Time Point | Mean | SD | df | t | p-Value |
|---|---|---|---|---|---|---|
| Anxiety | ||||||
| Pretest | 10.65 | 0.67 | 19 | 7.55 | 0.000 * | |
| Post-test | 9.15 | 0.81 | ||||
| Depression | ||||||
| Pretest | 10.40 | 0.82 | 19 | 5.44 | 0.000 * | |
| Post-test | 8.80 | 1.10 |
| Variables | Group | Mean | SD | df | t | p-Value |
|---|---|---|---|---|---|---|
| Anxiety | Experiment | 9.15 | 0.81 | 38 | 4.05 | 0.000 * |
| Control | 10.15 | 0.74 | ||||
| Depression | Experiment | 8.80 | 1.10 | 38 | 2.59 | 0.013 ** |
| Control | 9.80 | 1.32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klankaew, S.; Temthup, S.; Nilmanat, K.; Fitch, M.I. The Effect of a Nurse-Led Family Involvement Program on Anxiety and Depression in Patients with Advanced-Stage Hepatocellular Carcinoma. Healthcare 2023, 11, 460. https://doi.org/10.3390/healthcare11040460
Klankaew S, Temthup S, Nilmanat K, Fitch MI. The Effect of a Nurse-Led Family Involvement Program on Anxiety and Depression in Patients with Advanced-Stage Hepatocellular Carcinoma. Healthcare. 2023; 11(4):460. https://doi.org/10.3390/healthcare11040460
Chicago/Turabian StyleKlankaew, Sukhuma, Suthisa Temthup, Kittikorn Nilmanat, and Margaret I. Fitch. 2023. "The Effect of a Nurse-Led Family Involvement Program on Anxiety and Depression in Patients with Advanced-Stage Hepatocellular Carcinoma" Healthcare 11, no. 4: 460. https://doi.org/10.3390/healthcare11040460
APA StyleKlankaew, S., Temthup, S., Nilmanat, K., & Fitch, M. I. (2023). The Effect of a Nurse-Led Family Involvement Program on Anxiety and Depression in Patients with Advanced-Stage Hepatocellular Carcinoma. Healthcare, 11(4), 460. https://doi.org/10.3390/healthcare11040460