
Do Patients with Chronic Spinal Pain and Comorbid Insomnia Have More Features of Central Sensitization? A Case-Control Study

 , , , , , , , , , , ,
, , , , , , , , , , ,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
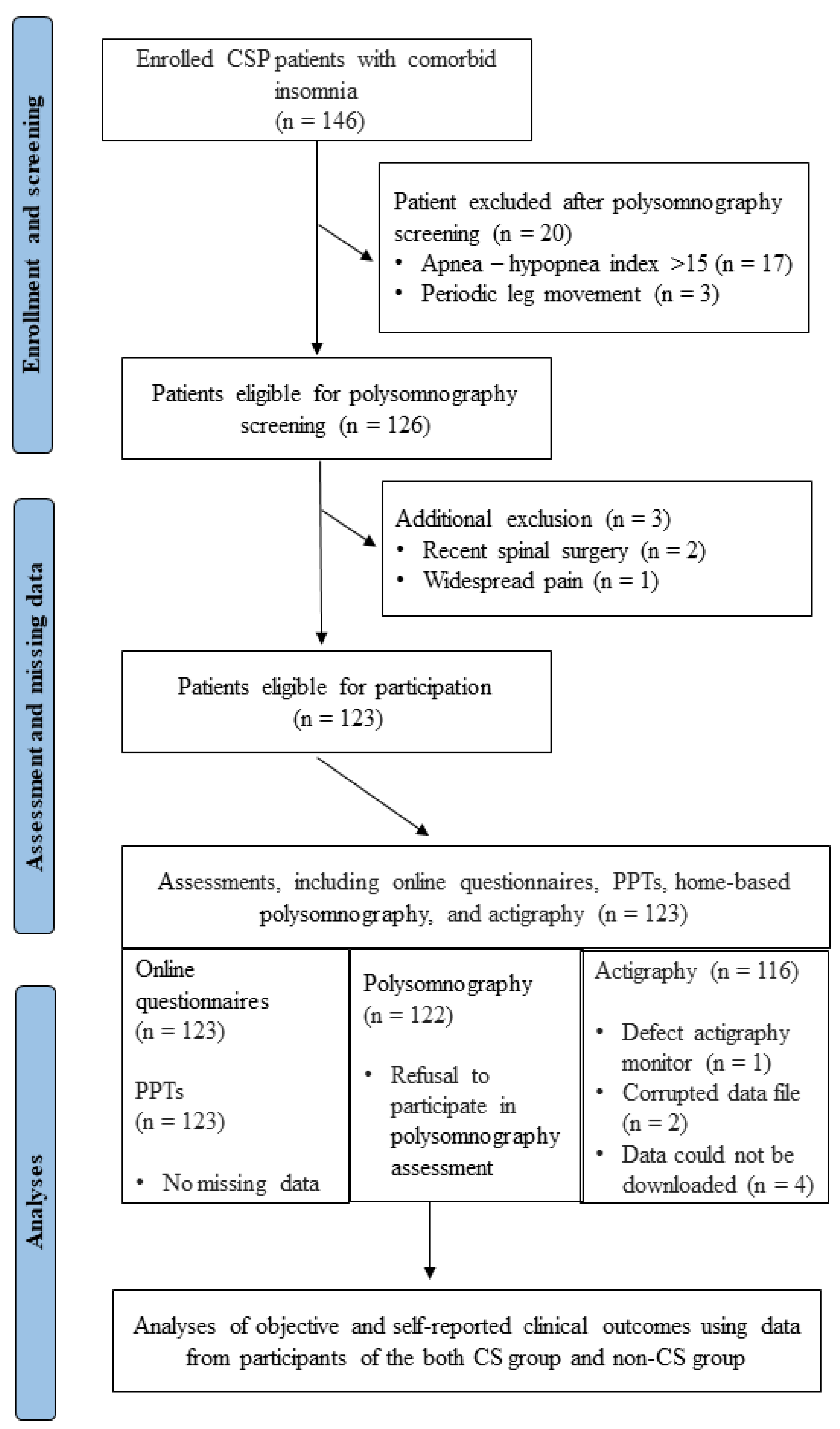
2.1. Study Design and Settings
2.2. Participants
2.3. Outcomes Measures
2.3.1. Pain-Related Information
2.3.2. Sleep-Related Outcomes
2.3.3. Physical Activity and Functioning Outcome
2.3.4. Anxiety, Depressive Symptoms, and Fatigue
2.3.5. Pressure Pain Thresholds
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Comparison Outcomes between CS and Non-CS Group
Sleep Outcomes
3.2. Physical Activity and Functioning Outcome
3.3. Anxiety, Depressive Symptoms, and Fatigue Outcomes
3.4. Pressure Pain Thresholds
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine J. 2006, 15, 834–848. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.; Conrad, D.; Volinn, E. Cost, controversy, crisis: Low back pain and the health of the public. Annu. Rev. Public Health 1991, 12, 141–156. [Google Scholar] [CrossRef]
- Daffner, S.D.; Hilibrand, A.S.; Hanscom, B.S.; Brislin, B.T.; Vaccaro, A.R.; Albert, T.J. Impact of neck and arm pain on overall health status. Spine 2003, 28, 2030–2035. [Google Scholar] [CrossRef]
- Von Korff, M.; Crane, P.; Lane, M.; Miglioretti, D.L.; Simon, G.; Saunders, K.; Stang, P.; Brandenburg, N.; Kessler, R. Chronic spinal pain and physical-mental comorbidity in the United States: Results from the national comorbidity survey replication. Pain 2005, 113, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.K.Y.; Wright, K.J.; Salkovskis, P.M. Prevalence and correlates of clinical insomnia co-occurring with chronic back pain. J. Sleep Res. 2007, 16, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Roth, T. Insomnia: Definition, Prevalence, Etiology, and Consequences. J. Clin. Sleep Med. 2007, 3 (Suppl. S5), S7. [Google Scholar] [CrossRef]
- Sayar, K.; Arikan, M.; Yontem, T. Sleep quality in chronic pain patients. Can. J. Psychiatry 2002, 47, 844–848. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, D.H.; Yoon, K.B.; An, J.R.; Yoon, D.M. Factors Associated with Increased Risk for Clinical Insomnia in Patients with Chronic Neck Pain. Pain Physician 2015, 18, 593–598. Available online: https://ir.ymlib.yonsei.ac.kr/handle/22282913/156955 (accessed on 1 September 2023).
- Gerhart, J.I.; Burns, J.W.; Post, K.M.; Smith, D.A.; Porter, L.S.; Burgess, H.J.; Schuster, E.; Buvanendran, A.; Fras, A.M.; Keefe, F.J. Relationships Between Sleep Quality and Pain-Related Factors for People with Chronic Low Back Pain: Tests of Reciprocal and Time of Day Effects. Ann. Behav. Med. 2017, 51, 365. [Google Scholar] [CrossRef]
- Kelly, G.A.; Blake, C.; Power, C.K.; Okeeffe, D.; Fullen, B.M. The association between chronic low back pain and sleep: A systematic review. Clin. J. Pain 2011, 27, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain 2013, 14, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R.M.; Hartzell, M.M.; Cohen, H.; Mayer, T.G.; Williams, M.; Choi, Y.M.; Gatchel, R.J.P. Ability of the central sensitization inventory to identify central sensitivity syndromes in an outpatient chronic pain sample. Clin. J. Pain 2015, 31, 323–332. [Google Scholar] [CrossRef]
- Neblett, R. The central sensitization inventory: A user’s manual. J. Appl. Biobehav. Res. 2018, 23, e12123. [Google Scholar] [CrossRef]
- Tang, N.K.Y.; Goodchild, C.E.; Sanborn, A.N.; Howard, J.; Salkovskis, P.M. Deciphering the temporal link between pain and sleep in a heterogeneous chronic pain patient sample: A multilevel daily process study. Sleep 2012, 35, 675–687. [Google Scholar] [CrossRef]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef]
- Roussel, N.A.; Nijs, J.; Meeus, M.; Mylius, V.; Fayt, C.; Oostendorp, R. Central sensitization and altered central pain processing in chronic low back pain: Fact or myth? Clin. J. Pain 2013, 29, 625–638. [Google Scholar] [CrossRef]
- Van Looveren, E.; Bilterys, T.; Munneke, W.; Cagnie, B.; Ickmans, K.; Mairesse, O.; Malfliet, A.; De Baets, L.; Nijs, J.; Goubert, D.; et al. The association between sleep and chronic spinal pain: A systematic review from the last decade. J. Clin. Med. 2021, 10, 3836. [Google Scholar] [CrossRef]
- Zusman, M. Forebrain-mediated sensitization of central pain pathways: ‘non-specific’ pain and a new image for, M.T. Man. Ther. 2002, 7, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Alsaadi, S.M.; McAuley, J.H.; Hush, J.M.; Maher, C.G. Prevalence of sleep disturbance in patients with low back pain. Eur. Spine J. 2011, 20, 737. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.T.; Haythornthwaite, J.A. How do sleep disturbance and chronic pain inter-relate? Insights from the longitudinal and cognitive-behavioral clinical trials literature. Sleep Med. Rev. 2004, 8, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Haack, M.; Scott-Sutherland, J.; Santangelo, G.; Simpson, N.S.; Sethna, N.; Mullington, J.M. Pain sensitivity and modulation in primary insomnia. Eur. J. Pain 2012, 16, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Steinmetz, A.; Hacke, F.; Delank, K.S. Pressure Pain Thresholds and Central Sensitization in Relation to Psychosocial Predictors of Chronicity in Low Back Pain. Diagnostics 2023, 13, 786. [Google Scholar] [CrossRef] [PubMed]
- Pedler, A.; Sterling, M. Patients with chronic whiplash can be subgrouped on the basis of symptoms of sensory hypersensitivity and posttraumatic stress. Pain 2013, 154, 1640–1648. [Google Scholar] [CrossRef] [PubMed]
- Aili, K.; Hillert, L.; Nyman, T.; Svartengren, M. Sleep disturbances predict future sickness absence among individuals with lower back or neck-shoulder pain: A 5-year prospective study. Scand. J. Public Health 2015, 43, 315–323. [Google Scholar] [CrossRef]
- Malfliet, A.; Bilterys, T.; Van Looveren, E.; Meeus, M.; Danneels, L.; Ickmans, K.; Cagnie, B.; Mairesse, O.; Neu, D.; Moens, M.; et al. The added value of cognitive behavioral therapy for insomnia to current best evidence physical therapy for chronic spinal pain: Protocol of a randomized controlled clinical trial. Braz. J. Phys. Ther. 2019, 23, 62–70. [Google Scholar] [CrossRef]
- Jungquist, C.R.; O’brien, C.; Matteson-Rusby, S.; Smith, M.T.; Pigeon, W.R.; Xia, Y.; Lu, N.; Perlis, M.L. The efficacy of cognitive-behavioral therapy for insomnia in patients with chronic pain. Sleep Med. 2010, 11, 302–309. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef]
- Smith, M.T.; Remeniuk, B.; Finan, P.H.; Speed, T.J.; Tompkins, D.A.; Robinson, M.; Gonzalez, K.; Bjurstrom, M.F.; Irwin, M.R. Sex differences in measures of central sensitization and pain sensitivity to experimental sleep disruption: Implications for sex differences in chronic pain. Sleep 2019, 42, zsy209. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Updates for 2017 (Version 2.4). J. Clin. Sleep Med. 2017, 13, 665. [Google Scholar] [CrossRef] [PubMed]
- Mathias, J.L.; Cant, M.L.; Burke, A.L.J. Sleep disturbances and sleep disorders in adults living with chronic pain: A meta-analysis. Sleep Med. 2018, 52, 198–210. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Gagnon, C.; Bélanger, L.; Ivers, H.; Morin, C.M. Validation of the Insomnia Severity Index in primary care. J. Am. Board Fam. Med. 2013, 26, 701–710. [Google Scholar] [CrossRef]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional beliefs and attitudes about sleep (DBAS): Validation of a brief version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef]
- Lapin, B.R.; Bena, J.F.; Walia, H.K.; Moul, D.E. The Epworth Sleepiness Scale: Validation of One-Dimensional Factor Structure in a Large Clinical Sample. J. Clin. Sleep Med. 2018, 14, 1293–1301. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef]
- Fabbri, M.; Beracci, A.; Martoni, M.; Meneo, D.; Tonetti, L.; Natale, V. Measuring Subjective Sleep Quality: A Review. Int. J. Environ. Res. Public Health 2021, 18, 1082. [Google Scholar] [CrossRef]
- Bastien, C.H.; Morin, C.M.; Ouellet, M.C.; Blais, F.C.; Bouchard, S. Cognitive-behavioral therapy for insomnia: Comparison of individual therapy, group therapy, and telephone consultations. J. Consult. Clin. Psychol. 2004, 72, 653–659. [Google Scholar] [CrossRef]
- Kendzerska, T.B.; Smith, P.M.; Brignardello-Petersen, R.; Leung, R.S.; Tomlinson, G.A. Evaluation of the measurement properties of the Epworth sleepiness scale: A systematic review. Sleep Med. Rev. 2014, 18, 321–331. [Google Scholar] [CrossRef]
- Martin, J.L.; Hakim, A.D. Wrist Actigraphy. Chest 2011, 139, 1514. [Google Scholar] [CrossRef] [PubMed]
- Aili, K.; Åström-Paulsson, S.; Stoetzer, U.; Svartengren, M.; Hillert, L. Reliability of Actigraphy and Subjective Sleep Measurements in Adults: The Design of Sleep Assessments. J. Clin. Sleep Med. 2017, 13, 39–47. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.A.; Ware, J.E.; Raczek, A.E. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Mairesse, O.; Damen, V.; Newell, J.; Kornreich, C.; Verbanck, P.; Neu, D. The Brugmann Fatigue Scale: An Analogue to the Epworth Sleepiness Scale to Measure Behavioral Rest Propensity. Behav. Slee. Med. 2019, 17, 437–458. [Google Scholar] [CrossRef]
- Fischer, A.A. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain 1987, 30, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Chesterton, L.S.; Sim, J.; Wright, C.C.; Foster, N.E. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters. Clin. J. Pain 2007, 23, 760–766. [Google Scholar] [CrossRef]
- Amiri, M.; Alavinia, M.; Singh, M.; Kumbhare, D. Pressure Pain Threshold in Patients with Chronic Pain: A Systematic Review and Meta-Analysis. Am. J. Phys. Med. Rehabil. 2021, 100, 656–674. [Google Scholar] [CrossRef] [PubMed]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012, 12, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Kregel, J.; Vuijk, P.J.; Descheemaeker, F.; Keizer, D.; van der Noord, R.; Nijs, J.; Cagnie, B.; Meeus, M.; van Wilgen, P. The Dutch Central Sensitization Inventory (CSI): Factor Analysis, Discriminative Power, and Test-Retest Reliability. Clin. J. Pain 2016, 32, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Heston, T.F.; King, J.M. Predictive power of statistical significance. World J. Methodol. 2017, 7, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152 (Suppl. S1), S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R.; Hartzell, M.M.; Mayer, T.G.; Cohen, H.; Gatchel, R.J. Establishing Clinically Relevant Severity Levels for the Central Sensitization Inventory. Pain Pract. 2017, 17, 166–175. [Google Scholar] [CrossRef]
- Chang, J.R.; Fu, S.-N.; Li, X.; Li, S.X.; Wang, X.; Zhou, Z.; Pinto, S.M.; Samartzis, D.; Karppinen, J.; Wong, A.Y. The differential effects of sleep deprivation on pain perception in individuals with or without chronic pain: A systematic review and meta-analysis. Sleep Med. Rev. 2022, 66, 101695. [Google Scholar] [CrossRef]
- Othman, R.; Jayakaran, P.; Swain, N.; Dassanayake, S.; Tumilty, S.; Mani, R. Relationships Between Psychological, Sleep, and Physical Activity Measures and Somatosensory Function in People with Peripheral Joint Pain: A Systematic Review and Meta-Analysis. Pain Pract. 2021, 21, 226–261. [Google Scholar] [CrossRef]
- Bilterys, T.; Van Looveren, E.; Malfliet, A.; Nijs, J.; Meeus, M.; Danneels, L.; Ickmans, K.; Cagnie, B.; Goubert, D.; Moens, M.; et al. Relationship, differences, and agreement between objective and subjective sleep measures in chronic spinal pain patients with comorbid insomnia: A cross-sectional study. Pain 2023, 164, 2016–2028. [Google Scholar] [CrossRef]
- NICE. Overview—Physical Activity: Exercise Referral Schemes—Guidance. Available online: https://www.nice.org.uk/guidance/ph54 (accessed on 30 August 2023).
- Hamer, M.; Ingle, L.; Carroll, S.; Stamatakis, E. Physical activity and cardiovascular mortality risk: Possible protective mechanisms? Med. Sci. Sports Exerc. 2012, 44, 84–88. [Google Scholar] [CrossRef]
- Koes, B.W.; Van Tulder, M.; Lin, C.W.C.; Macedo, L.G.; McAuley, J.; Maher, C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur. Spine J. 2010, 19, 2075. [Google Scholar] [CrossRef] [PubMed]
- Tesarz, J.; Schuster, A.K.; Hartmann, M.; Gerhardt, A.; Eich, W. Pain perception in athletes compared to normally active controls: A systematic review with meta-analysis. Pain 2012, 153, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Frey-Law, L.; Bement, M.H. Exercise-induced pain and analgesia? Underlying mechanisms and clinical translation. Pain 2018, 159 (Suppl. S1), S91–S97. [Google Scholar] [CrossRef] [PubMed]
- De Zoete, R.M.J.; Chen, K.; Sterling, M. Central neurobiological effects of physical exercise in individuals with chronic musculoskeletal pain: A systematic review. BMJ Open 2020, 10, e036151. [Google Scholar] [CrossRef]
- Blay, S.L.; Andreoli, S.B.; Gastal, F.L. Chronic painful physical conditions, disturbed sleep and psychiatric morbidity: Results from an elderly survey. Ann. Clin. Psychiatry 2007, 19, 169–174. [Google Scholar] [CrossRef]
- Mork, P.J.; Vik, K.L.; Moe, B.; Lier, R.; Bardal, E.M.; Nilsen, T.I.L. Sleep problems, exercise and obesity and risk of chronic musculoskeletal pain: The Norwegian HUNT study. Eur. J. Public Health 2014, 24, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Bilterys, T.; Siffain, C.; De Maeyer, I.; Van Looveren, E.; Mairesse, O.; Nijs, J.; Meeus, M.; Ickmans, K.; Cagnie, B.; Goubert, D.; et al. Associates of insomnia in people with chronic spinal pain: A systematic review and meta-analysis. J. Clin. Med. 2021, 10, 3175. [Google Scholar] [CrossRef]
- Louw, A.; Diener, I.; Butler, D.S.; Puentedura, E.J. The Effect of Neuroscience Education on Pain, Disability, Anxiety, and Stress in Chronic Musculoskeletal Pain. Arch. Phys. Med. Rehabil. 2011, 92, 2041–2056. [Google Scholar] [CrossRef]
- Shigetoh, H.; Tanaka, Y.; Koga, M.; Osumi, M.; Morioka, S. The Mediating Effect of Central Sensitization on the Relation between Pain Intensity and Psychological Factors: A Cross-Sectional Study with Mediation Analysis. Pain Res. Manag. 2019, 2019, 3916135. [Google Scholar] [CrossRef]
- Neblett, R.; Hartzell, M.M.; Williams, M.; Bevers, K.R.; Mayer, T.G.; Gatchel, R.J. Use of the Central Sensitization Inventory (CSI) as a treatment outcome measure for patients with chronic spinal pain disorder in a functional restoration program. Spine J. 2017, 17, 1819–1829. [Google Scholar] [CrossRef]
- Finan, P.H.; Buenaver, L.F.; Runko, V.T.; Smith, M.T. Cognitive-Behavioral Therapy for Comorbid Insomnia and Chronic Pain. Sleep Med. Clin. 2014, 9, 261. [Google Scholar] [CrossRef] [PubMed]
- Walton, D.; Macdermid, J.; Nielson, W.; Teasell, R.; Nailer, T.; Maheu, P. A descriptive study of pressure pain threshold at 2 standardized sites in people with acute or subacute neck pain. J. Orthop. Sports Phys. Ther. 2011, 41, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Den Boer, C.; Terluin, B.; van der Wouden, J.C.; Blankenstein, A.H.; van der Horst, H.E. Tests for central sensitization in general practice: A Delphi study. BMC Fam. Pract. 2021, 22, 206. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Inclusion | Exclusion |
|---|---|
| Aged between 18 and 65 years | Severe underlying sleep pathology (identified through baseline data of polysomnography) |
| Nonspecific spinal pain (≥3 months duration), and presence of pain ≥ 3 days/week. | Neuropathic pain and chronic widespread pain syndromes |
| Seeking care because of neck pain or low back pain | Shift workers |
| Native Dutch speaker | Being pregnant or became a parent in the preceding year |
| Having insomnia: no presence of other intrinsic sleep disorders | Thoracic pain in absence of neck or low back pain |
| Not starting new treatments or medication, and continuing their usual care six weeks prior to and during study participation (to obtain a steady state) | Spinal surgery history (i.e., surgery for spinal stenosis) |
| Refraining from analgesics and other substances that modulate the nervous system (caffeine, alcohol, or nicotine) in the 48 h prior to the assessments | Body Mass Index > 30 kg/m2 |
| Nonspecific failed back surgery > 3 years are permitted | Current depression diagnosed by a doctor |
| Not undertaking exercise 3 days before the assessments | Not willing to refrain from analgesics in the 48 h prior to the assessments |
| Characteristics | CS Group (n = 82) | Non-CS Group (n = 41) | 95% CI | p-Value |
|---|---|---|---|---|
| Age, years | 38.7 ± 10.2 | 43.6 ± 12 | 0.80, 9.02 | 0.02 |
| Body Mass Index, kg/m2 | 23 ± 3.3 | 23.9 ± 2.74 | −0.32, 2.04 | 0.15 |
| Pain duration, months | 87 ± 92.3 | 93.4 ± 104 | −30.7, 43.4 | 0.70 |
| Sex, n (%) | ||||
| Female | 64 (78) | 18 (44) | −0.51, −0.17 | <0.001 |
| Pain location, n (%) | ||||
| Cervical pain | 50 (61) | 21 (51.2) | −0.42, 1.58 | 0.19 |
| Back pain | 32 (39) | 20 (48.8) | −0.06, 0.31 | 0.21 |
| CSI score range, n (%) | ||||
| 0–29 | − | 10 (8) | ||
| 30–39 | − | 31 (25) | ||
| 40–49 | 45 (36) | − | ||
| 50–59 | 26 (21) | − | ||
| 60–100 | 11 (9) | − | ||
| CSI total score | 49.5 ± 7.4 | 32 ± 6 | −19.9, −15.0 | <0.001 |
| Outcomes | CS Group (n = 81) | Non-CS Group (n = 41) | 95% CI | p-Value |
| Objective sleep, median (Q3–Q1) | ||||
| Time in bed | 476.7 (95) | 471.7 (82.1) | −36.3, 18.5 | 0.60 |
| Total sleep time | 433.5 (79.1) | 409.5 (87) | −42, 3.3 | 0.07 |
| Sleep onset latency | 10.5 (12) | 9.5 (12) | −8.8, 4.7 | 0.70 |
| Wake duration after sleep onset | 26.7 (25.5) | 37.7 (49.5) | −0.53, 25.7 | 0.08 |
| Sleep efficiency | 91.4 (8.1) | 90.7 (8.3) | −5.2, 0.37 | 0.15 |
| Self-reported sleep, mean ± SD | ||||
| Outcomes | CS group (n = 82) | Non-CS group (n = 41) | 95% CI | p-Value |
| PSQI | 10.1 ± 2.6 | 8.3 ± 2.3 | −2.7, −0.90 | <0.01 |
| ISI | 16.2 ± 3.8 | 13 ± 3.8 | −0.73, −0.33 | <0.01 |
| DBAS-16 | 3.17 ± 0.4 | 2.65 ± 0.6 | −0.61, −0.24 | <0.01 |
| ESS | 8.5 ± 4.7 | 7.7 ± 4.5 | −2.5, 0.96 | 0.30 |
| Outcomes | CS Group (n = 76) | Non-CS Group (n = 40) | 95% CI | p-Value |
|---|---|---|---|---|
| Actigraphy, mean ± SD | ||||
| % in light | 39.3 ± 6.1 | 39 ± 5.4 | −2.5, 1.96 | 0.79 |
| % in sedentary | 48.4 ± 7.2 | 50 ± 6.9 | −1.1, 4.27 | 0.20 |
| % in moderate | 12.1 ± 4.1 | 10.9 ± 4 | −2.8, 0.31 | 0.10 |
| Functioning, mean ± SD | ||||
| PCS (SF-36) | 213.6 ± 63.8 | 268.3 ± 59.7 | 31.5, 78.4 | <0.01 |
| MCS (SF-36) | 238.8 ± 74 | 287 ± 67.2 | 21, 75.4 | 0.01 |
| Outcomes | CS Group (n = 82) | Non-CS Group (n = 41) | 95% CI | p-Value |
|---|---|---|---|---|
| HADS, mean ± SD | ||||
| Anxiety | 9.6 ± 3.6 | 7 ± 2.7 | −3.7, −1.3 | <0.001 |
| Depressive symptoms | 5.6 ± 3.2 | 4.2 ± 3.2 | −2.6, −0.18 | <0.001 |
| BFS, mean ± SD | ||||
| Physical | 3.8 ± 2.1 | 2.4 ± 1.8 | −2, −0.62 | 0.001 |
| Mental | 3.6 ± 2.5 | 2.5 ± 2.3 | −2, −0.14 | 0.02 |
| Outcomes | CS Group (n = 82) | Non-CS Group (n = 41) | 95% CI | p-Value |
|---|---|---|---|---|
| Symptomatic site, mean ± SD | ||||
| Trapezius (KPa) | 3.8 ± 2.3 | 5 ± 2.4 | 0.06, 1.8 | 0.03 |
| Lumbar (KPa) | 5.2 ± 2.1 | 7.1 ± 3.3 | 0.08, 2.8 | <0.001 |
| Remote site, mean ± SD | ||||
| Hand (KPa) | 3.8 ± 1.3 | 4.5 ± 1.8 | 0.08, 1.2 | 0.02 |
| Calf (KPa) | 4.5 ± 1.5 | 5.5 ± 2.1 | 0.03, 1.7 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araújo Almeida, L.; Bilterys, T.; Van Looveren, E.; Mairesse, O.; Cagnie, B.; Meeus, M.; Moens, M.; Goubert, D.; Munneke, W.; Danneels, L.; et al. Do Patients with Chronic Spinal Pain and Comorbid Insomnia Have More Features of Central Sensitization? A Case-Control Study. Healthcare 2023, 11, 3152. https://doi.org/10.3390/healthcare11243152
Araújo Almeida L, Bilterys T, Van Looveren E, Mairesse O, Cagnie B, Meeus M, Moens M, Goubert D, Munneke W, Danneels L, et al. Do Patients with Chronic Spinal Pain and Comorbid Insomnia Have More Features of Central Sensitization? A Case-Control Study. Healthcare. 2023; 11(24):3152. https://doi.org/10.3390/healthcare11243152
Chicago/Turabian StyleAraújo Almeida, Lucas, Thomas Bilterys, Eveline Van Looveren, Olivier Mairesse, Barbara Cagnie, Mira Meeus, Maarten Moens, Dorien Goubert, Wouter Munneke, Lieven Danneels, and et al. 2023. "Do Patients with Chronic Spinal Pain and Comorbid Insomnia Have More Features of Central Sensitization? A Case-Control Study" Healthcare 11, no. 24: 3152. https://doi.org/10.3390/healthcare11243152
APA StyleAraújo Almeida, L., Bilterys, T., Van Looveren, E., Mairesse, O., Cagnie, B., Meeus, M., Moens, M., Goubert, D., Munneke, W., Danneels, L., Ickmans, K., Rezende Camargo, P., Nijs, J., Malfliet, A., & De Baets, L. (2023). Do Patients with Chronic Spinal Pain and Comorbid Insomnia Have More Features of Central Sensitization? A Case-Control Study. Healthcare, 11(24), 3152. https://doi.org/10.3390/healthcare11243152