
The Influence of Listening to Preferred versus Non-Preferred Music on Static and Dynamic Balance in Middle-Aged Women

 ,
,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
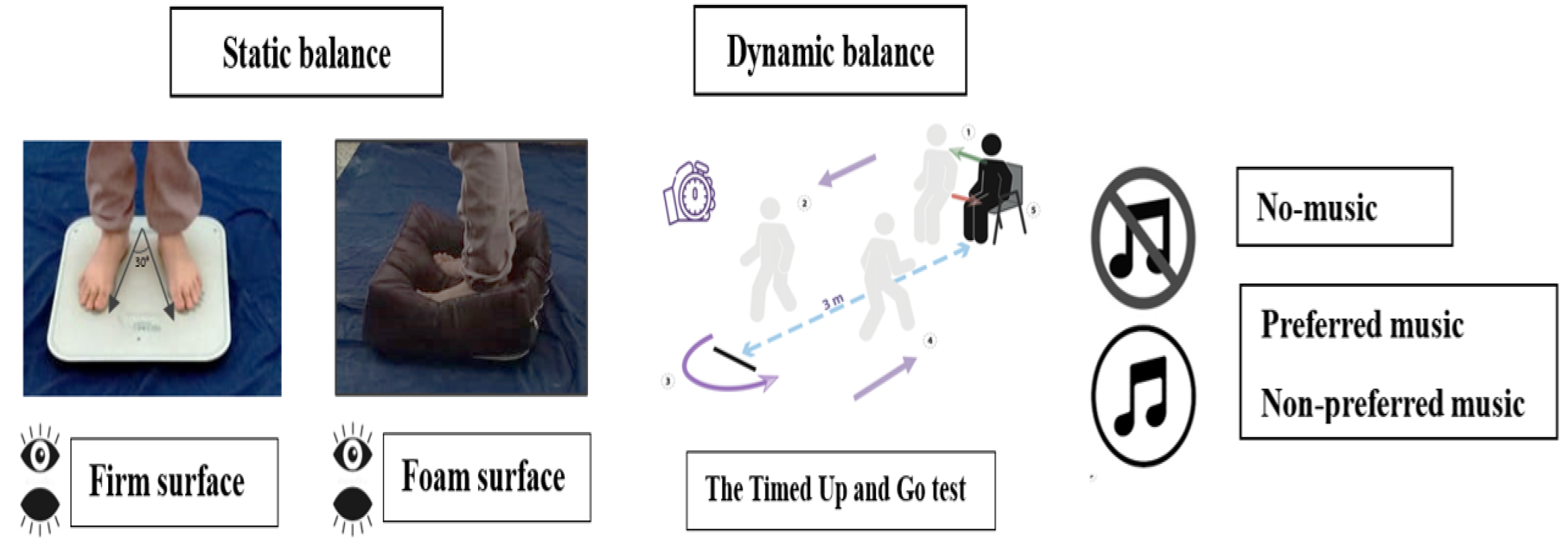
2.3. Postural Balance Assessment
2.3.1. Static Balance
2.3.2. Dynamic Balance
2.4. Statistical Analyses
3. Results
3.1. Static Balance
3.2. Dynamic Balance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Title | Artist | Genre | Tempo | Mode | Energy | Number of Participants | |
|---|---|---|---|---|---|---|---|
| Preferred music | Batwanes Beek | Warda | Classical | 161 BPM | Major | Low energy | 3 |
| Alf Leila We Leila | Umm Kulthum | Classical | 132 BPM | Major | Average energy | 6 | |
| Enta 3omri | Umm Kulthum | Classical | 118 BPM | Major | Average energy | 7 | |
| Elmahfel | Chirine Lajmi | Country | 102 BPM | Minor | High energy | 5 | |
| Miselch Golouh | Chirine Lajmi | Country | 93 BPM | Minor | High energy | 4 | |
| Non-preferred music | Sans Visa | Soulking | Rap | 153 BPM | Minor | High energy | 3 |
| Dima Lebess | Klay BBG | Rap | 190 BPM | Minor | High energy | 4 | |
| Galbi | Samara | Rap | 101 BPM | Minor | High energy | 11 | |
| Cheek To Cheek | Ella Fitzgerald | Jazz | 122 BPM | Major | Low energy | 1 | |
| Sabah Wu Masaa | Fairouz | Jazz | 120 BPM | Major | Average energy | 2 | |
| Kifou Hal Helou | Tania Saleh | Jazz | 104 PRM | Minor | Low energy | 5 |
References
- King, A. Health risks of physical inactivity similar to smoking. Nat. Rev. Cardiol. 2012, 9, 492. [Google Scholar] [CrossRef] [PubMed]
- Wiemers, E.E.; Bianchi, S.M. Competing demands from aging parents and adult children in two cohorts of American women. Popul. Dev. Rev. 2015, 41, 127–146. [Google Scholar] [CrossRef] [PubMed]
- Wassel, J.I.; Cutler, N.E. Yet Another Boomer Challenge for Financial Professionals: The “Senior” Sandwich Generation. J. Financ. Serv. Prof. 2016, 70, 61–73. [Google Scholar]
- Matthews, K.A.; Wing, R.R.; Kuller, L.H.; Meilahn, E.N.; Kelsey, S.F.; Costello, E.J.; Caggiula, A.W. Influences of natural menopause on psychological characteristics and symptoms of middle-aged healthy women. J. Consult. Clin. Psychol. 1990, 58, 345. [Google Scholar] [CrossRef] [PubMed]
- Nitz, J.; Low Choy, N. Changes in activity level in women aged 40–80 years. Climacteric 2007, 10, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Nitz, J.C.; Choy, N.L. The relationship between ankle dorsiflexion range, falls and activity level in women aged 40 to 80 years. N. Z. J. Physiother. 2004, 32, 121–125. [Google Scholar]
- Choy, N.L.; Brauer, S.; Nitz, J. Changes in postural stability in women aged 20 to 80 years. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, M525–M530. [Google Scholar] [CrossRef]
- Wang, S.; Phillips, D.; Lee, J. Disability prevalence in midlife (aged 55–65 years): Cross-Country comparisons of gender differences and time trends. Women’s Midlife Health 2021, 7, 1. [Google Scholar] [CrossRef]
- Muehlbauer, T.; Besemer, C.; Wehrle, A.; Gollhofer, A.; Granacher, U. Relationship between strength, power and balance performance in seniors. Gerontology 2012, 58, 504–512. [Google Scholar] [CrossRef]
- Sobera, M.; Siedlecka, B.; Syczewska, M. Posture control development in children aged 2–7 years old, based on the changes of repeatability of the stability indices. Neurosci. Lett. 2011, 491, 13–17. [Google Scholar] [CrossRef]
- Mack, K.A.; Rudd, R.A.; Mickalide, A.D.; Ballesteros, M.F. Fatal unintentional injuries in the home in the US, 2000–2008. Am. J. Prev. Med. 2013, 44, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Rockett, I.R.; Regier, M.D.; Kapusta, N.D.; Coben, J.H.; Miller, T.R.; Hanzlick, R.L.; Todd, K.H.; Sattin, R.W.; Kennedy, L.W.; Kleinig, J. Leading causes of unintentional and intentional injury mortality: United States, 2000–2009. Am. J. Public Health 2012, 102, e84–e92. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.A.; Corso, P.S.; Finkelstein, E.A.; Miller, T.R. The costs of fatal and non-fatal falls among older adults. Inj. Prev. 2006, 12, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Melton, L.J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Menz, H.B. Physiologic, psychologic, and health predictors of 6-minute walk performance in older people. Arch. Phys. Med. Rehabil. 2002, 83, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Delbaere, K.; Sturnieks, D.L.; Crombez, G.; Lord, S.R. Concern about falls elicits changes in gait parameters in conditions of postural threat in older people. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2009, 64, 237–242. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, ii7–ii11. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Yost, W.A. Relationship between postural stability and spatial hearing. J. Am. Acad. Audiol. 2013, 24, 782–788. [Google Scholar] [CrossRef]
- Schaffert, N.; Janzen, T.B.; Mattes, K.; Thaut, M.H. A review on the relationship between sound and movement in sports and rehabilitation. Front. Psychol. 2019, 10, 244. [Google Scholar] [CrossRef]
- Simpson, S.D.; Karageorghis, C.I. The effects of synchronous music on 400-m sprint performance. J. Sports Sci. 2006, 24, 1095–1102. [Google Scholar] [CrossRef]
- Karageorghis, C.I.; Priest, D.-L. Music in the exercise domain: A review and synthesis (Part I). Int. Rev. Sport Exerc. Psychol. 2012, 5, 44–66. [Google Scholar] [CrossRef] [PubMed]
- Forti, S.; Filipponi, E.; Di Berardino, F.; Barozzi, S.; Cesarani, A. The influence of music on static posturography. J. Vestib. Res. 2010, 20, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Pacchetti, C.; Mancini, F.; Aglieri, R.; Fundarò, C.; Martignoni, E.; Nappi, G. Active music therapy in Parkinson’s disease: An integrative method for motor and emotional rehabilitation. Psychosom. Med. 2000, 62, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Carrick, F.R.; Oggero, E.; Pagnacco, G. Posturographic changes associated with music listening. J. Altern. Complement. Med. 2007, 13, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, T.; Beşli, M.; Ünver, B.; Şengül, Y.S. Influence of different genres of music on static and dynamic balance control of young adults. J. Health Sci. Prof. 2019, 6, 342–349. [Google Scholar] [CrossRef]
- Maclean, L.M.; Brown, L.J.; Astell, A.J. The effect of rhythmic musical training on healthy older adults’ gait and cognitive function. Gerontologist 2014, 54, 624–633. [Google Scholar] [CrossRef] [PubMed]
- De Bartolo, D.; Morone, G.; Giordani, G.; Antonucci, G.; Russo, V.; Fusco, A.; Marinozzi, F.; Bini, F.; Spitoni, G.; Paolucci, S. Effect of different music genres on gait patterns in Parkinson’s disease. Neurol. Sci. 2020, 41, 575–582. [Google Scholar] [CrossRef] [PubMed]
- De Dreu, C.K.; Nijstad, B.A.; Baas, M.; Wolsink, I.; Roskes, M. Working memory benefits creative insight, musical improvisation, and original ideation through maintained task-focused attention. Personal. Soc. Psychol. Bull. 2012, 38, 656–669. [Google Scholar] [CrossRef]
- Sung, H.-C.; Chang, A.M.; Lee, W.-L. A preferred music listening intervention to reduce anxiety in older adults with dementia in nursing homes. J. Clin. Nurs. 2010, 19, 1056–1064. [Google Scholar] [CrossRef]
- Sung, H.-c.; Chang, A.M. Use of preferred music to decrease agitated behaviours in older people with dementia: A review of the literature. J. Clin. Nurs. 2005, 14, 1133–1140. [Google Scholar] [CrossRef]
- Blood, A.J.; Zatorre, R.J. Intensely pleasurable responses to music correlate with activity in brain regions implicated in reward and emotion. Proc. Natl. Acad. Sci. USA 2001, 98, 11818–11823. [Google Scholar] [CrossRef]
- Maatoug, H.; Baccouch, R.; Borji, R.; Rebai, H.; Sahli, S. Effects of music listening on postural balance in adolescents with visual impairment. Percept. Mot. Ski. 2023, 130, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Ballmann, C.G.; McCullum, M.J.; Rogers, R.R.; Marshall, M.R.; Williams, T.D. Effects of preferred vs. nonpreferred music on resistance exercise performance. J. Strength Cond. Res. 2021, 35, 1650–1655. [Google Scholar] [CrossRef] [PubMed]
- Ballmann, C.G.; Maynard, D.J.; Lafoon, Z.N.; Marshall, M.R.; Williams, T.D.; Rogers, R.R. Effects of listening to preferred versus non-preferred music on repeated wingate anaerobic test performance. Sports 2019, 7, 185. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Robb, S.L.; Carpenter, J.S.; Burns, D.S. Reporting guidelines for music-based interventions. J. Health Psychol. 2011, 16, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Fransson, P.-A.; Lush, D.; Gomez, S. The effect of foam surface properties on postural stability assessment while standing. Gait Posture 2008, 28, 649–656. [Google Scholar] [CrossRef]
- Jeka, J.; Kiemel, T.; Creath, R.; Horak, F.; Peterka, R. Controlling human upright posture: Velocity information is more accurate than position or acceleration. J. Neurophysiol. 2004, 92, 2368–2379. [Google Scholar] [CrossRef]
- Paillard, T.; Noé, F. Techniques and methods for testing the postural function in healthy and pathological subjects. BioMed Res. Int. 2015, 2015, 891390. [Google Scholar] [CrossRef]
- Van Parys, J.; Njiokiktjien, C.J. Romberg’s sign expressed in a quotient. Agressol. Rev. Int. Physio-Biol. Pharmacol. Appl. Eff. L’agression 1976, 17, 95–99. [Google Scholar]
- Gago, M.F.; Fernandes, V.; Ferreira, J.; Yelshyna, D.; Silva, H.D.; Rodrigues, M.L.; Rocha, L.; Bicho, E.; Sousa, N. Role of the visual and auditory systems in postural stability in Alzheimer’s disease. J. Alzheimer’s Dis. 2015, 46, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Vereeck, L.; Wuyts, F.; Truijen, S.; Van de Heyning, P. Clinical assessment of balance: Normative data, and gender and age effects. Int. J. Audiol. 2008, 47, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Bouchaala, F.; Laatar, R.; Lahiani, M.; Zouabi, A.; Borji, R.; Rebai, H.; Sahli, S. Time of day effect on balance performance, functional capacities and risk of fall in women with rheumatoid arthritis. Chronobiol. Int. 2020, 37, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.N.; Carroll, S.G.; Reddihough, D.S.; Phillips, B.A.; Galea, M.P. Investigation of the Timed ‘Up & Go’ test in children. Dev. Med. Child Neurol. 2005, 47, 518–524. [Google Scholar] [CrossRef]
- McHugh, M.L. Multiple comparison analysis testing in ANOVA. Biochem. Medica 2011, 21, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Steiger, J.H. Beyond the F test: Effect size confidence intervals and tests of close fit in the analysis of variance and contrast analysis. Psychol. Methods 2004, 9, 164. [Google Scholar] [CrossRef]
- Boso, M.; Politi, P.; Barale, F.; Emanuele, E. Neurophysiology and neurobiology of the musical experience. Funct. Neurol. 2006, 21, 187. [Google Scholar]
- Satoh, M.; Takeda, K.; Nagata, K.; Hatazawa, J.; Kuzuhara, S. The anterior portion of the bilateral temporal lobes participates in music perception: A positron emission tomography study. Am. J. Neuroradiol. 2003, 24, 1843–1848. [Google Scholar]
- Dieterich, M.; Bense, S.; Lutz, S.; Drzezga, A.; Stephan, T.; Bartenstein, P.; Brandt, T. Dominance for vestibular cortical function in the non-dominant hemisphere. Cereb. Cortex 2003, 13, 994–1007. [Google Scholar] [CrossRef]
- Popescu, M.; Otsuka, A.; Ioannides, A.A. Dynamics of brain activity in motor and frontal cortical areas during music listening: A magnetoencephalographic study. Neuroimage 2004, 21, 1622–1638. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Chong, H.J. A comparative study of the perception of music emotion between adults with and without visual impairment. Psychol. Music 2019, 47, 225–240. [Google Scholar] [CrossRef]
- Terry, P.C.; Karageorghis, C.I.; Saha, A.M.; D’Auria, S. Effects of synchronous music on treadmill running among elite triathletes. J. Sci. Med. Sport 2012, 15, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Lingham, J.; Theorell, T. Self-selected “favourite” stimulative and sedative music listening–how does familiar and preferred music listening affect the body? Nord. J. Music Ther. 2009, 18, 150–166. [Google Scholar] [CrossRef]
- Teasdale, N.; Simoneau, M. Attentional demands for postural control: The effects of aging and sensory reintegration. Gait Posture 2001, 14, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Maylor, E.A.; Wing, A.M. Age differences in postural stability are increased by additional cognitive demands. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1996, 51, P143–P154. [Google Scholar] [CrossRef] [PubMed]
- Ben Waer, F.; Laatar, R.; Srihi, S.; Jouira, G.; Rebai, H.; Sahli, S. Acute effects of low versus high caffeine dose consumption on postural balance in middle-aged women. J. Women Aging 2020, 33, 620–634. [Google Scholar] [CrossRef] [PubMed]
- Brauer, S.G.; Woollacott, M.; Shumway-Cook, A. The interacting effects of cognitive demand and recovery of postural stability in balance-impaired elderly persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M489–M496. [Google Scholar] [CrossRef]
- Roe, B.; Howell, F.; Riniotis, K.; Beech, R.; Crome, P.; Ong, B.N. Older people’s experience of falls: Understanding, interpretation and autonomy. J. Adv. Nurs. 2008, 63, 586–596. [Google Scholar] [CrossRef]
- Goltz, F.; Sadakata, M. Do you listen to music while studying? A portrait of how people use music to optimize their cognitive performance. Acta Psychol. 2021, 220, 103417. [Google Scholar] [CrossRef]
- Johansson, R.; Holmqvist, K.; Mossberg, F.; Lindgren, M. Eye movements and reading comprehension while listening to preferred and non-preferred study music. Psychol. Music 2012, 40, 339–356. [Google Scholar] [CrossRef]
- Salamé, P.; Baddeley, A. Effects of background music on phonological short-term memory. Q. J. Exp. Psychol. 1989, 41, 107–122. [Google Scholar] [CrossRef]
- Ross, J.M.; Warlaumont, A.S.; Abney, D.H.; Rigoli, L.M.; Balasubramaniam, R. Influence of musical groove on postural sway. J. Exp. Psychol. Hum. Percept. Perform. 2016, 42, 308. [Google Scholar] [CrossRef]
- Ben Waer, F.; Laatar, R.; Jouira, G.; Lahiani, M.; Rebai, H.; Sahli, S. Effects of 12 weeks of caffeine supplementation and Zumba training on postural balance and cognitive performances in middle-aged women. Health Care Women Int. 2023, 6, 1–21. [Google Scholar] [CrossRef]


| No-Music | Preferred Music | Non-Preferred Music | |
|---|---|---|---|
| Firm Surface | |||
| EO | 8.06 ± 1.24 | 6.96 ± 0.72 + | 8.27 ± 1.28 £ |
| EC | 9.49 ± 1.21 # | 9.36 ±1.12 # | 11.06 ± 1.71 **#££ |
| Foam Surface | |||
| EO | 10.25 ± 1.4 $ | 10.28 ± 1.39 $ | 11.76 ± 2.2 **#££ |
| EC | 13.52 ± 1.5 #$ | 13.45 ± 2.15 #$ | 16.34 ± 2.3 **#$££ |
| TUGT (scores) | 7.66 ± 0.6 | 7.26 ± 0.65 + | 7.88 ± 0.68 *££ |
| RI1-Auditory Contribution (EOA/EO) | RI2-Auditory Contribution with EC (ECA/EC) | |||
|---|---|---|---|---|
| Preferred Music | Non-Preferred Music | Preferred Music | Non-Preferred Music | |
| Firm Surface | −13.55% (0.15) | 6.64% (0.28) ** | −0.07% (0.16) | 20.09% (0.23) * |
| Foam Surface | 2.33% (0.19) | 19.13% (0.29) *** | 0.66% (0.21) | 23.34% (0.18) *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waer, F.B.; Alexe, C.I.; Tohănean, D.I.; Čaušević, D.; Alexe, D.I.; Sahli, S. The Influence of Listening to Preferred versus Non-Preferred Music on Static and Dynamic Balance in Middle-Aged Women. Healthcare 2023, 11, 2681. https://doi.org/10.3390/healthcare11192681
Waer FB, Alexe CI, Tohănean DI, Čaušević D, Alexe DI, Sahli S. The Influence of Listening to Preferred versus Non-Preferred Music on Static and Dynamic Balance in Middle-Aged Women. Healthcare. 2023; 11(19):2681. https://doi.org/10.3390/healthcare11192681
Chicago/Turabian StyleWaer, Fatma Ben, Cristina Ioana Alexe, Dragoș Ioan Tohănean, Denis Čaušević, Dan Iulian Alexe, and Sonia Sahli. 2023. "The Influence of Listening to Preferred versus Non-Preferred Music on Static and Dynamic Balance in Middle-Aged Women" Healthcare 11, no. 19: 2681. https://doi.org/10.3390/healthcare11192681
APA StyleWaer, F. B., Alexe, C. I., Tohănean, D. I., Čaušević, D., Alexe, D. I., & Sahli, S. (2023). The Influence of Listening to Preferred versus Non-Preferred Music on Static and Dynamic Balance in Middle-Aged Women. Healthcare, 11(19), 2681. https://doi.org/10.3390/healthcare11192681