


An Early Indicator in Evaluating Cardiac Dysfunction Related to Premature Ventricular Complexes: Cardiorespiratory Capacity


Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. CPET Method
2.3. Statistical Analysis
3. Results
3.1. Baseline Information
3.2. CPET Data
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cronin, E.M.; Bogun, F.M.; Maury, P.; Peichl, P.; Chen, M.; Namboodiri, N.; Aguinaga, L.; Leite, L.R.; Al-Khatib, S.M.; Anter, E.; et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Heart Rhythm 2020, 17, e2–e154. [Google Scholar] [CrossRef] [PubMed]
- Baman, T.S.; Lange, D.C.; Ilg, K.J.; Gupta, S.K.; Liu, T.-Y.; Alguire, C.; Armstrong, W.; Good, E.; Chugh, A.; Jongnarangsin, K.; et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm 2010, 7, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Munoz, F.D.C.; Syed, F.F.; Noheria, A.; Cha, Y.-M.; Friedman, P.A.; Hammill, S.C.; Munger, T.M.; Venkatachalam, K.; Shen, W.-K.; Packer, D.L.; et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: Study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J. Cardiovasc. Electrophysiol. 2011, 22, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Dukes, J.W.; Dewland, T.A.; Vittinghoff, E.; Mandyam, M.C.; Heckbert, S.R.; Siscovick, D.S.; Stein, P.K.; Psaty, B.M.; Sotoodehnia, N.; Gottdiener, J.S.; et al. Ventricular Ectopy as a Predictor of Heart Failure and Death. J. Am. Coll. Cardiol. 2015, 66, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Chang, S.-L.; Lin, Y.-J.; Lo, L.-W.; Chung, F.-P.; Chen, Y.-Y.; Chao, T.-F.; Hu, Y.-F.; Tuan, T.-C.; Liao, J.-N.; et al. Long-term outcome of multiform premature ventricular complexes in structurally normal heart. Int. J. Cardiol. 2015, 180, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Huizar, J.F.; Tan, A.Y.; Kaszala, K.; Ellenbogen, K.A. Clinical and translational insights on premature ventricular contractions and PVC-induced cardiomyopathy. Prog. Cardiovasc. Dis. 2021, 66, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Weber, K.T.; Kinasewitz, G.T.; Janicki, J.S.; Fishman, A.P. Oxygen utilization and ventilation during exercise in patients with chronic cardiac failure. Circulation 1982, 65, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 29.0; IBM Corp.: Armonk, NY, USA, 2022. [Google Scholar]
- Zalzstein, E.; Wagshal, A.; Zucker, N.; Levitas, A.; Ovsyshcher, I.E.; Katz, A. Ablation therapy of tachycardia-related cardiomyopathy. Isr. Med. Assoc. J. IMAJ 2003, 5, 64–65. [Google Scholar] [PubMed]
- Sekiguchi, Y.; Aonuma, K.; Yamauchi, Y.; Obayashi, T.; Niwa, A.; Hachiya, H.; Takahashi, A.; Nitta, J.; Iesaka, Y.; Isobe, M. Chronic hemodynamic effects after radiofrequency catheter ablation of frequent monomorphic ventricular premature beats. J. Cardiovasc. Electrophysiol. 2005, 16, 1057–1063. [Google Scholar] [CrossRef]
- Latchamsetty, R.; Bogun, F. Premature Ventricular Complex-Induced Cardiomyopathy. JACC Clin. Electrophysiol. 2019, 5, 537–550. [Google Scholar] [CrossRef]
- Corrado, D.; Perazzolo Marra, M.; Zorzi, A.; Beffagna, G.; Cipriani, A.; Lazzari, M.; Migliore, F.; Pilichou, K.; Rampazzo, A.; Rigato, I.; et al. Diagnosis of arrhythmogenic cardiomyopathy: The Padua criteria. Int. J. Cardiol. 2020, 319, 106–114. [Google Scholar] [CrossRef]
- Yokokawa, M.; Kim, H.M.; Good, E.; Chugh, A.; Pelosi, F.; Alguire, C.; Armstrong, W.; Crawford, T.; Jongnarangsin, K.; Oral, H.; et al. Relation of symptoms and symptom duration to premature ventricular complex-induced cardiomyopathy. Heart Rhythm 2012, 9, 92–95. [Google Scholar] [CrossRef]
- Jouven, X.; Zureik, M.; Desnos, M.; Courbon, D.; Ducimetière, P. Long-term outcome in asymptomatic men with exercise-induced premature ventricular depolarizations. N. Engl. J. Med. 2000, 343, 826–833. [Google Scholar] [CrossRef]
- Takemoto, M.; Yoshimura, H.; Ohba, Y.; Matsumoto, Y.; Yamamoto, U.; Mohri, M.; Yamamoto, H.; Origuchi, H. Radiofrequency catheter ablation of premature ventricular complexes from right ventricular outflow tract improves left ventricular dilation and clinical status in patients without structural heart disease. J. Am. Coll. Cardiol. 2005, 45, 1259–1265. [Google Scholar] [CrossRef]
- Walters, T.E.; Rahmutula, D.; Szilagyi, J.; Alhede, C.; Sievers, R.; Fang, Q.; Olgin, J.; Gerstenfeld, E.P. Left Ventricular Dyssynchrony Predicts the Cardiomyopathy Associated With Premature Ventricular Contractions. J. Am. Coll. Cardiol. 2018, 72, 2870–2882. [Google Scholar] [CrossRef] [PubMed]
- Napier, M.D.; Franceschini, N.; Gondalia, R.; Stewart, J.D.; Méndez-Giráldez, R.; Sitlani, C.M.; Seyerle, A.A.; Highland, H.M.; Li, Y.; Wilhelmsen, K.C.; et al. Genome-wide association study and meta-analysis identify loci associated with ventricular and supraventricular ectopy. Sci. Rep. 2018, 8, 5675. [Google Scholar] [CrossRef] [PubMed]
- Park, K.-M.; Im, S.I.; Park, S.-J.; Kim, J.S.; On, Y.K. Risk factor algorithm used to predict frequent premature ventricular contraction-induced cardiomyopathy. Int. J. Cardiol. 2017, 233, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Cağdaş, D.; Celiker, A.; Ozer, S. Premature ventricular contractions in normal children. Turk. J. Pediatr. 2008, 50, 260–264. [Google Scholar] [PubMed]
- Lee, V.; Hemingway, H.; Harb, R.; Crake, T.; Lambiase, P. The prognostic significance of premature ventricular complexes in adults without clinically apparent heart disease: A meta-analysis and systematic review. Heart 2012, 98, 1290–1298. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Controls (n = 98) | PVCs (n = 94) | p Value |
|---|---|---|---|
| Age (yrs) | 50.84 ± 9.41 | 49.83 ±13.63 | 0.551 |
| Male (n,%) | 55 (56.1) | 47 (50.0) | 0.395 |
| Height (cm) | 166.54 ± 7.58 | 165.97 ± 6.89 | 0.590 |
| Weight (kg) | 69.39 ± 13.38 | 65.92 ± 10.95 | 0.052 |
| Body mass index (kg/m2) | 24.89 ± 3.65 | 23.87 ± 3.36 | 0.050 |
| Smoking (n,%) | 15 (15.3) | 11 (11.8) | 0.484 |
| CAD (n,%) | 18 (18.1) | 16 (17.0) | 0.156 |
| ACS (n,%) | 10 (10.2) | 9 (9.6) | 0.892 |
| Number of lesional coronary artery | 0.771 | ||
| 1-vessel CAD (n,%) | 6 (6.1) | 8 (8.5) | |
| 2-vessel CAD (n,%) | 4 (4.1) | 3 (3.1) | |
| 3-vessel CAD (n,%) | 8 (8.2) | 5 (5.3) | |
| Gensini score | 16.77 ± 11.45 | 19.20 ± 17.01 | 0.672 |
| Hypertension (n,%) | 33 (33.7) | 47 (50.0) | 0.071 |
| Hyperlipidemia (n,%) | 23 (23.5) | 24 (25.5) | 0.997 |
| Diabetes (n,%) | 12 (12.2) | 14 (14.9) | 0.758 |
| Medication use | |||
| Beta-blocker (n,%) | 44 (44.9) | 37 (37.8) | 0.204 |
| Calcium channel blocker (n,%) | 19 (19.4) | 28 (28.6) | 0.178 |
| Laboratories | |||
| NT-proBNP (pg/mL) | 35.5 (49.5) | 62.1 (83.0) | 0.044 † |
| cTnI (ng/mL) | 5.32 ± 14.30 | 4.24 ± 6.81 | 0.509 |
| eGFR (mL/min/1.73 m²) | 91.86 ± 12.83 | 89.34 ± 20.97 | 0.532 |
| Characteristics | |
|---|---|
| QRS duration (ms) | 140 ± 33 |
| pseudo delta waves (n,%) | 10 (10.6) |
| axis | |
| superior axis (n,%) | 24 (25.5) |
| inferior axis (n,%) | 70 (74.5) |
| bundle branch-like morphology | |
| left (n,%) | 77 (81.9) |
| right (n,%) | 17 (18.1) |
| Subject | Controls | PVCs | p Value |
|---|---|---|---|
| LV size (mm) | 47.02 ± 4.68 | 47.93 ± 4.83 | 0.212 |
| LA size (mm) | 35.62 ± 4.99 | 35.88 ± 5.78 | 0.749 |
| IVS(mm) | 9.93 ± 1.80 | 9.44 ± 1.80 | 0.074 |
| LVPW (mm) | 9.46 ± 1.32 | 9.24 ± 1.52 | 0.305 |
| LVEF (%) | 63.11 ± 6.08 | 60.96 ± 8.1 | 0.055 |
| FS (%) | 34.47 ± 5.32 | 33.23 ± 6.19 | 0.157 |
| E/A | 1.17 ± 0.53 | 1.27 ± 0.58 | 0.224 |
| E/E′ | 11.46 ± 3.61 | 12.6 ± 5.45 | 0.107 |
| Subject | Controls (n = 98) | PVCs (n = 94) | p Value | Reference Value | Effect Size |
|---|---|---|---|---|---|
| AT (l/min) | 0.91 ± 0.22 | 0.80 ± 0.24 | 0.002 | - | −0.478 |
| V’O2 peak (l/min) | 1.42 ± 0.39 | 1.25 ± 0.40 | 0.004 | - | −0.430 |
| V’E peak (l/min) | 48.26 ± 12.16 | 42.37 ± 12.29 | 0.001 | - | −0.482 |
| SBP rest (mmHg) | 129.74 ± 26.15 | 126.61 ± 21.74 | 0.370 | - | −0.130 |
| DBP rest (mmHg) | 78.14 ± 15.64 | 78.52 ± 13.70 | 0.859 | - | 0.026 |
| HR rest (bpm) | 87.40 ±13.81 | 87.96 ± 14.63 | 0.785 | - | 0.039 |
| HR AT (bpm) | 111.39 ± 14.97 | 108.18 ± 18.50 | 0.188 | - | −0.191 |
| HR peak (bpm) | 142.66 ± 17.88 | 138.88 ± 26.58 | 0.247 | - | −0.168 |
| Load AT (W) | 59.34 ± 21.06 | 52.49 ± 23.51 | 0.035 | - | −0.307 |
| Load peak (W) | 101.97 ± 37.97 | 92.53 ± 37.35 | 0.084 | - | −0.251 |
| V’O2/HR peak | 0.010 ± 0.003 | 0.009 ± 0.003 | 0.016 | - | −0.333 |
| V’O2 peak (%pred) | 0.74 ± 0.14 | 0.68 ± 0.15 | 0.009 | ≥85% pred | −0.414 |
| V’O2 AT (%pred) | 0.48 ± 0.11 | 0.44 ± 0.10 | 0.005 | 40–60% | −0.380 |
| V’E/V’CO2 slope | 26.44 ± 5.18 | 26.76 ± 7.58 | 0.750 | <35 | 0.049 |
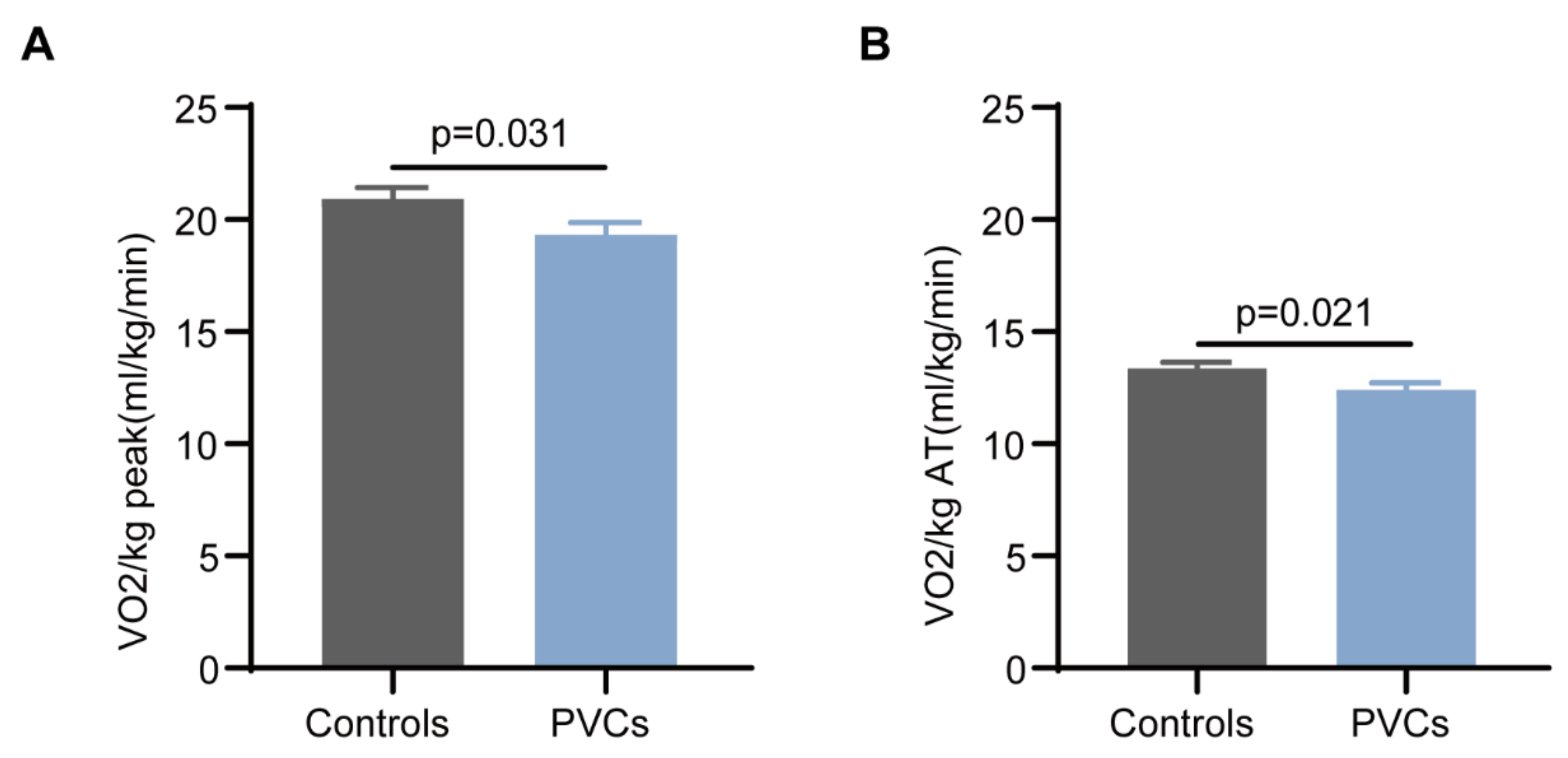
| V’O2/KG AT (ml/kg/min) | 13.36 ± 2.70 | 12.40 ± 3.02 | 0.021 | - | −0.336 |
| V’O2/KG peak (ml/kg/min) | 20.92 ± 4.99 | 19.32 ± 5.20 | 0.031 | - | −0.314 |
| V’E/KG peak (ml/kg/min) | 713.62 ± 155.25 | 657.38 ± 168.60 | 0.017 | - | −0.347 |
| ΔV’O2/ΔWR ((ml/min)/W) | 9.69 ± 1.92 | 8.84 ± 2.66 | 0.013 | >8.6 | −0.368 |
| Post Hoc | |||||||
|---|---|---|---|---|---|---|---|
| Subject | <10,000/24 h (n = 55) | 10,000–20,000/24 h (n = 23) | >20,000/24 h (n = 16) | p value | <10,000/24 h vs. >20,000/24 h | 10,000–20,000/24 h vs. >20,000/24 h | <10,000/24 h vs. 10,000–20,000/24 h |
| AT (l/min) | 0.78 ± 0.25 | 0.88 ± 0.25 | 0.79 ± 0.21 | 0.270 | |||
| V’O2 peak (l/min) | 1.18 ± 0.41 | 1.36 ± 0.36 | 1.35 ± 0.36 | 0.110 | |||
| V’O2 AT (%pred) | 0.45 ± 0.11 | 0.43 ± 0.1 | 0.40 ± 0.08 | 0.289 | |||
| V’O2 peak (%pred) | 0.67 ± 0.16 | 0.66 ± 0.12 | 0.70 ± 0.15 | 0.726 | |||
| V’O2/KG AT (ml/kg/min) | 12.01 ± 3.03 | 13.23 ± 3.61 | 12.7 ± 2.38 | 0.282 | |||
| V’O2/KG peak (ml/kg/min) | 18.18 ± 5.29 | 20.46 ± 5.31 | 21.67 ± 4.34 | 0.040 | 0.023 | 0.490 | 0.090 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, X.; Yan, J.; Liu, W. An Early Indicator in Evaluating Cardiac Dysfunction Related to Premature Ventricular Complexes: Cardiorespiratory Capacity. Healthcare 2023, 11, 2940. https://doi.org/10.3390/healthcare11222940
Ma X, Yan J, Liu W. An Early Indicator in Evaluating Cardiac Dysfunction Related to Premature Ventricular Complexes: Cardiorespiratory Capacity. Healthcare. 2023; 11(22):2940. https://doi.org/10.3390/healthcare11222940
Chicago/Turabian StyleMa, Xiaozhu, Jiangtao Yan, and Wanjun Liu. 2023. "An Early Indicator in Evaluating Cardiac Dysfunction Related to Premature Ventricular Complexes: Cardiorespiratory Capacity" Healthcare 11, no. 22: 2940. https://doi.org/10.3390/healthcare11222940
APA StyleMa, X., Yan, J., & Liu, W. (2023). An Early Indicator in Evaluating Cardiac Dysfunction Related to Premature Ventricular Complexes: Cardiorespiratory Capacity. Healthcare, 11(22), 2940. https://doi.org/10.3390/healthcare11222940