
Factors Associated with Burnout in Medical Staff: A Look Back at the Role of the COVID-19 Pandemic


 ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Setting
2.2. Study Population
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Data Collection and Measures
2.3.1. Procedure
2.3.2. The Screening Tool
2.4. Data Analysis
3. Results
- A. The demographic data of our group are presented in Table 1.
- B. Correlations between burn-out level and pandemic/non-pandemic stressors
- (1)
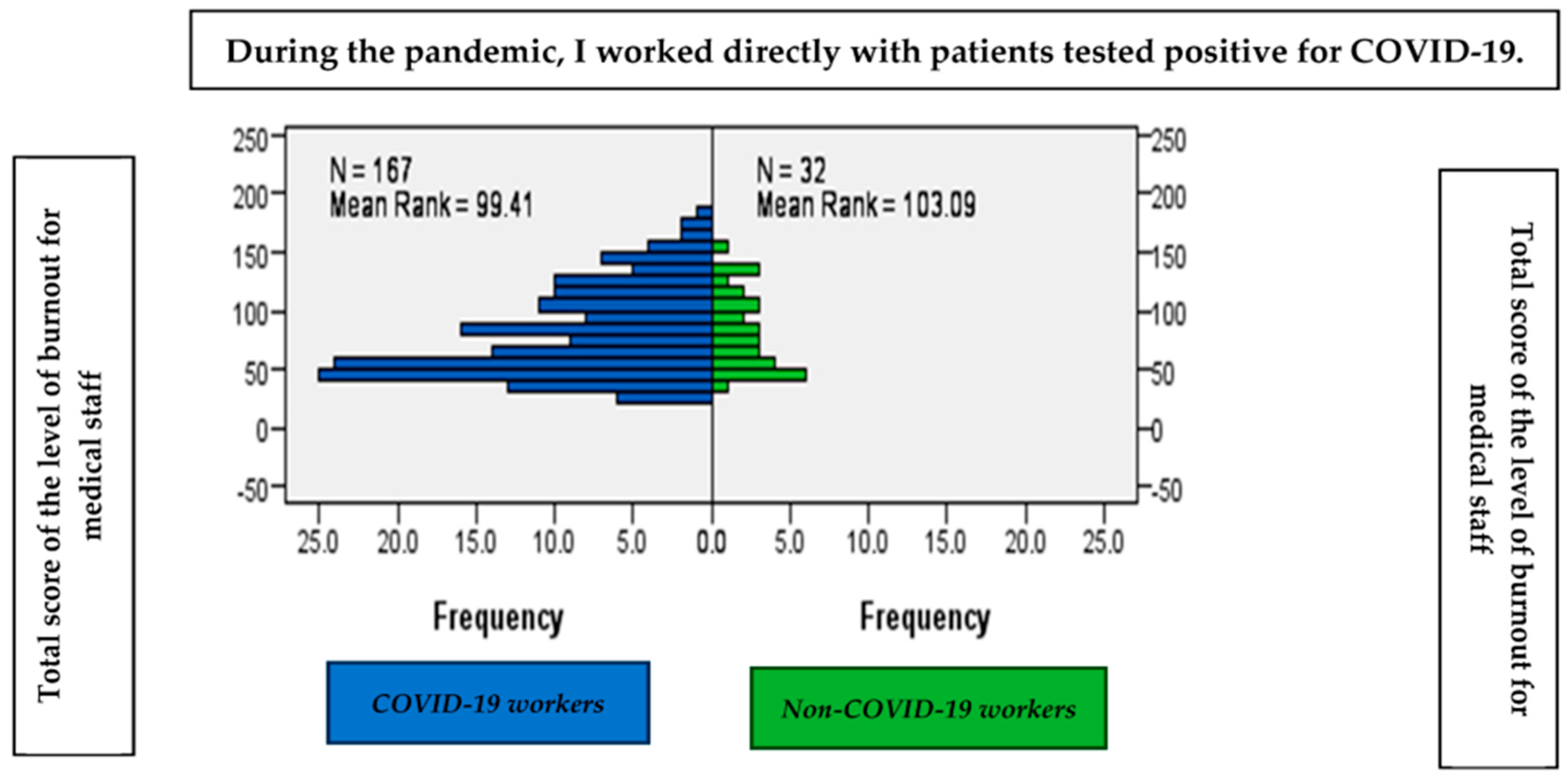
- Degree of exposure
- (2)
- Pandemic stressors associated with burnout in all medical staff and those on the front line
- (3)
- Total burnout score for those working with COVID-19: nonspecific variables
4. Discussion
5. Conclusions
5.1. Research Limitations
5.2. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Freudenberger, H.J. The staff burn-out syndrome in alternative institutions. Psychotherapy 1975, 12, 73–82. [Google Scholar] [CrossRef]
- Freudenberger, H.J. Burn-out: Occupational hazard of the child care worker. Child Care Q. 1977, 6, 90–99. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory. In Evaluating Stress: A Book of Resources, 3rd ed.; Zalaquett, C.P., Wood, R.J., Eds.; Scarecrow Education: Lanham, MD, USA, 1997; pp. 191–218. [Google Scholar]
- Shields, K.; Somerville, P. In the Tiger’s Mouth: An Empowerment Guide for Social Action; New Society Publishers: Gabriola Island, BC, Canada, 1993; p. 130. [Google Scholar]
- Leiter, M.P.; Schaufeli, W.B. Consistency of the burnout construct across occupations. Anxiety Stress Coping 1996, 9, 229–243. [Google Scholar] [CrossRef]
- Wong, A.M.F. Beyond burnout: Looking deeply into physician distress. Can. J. Ophthalmol. 2020, 55 (Suppl. S1), 7–16. [Google Scholar] [CrossRef]
- Yung, M.; Du, B.; Gruber, J.; Yazdani, A. Developing a Canadian fatigue risk management standard for first responders: Defining the scope. Saf. Sci. 2021, 134, 105044. [Google Scholar] [CrossRef]
- Zhou, A.Y.; Panagioti, M.; Esmail, A.; Agius, R.; Van Tongeren, M.; Bower, P. Factors Associated with Burnout and Stress in Trainee Physicians: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2013761. [Google Scholar] [CrossRef]
- Gunawan, J.; Aungsuroch, Y.; Fisher, M.L.; Marzilli, C.; Liu, Y. Factors Related to the Clinical Competence of Registered Nurses: Systematic Review and Meta-Analysis. J. Nurs. Scholarsh. 2020, 52, 623–633. [Google Scholar] [CrossRef]
- Kansoun, Z.; Boyer, L.; Hodgkinson, M.; Villes, V.; Lançon, C.; Fond, G. Burnout in French physicians: A systematic review and meta-analysis. J. Affect. Disord. 2019, 246, 132–147. [Google Scholar] [CrossRef]
- Rothenberger, D.A. Physician Burnout and Well-Being: A Systematic Review and Framework for Action. Dis. Colon Rectum 2017, 60, 567–576. [Google Scholar] [CrossRef]
- Hu, Z.; Wang, H.; Xie, J.; Zhang, J.; Li, H.; Liu, S.; Li, Q.; Yang, Y.; Huang, Y. Burnout in ICU doctors and nurses in mainland China-A national cross-sectional study. J. Crit. Care 2021, 62, 265–270. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar] [CrossRef]
- De Hert, S. Burnout in Healthcare Workers: Prevalence, Impact and Preventative Strategies. Local Reg. Anesth. 2020, 13, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Zhou, F.C.; Xu, S.W.; Zhang, Q.; Ng, C.H.; Ungvari, G.S.; Xiang, Y.T. Prevalence of suicide-related behaviors among physicians: A systematic review and meta-analysis. Suicide Life Threat. Behav. 2020, 50, 1264–1275. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.S.; Bachu, R.; Adikey, A.; Malik, M.; Shah, M. Factors Related to Physician Burnout and Its Consequences: A Review. Behav. Sci. 2018, 8, 98. [Google Scholar] [CrossRef]
- Serrano-Ripoll, M.J.; Meneses-Echavez, J.F.; Ricci-Cabello, I.; Fraile-Navarro, D.; Fiol-deRoque, M.A.; Pastor-Moreno, G.; Castro, A.; Ruiz-Pérez, I.; Zamanillo Campos, R.; Gonçalves-Bradley, D.C. Impact of viral epidemic outbreaks on mental health of healthcare workers: A rapid systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 347–357. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Fujino, J.; Shiwaku, H.; Miyajima, M.; Doi, S.; Hirai, N.; Jitoku, D.; Takagi, S.; Tamura, T.; Maruo, T.; et al. Factors affecting mental illness and social stress in hospital workers treating COVID-19: Paradoxical distress during pandemic era. J. Psychiatr. Res. 2021, 137, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Athanasiou, N.; Sakkas, N.; Patrinos, S.; Sakka, E.; Barmparessou, Z.; Tsikrika, S.; Adraktas, A.; Pataka, A.; Migdalis, I.; et al. From Recession to Depression? Prevalence and Correlates of Depression, Anxiety, Traumatic Stress and Burnout in Healthcare Workers during the COVID-19 Pandemic in Greece: A Multi-Center, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 2390. [Google Scholar] [CrossRef]
- Thatrimontrichai, A.; Weber, D.J.; Apisarnthanarak, A. Mental health among healthcare personnel during COVID-19 in Asia: A systematic review. J. Formos. Med. Assoc. 2021, 120, 1296–1304. [Google Scholar] [CrossRef]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi, R.S. Burnout among Healthcare Providers of COVID-19; a Systematic Review of Epidemiology and Recommendations. Arch. Acad. Emerg. Med. 2021, 9, e7. [Google Scholar]
- Zhang, X.J.; Song, Y.; Jiang, T.; Ding, N.; Shi, T.Y. Interventions to reduce burnout of physicians and nurses: An overview of systematic reviews and meta-analyses. Medicine 2020, 99, e20992. [Google Scholar] [CrossRef]
- Chen, J.; Liu, X.; Wang, D.; Jin, Y.; He, M.; Ma, Y.; Zhao, X.; Song, S.; Zhang, L.; Xiang, X.; et al. Risk factors for depression and anxiety in healthcare workers deployed during the COVID-19 outbreak in China. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Shanafelt, T.D.; Johnson, P.O.; Johnson, L.A.; Satele, D.; West, C.P. A cross-sectional study exploring the relationship between burnout, absenteeism, and job performance among American nurses. BMC Nurs. 2019, 18, 57. [Google Scholar] [CrossRef] [PubMed]
- Elshaer, N.S.M.; Moustafa, M.S.A.; Wagdy, M.A.; Ramadan, M.I.E. Job Stress and Burnout Syndrome among Critical Care Healthcare Workers. Alex. J. Med. 2018, 3, 273–277. [Google Scholar] [CrossRef]
- Zhou, Q.; Lai, X.; Wan, Z.; Zhang, X.; Tan, L. Impact of burnout, secondary traumatic stress and compassion satisfaction on hand hygiene of healthcare workers during the COVID-19 pandemic. Nurs. Open 2021, 8, 2551–2557. [Google Scholar] [CrossRef]
- Albott, C.S.; Wozniak, J.R.; McGlinch, B.P.; Wall, M.H.; Gold, B.S.; Vinogradov, S. Battle Buddies: Rapid Deployment of a Psychological Resilience Intervention for Health Care Workers During the COVID-19 Pandemic. Anesth. Analg. 2020, 131, 43–54. [Google Scholar] [CrossRef]
- Alexa-Stratulat, T.; Neagu, M.; Neagu, A.I.; Alexa, I.D.; Ioan, B.G. Consent for participating in clinical trials—Is it really informed? Dev. World Bioeth. 2018, 18, 299–306. [Google Scholar] [CrossRef]
- Navinés, R.; Olivé, V.; Fonseca, F.; Martín-Santos, R. Work stress and resident burnout, before and during the COVID-19 pandemia: An up-date. Med. Clin. 2021, 157, 130–140. [Google Scholar] [CrossRef]
- Shah, K.; Chaudhari, G.; Kamrai, D.; Lail, A.; Patel, R.S. How Essential Is to Focus on Physician’s Health and Burnout in Coronavirus (COVID-19) Pandemic? Cureus 2020, 12, e7538. [Google Scholar] [CrossRef]
- Lasalvia, A.; Amaddeo, F.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Bonetto, C. Levels of burn-out among healthcare workers during the COVID-19 pandemic and their associated factors: A cross-sectional study in a tertiary hospital of a highly burdened area of north-east Italy. BMJ Open 2021, 11, e045127. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Assiri, H.; Alharbi, H.Y.; Nasser, A.; Alkhamees, M.A. Burnout and depression among psychiatry residents during COVID-19 pandemic. Hum. Resour. Health 2021, 19, 46. [Google Scholar] [CrossRef]
- Treluyer, L.; Tourneux, P. Burnout among paediatric residents during the COVID-19 outbreak in France. Eur. J. Pediatr. 2021, 180, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Murat, M.; Köse, S.; Savaşer, S. Determination of stress, depression and burnout levels of front-line nurses during the COVID-19 pandemic. Int. J. Ment. Health Nurs. 2021, 30, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Kachadourian, L.K.; Feder, A.; Murrough, J.W.; Feingold, J.H.; Kaye-Kauderer, H.; Charney, D.; Southwick, S.M.; Peccoralo, L.; Ripp, J.; Pietrzak, R.H. Transdiagnostic Psychiatric Symptoms, Burnout, and Functioning in Frontline Health Care Workers Responding to the COVID-19 Pandemic: A Symptomics Analysis. J. Clin. Psychiatry 2021, 82, 20m13766. [Google Scholar] [CrossRef] [PubMed]
- Babamiri, M.; Bashirian, S.; Khazaei, S.; Sohrabi, M.S.; Heidarimoghadam, R.; Mortezapoor, A.; Zareian, S. Burnout and Mental Health of COVID-19 Frontline Healthcare Workers: Results from an Online Survey. Iran. J. Psychiatry 2022, 17, 136–143. [Google Scholar] [CrossRef]
- Melnikow, J.; Padovani, A.; Miller, M. Frontline physician burnout during the COVID-19 pandemic: National survey findings. BMC Health Serv. Res. 2022, 22, 365. [Google Scholar] [CrossRef]
- Mosolova, E.; Sosin, D.; Mosolov, S. Stress, anxiety, depression and burnout in frontline healthcare workers during two peaks of COVID-19 pandemic in Russia. Psychiatry Res. 2021, 306, 114226. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, J.; Hao, Y.; Wu, K.; Jiao, M.; Liang, L.; Gao, L.; Ning, N.; Kang, Z.; Shan, L.; et al. Prevalence and Factors Associated with Burnout of Frontline Healthcare Workers in Fighting Against the COVID-19 Pandemic: Evidence From China. Front. Psychol. 2021, 12, 680614. [Google Scholar] [CrossRef]
- Pereira-Lima, K.; Loureiro, S.R.; Silveira, I.L.M.; Crippa, J.A.; Hallak, J.E.C.; Zuardi, A.W.; Osório, F.L. Workplace Protections and Burnout Among Brazilian Frontline Health Care Professionals During the COVID-19 Pandemic. Front. Psychol. 2022, 13, 880049. [Google Scholar] [CrossRef]
- Wang, H.; Zhou, X.; Jia, X.; Song, C.; Luo, X.; Zhang, H.; Wu, H.; Ye, J. Emotional exhaustion in front-line healthcare workers during the COVID-19 pandemic in Wuhan, China: The effects of time pressure, social sharing and cognitive appraisal. BMC Public Health 2021, 21, 829. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Mazzi, M.; Wu, A.W.; Rimondini, M. What We Have Learned from Two Decades of Epidemics and Pandemics: A Systematic Review and Meta-Analysis of the Psychological Burden of Frontline Healthcare Workers. Psychother. Psychosom. 2021, 90, 178–190. [Google Scholar] [CrossRef]
- Marvaldi, M.; Mallet, J.; Dubertret, C.; Moro, M.R.; Guessoum, S.B. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 126, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Talaee, N.; Varahram, M.; Jamaati, H.; Salimi, A.; Attarchi, M.; Kazempour Dizaji, M.; Sadr, M.; Hassani, S.; Farzanegan, B.; Monjazebi, F.; et al. Stress and burnout in health care workers during COVID-19 pandemic: Validation of a questionnaire. Z. Gesundh. Wiss. 2022, 30, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Wei, J.; Zhu, H.; Duan, Y.; Geng, W.; Hong, X.; Jiang, J.; Zhao, X.; Zhu, B. A Study of Basic Needs and Psychological Wellbeing of Medical Workers in the Fever Clinic of a Tertiary General Hospital in Beijing during the COVID-19 Outbreak. Psychother. Psychosom. 2020, 89, 252–254. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.T.; Seo, B.; Hladkyj, S.; Lovell, B.L.; Schwartzmann, L. Correlates of physician burnout across regions and specialties: A meta-analysis. Hum. Resour. Health 2013, 11, 48. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Singh, R.; Subedi, M. COVID-19 and stigma: Social discrimination towards frontline healthcare providers and COVID-19 recovered patients in Nepal. Asian J. Psychiatr. 2020, 53, 102222. [Google Scholar] [CrossRef]
- Gupta, S.; Sahoo, S. Pandemic and mental health of the front-line healthcare workers: A review and implications in the Indian context amidst COVID-19. Gen. Psychiatr. 2020, 33, e100284. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef]
- Demerouti, E. Individual strategies to prevent burnout. In Burnout at Work: A Psychological Perspective; Leiter, M.P., Bakker, A.B., Maslach, C., Eds.; Psychology Press: London, UK, 2014; pp. 32–55. [Google Scholar]
- Leiter, M.P.; Maslach, C. Interventions to prevent and alleviate burnout. In Burnout at Work: A Psychological Perspective; Leiter, M.P., Bakker, A.B., Maslach, C., Eds.; Psychology Press: London, UK, 2014; pp. 145–167. [Google Scholar]
- Restauri, N.; Sheridan, A.D. Burnout and Posttraumatic Stress Disorder in the Coronavirus Disease 2019 (COVID-19) Pandemic: Intersection, Impact, and Interventions. J. Am. Coll. Radiol. 2020, 17, 921–926. [Google Scholar] [CrossRef]


{kind=link}
| COVID-19 Healthcare Staff | Non-COVID-19 Healthcare Staff | p | r | ||
|---|---|---|---|---|---|
| Total workers | 167 (83.91%) | 32 (16%) | |||
| Sex | Female | 150 (89.82%) | 30 (93.75%) | 0.488 | 0.491 |
| Male | 17 (10.18%) | 2 (6.25%) | |||
| Workplace location | Rural | 14 (8.38%) | 2 (6.25%) | 0.685 | 0.686 |
| Urban | 153 (91.62%) | 30 (93.75%) | |||
| Profession | Senior doctor | 43 (25.75%) | 10 (31.25%) | 0.045 | 0.047 |
| Resident doctor | 70 (41.92%) | 13 (40.63%) | |||
| Nurse | 47 (28.14%) | 6 (18.75%) | |||
| Orderly | 6 (3.59%) | 0 (0%) | |||
| Auxiliary personnel | 1 (0.6%) | 3 (9.38%) | |||
| Work type | Hospital | 152 (91.02%) | 23 (71.88%) | ||
| Ambulatory | 9 (5.39%) | 7 (21.88%) | 0.015 | 0.003 | |
| Ambulance | 6 (3.59%) | 2 (6.25%) | |||
| Workplace seniority | ≤5 years’ experience | 84 (50.3%) | 18 (56.25%) | ||
| >5 years’ experience | 83 (49.7%) | 14 (43.75%) | 0.480 | 0.163 | |
| Marital status | Married | 92 (55.09%) | 20 (62.5%) | ||
| Divorced | 9 (5.39%) | 1 (3.13%) | |||
| In a relationship | 47 (28.14%) | 7 (21.88%) | 0.555 | 0.525 | |
| Single | 22 (13.17%) | 4 (12.5%) | |||
| Living conditions | House | 49 (29.34%%) | 6 (18.75%) | 0.221 | 0.222 |
| Apartment | 118 (70.66%) | 26 (81.25%) | |||
| Children in care | With | 73 (43.71%) | 13 (40.63%) | 0.671 | 0.730 |
| Without | 94 (56.29%) | 19 (59.38%) | |||
| Seniors in care | With | 32 (19.16%) | 3 (9.38%) | 0.111 | 0.158 |
| Without | 135 (80.84%) | 29 (90.63%) | |||
| COVID-19 Generated Stress Factors | All Medical Staff | Working with COVID-19 Medical Staff | ||
|---|---|---|---|---|
| p | r | p | r | |
| Lack of medical resources | ||||
| During the COVID-19 period, protective equipment was limited. | 0.01 | 0.358 | 0.585 | −0.043 |
| During the COVID-19, I had to improvise or buy protective equipment. | 0.01 | 0.303 | 0.247 | −0.090 |
| Lately, I have had difficulty coping with the lack of material resources, in the context of the increased volume of work | 0.111 | 0.113 | 0.379 | 0.069 |
| There were periods when sanitizing solutions were limited. | 0.01 | 0.370 | 0.711 | 0.029 |
| Lately, I’ve been frustrated because there weren’t enough machines to help infected patients breathe | 0.871 | −0.012 | 0.655 | −0.035 |
| Poor workplace quality of life | ||||
| I felt exasperation due to prolonged wearing of protective equipment | 0.436 | −0.055 | 0.257 | −0.088 |
| Recently, I have endured high temperatures, in the context of using protective equipment | 0.194 | 0.092 | 0.878 | −0.012 |
| Lately I have not been properly hydrated in the context of using protective equipment | 0.305 | 0.073 | 0.490 | 0.054 |
| Lately, I haven’t been able to eat at work, due to the COVID-19 restrictions | 0.081 | −0.124 | 0.148 | −0.112 |
| I had to endure repeated testing for the detection of SARS-CoV-2 | 0.018 | 0.168 | 0.063 | 0.144 |
| I feel that the last period has affected my quality of life | 0.421 | 0.057 | 0.413 | 0.064 |
| Recently, the relationship with work colleagues has deteriorated | 0.836 | 0.015 | 0.833 | −0.016 |
| I felt alone in the fight against COVID-19 while my colleagues were avoiding | 0.017 | 0.169 | 0.255 | 0.089 |
| Lately, I have felt extra pressure because I work in a prestigious hospital | 0.283 | 0.076 | 0.300 | 0.081 |
| Worsening of personal life quality | ||||
| During COVID-19, I had to isolate myself from family and friends | 0.644 | 0.033 | 0.212 | −0.097 |
| Lately, I have tended to drink more alcohol than before | 0.257 | 0.081 | 0.186 | 0.103 |
| Lately, I have had a tendency to use narcotics | 0.958 | −0.004 | 0.688 | −0.031 |
| Lately, the relationship with my family has worsened | 0.196 | 0.092 | 0.118 | 0.122 |
| Lately, I have had to avoid meetings with relatives and friends | 0.750 | −0.023 | 0.758 | −0.024 |
| I had to care for close relatives who were infected | 0.232 | 0.085 | 0.902 | 0.010 |
| Limiting of free time | ||||
| Lately, the number of free days available to me has decreased | 0.854 | −0.013 | 0.689 | −0.031 |
| Lately, I’ve been working a lot of overtime. | 0.01 | 0.407 | 0.707 | 0.029 |
| In the last period, I worked extra shifts, to replace colleagues infected with SARS-CoV-2 | 0.067 | 0.130 | 0.468 | 0.057 |
| Lately, I felt that the system in which I work is willing to sacrifice me according to its own goals | 0.714 | 0.026 | 0.393 | −0.067 |
| Fears in relation to the COVID-19 pandemic | ||||
| Lately, I have been living with the fear of getting infected with SARS-CoV-2. | 0.01 | 0.379 | 0.935 | 0.006 |
| Lately, I was afraid of transmitting the SARS-CoV-2 infection. | 0.01 | 0.408 | 0.603 | −0.041 |
| During the quarantine, I felt insecure about what was to come. | 0.01 | 0.498 | 0.603 | 0.041 |
| The fact that I have associated diseases made me feel the fear of contacting the infection | 0.459 | −0.053 | 0.922 | −0.008 |
| Lately, any pharyngeal pain made me think that I had contacted the SARS-CoV-2 infection. | 0.01 | 0.315 | 0.790 | −0.021 |
| I feel that I have been exposed more than other colleagues to the risk of infection | 0.154 | 0.101 | 0.481 | 0.055 |
| I was concerned when I saw the increasing number of COVID-19 cases | 0.455 | −0.053 | 0.670 | −0.033 |
| I felt fear when I had to take over the shifts of infected colleagues | 0.221 | 0.087 | 0.963 | −0.004 |
| I felt anxiety when close colleagues fell ill | 0.088 | −0.021 | 0.194 | −0.101 |
| I felt like I had to fend for myself the whole time I was working with positive patients | 0.304 | 0.073 | 0.551 | −0.046 |
| I was scared by the increased incidence of COVID-19 cases in the local area | 0.967 | −0.003 | 0.965 | 0.003 |
| During the time I worked with positive patients, I was afraid of being marginalized | 0.008 | 0.187 | 0.208 | 0.084 |
| Work environment reorganization | ||||
| Lately, I felt affected by the reorganization of intra-hospital circuits. | 0.01 | 0.417 | 0.253 | 0.089 |
| I feel uncertain about the effectiveness of infection control measures, given the frequent changes in action protocols | 0.582 | −0.039 | 0.989 | −0.001 |
| Recently, the environment in which I worked has changed substantially | 0.701 | −0.027 | 0.187 | −0.103 |
| Recently, I have been exposed to aerosol-generating procedures and invasive resuscitation interventions (tracheostomy, oro-tracheal intubation). | 0.083 | 0.123 | 0.333 | 0.075 |
| I worked in quarantine areas for a long time | 0.160 | 0.100 | 0.983 | −0.002 |
| I was affected by the loss of records of old patients, in the context of the restrictions | 0.671 | 0.030 | 0.857 | 0.014 |
| I received the appropriate income increase for the degree of exposure to COVID-19 and the work performed | 0.101 | 0.116 | 0.251 | 0.089 |
| Lack of information and experience on COVID-19 | ||||
| I feel dissatisfaction that there is not enough information about the complications and total eradication of COVID-19 | 0.927 | −0.007 | 0.411 | −0.064 |
| I had the feeling that the system in which I work is not prepared to fight the infection with SARS-CoV-2. | 0.01 | 0.419 | 0.628 | −0.038 |
| My lack of experience in caring for patients with COVID-19 worried me. | 0.01 | 0.364 | 0.030 | −0.168 |
| I feel uncertainty about how the condition of each patient with COVID-19 will evolve | 0.254 | −0.081 | 0.500 | −0.053 |
| I felt worried at the thought that there is no treatment to combat COVID-19 | 0.124 | −0.109 | 0.271 | −0.086 |
| I experienced a sense of frustration following the misinformation about COVID-19 spread by the media | 0.725 | −0.025 | 0.326 | −0.076 |
| Worsening of medical care quality | ||||
| The relationship with patients has become difficult due to false information spread by the media | 0.869 | −0.012 | 0.885 | −0.011 |
| During COVID-19, I had to give care primarily to patients who had a better chance of survival | 0.034 | 0.150 | 0.313 | 0.079 |
| Recently, I have faced many cases of deaths among patients | 0.517 | 0.046 | 0.432 | −0.061 |
| Lately, I have experienced increased suffering among the sick | 0.612 | 0.036 | 0.689 | −0.031 |
| I had periods when the number of patients with COVID-19 that I was dealing with increased substantially | 0.941 | −0.005 | 0.030 | −0.168 |
| Lately, I have interacted more than ever with desperate families of patients | 0.634 | 0.034 | 0.587 | −0.042 |
| Lately, communication with patients has been much more difficult, in the context of the use of protective masks | 0.723 | −0.025 | 0.336 | −0.075 |
| Non-Pandemic Stressor Factors for Medical Staff Working with COVID-19 | p | r |
|---|---|---|
| Poor workplace quality of life | ||
| I have been working with depressed patients for a long time | 0.162 | −0.109 |
| I feel a lot of pressure from the hospital management | 0.694 | 0.031 |
| I face a routine in the activities carried out at work | 0.795 | −0.020 |
| I often interact with violent patients | 0.214 | −0.097 |
| At work I encounter conflicting situations with colleagues | 0.552 | 0.046 |
| I always feel that I have to do many things in a short time | 0.749 | −0.025 |
| I felt harassed at work | 0.936 | −0.06 |
| I felt discriminated against because of my ethnicity | 0.770 | 0.023 |
| When making decisions at work I must consult my superiors | 0.600 | −0.041 |
| I always interact with patients who are uncooperative or question what I tell them | 0.263 | −0.087 |
| I am always faced with unrealistic expectations from patients | 0.865 | −0.013 |
| Personal life implications | ||
| Patients call me constantly, including at home and even at night | 0.870 | 0.013 |
| I have a social life | 0.272 | −0.086 |
| In my free time I always think about patients’ cases | 0.244 | −0.091 |
| I suffer from psychiatric conditions for which I take medication | 0.008 | 0.204 |
| Exaggerated bureaucratic work | ||
| I deal more with medical documents than with patients | 0.376 | −0.069 |
| It bothers me that I have to deal with the administrative side as well, not just the patients | 0.946 | −0.05 |
| Ethical issues and self-culpability | ||
| I am constantly afraid of making a mistake that could cost a patient’s life | 0.491 | −0.054 |
| I care more about patients than family | 0.768 | −0.023 |
| I feel the pressure of my responsibility to patients all the time | 0.619 | −0.039 |
| I am bothered by certain medical mistakes I have made | 0.406 | −0.065 |
| I feel overwhelmed in certain cases and cannot react professionally | 0.112 | −0.124 |
| I feel regret for the decisions I have made in the cases of certain patients | 0.220 | −0.095 |
| I always put patients first | 0.676 | −0.033 |
| I feel that I am not completely fair in the professional environment, having to make certain compromises | 0.408 | 0.064 |
| The responsibility I have at work is very high also due to the position I hold | 0.557 | 0.046 |
| Career progress issues | ||
| I am worried about the future of my chosen profession | 0.874 | −0.012 |
| I have time to update my knowledge or learn new things in my field | 0.828 | −0.017 |
| I am worried that I do not have a permanent employment contract | 0.557 | 0.046 |
| The country I live in has respected me for all the dedication and efforts made for patients | 0.133 | 0.117 |
| I felt respected by the hospital management and colleagues for my work and dedication | 0.757 | −0.024 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Țăranu, S.-M.; Ștefăniu, R.; Rotaru, T.-Ș.; Turcu, A.-M.; Pîslaru, A.I.; Sandu, I.A.; Herghelegiu, A.M.; Prada, G.I.; Alexa, I.D.; Ilie, A.C. Factors Associated with Burnout in Medical Staff: A Look Back at the Role of the COVID-19 Pandemic. Healthcare 2023, 11, 2533. https://doi.org/10.3390/healthcare11182533
Țăranu S-M, Ștefăniu R, Rotaru T-Ș, Turcu A-M, Pîslaru AI, Sandu IA, Herghelegiu AM, Prada GI, Alexa ID, Ilie AC. Factors Associated with Burnout in Medical Staff: A Look Back at the Role of the COVID-19 Pandemic. Healthcare. 2023; 11(18):2533. https://doi.org/10.3390/healthcare11182533
Chicago/Turabian StyleȚăranu, Sabinne-Marie, Ramona Ștefăniu, Tudor-Ștefan Rotaru, Ana-Maria Turcu, Anca Iuliana Pîslaru, Ioana Alexandra Sandu, Anna Marie Herghelegiu, Gabriel Ioan Prada, Ioana Dana Alexa, and Adina Carmen Ilie. 2023. "Factors Associated with Burnout in Medical Staff: A Look Back at the Role of the COVID-19 Pandemic" Healthcare 11, no. 18: 2533. https://doi.org/10.3390/healthcare11182533
APA StyleȚăranu, S.-M., Ștefăniu, R., Rotaru, T.-Ș., Turcu, A.-M., Pîslaru, A. I., Sandu, I. A., Herghelegiu, A. M., Prada, G. I., Alexa, I. D., & Ilie, A. C. (2023). Factors Associated with Burnout in Medical Staff: A Look Back at the Role of the COVID-19 Pandemic. Healthcare, 11(18), 2533. https://doi.org/10.3390/healthcare11182533